
Abstract
Background:
Advance care planning in dementia does not always happen. As dementia progresses, decisions are often left for family carers to make with professionals.
Aim:
To test the feasibility and acceptability of the delivery and use of a decision aid for family carers of people with severe dementia or towards the end-of-life.
Design:
Feasibility study using a before-after design of a paper-based decision aid with family carers of people with severe dementia or towards the end-of-life. Criteria for whether to progress to full evaluation included achieving: 70% recruitment rate of target of 30 people, and retention of 70% at 6 months. Outcome measures at baseline, 3 and 6 months, included: the Decisional Conflict Scale (DCS), Kessler Psychological Distress Scale (K10), EQ5D-5L and Satisfaction with Care at the End of Life (SWC-EOLD).
Participants:
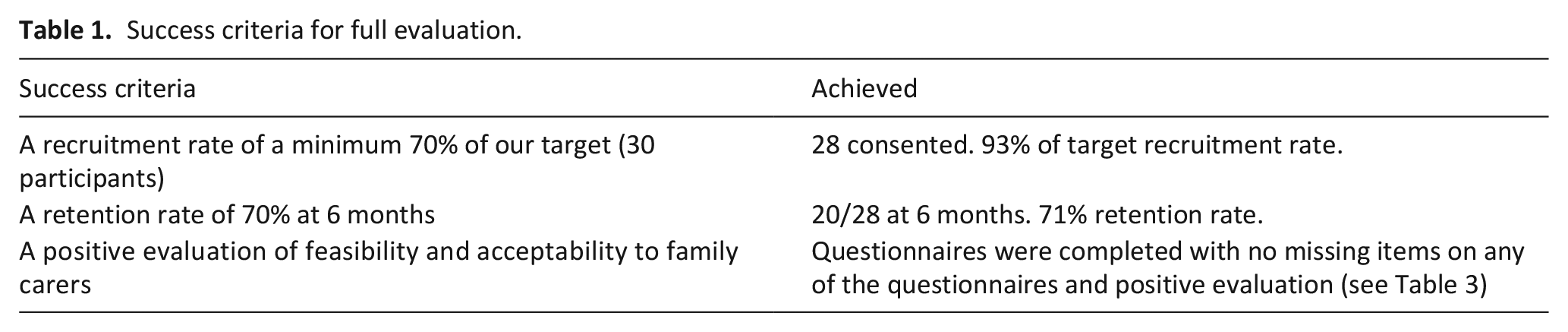
Twenty-eight family carers were recruited (93% of target), 26 completed baseline assessment and 20 (71%) of those were followed-up at 6 months.
Results:
Almost all outcomes changed indicating improvement over 6 months. The DCS and K10 scores decreased indicating less decisional conflict and less psychological distress. The decision aid was acceptable, 25% found it very helpful and 55% a little helpful at 6 months.
Conclusion:
We met the success criteria demonstrating this study was feasible and acceptable to carers. Future research should test the effectiveness of the decision aid in a full scale evaluation.
Advance care planning does not always happen with people living with dementia and as dementia progresses they are less able to participate in decision making.
Family carers find making decisions emotional and difficult, especially decisions about end-of-life care.
There are a lack of decision aids which focus on more than one decision in dementia care.
A decision aid with multiple decisions in dementia care is acceptable to family carers.
It is feasible to test a decision aid for family carers of people living with severe dementia or towards the end-of-life, including being able to recruit and retain participants over 6 months.
A full-scale evaluation of this decision aid is warranted to evaluate effectiveness.
Introduction
Despite efforts to increase advance care planning for people with dementia, 1 this does not always happen. 2 As dementia progresses, people with dementia are less likely and able to be involved in making decisions. 3 In the UK the Mental Capacity Act states decisions about those who lack capacity must be made in the person’s best interest. 4 Decisions may include decisions about everyday wellbeing, moving to a care home, or even some end-of-life decisions with professionals about starting or stopping medical treatments.5,6 Carers often feel responsible for making decisions,5,7,8 and find decision making difficult and emotional, 9 especially decisions about end-of-life care. 5
Family carers may benefit from support in making decisions.8,10,11 Decision aids are effective to support decision making among patients and family carers including improving patient knowledge and expectations.12,13 Decision aids explicitly state the decision, provide information about the decision and summarise options along with associated benefits and harms. 12
Existing dementia care decision aids either focus on single decisions such as place of care, or topics such as goals of care which can encompass several broad decisions about care.14,15 When caring for someone with dementia towards end-of-life, family carers are often faced with multiple, interrelated decisions. 14 There is a need for a decision aid which covers this variety of decisions and topics including, specifically, place of care, as well as broader decisions about care approaches, considering the complexities faced by carers towards the end of life. We developed a decision aid to support family carers making decisions on behalf of the person with severe dementia or those towards the end-of-life, covering multiple decisions. 16
Aims
To test the feasibility and acceptability of delivering and use of a decision aid for family carers of people with severe dementia or those towards the end-of-life.
