
Abstract
Background:
Patients with advanced cancer are increasingly expected to self-manage. Thus far, this topic has received little systematic attention.
Aim:
To summarise studies describing self-management strategies of patients with advanced cancer and associated experiences and personal characteristics. Also, to summarise attitudes of relatives and healthcare professionals towards patient self-management.
Design:
A systematic review including non-experimental quantitative and qualitative studies. Data were analysed using critical interpretive synthesis. Included studies were appraised on methodological quality and quality of reporting.
Data sources:
MEDLINE, Embase, Cochrane Central, PsycINFO, CINAHL, Web of Science and Google Scholar (until 11 June 2019).
Results:
Of 1742 identified articles, 31 moderate-quality articles describing 8 quantitative and 23 qualitative studies were included. Patients with advanced cancer used self-management strategies in seven domains: medicine and pharmacology, lifestyle, mental health, social support, knowledge and information, navigation and coordination and medical decision-making (29 articles). Strategies were highly individual, sometimes ambivalent and dependent on social interactions. Older patients and patients with more depressive symptoms and lower levels of physical functioning, education and self-efficacy might have more difficulties with certain self-management strategies (six articles). Healthcare professionals perceived self-management as desirable and achievable if based on sufficient skills and knowledge and solid patient–professional partnerships (three articles).
Conclusion:
Self-management of patients with advanced cancer is highly personal and multifaceted. Strategies may be substitutional, additional or even conflicting compared to care provided by healthcare professionals. Self-management support can benefit from an individualised approach embedded in solid partnerships with relatives and healthcare professionals.
Keywords
Self-management has predominantly been studied in the context of chronic diseases, where it has been defined as ‘the ability to manage the symptoms, treatment, physical and psychosocial consequences, and lifestyle changes inherent in living with the condition’.
Patients with advanced cancer experience severe, multidimensional symptoms and challenges and are increasingly expected to actively manage their health and care.
There still is a lack of insight into the full range of self-management experiences of patients with advanced cancer and the attitudes of relatives and healthcare professionals towards self-management of these patients.
This study demonstrates that self-management strategies of patients with advanced cancer span many domains: medicine and pharmacology, lifestyle, psychology, social support, knowledge and information, navigation and coordination and medical decision-making.
Patients’ self-management strategies and experiences are highly individual and divergent and may be substitutional, additional and distinctive or conflicting compared to care provided by healthcare professionals.
Healthcare professionals perceive self-management as both desirable and achievable if based on sufficient skills and knowledge and solid patient–professional partnerships.
Self-management support programmes for patients with advanced cancer can benefit from an individualised approach that re-evaluates patients’ needs and wishes, is embedded in solid partnerships with relatives and healthcare professionals, and is incorporated into existing models of care.
Future studies on self-management of patients with advanced cancer need to further examine attitudes of relatives and healthcare professionals and investigate effectiveness and working mechanisms at the levels of patients, communities and healthcare organisations and policy.
Introduction
Learning that one’s cancer has progressed to an advanced and incurable stage is for most patients and their relatives an overwhelming experience that often includes shifting from curative treatment to focusing on life extension and/or quality of life. Because patients have to live with the prospect of impending death and are increasingly unable to continue their daily activities and fulfil their usual social roles, they need to deal with considerable emotional, psychosocial and lifestyle consequences. 1 They do this in the face of increasing multidimensional symptoms, such as fatigue, pain, anxiety and depression.1–4 Although usually, many healthcare providers are involved in medical care,5,6 most of the time, patients, together with their relatives, need to manage a huge part of their care and lives themselves. This can be highly complex.
In recent years, patients have been increasingly stimulated to actively manage their health: healthcare policies have shifted towards out-of-hospital delivery of care, partly driven by increasing numbers of patients, 7 workforce challenges 8 and a tendency to reduce costs. 9 Self-management has frequently been studied in the context of chronic diseases, such as diabetes. In this context, self-management has been defined as ‘the person’s ability to manage the symptoms, treatment, physical and psychosocial consequences and lifestyle changes inherent in living with a chronic condition’. 10 Key to this definition is that self-management involves more than management of problems in the medical domain. A growing body of evidence demonstrates that people living with chronic conditions might use a wide range of self-management strategies, such as adhering to a special diet and dealing with emotions.10–18
Because advanced cancer is generally characterised by a shorter prognosis compared to chronic diseases, such as diabetes, and increased complexity of healthcare (including rapid medical–technological developments, such as immunotherapy), self-management domains and strategies observed among patients with chronic diseases cannot self-evidently be extrapolated to patients with advanced cancer. Yet, self-management of patients with advanced cancer has received surprisingly little systematic attention. Several studies have assessed the topic, but among these studies, there is a lack of conceptual clarity (e.g. inconsistent use of terms like self-management, self-care and self-help; either a broad focus or a focus on certain domains, such as symptom self-management) and a large degree of heterogeneity regarding study designs and patient populations (e.g. all cancer types vs specific cancer types). Previous reviews have shown that patients with advanced cancer engage in multiple different self-management behaviours, including psychosocial and emotional strategies, to manage the end of life, such as preparing for death.19,20 However, one systematic review was published in 2009, 20 whereas especially in the past decade, healthcare policies have increasingly steered towards out-of-hospital care and patient self-management, presumably affecting self-management experiences. The other review concerns a scoping review that predominantly focuses on self-management support interventions and lacks quality appraisal of the included studies. 19 In addition, both reviews only assess patient perspectives, while it is also relevant to include perspectives of relatives and healthcare professionals.21–25 Comprehensive insight in self-management of this vulnerable patient population is needed to develop healthcare policies and self-management support programmes that are tailored to the needs and abilities of patients and their relatives, while also fitting in the healthcare system. Hence, this integrated systematic review of empirical studies aimed to obtain this insight by thoroughly analysing the non-experimental evidence currently available. For the population of patients with advanced cancer, we therefore examined the following:
The concept of self-management and its domains;
Patients’ self-management strategies and corresponding experiences;
Patient characteristics that might be associated with the use of self-management strategies;
The attitudes of relatives and healthcare professionals towards patient self-management.
Methods
Design
Following the principles of a mixed research synthesis, 26 we conducted a systematic review 27 of published non-experimental quantitative and qualitative research. We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for reporting and presentation of the flow of information through the different phases of the review. 28
Data collection
With help of biomedical information specialists (G.d.J. and W.B.), systematic electronic searches were performed in MEDLINE (Ovid), Embase, Cochrane Central, PsycINFO (Ovid), CINAHL (EBSCO), Web of Science and Google Scholar from inception until 11 June 2019. Supplementary Table 1 lists the search terms. Search components consisted of Medical Subject Headings (MeSH terms) or equivalent and free text words related to (1) self-management (identified using MeSH trees and search strings of previous research) and (2) advanced cancer. No automatic restrictions were placed on study type and year and language of publication. Articles were entered in Endnote, and duplicates were removed.
