
Abstract
Background:
Medical robots are increasingly used for a variety of applications in healthcare. Robots have mainly been used to support surgical procedures, and for a variety of assistive uses in dementia and elderly care. To date, there has been limited debate about the potential opportunities and risks of robotics in other areas of palliative, supportive and end-of-life care.
Aim:
The objective of this article is to examine the possible future impact of medical robotics on palliative, supportive care and end-of-life care. Specifically, we will discuss the strengths, weaknesses, opportunities and threats (SWOT) of this technology.
Methods:
A SWOT analysis to understand the strengths, weaknesses, opportunities and threats of robotic technology in palliative and supportive care.
Results:
The opportunities of robotics in palliative, supportive and end-of-life care include a number of assistive, therapeutic, social and educational uses. However, there are a number of technical, societal, economic and ethical factors which need to be considered to ensure meaningful use of this technology in palliative care.
Conclusion:
Robotics could have a number of potential applications in palliative, supportive and end-of-life care. Future work should evaluate the health-related, economic, societal and ethical implications of using this technology. There is a need for collaborative research to establish use-cases and inform policy, to ensure the appropriate use (or non-use) of robots for people with serious illness.
Medical robots have mainly been used to support surgical procedures and for a variety of assistive uses in dementia and elderly care.
There has been limited debate about the potential opportunities and risks of robotics in other areas of palliative, supportive and end-of-life care.
The potential opportunities of robotics in palliative, supportive and end-of-life care include a number of assistive, therapeutic, social and educational uses.
There is concern that robots will exacerbate healthcare inequalities, disrupt the workforce and reduce face-to-face human interaction.
Future work should evaluate the health-related, economic, societal and ethical implications of using robotic technology in palliative, supportive and end-of-life care.
There is a need for collaborative research to establish use-cases and policy recommendations to guide the appropriate use of robots for people with serious illness.
Background
A robot is ‘a reprogrammable, multi-functional manipulator designed to move materials, parts, tools, or other specialised devices through various programmed motions for the performance of a variety of tasks’. 1 Medical robots are increasingly used for a variety of applications in clinical medicine1–4 such as laparoscopic surgery, 5 surgical training,6,7 rehabilitation8,9 and assistive personal care.10,11 Furthermore, robots have been used for non-patient-orientated purposes, such as medical cleaning, automated medication delivery and transport of equipment.1,12 Robots have also been used for a variety of assistive uses in dementia and elderly care13–16; however, to date, there is limited debate about the potential opportunities and risks of robotics specifically related to palliative, supportive and end-of-life care.13–18 The global need for palliative care is increasing, 19 more purposeful use of healthcare robots has been proposed as solution for health services to meet the needs of an increasingly frail population. 20 Consequently, it is essential to evaluate the benefits and risks of the development and use of robotics in this area, to ensure future policy is informed by evidence.
Aim
This article examines the possible future impacts of medical robotics within palliative, supportive and end-of-life care. Specifically, we will discuss the strengths, weaknesses, opportunities and threats (SWOT) of this technology.
Method
A SWOT analysis was undertaken to understand the strengths, weaknesses, opportunities and threats of robotic technology in palliative, supportive and end-of-life care. A SWOT approach was chosen for its ability to provide a wide narrative overview of the subject. A systematic review was not considered for the following reasons. First, there are relatively few published papers specifically about the use of robots in palliative and end-of-life care. Second, there is great heterogeneity in the published work about healthcare robotics, involving different study designs and outcome measures (e.g. social vs assistive robotics). Therefore, most meaningful analyses will likely be derived from narrow systematic reviews, which focus on specific applications of robotics in palliative care. We therefore chose the SWOT approach to provide an overview of robotics in this area. This will support the conduct of focused systematic reviews to further explore the areas identified by this SWOT analysis.