Methods
Design
Six-month feasibility study using a before-after design with a target of 30 family carers, reported using the CONSORT 2010 statement extension for pilot and feasibility studies. 17
The decision aid intervention
A paper-based decision aid for family carers providing care for someone with severe dementia or those towards the end-of-life living at home or in a nursing home. The decision aid includes four key decision topics: (1) changes in care; (2) eating and drinking difficulties; (3) everyday well-being and (4) healthcare, tests and medication. Carers can record their preference for these decisions. Detailed information on the co-design of the decision aid and content are published separately. 16
Sample and recruitment
Family carers of people with severe dementia or towards the end-of-life were recruited between April 2020 and October 2020 through:
(1) Local and national dementia, carer, palliative care, research and professional networks;
(2) NIHR Join Dementia Research (JDR): an online dementia research registry;
(3) Social media.
Interested potential participants were asked to respond using any means of communication to either the research team or the inviting organisation.
Our protocol also included recruitment via NHS hospital trusts and nursing homes. However, the study commenced in April 2020 and due to Covid-19 we did not recruit via these sites.
Inclusion criteria
Family carers:
Family member or friend over the age of 18 years who identified as a carer/main decision maker for someone with severe dementia or towards the end-of-life who lives at home in the community or in a nursing home;
Able to provide informed consent;
Able to read and speak English.
The person with dementia being cared for had to:
Be over the age of 65 years;
Have a clinical diagnosis of any type of dementia as categorised in ICD-11 (informed by clinical record or family carer);
Judged by the research or clinical team to be towards the end-of-life, have severe dementia or live in a nursing home.
End-of-life is difficult to predict and define in dementia, 18 we therefore devised a broad overview of the characteristics of someone with dementia who may be towards end-of-life. These were pragmatically informed by the Clinical Dementia Rating (CDR) score of 3 for severe dementia. 19 Not everyone who is towards the end-of-life may have severe dementia and may not experience the symptoms listed below. A clinical judgement was made by clinical team members about the stage of dementia and not by formal rating. Someone with dementia towards the end-of-life is likely be to be physically frail and experience repeated instances of illness. We considered a combination of two or more of these as an indication that someone with dementia may be near the end-of-life:
Severe memory loss;
Unable to make judgements or solve problems including an inability to communicate;
Increasing frailty and reduced mobility, becoming bed bound;
Recurrent episodes of infections (i.e. chest infections);
Recurrence of bed sores;
Eating less, swallowing difficulties and loss of weight;
Bedbound;
Frequent incontinence;
Requires much help with personal care;
Other severe or life limiting illness (i.e. cancer or lung disease).19,20
Exclusion criteria
Family carers who had a cognitive impairment themselves;
Family carers not living in the UK
Sample size calculation
No formal sample size calculation was undertaken, as this is a feasibility study. Numbers were chosen on pragmatic grounds to demonstrate feasibility of recruitment, acceptance of the intervention and retention. We aimed to recruit 30 carers, and assuming 14% attrition anticipated that 26 participants would complete the study. About 14% attrition is based on similar studies of people with dementia towards the end-of-life.21,22
Ethical approval and consent
London – Queen Square Research Ethics Committee and Heath Research Authority approved the study March 2020 (20/LO/0210). We collected written or recorded verbal consent.
Measures
A research assistant completed baseline assessments and follow-up assessments at 3 and 6 months via telephone. Measures included:
Decisional Conflict Scale (DCS): to evaluate the quality of a decision about care. 23
Kessler Psychological Distress Scale 10 (K-10): providing a global measure of distress. 24
Satisfaction with Care at the End of Life (SWC-EOLD). 25
Carers Quality of Life measured using EQ-5D-5L, EuroQol. 26
We used the DCS twice per assessment: (1) participants were asked to answer the question reflecting on one decision (single decision) included in the decision aid they had made and (2) participants were asked to reflect on all decisions they were currently making (all decisions).