Study selection
Articles were included when they met the inclusion criteria (see Box 1). To determine eligibility of articles that purported to be on self-management (or a related search term), we adapted Barlow’s self-management definition to the context of advanced cancer. 10 The advanced cancer criterion was considered met when articles specifically addressed a population of patients with cancer that was ‘unlikely to be cured’. 29 Healthcare professionals may also use the terms ‘secondary’, ‘metastatic’, ‘terminal’ or ‘progressive’ cancer to describe it. Studies were only included if they reported results specifically for this patient group (i.e. studies addressing a mixed population with various cancer stages were excluded if they did not stratify results according to cancer stage). We selected articles with non-experimental quantitative, qualitative and mixed-method study designs. 26
Box 1.
Inclusion criteria for study selection.
1. Articles concerning self-management (i.e. ‘the strategies used by persons to manage the symptoms, treatment, physical and psychosocial consequences and lifestyle changes inherent in living with advanced cancer’). 10
2. Articles concerning patients with advanced cancer (i.e. ‘cancer that is unlikely to be cured’). 29
3. Articles concerning perspectives of patients with advanced cancer, their relatives (not necessarily restricted to family members, but could also include significant others, for example, close friends) and/or healthcare professionals.
4. Articles concerning empirical research with a non-experimental quantitative, qualitative or mixed-methods study design and a sample size of ⩾1 (i.e. no case studies, case reports, reviews and intervention studies). 26
5. Articles published in the English or Dutch language in peer-reviewed scientific journals (i.e. no conference proceedings, abstracts and posters).
6. Articles concerning adults (⩾18 years) only.
Two reviewers (K.d.N. and S.I.v.D.) independently used a stepwise procedure to identify relevant articles. In case of disagreement, consensus was reached through discussion with a third reviewer (J.A.C.R.). Study selection was carried out with the online software Covidence. 30 Articles were first screened based on title and abstract. Subsequently, remaining articles were screened based on full text. Articles of references selected for full text evaluation were downloaded, or, if not electronically available, requested from the first author. If full text articles were excluded, the first of the hierarchical inclusion criteria not satisfied (see Box 1) was considered the main reason for exclusion.
Quality appraisal
Two reviewers (K.d.N. and R.S.) independently appraised the quality of included studies. Methodological quality of quantitative studies was assessed using a modified version of the guidelines of Cochrane Netherlands.31,32 This form consists of the following seven items: (1) research hypothesis, (2) study population, (3) selection bias, (4) exposure, (5) outcome, (6) confounding and (7) general opinion. Each criterion was assigned a score of 1 when it was sufficiently met, a score of 0 when it was insufficiently met or a question mark when it could not be rated due to lacking information. For each of the studies, a total score was calculated (ranging from 0 to 7). The quality of reporting of the qualitative studies was assessed with the consolidated criteria for reporting qualitative research (COREQ) checklist, which is recommended by Cochrane Netherlands. 33 The COREQ checklist also includes aspects of methodological quality and is applicable to various types of qualitative research.33,34 It consists of 32 items that evaluate three domains, that is, (1) research team and reflexivity, (2) study design and (3) analysis and findings. Each criterion was assigned a score of 1.0 when it was properly described, a score of 0.5 when it was partially described or a score of 0.0 when it was not or unclearly described. For each of the studies, a total score was calculated (ranging from 0.0 to 32.0). Disagreements were discussed and resolved.
Data extraction and data analyses
To systematically extract data from included articles, we developed a data extraction form. This form included items on general study characteristics and characteristics of the study population. It also included open items about the definition of self-management and the self-management strategies addressed. We also extracted information regarding patients’ experiences and characteristics associated with these self-management strategies. In addition, we extracted information concerning the attitudes of relatives and healthcare professionals towards patient self-management. The extraction form was completed by two reviewers (K.d.N. and S.I.v.D.); disagreements were solved by discussion.
Data were analysed using critical interpretive synthesis. 35 Departing from the framework of self-management support components developed by Barlow and colleagues in the context of chronic diseases, 10 we categorised self-management strategies into domains. Subsequently, we integrated data on self-management strategies with data on corresponding experiences, and compared these findings within and across self-management domains. In addition, we interpreted findings in light of self-management definitions provided by the included studies and compared them with findings from the context of chronic diseases.
Results
Study selection
The database search yielded 2935 articles (see PRISMA flowchart in Figure 1). After removal of duplicates, 1742 articles were screened based on title and abstract. The remaining 187 articles were screened based on full text. Finally, 31 articles about 31 unique studies were included for analysis. Eight of these articles had a quantitative study design and 23 of them had a qualitative study design (see Table 1).
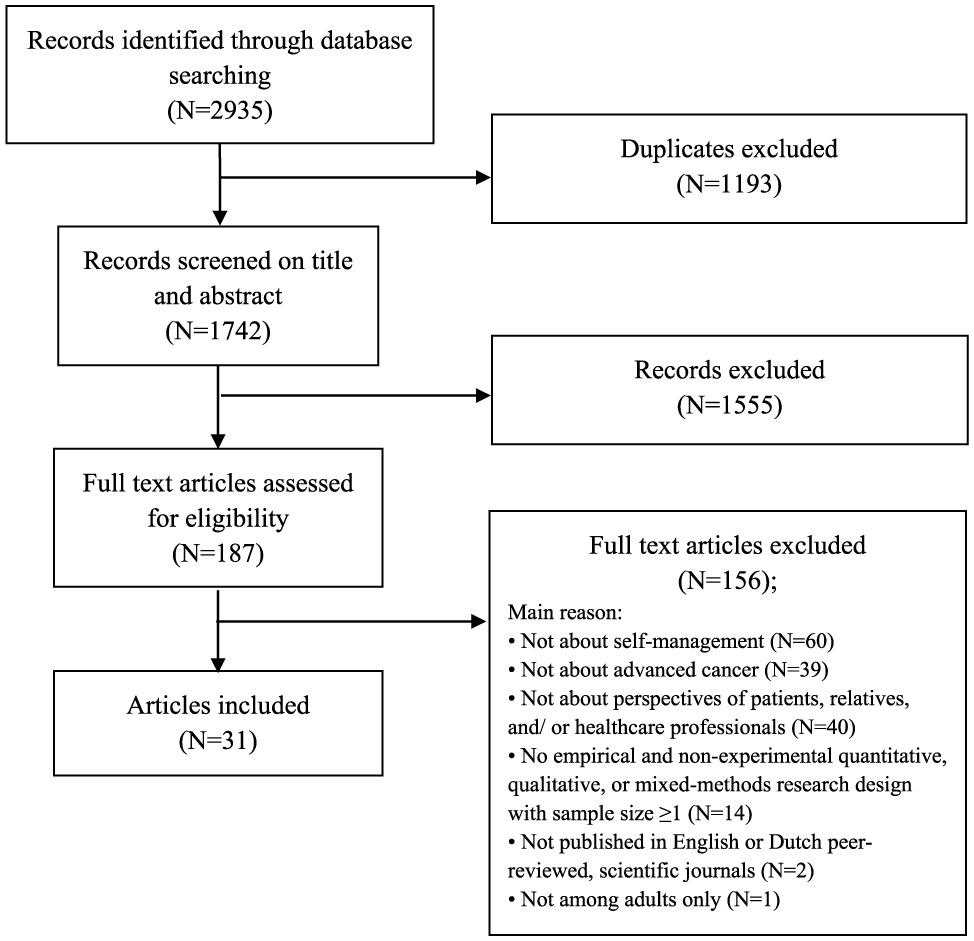
Process of study selection (PRISMA flowchart).