SWOT development
Potential applications of robots in palliative care were imagined through discussion and debate, through meetings between computer scientists (T.R.P. and B.S.), a palliative care researcher (S.M.) and a clinician in palliative care (A.C.N.). A protocol was developed to explore the capabilities of a robot to exhibit human emotional responses (see supplementary files). The robot was developed (by B.S. and T.R.P.) and was presented (by A.C.N.) at a series of events which aimed to imagine the future of healthcare. The opportunities and risks of using robots to support palliative care patients and their families, and the delivery of services were discussed. These events were
A public engagement debate with a multi-professional audience including computer scientists, academics, clinicians, social scientists, ethicists and members of the public (University of Liverpool). Data were generated via a group discussion where feedback was recorded via flip chart paper.
A computer science seminar attended by computer scientists, data experts and healthcare professionals (University of Liverpool). Data were generated via a group discussion where feedback was recorded via flip chart paper.
An oral presentation at a dedicated robotics session at an international palliative care conference (the Association for Palliative Medicine (APM) Annual Supportive & Palliative Care (ASP) conference, Belfast, 2017 21 ). Following the session, written feedback was recorded to summarise the questions, discussion and debate.
Data from these events were collated and categorised into the themes of strengths, weaknesses, opportunities and threats. The SWOT was further informed by a round table discussion at the Winter Forum of the Palliative Care Institute Liverpool, University of Liverpool. This is a multi-professional meeting involving researchers, healthcare professionals and public representatives. Forum attendees (approximately 50) were invited to participate in the round table discussion. A modified world café method 22 was used to answer the question ‘what are the strengths, weaknesses, opportunities and threats of robotic technology in palliative care?’ The procedure involved three 20-min rounds of conversation for rotating small groups seated around a table. A facilitator (A.C.N.) promoted discussion through open questions and a scribe (T.McG.) collected written notes. The brief was to discuss their opinions of the (1) strengths, (2) weaknesses, (3) opportunities and (4) threats of robotic technology in palliative care. In total, 15 individuals (5 lay representatives, 5 clinicians, 3 researchers and 2 nurses) voluntarily participated in the round table discussion. After completion of the group discussion, individuals were invited to share their insights with the rest of the forum attendees.
Results
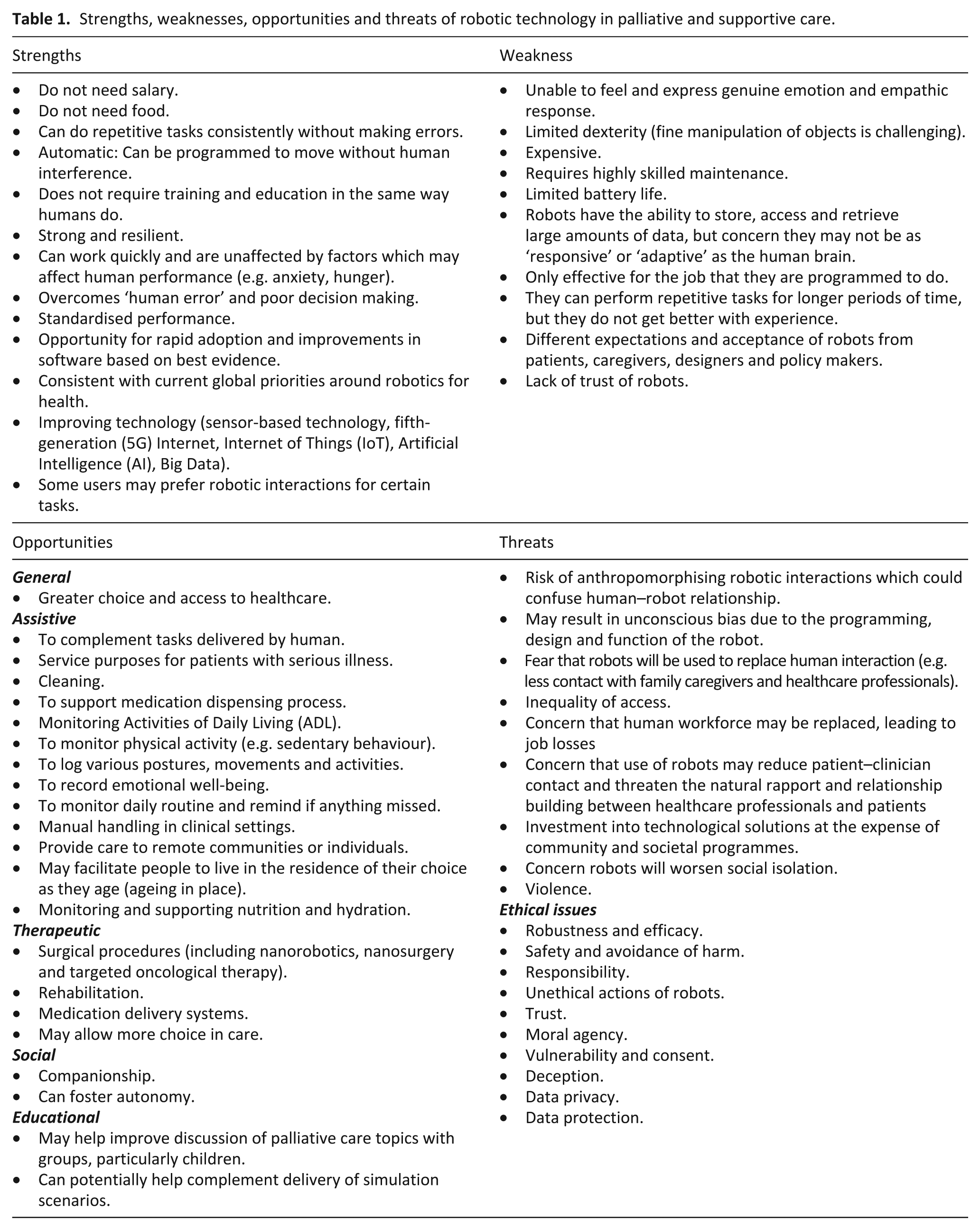
A summary of the SWOT analysis is presented in Table 1.
Strengths, weaknesses, opportunities and threats of robotic technology in palliative and supportive care.
Strengths of robotic technology