We collected data on the acceptability of being involved in the study including assessment length, helpfulness of the study and any distress caused.
Analysis
Data analysis was descriptive. Summary measures are presented for the baseline characteristics as mean and standard deviations for continuous variables and frequencies and percentages for categorial variables. The summary results are based on observed observations only. We estimated changes in pre- and post-intervention scores (with confidence intervals). We pre-defined success criteria for determining whether it is appropriate to progress to a full evaluation (see Table 1).
Success criteria for full evaluation.
Results
Sample
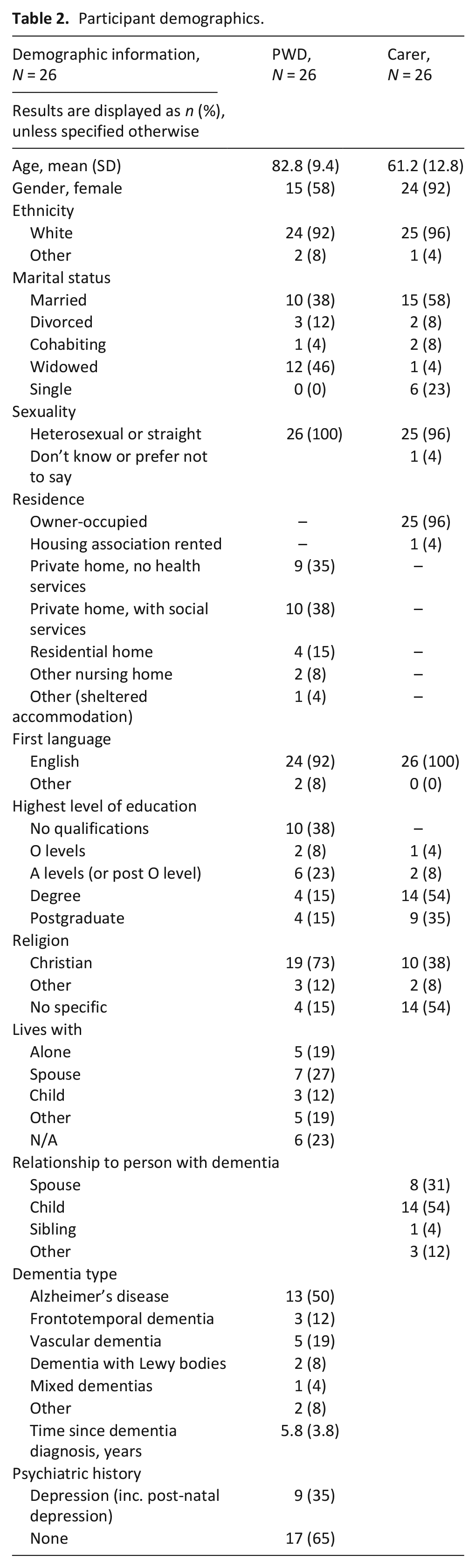
Twenty-eight participants (see Table 2) from a target of 30 (93% of target) consented to be part of the study. Figure 1 shows flow of participants which includes reasons for withdrawal.
Participant demographics.