Characteristics of the included articles (31 studies).
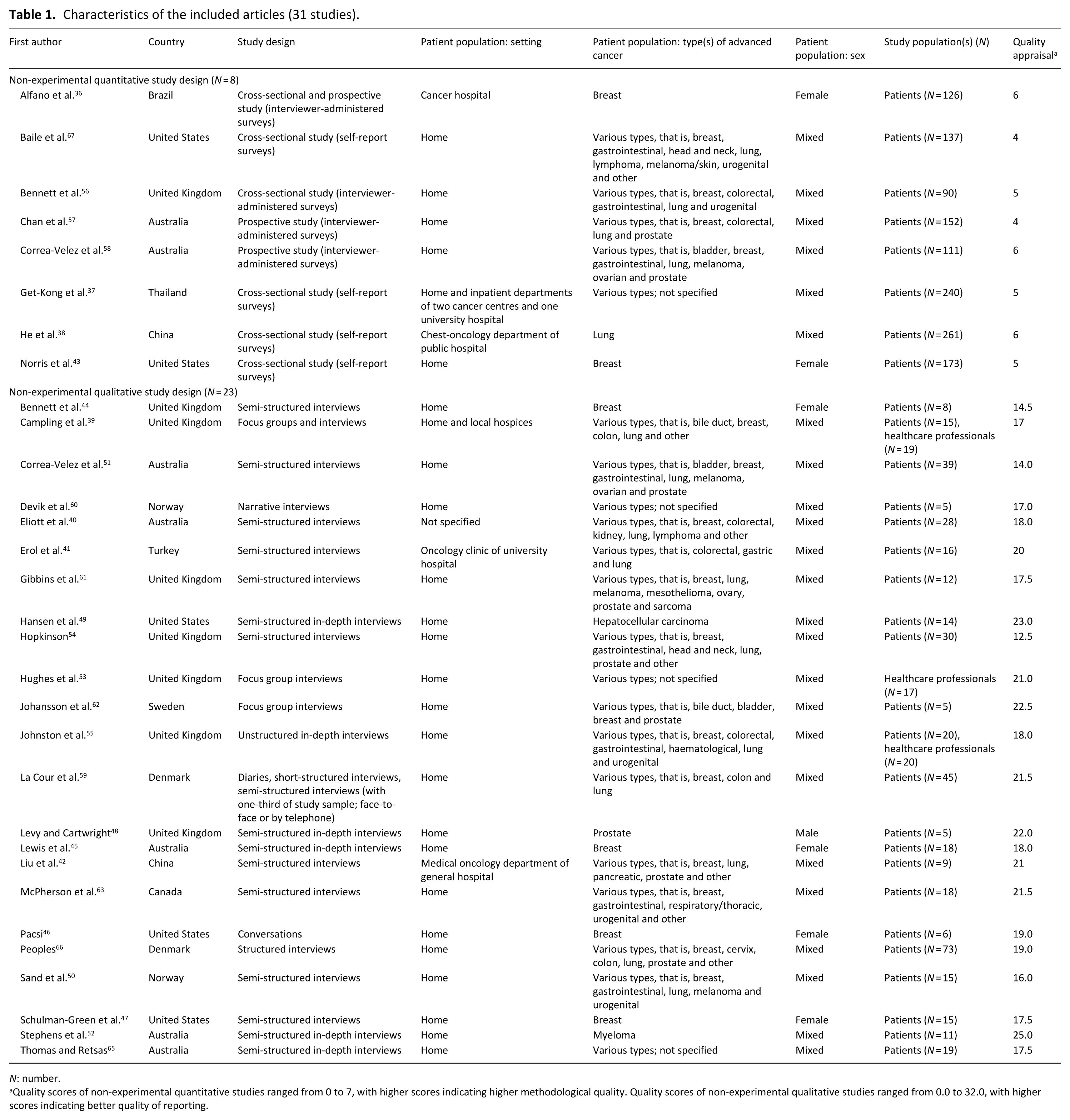
N: number.
Quality scores of non-experimental quantitative studies ranged from 0 to 7, with higher scores indicating higher methodological quality. Quality scores of non-experimental qualitative studies ranged from 0.0 to 32.0, with higher scores indicating better quality of reporting.
Quality of included studies
For non-experimental quantitative studies, the mean total methodological quality score was 5 out of 7 (range: 4–7; see Table 1). The studies had good ratings on the criteria for ‘Research hypothesis’, ‘Study population’ and ‘Outcome’, but nearly all of them scored poorly on the criteria for ‘Selection bias’ and ‘Confounding’. For qualitative studies, the mean total score for quality of reporting was 19.0 out of 32.0 (range: 12.5–25.0). Almost all qualitative studies had poor ratings on the first domain, ‘Research team and reflexivity’. Generally, studies with the highest scores on the first domain also provided sufficient information on the domains ‘Study design’ and ‘Analysis and findings’, thus resulting in a higher overall quality score.
Study characteristics
Study populations of 28 studies consisted of patients (see Table 1), one study was conducted among healthcare professionals only, and two studies contained both groups. None of the studies assessed the perspective of relatives. All but seven articles described assessment of self-management of patients residing primarily at home.36–42 Except for five studies that were performed in Brazil, China, Thailand and Turkey, respectively,36–38,41,42 studies were conducted in high-income countries, such as Australia (seven studies), Canada (one study), the United Kingdom (eight studies), the United States (five studies) and Scandinavia (five studies). Eighteen studies included various cancer diagnosis groups; the other studies specifically focused on lung cancer, 38 breast cancer,36,43–47 prostate cancer, 48 hepatocellular cancer 49 or myeloma. 43 Some studies focussed on assessing specific self-management strategies, such as medication management, 50 or the use of complementary and alternative medicine.36,51
The concept of self-management and its domains in patients with advanced cancer
Self-management definitions
Twenty-one of the 31 included articles did not explicitly define self-management or any of the related terms. Three of the included articles provided a definition of ‘self-management’.47,52,53 Three other articles defined ‘self-care’.43,54,55 These definitions are described in Box 2. One of the definitions relates self-management to self-care, describing self-management as ‘maintaining ones usual practices of self-care’. 55 While some definitions conceptualise self-management as behaviours (or strategies, actions, activities, practices),43,53–55 others also include patients’ self-management skills, such as action-planning and using resources.47,52 Most definitions focus predominantly on the patient, with one of them explicitly emphasising the aim of self-mastering problems rather than relinquishing these to others. Yet, two definitions assign a role for relatives and healthcare professionals as well, describing self-management as a participatory process that may even be undertaken to serve (well-being of) others. 54 Finally, the self-management definitions cover various domains of health and functioning and include different self-management outcomes, for example, enhanced quality of life,43,54 maintenance of physical and mental health and/or daily functioning,43,54 reduced symptom burden 53 and increased coping. 53
Box 2.