Robots can work automatically without human interference, meaning they can undertake time-saving tasks. 23 They are useful in environments that are hazardous for humans (e.g. ionising radiation or airborne diseases). 24 Furthermore, a robot can be standardised to ensure consistent, error-free performance, which is not affected by anxiety, fatigue and hunger. 1 Some individuals may prefer robot interactions for certain procedures, for example, for convenience (e.g. blood pressure monitoring) or to maintain privacy or avoid embarrassment (e.g. personal care). A robot does not require lengthy training or educational interventions which are necessary for human workers. For example, robots have the potential to rapidly incorporate software updates to improve performance based on best evidence, whereas for human workforces, adoption of new systems or changing practice is comparatively more challenging. Furthermore, continued technological developments will create further opportunities to integrate robotics in healthcare, for example, improvements in battery storage capacity, graphene,25,26 quantum computing, 27 fifth-generation (5G) Internet, 28 artificial intelligence (AI) 29 and Internet of things (IoT) technology. 30
Opportunities in palliative care
A general opportunity presented by robotics is to increase the choice and access of healthcare for patients. 11 Furthermore, current evidence suggests robotics can support a number of communication and assistive uses for the elderly. Such uses include applications for supporting mobility,31–34 activities of daily living,11,32–40 physical activity tracking/monitoring,34,41 medication management,37,40,42 and to support (and monitor) nutrition and hydration.32,40,43 For healthcare professionals, robots may improve the efficiency (and safety) of manual handling 44 and cleaning procedures.24,45 Robots can potentially support pharmacy processes by improving efficiency of medication dispensing.42,46
Therapeutic uses for robots include the potential to improve mobility following spinal procedures47,48 and to improve limb rehabilitation following stroke. 49 Minimally invasive robotic surgical procedures50–53 combined with nanorobotics (robots at the scale of a nanometre (10−9 m)) offers the potential to improve care for patients through nano-procedures (medical and surgical) which do not currently exist.54,55 Robots can potentially provide companionship in advanced illness. For example, elderly patients with dementia have been shown to gain therapeutic benefit from using a robotic seal (Paro) as a social companion.56,57 Paro may also help older adults without cognitive limitations58,59; however, those with severe mental impairment are unlikely to benefit. 60
Robots also have the potential to support educational initiatives. For example, in Japan, robots have been used to support health education programmes. 61 Previous studies have demonstrated that social robotics can benefit language and social development in autistic children, 62 presenting an opportunity for robots to facilitate education in wider society to promote better understanding of palliative care. Robots also have the potential to support palliative care training for healthcare professionals by creating immersive learning environments through the use of virtual reality. 63 In addition, robots may enhance high-fidelity patient simulation (HPS) by improving the functional ability of the manikin to exhibit emotion, move and respond to the learner. 64
Weaknesses