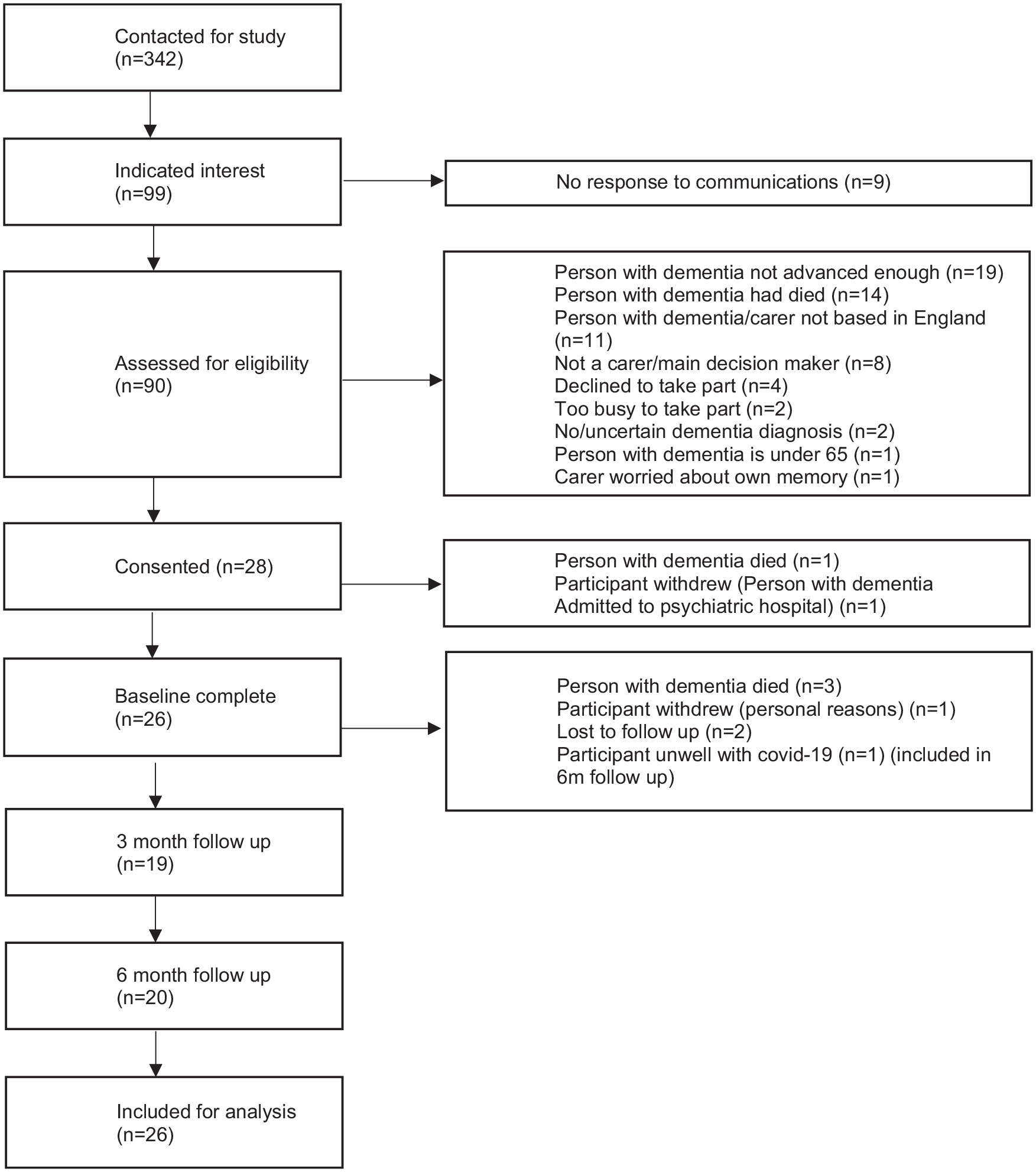
Flow chart of study participants.
Acceptability
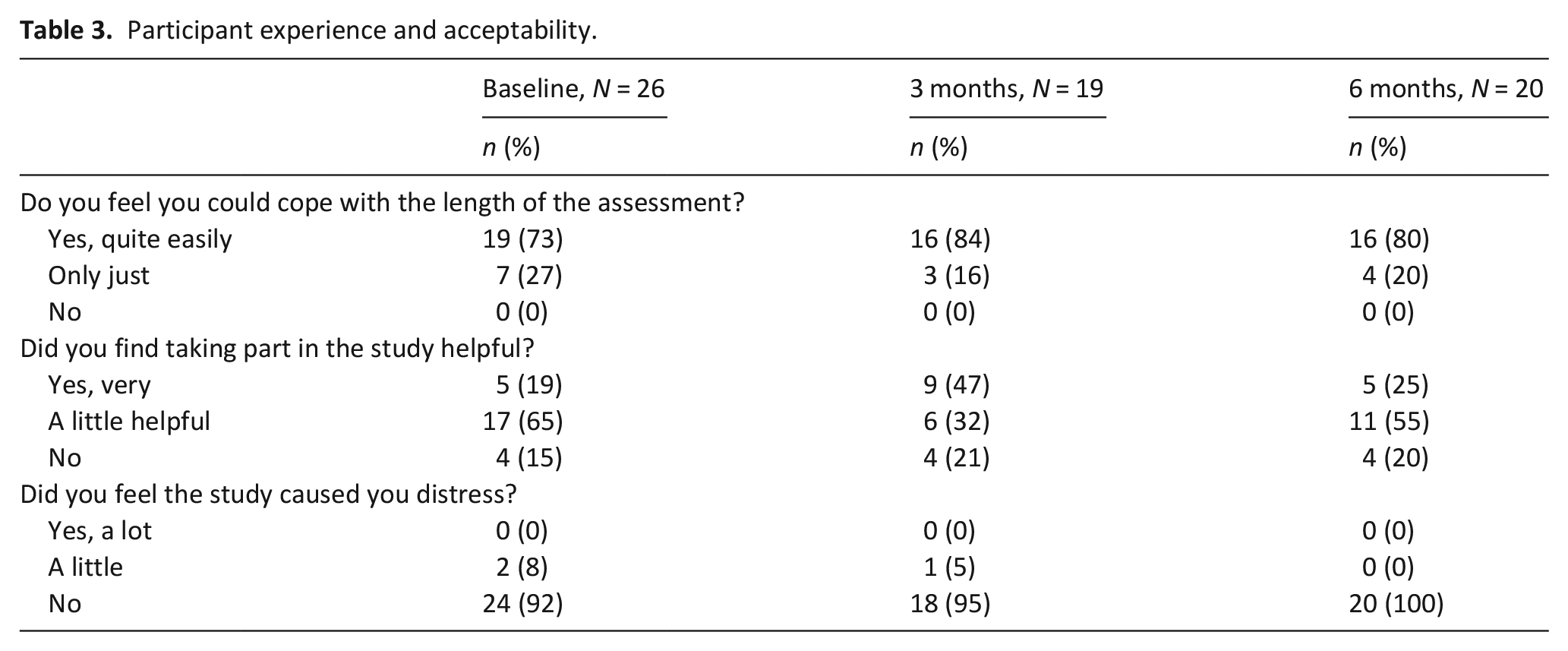
No participants felt the study caused ‘significant distress’. Only two participants at baseline and 1 at 3 months found it a ‘little distressing’. None were distressed at 6 months (See Table 3). At 6 