Definitions of self-management or related terms in the included articles.
‘Self-management’ (three articles):
• ‘Self-management has been defined as any behaviour which an individual engages in specifically to try and relieve, minimise or prevent pain or more broadly to cope with their illness’. 53
• ‘Self-management involves daily behaviours that individuals perform to handle a health condition, it includes the skills of problem solving, goal setting, decision making, using resources, forming patient-provider partnerships, action planning, and self-tailoring’. 47
• ‘Self-management has been described as a participatory process where patients and clinicians develop strategies together to equip patients with the skills and knowledge to manage the impact of the condition, monitor their disease and make effective use of support services outside of the clinical setting’. 52
‘Self-care’ (three articles):
• ‘Self care includes the actions individuals and carers take for themselves, their children and their families to stay fit and maintain good physical and mental health; meet social and psychological needs; prevent illness or accidents; care for minor ailments and long-term conditions; and maintain health and well-being after an acute illness or discharge from hospital’. 54
• ‘Self-care can be used as an umbrella term to refer to all activities of self-management. [. . .]. It is defined as “maintaining ones usual practices of self-care – those things that are important and unique to oneself in maintaining ones sense of self. . . being given the means to master or deal with problems, rather than relinquish them to others”. 55
• ‘Self-care involves the voluntary use of activities to promote one’s own well-being. Self-care has been defined as the range of voluntary activities that an individual uses to maintain life, health and well-being’. 43
Self-management domains
Self-management strategies used by patients in the 29 non-experimental quantitative and qualitative studies could be categorised into seven overarching domains: medicine and pharmacology, lifestyle, psychology/mental health, social support, knowledge and information, navigation and coordination and medical decision-making (see Table 2). Five studies provided information about one self-management domain,36,40,51,54,55 five studies reported on two self-management domains44,56–59 and the remaining 19 studies covered three or more self-management domains.
Self-management domains and self-management strategies used by patients with advanced cancer (29 studies).
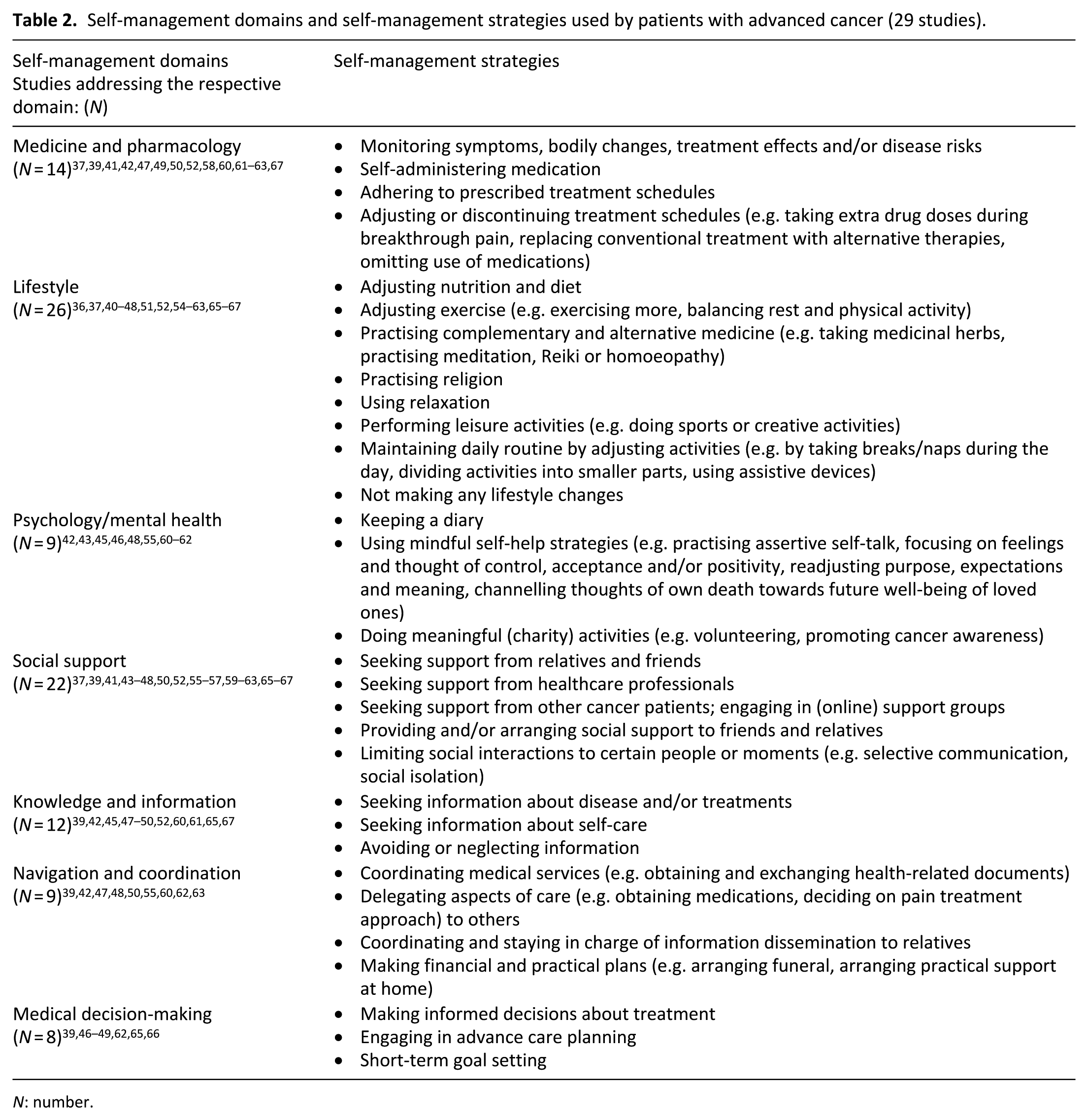
N: number.
Self-management strategies and corresponding experiences of patients with advanced cancer
Non-experimental quantitative results concerning self-management strategies and corresponding experiences of patients with advanced cancer are displayed in Table 3. The results of the qualitative studies are presented in Supplementary Table 2.
Non-experimental quantitative study results on self-management strategies and associated experiences and personal characteristics of patients with advanced cancer (eight studies).