Robots are expensive and require supporting infrastructure to function (e.g. Internet connection, power supply and maintenance). Consequently, the technology is currently best suited to affluent healthcare organisations. Issues regarding infection control currently limit the practicality of using robots in some healthcare environments. 65 Robots can only do tasks they are programmed to do; therefore, they are suited for specific tasks but are less useful for problem solving. 2 Robots generally struggle with fine motor activities which reduces their usefulness for dextrous tasks like dressing, cooking and opening doors. 66 Robots can perform repetitive tasks for long periods of time but do not get better with experience (unless this is part of their programming). Robots are unable to feel and express genuine emotion which may reduce emotional connection and contribute to fear and distrust.2,38,67,68 The expectations and acceptance of robots are likely to differ between patients, caregivers, designers and policy makers. It is therefore important to determine whether individuals want (and will accept) this technology in their lives.43,44,69
Threats
Robots may widen inequalities in society, as certain individuals and organisations may have no access to this technology. Furthermore, there is a risk that robots may propagate unconscious bias. Evidence demonstrates that the individuals involved in the development and testing of data-driven technologies are generally small and homogeneous; therefore, there is a risk that the technology may not represent the needs of wider society. 70 Consequently, robotic systems may have implicit perceived social norms which may result in unintended consequences. 71 It is feared that robots will replace human contact and will cause job losses, leading to decreased patient-contact with healthcare professionals, and increased social isolation of the elderly.67,68 Such fears have resulted in violence against robots. 72 For public health, there is concern that technological investment will replace other societal initiatives. 68 A number of ethical issues also need to be considered.73–75 These include concerns about the robustness and efficacy of robots to ensure human safety. It is important to determine responsibility for robots and their software, (particularly if the devices fail) to prevent breeches of data protection and confidentiality. Furthermore, this raises questions of whether robots should always follow the instruction of their masters, even if the intended actions are unlawful or harmful (e.g. facilitating use of illicit substances, euthanasia, alcohol consumption, etc.). A robot that chooses (or is programmed) to disobey its master for a particular reason (e.g. to avoid harm) may lose the trust of the operator. These issues emphasise the moral agency of robots, particularly their use with vulnerable individuals with serious illness. In addition, the use (or continued use) of robots in those who lose capacity needs further evaluation (to determine best interests) and debate around other important questions such as whether using robots as social companions (e.g. animal substitutes in dementia) is deceptive. There is also an increased threat to data privacy and protection as robots are likely to access, record and generate a large amount of personal data which could be used without the consent of the individual. 76
Discussion
Main findings and new knowledge
This article discusses the potential strengths, weaknesses, opportunities and threats (SWOT analysis) of robotic technology in palliative, supportive and end-of-life care. This narrative overview highlights opportunities for the future role of robotics in a variety of assistive, therapeutic, social and educational uses in palliative, supportive and end-of-life care. Identified threats highlighted by this article include the risk of greater social inequalities, increased social isolation, inherent unconscious bias, reduced human contact, job losses and a deleterious impact on public health.