months 25% reported they found it very helpful and 55% a little helpful. Detailed acceptability information was collected from semi-structured qualitative interviews and is reported separately.
Participant experience and acceptability.
Outcomes measures
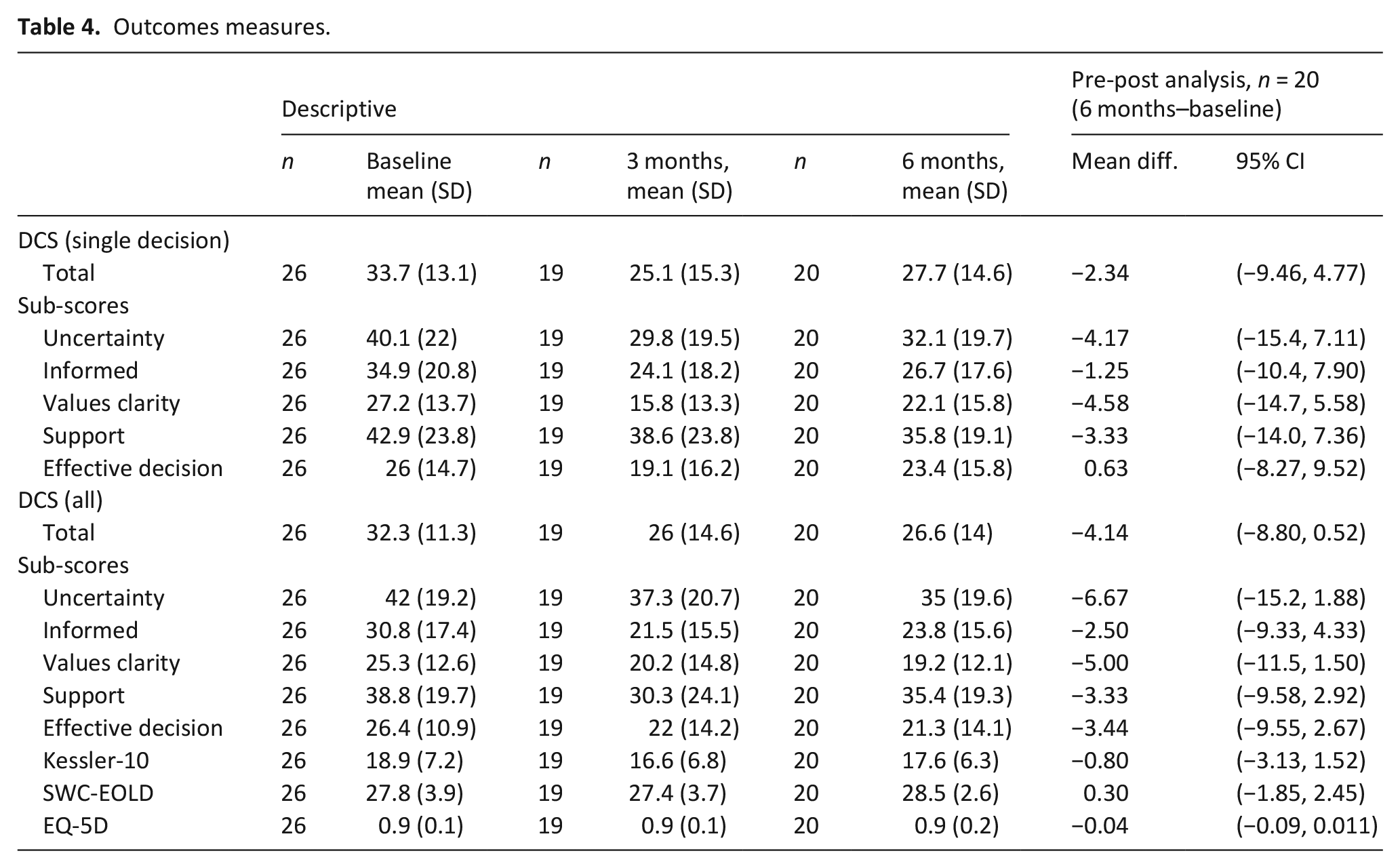
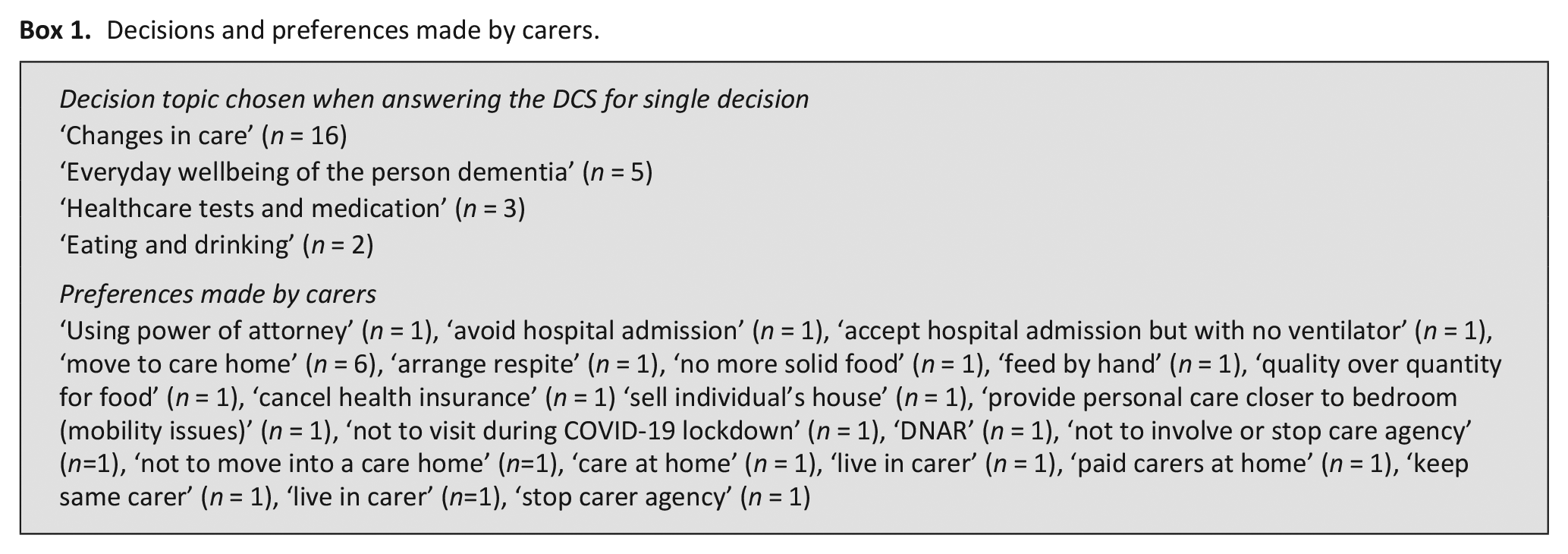
Scores across all outcome measures can be seen in Table 4, improvements were recorded in decisional conflict, distress and satisfaction with care, but not in quality of life. See Box 1 for the decision topics participants selected and the preference they reported for these decisions when answering the DCS for a single decision.