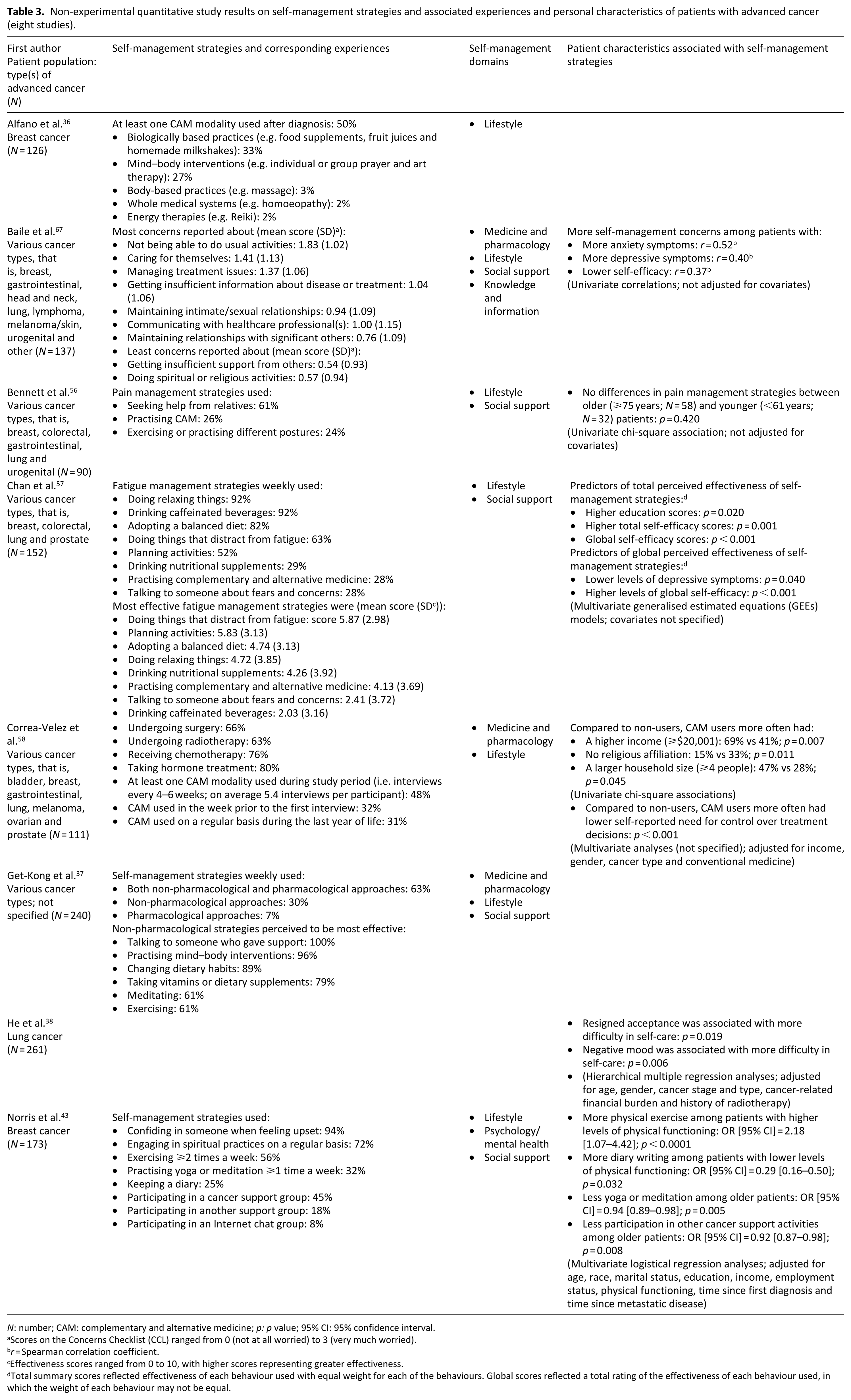
N: number; CAM: complementary and alternative medicine; p: p value; 95% CI: 95% confidence interval.
Scores on the Concerns Checklist (CCL) ranged from 0 (not at all worried) to 3 (very much worried).
r = Spearman correlation coefficient.
Effectiveness scores ranged from 0 to 10, with higher scores representing greater effectiveness.
Total summary scores reflected effectiveness of each behaviour used with equal weight for each of the behaviours. Global scores reflected a total rating of the effectiveness of each behaviour used, in which the weight of each behaviour may not be equal.
Medicine and pharmacology
Medical and pharmacological strategies varied from self-monitoring 49 and self-administering medications and following prescribed treatment regimens37,47,58,60 to adjusting or discontinuing treatment schedules and taking extra doses of additional (pain) medications.39,41,42,47,50,52,61–63 Patients used self-monitoring to better understand and describe their disease. 49 Reasons for not taking medications as prescribed included a desire to alleviate suffering, 62 attempts to find the optimal balance between beneficial and adverse (side) effects,39,50,63 fears of tolerance and addiction, 63 non-pharmacological alternatives to manage pain, 63 preferring ‘grip on the pain’ over ‘becoming pain free’, 61 sedative side effects that were experienced to be a ‘threat to usual self’ 61 and uncertainty about treatment efficacy. 49
Lifestyle
Within the lifestyle domain, we identified different self-management strategies. Three non-experimental quantitative studies showed that 24%–56% of the patients used physical exercise to manage symptoms, for instance, fatigue.37,43,56 Two quantitative studies37,57 and three qualitative studies46,52,54 showed that many patients changed their diet (i.e. 70%–82% adopted a balanced diet). The two quantitative studies also indicated that 92% and 89%, respectively, used relaxation to relieve cancer symptoms.37,57 In addition, six quantitative studies showed that 26%–72% of the patients used at least one complementary and alternative medicine modality (classified according to the criteria provided by the National Centre for Complementary and Alternative Medicine), 64 such as acupuncture or homoeopathy.36,37,43,56–58 Both quantitative and qualitative studies provided evidence that patients experienced benefits from using complementary and alternative therapies, such as an improved quality of life.40,51,55,65 Generally, health behaviours were adopted or changed in order to prolong life,40,58 boost strength, energy and immunity,52,58 improve quality of life,40,51,62 increase feelings of control and independence40,54 and please relatives.40,54 Some patients decided to spend more time on their hobbies or engaged in new hobbies to distract them from disease-related symptoms and concerns,41,42,48,61–63 maintain physical ability 48 or get a sense of enrichment.48,59 At the same time, patients indicated to strive for normality and maintenance of usual daily activities: 10 qualitative studies45–48,55,59–62,66 and 1 quantitative study 67 showed that this was of great importance to most of them among others because it made them feel functional and helped them to maintain role, self and independence. For some patients, continuing life as it used to be was so important that they deliberately chose not to make any major lifestyle changes at all. 45 Other patients maintained their daily routine using assistive devices, adjusting activities, dividing tasks into smaller parts or taking more breaks during the day.61–63,66
Psychology/mental health
Several patients managed their psychological well-being by keeping a diary 43 and participating in meaningful charity activities, such as volunteering and promoting cancer awareness.46,48 Furthermore, eight qualitative studies showed that patients used assertive self-talk or tried to control or accept their situation, readjust purpose, expectations and meaning in life, think of their family’s future well-being rather than of their own death and focus on positive thoughts (e.g. good memories) and feelings.42,45,46,48,55,60–62 This often enhanced coping with the disease, but could also lead to psychological turmoil when motives were incompatible. 48
Social support
Four quantitative37,43,56,57 and 15 qualitative studies 39,45–48,50,52,55,59–63,65,66 indicated that many patients sought support from relatives and friends (28%–94% in the quantitative studies). This was mentioned as an effective strategy by 61% and 100% of the patients in two quantitative studies on pain management and general symptom management, respectively.37,57 Besides seeking social support, providing or arranging social support for relatives was also mentioned as a self-management strategy.45–48,62 Patients considered maintaining or intensifying relationships with relatives important, because it gave them emotional strength,45,57,60,65 provided distraction from their cancer symptoms, 62 made them feel important and helpful to others, 62 protected their identities and usual social roles 48 and enabled them to rely on relatives in case their condition would worsen. 39 In several qualitative studies, however, patients also mentioned that they found it difficult to accept or ask for support from relatives and friends, because they did not want to be a burden.55,59–63,65 Some of them only asked for help when they could no longer perform their usual activities50,60,61,63,66 or restricted their social contacts to close relatives or moments when they felt good.57,66 Some patients mentioned selective communication of their thoughts and emotions or self-isolation as strategies to protect themselves and their loved ones from mental and emotional distress.48,52,57,63 A quantitative study among women with metastatic breast cancer demonstrated participation in cancer support groups (45%), Internet chat groups (8%) and other cancer support programmes (18%). 43 Compared to support from relatives and friends, support from fellow patients was sometimes perceived to be more effective.55,59,65 Some patients experienced professional support as positive when the severity of their pain increased, 41 others reported that this depended on the person providing it.55,60,62,65 According to other patients, healthcare professionals listened insufficiently or paid too little attention to their emotional needs.50,61,65