How this work relates to current developments
There is a lack of studies which specifically examine the potential of robotics in palliative care; however, our discussion supports work from other disciplines that outline the potential of robotics in healthcare. It is important to note the political importance of healthcare robotics. For example, China is ageing more rapidly than almost any country in recent history. 77 Currently, investment in healthcare robots is a priority for the Chinese government, who hope that robots will support economic growth. 78 Although population ageing is a global challenge, it is important to acknowledge that China’s experience may not translate to other areas due to cultural, infrastructural and political differences. A notable theme throughout this article is the association between robotics and public health. There is concern that robotics will exacerbate health inequalities, disrupt the workforce and reduce face-to-face human interaction. Our discussion highlights the importance of evaluating the health-related, economic, societal and ethical implications of using technology in palliative, supportive and end-of-life care. Future forecasting needs to consider how robots will interface with other related disciplines, such as architecture, transportation and public services.
Limitations
There are a number of limitations of this analysis. First, a SWOT analysis is limited by a degree of subjectivity and a lack of ability to clearly forecast the future. This SWOT analysis does not include non-English articles. Because China drives much of the innovation in healthcare robotics, it is likely that relevant data were excluded from this article. This analysis is not a systematic review; therefore, it is possible that important data were not included. We are unable to provide conclusions about the usefulness, efficacy or effectiveness of a robot in palliative, supportive and end-of-life care.
Future opportunities and research possibilities
This article provides a foundation for future systematic reviews to study specific areas arising from this SWOT analysis. Future research should identify use-cases (a list of actions or event steps typically defining the interactions between a role and a system, in order to achieve a goal 79 ) for robots in palliative care. Broadly, these relate to assistive, therapeutic, social and education purposes. Research should evaluate how human factors (e.g. culture, gender and age) can influence perception, acceptance and use of robotic systems. Studies can explore opportunities to use Big Data and Artificial Intelligence in combination with robotic systems in palliative care. 76 As a priority, researchers should evaluate the long-term public health, societal, ethical and economic implications of this technology.
Conclusion
Robotics may have a number of potential applications in palliative, supportive and end-of-life care. It is imperative that future work evaluates the health-related, economic, societal and ethical implications of using this technology. There is a need for collaborative research to establish use-cases and inform policy to ensure appropriate use of robotics for people with serious illness.
Supplemental Material
857628_supp_mat – Supplemental material for Robotic technology for palliative and supportive care: Strengths, weaknesses, opportunities and threats
Supplemental material, 857628_supp_mat for Robotic technology for palliative and supportive care: Strengths, weaknesses, opportunities and threats by Amara Callistus Nwosu, Bethany Sturgeon, Tamsin McGlinchey, Christian DG Goodwin, Ardhendu Behera, Stephen Mason, Sarah Stanley and Terry R Payne in Palliative Medicine
Supplemental Material
857628_supp_mat_table – Supplemental material for Robotic technology for palliative and supportive care: Strengths, weaknesses, opportunities and threats
Supplemental material, 857628_supp_mat_table for Robotic technology for palliative and supportive care: Strengths, weaknesses, opportunities and threats by Amara Callistus Nwosu, Bethany Sturgeon, Tamsin McGlinchey, Christian DG Goodwin, Ardhendu Behera, Stephen Mason, Sarah Stanley and Terry R Payne in Palliative Medicine
Footnotes
Acknowledgements
Amara Nwosu and Sarah Stanley’s hospice posts are supported by Marie Curie. Amara Nwosu and Sarah Stanley’s academic posts are supported by the National Institute for Health Research (NIHR) North West Coast–Clinical Research Network (CRN).
Author contributions
The author’s responsibilities were as follows: Project design: A.C.N., S.M. and T.R.P. Data collection: A.C.N. and T.McG. Robot programming: B.S. and T.R.P. Paper writing: A.C.N., T.McG. and C.D.G.G. Critique and review of the final manuscript: A.C.N., B.S., T.McG., S.M, C.D.G.G., A.B., S.S. and T.R.P.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
This project did not constitute research. Therefore, ethics committee approval was not required.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.