Outcomes measures.
Decisions and preferences made by carers.
DCS (Decisional Conflict Scale) range 0–100, higher score indicates high decisional conflict; Kessler 10: range 10–50, higher scores indicate a higher level of psychological distress; SWC-EOLD (satisfaction with care end-of-life dementia), range 10–40, higher scores indicating more satisfaction; EQ-5D, range 0–1, higher scores indicate better health.
Discussion
Main findings
We demonstrated our intervention is feasible and acceptable to family carers supporting someone with severe dementia or towards end-of-life. This was a feasibility study so not powered to report effectiveness, but results indicated that decisional conflict reduced post intervention for both individual decisions (standardised effect size 0.6) and when asked to consider all the decisions they had made (standardised effect size 1.7). These are larger than the meaningful difference of 0.3–0.4. recommended in the DCS manual. This suggests the decision aid supported participants’ confidence and certainty about making decisions. Measures of distress and satisfaction with care also improved.
Our results support previous studies which have demonstrated similar effects when using decision aids to support family carers of people living with dementia make specific decisions, 14 but also suggest decision aids are able to cover more than one topic.
Many potential participants were keen to participate but did not meet the eligibility criteria of end-of-life or severe dementia. Future evaluation could widen the inclusion criteria to include all stages of dementia where carers feel they are contributing to decision making.
What this study adds Meeting the success criteria supports a larger fully powered evaluation of the decision aid using the outcomes from this study. The decision aid has the potential to support planning for palliative care but also real-time decisions about palliative care. The DCS may not be best suited for this decision aid covering multiple topics and decisions. The DCS is designed to focus on single decisions, however participants in this study were considering multiple decisions with multiple potential options/preferences. We therefore measured the DCS both on a single decision participants made (based on their choice, see Box 1), as well as separately to record their experiences of general decision making. Future work should explore the use of the DCS or similar measure to cover multiple decisions.
Strengths and limitations
Most participants were white, a larger evaluation study would need to increase sample diversity and ensure underserved populations are included. Using online recruitment methods meant we were able to broaden the geographical scope, ensuring we were not limited to participants in highly researched areas such as London, but may still have excluded some people. A detailed qualitative evaluation will be published separately. Convenience sampling due to the covid pandemic meant most participants had already made some of the decisions in the decision aid and used the aid to reflect on decisions and plan for future decisions. If we had recruited via the NHS or care homes, we may have identified carers currently making decisions in the decision aid.
Conclusion
Our decision aid was feasible and acceptable to family carers. We were able to successfully recruit and follow up family carers over 6 months. A larger evaluation is warranted to test effectiveness of the decision aid.
Footnotes
Acknowledgements
We would like to thank all participants who agreed to take part in this study. We would like to thank members of Patient and Public Involvement group: Jane Ward, Frank Arrojo and Angela Baldock. Finally, we would like to thank members of the study steering committee and wider team: Prof Steve Iliffe, Dr Sarah Russell, Dr Andrew Thorns, Dr Kathryn Lord, Dr Anna Gola, Dr Karen Harrison-Dening, Dr Kirsten Moore, Prof Jill Manthorpe and Prof Kate Walters.
Description of authors’ roles
Davies designed the study, supervised data collection and analysis, and wrote the paper. Aker collected data and contributed to writing the paper. Vickerstaff designed the study, analysed the data and contributed to writing the paper. Sampson designed the study, supervised data collection and analysis, and contributed to writing the paper. Rait designed the study, supervised data collection and analysis, and contributed to writing the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclose receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Alzheimer’s Society (grant number AS-JF-16b-012).
Availability of data and material
All the relevant data are available. The method of data collection, analysis, and sample characteristics are reported in this article.
Ethics approval and consent to participate
The description regarding ethics approval is reported in this article.