Knowledge and information
Several patients searched for more information about their disease, care and treatment.37,39,42,47–49,52,61,65,67 Most of them perceived this as an effective strategy to manage symptoms and other disease consequences, as it empowered them to optimise both their physical and psychological well-being.48,52 Also, lack of understanding of, for example, the meaning of palliative care or cancer symptoms could lead to confusion and concerns and, subsequently, hamper effective self-management.47,60 However, when obtaining useful information was complicated, this could also become a burden. 47 Some patients preferred not to think, talk or read about cancer over obtaining knowledge and information, as this made them feel able to exert control over their disease experiences and protected them from sad feelings. 45
Navigation and coordination
Three studies described how patients prepared for their death by making financial and practical plans (e.g. planning funeral, sorting out affairs).48,55,62 This was considered beneficial, because it enhanced patients’ feelings of control over their death and the future well-being of their families, thus also protecting their own identities and family roles. 48 In another study, patients with advanced breast cancer coordinated medical services between different healthcare providers, for example, by collecting and exchanging health-related documents. 47 Patients also coordinated their care by delegating some of its aspects (e.g. responsibility for making and attending medical appointments, decisions on pain treatment approach) to relatives and friends,47,50,63 and by delegating or staying in charge of information dissemination from healthcare professionals to relatives or vice versa.39,63 A study among older patients who received outpatient cancer treatment and lived alone in rural areas showed that these patients perceived limited control over practical arrangements (e.g. arranging treatment schedules and public transport back home) and experienced navigating through the healthcare system (e.g. ordering tests, making appointments) as very energy-consuming. 60
Medical decision-making
Several patients participated in advance care planning or made together with their healthcare professionals shared decisions regarding future medical care and treatments. 47 Others used short-term goal setting as a strategy to reach long-term goals.39,48,65,66 Over time, several patients shifted their focus on quality of life, and for this reason, some of them considered foregoing treatment. 49
Personal characteristics associated with the use of self-management strategies among patients with advanced cancer
Two studies explored the cross-sectional association between age and self-management strategies (see Table 3). Older and younger patients did not differ in pain management strategies, 56 but younger patients were shown to be more likely than older patients to practise yoga/meditation and to participate in other cancer patient support activities (e.g. cancer retreats). 43 Patients with higher levels of physical functioning were more likely to practise physical exercise, while patients with lower levels of physical functioning were more likely to keep a diary. Use of complementary and alternative medicine seemed to be more prevalent among patients with higher income levels, larger household sizes, no religious affiliation and less need for control over treatment decisions. 58 Higher education and self-efficacy levels and lower depressive symptom levels were positively associated with perceived effectiveness of self-management behaviours. 57 Resigned acceptance and negative mood were associated with more difficulty. 38 Furthermore, patients with lower self-efficacy and more anxiety and/or depressive symptoms reported more self-management concerns. 67
Healthcare professionals’ attitudes towards self-management of patients with advanced cancer
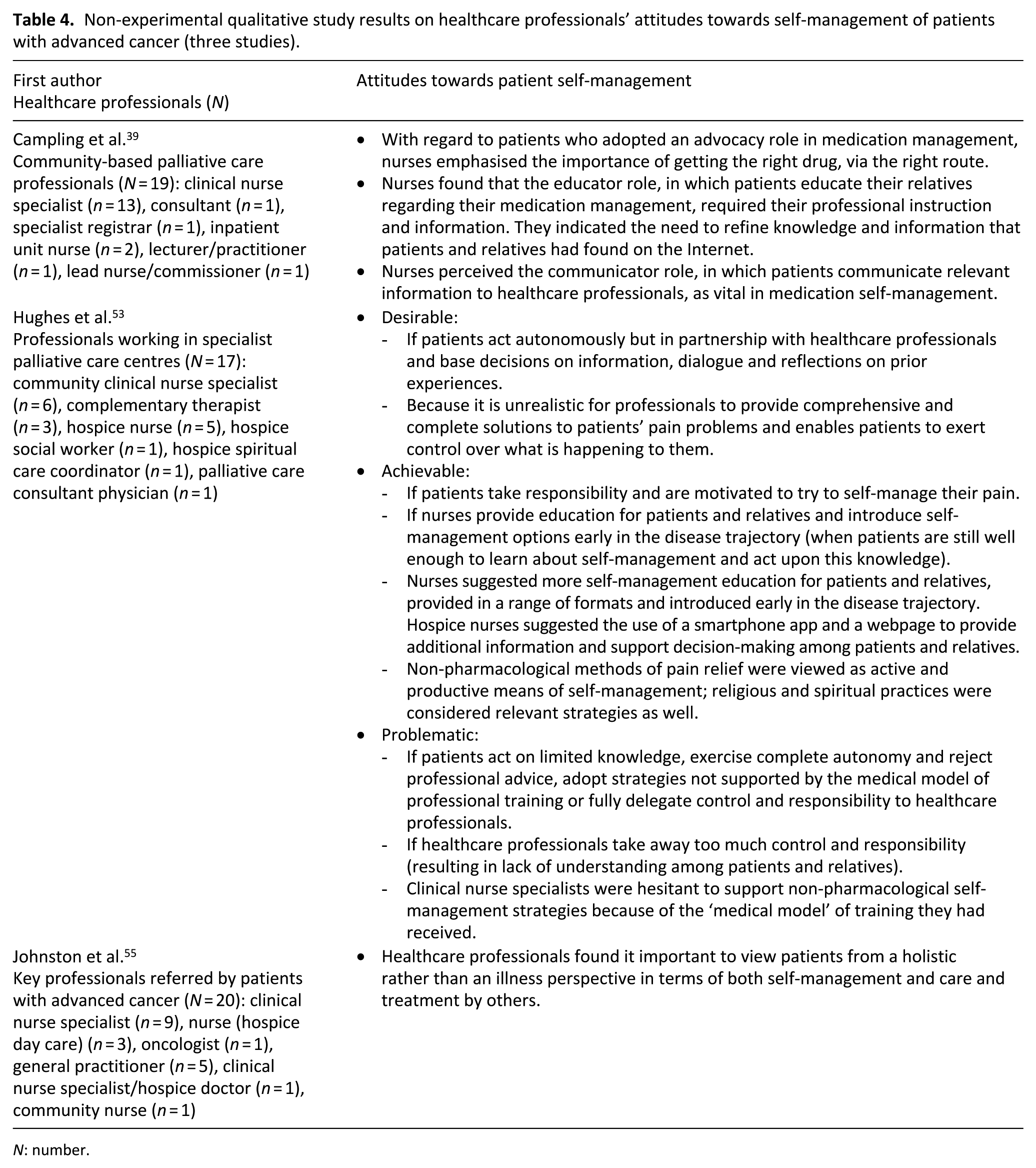
Table 4 summarises the three articles about attitudes of healthcare professionals towards self-management of patients with advanced cancer. In one study, primary healthcare professionals concurred with patients in their view that it is important to view a patient holistically, that is, as an entire person rather than an illness, in terms of both self-management and care and treatment by others. 55 Another study showed that healthcare professionals working in a specialist palliative care service perceived patient self-management as both desirable and achievable, but only if undertaken in partnership with them. 53 Self-management could also be perceived as problematic, for example, when patients acted on limited knowledge. 53 Some clinical nurse specialists were worried about supporting non-pharmacological methods because of the ‘medical model’ of training they had received. Nurses suggested more self-management education for patients and their relatives, for example, by means of a smart phone app and a webpage that stimulated active participation in obtaining information and medical decision-making. 53 Community-based palliative care nurses also indicated that patients required their instruction and information to adequately educate their relatives regarding medication management. 39 Communication between patients and healthcare professionals was perceived as vital in medication self-management. 39
Non-experimental qualitative study results on healthcare professionals’ attitudes towards self-management of patients with advanced cancer (three studies).
N: number.
Discussion
Main findings
This review summarised results from 31 non-experimental quantitative and qualitative studies that examined self-management of patients with advanced cancer. The vast majority of these studies were of acceptable quality and examined self-management from the perspective of patients. Most studies included mixed sex and diagnosis groups and had been conducted in Western high-income countries. Overall, the reviewed literature clearly shows that self-management of patients with advanced cancer covers numerous domains: medicine and pharmacology (e.g. self-administering pain medications), lifestyle (e.g. practising complementary and alternative medicine, taking breaks when doing daily chores), psychology (e.g. keeping a diary), social support (e.g. engaging in support groups), knowledge and information (e.g. seeking treatment information), navigation and coordination (e.g. making financial plans) and medical decision-making (e.g. participating in advance care planning). Within each of these domains, patients might use multiple strategies that are highly individual, sometimes ambivalent and generally aimed at optimising their own well-being and/or (future) well-being of loved ones. Healthcare professionals perceive self-management as both desirable and achievable if based on sufficient skills, knowledge, information and solid patient–professional partnerships.
That strategies used by patients with advanced cancer vary widely and sometimes even comprise contradictory behaviours is well illustrated by our data on lifestyle self-management strategies, which was the domain most often addressed by the included studies. On the one hand, patients frequently mentioned that the diagnosis of advanced cancer had caused them to change lifestyle habits and start complementary and alternative medicine or new hobbies. On the other hand, however, many of them also indicated that they preferred to maintain their usual daily routines as much as possible. In the social support domain, self-management strategies also varied strongly, from seeking and providing social support to limiting and even avoiding social support. Although most patients experienced social support as essential, for some of them, seeking and accepting it was hampered by fears of becoming a burden to loved ones and losing their established roles and identity. A large diversity of strategies and experiences with these strategies was observed in the other self-management domains as well. Medical and pharmacological strategies ranged from adhering to prescribed treatment to adjusting and discontinuing treatment. Whereas some patients actively gathered information about treatment and disease, others avoided obtaining more knowledge, because it was too energy-consuming or made them feel sad. More generally, ambiguity and inconsistency in self-management strategies often seemed to reflect a conflict between two seemingly opposing attitudes: appreciating life in the present versus planning for the future; readjusting purpose and expectations versus maintaining normality and a sense of established identity; and taking control versus letting things happen.
By including a larger number of studies as well as more recent studies, and by focussing more specifically on patients’ self-management strategies and healthcare professionals’ attitudes, our systematic review provides novel insights compared to the two prior review studies on self-management in advanced cancer care.19,20 The scoping review of Budhwani and colleagues merely distinguished between physical and psychosocial domains, 19 while our review also describes domains of lifestyle, knowledge and information, navigation and coordination and medical decision-making. Furthermore, we provide a more detailed overview of the full range of self-management strategies and experiences in these domains, thereby also revealing divergence and ambivalence between these strategies and experiences. Only a few studies explicitly defined self-management (or self-care). Although these definitions were not univocal regarding the nature of self-management, our review’s findings on the divergence of strategies and experiences suggest that the question should not be whether or not, but how someone engages in self-management. This corroborates the previously proposed idea that ‘one cannot not self-manage’ 15 and argues against a normative approach to self-management (support). It also implies that self-management, although affected by personal and contextual factors, is not restricted to particular settings or disease stages. It may thus be facilitated anywhere and anytime (until the very end), if tailored to individual circumstances, abilities and preferences.
The seven domains we distinguished partly overlap with those observed within chronic disease populations, the field on which studies about disease self-management have thus far predominantly focused. Many of the models proposed to describe and enhance chronic disease self-management also include domains of social support, information, navigation and decision-making.10,11,17,18 Remarkable, however, is that the self-management strategies and experiences we identified among patients with advanced cancer are generally more divergent and ambivalent than those described for patients with chronic, generally less advanced diseases. For example, while we found that avoiding or ignoring (medical) information may be a self-management strategy among patients with advanced cancer, reviews about self-management among patients with chronic diseases merely report on the opposite, that is, seeking and obtaining information.10,68–71 Possibly, the prospect of imminent deterioration and, ultimately, death adds to the complexity of self-management. After all, these prospects can drastically change the way someone relates to space, place, time, self and others. These changes, in turn, interact and consequently affect self-management, thus complicating its dynamics and increasing its susceptibility to different, potentially competing values, priorities and interests. This interpretation is supported by recent chronic disease studies showing that self-management is perceived to be more challenging during periods of transition, disease progression or acute events (e.g. exacerbations of chronic obstructive pulmonary disease).16,72,73 It also resonates with findings from several advanced disease studies.22,74–78 Two recent systematic reviews indicated that patients with advanced diseases were ambivalent towards discussing mortality and advance care planning.77,78 Furthermore, a recent literature review on life values of elderly people with advanced cancer showed that these patients often fluctuated between avoiding and facing the truth about their medical condition. 75 Many of them also considered maintaining independence and withholding emotions to contribute to a good death, as this was perceived to minimise strain on their loved ones.
In six studies, we identified several sociodemographic and functional patient characteristics that might affect self-management of patients with advanced cancer. These results were derived from non-experimental quantitative studies with moderate sample sizes and limited adjustments for confounding and selection bias, and should thus be interpreted cautiously. Nevertheless, they provide some explorative insights that could generate hypotheses for future research. Younger patients and patients with higher levels of physical functioning might, for instance, be more likely to adopt physically and socially active self-management strategies (e.g. yoga, physical exercise, participation in cancer support groups) than older patients and patients with lower levels of physical functioning.43,56 Another study suggested that fewer depressive symptoms, higher educational levels 57 and greater self-efficacy 57 positively predicted self-perceived effectiveness of applied self-management strategies. 57 Resigned acceptance and negative mood were also associated with more self-management difficulties. 38 One of the explanations could be that patients with more depressive symptoms and a negative mood lack motivation and energy to actively self-manage. 79 In addition, higher educated patients are generally more health-literate, 80 and might therefore be more likely than lower educated patients to take a proactive approach in self-management and acquire accurate knowledge and understanding of their condition and self-management possibilities.16,81 Furthermore, patients with higher self-efficacy levels are more likely to perceive symptoms and other disease consequences as modifiable and might therefore invest more in self-management strategies than patients with lower self-efficacy levels. 82
Only three qualitative studies assessed attitudes of healthcare professionals towards patient self-management.53,55 Healthcare professionals in these studies were generally optimistic about patient self-management, but also set conditions for its effectiveness, such as solid patient–professional partnerships and sufficient skills, knowledge and information. Suggestions to provide patients with more education, introduced early in the disease trajectory and in a range of different formats, are in line with remarks made by nurses participating in a recent online focus group study on self-management support and eHealth for patients and relatives confronted with advanced cancer. 83 We identified a lack of studies among relatives, and inconsistencies regarding the roles and responsibilities assigned to others (i.e. healthcare professionals, relatives) in the self-management definitions provided by some of the included studies. Nevertheless, our findings evidently show that important others play a crucial role in patient self-management, and should thus somehow be involved in self-management support. However, also fears of becoming a burden to relatives were commonly described by patients in our review as well as in previous studies.84,85 Together with findings that some patients appreciated each other’s company and derived satisfaction from participation in cancer-related charity activities, this suggests that peer support could be a promising pillar in patient self-management. The mutual benefits of peer support are increasingly recognised, also among patients with advanced cancer.86,87
Strengths and limitations
To our knowledge, this is the first systematic review on patient self-management in advanced cancer care that includes perspectives of both patients and healthcare professionals. A strength is that we used a comprehensive search strategy with a broad operational definition of self-management. Nevertheless, we may have missed studies reporting on self-management without labelling it as such (or as a related term, e.g. self-care). The moderate quality of some of the included individual studies affected the evidential value of this systematic review, especially regarding selection bias: patients who had participated in the included studies may have been more able and willing to engage in the self-management strategies studied. This may have caused an overestimation of the prevalence and impact of self-management strategies.
Relevance for clinical practice
Our review provides several clinically relevant insights into self-management in the context of advanced cancer. Compared to care provided by healthcare professionals, patients’ self-management strategies may be substitutional (such as self-administering pain medications at home), additional and distinctive (such as mobilising peer support) or even conflicting (such as refraining from taking prescribed medications). This highlights the importance of solid patient–professional partnerships, in which preferences, experiences and expertise are mutually shared. Our review also provides a foundation for the development of self-management support interventions. Such programmes should be tailored to the domains in which patients need additional support. The findings on sociodemographic and functional characteristics associated with self-management strategies also provide useful preliminary targets for self-management support programmes. For example, patients with low levels of education may need additional support in self-management domains of information, and navigation and coordination. Finally, a key challenge in the development of self-management support programmes will be to incorporate them into existing models of care. 19
Implications for future research
To enhance conceptual clarity regarding self-management in the advanced cancer context, we recommend consistency in terminology used as well as further elaboration of its definition and conceptual framework. Given the important role of formal and informal caregivers in supporting patient self-management, additionally, we recommend that future studies identify their experiences and attitudes as well. Finally, we recommend that future studies investigate the effectiveness and working mechanisms of self-management strategies used by patients with advanced cancer at the levels of patients, communities and healthcare organisations and policy.
Conclusion
This systematic review shows that self-management of patients with advanced cancer is complex and multifaceted, covering multiple domains and a broad range of strategies and experiences that are highly dependent on individual preferences and characteristics. Possibly, the prospect of imminent deterioration and death adds to its complexity, as subsequent changes in values, priorities, interests and social interactions are likely to affect self-management strategies and experiences. Therefore, self-management support programmes for this vulnerable group could benefit from an individualised approach that re-evaluates patients’ needs and wishes, is embedded in solid partnerships with relatives and healthcare professionals, and is incorporated into existing models of care.
Supplemental Material
Systematic_Review_Self-Management_Advanced_Cancer_-_Revisie_-_Supplementary_files-1 – Supplemental material for Self-management of patients with advanced cancer: A systematic review of experiences and attitudes
Supplemental material, Systematic_Review_Self-Management_Advanced_Cancer_-_Revisie_-_Supplementary_files-1 for Self-management of patients with advanced cancer: A systematic review of experiences and attitudes by Sophie I van Dongen, Kim de Nooijer, Jane M Cramm, Anneke L Francke, Wendy H Oldenmenger, Ida J Korfage, Frederika E Witkamp, Rik Stoevelaar, Agnes van der Heide and Judith AC Rietjens in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank Gerdien de Jonge and Wichor Bramer, biomedical information specialists, at the Erasmus University Medical Centre Rotterdam, for assisting in developing and conducting the search strategy for this systematic review.
Author contributions
All authors have contributed to the following categories for authorship: (1a) study conception and design: S.I.v.D., K.d.N. and J.A.C.R.; (1b) acquisition of data: S.I.v.D., K.d.N. and J.A.C.R.; (1c) analysis and interpretation of data: S.I.v.D., K.d.N., J.M.C., A.L.F., W.H.O., I.J.K., F.E.W., R.S., A.v.d.H. and J.A.C.R.; (2) drafting the article: S.I.v.D., K.d.N., J.M.C., A.L.F., W.H.O., I.J.K., F.E.W., R.S., A.v.d.H. and J.A.C.R.; (3) critical revision: S.I.v.D., K.d.N., J.M.C., A.L.F., W.H.O., I.J.K., F.E.W., R.S., A.v.d.H. and J.A.C.R. All authors have approved the final article and agree to be accountable for all aspects of the work. Questions related to the accuracy or integrity of any part of the work will be appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was funded by the Innovational Research Incentives Scheme Vidi of the Netherlands Organisation for Scientific Research (grant number: 91717386, Dr. Rietjens) and by an EUR Fellowship of the Erasmus University Rotterdam (Dr. Rietjens).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.