
Abstract
Background:
Facilitating advance care planning with community-dwelling frail elders can be challenging. Notably, frail elders’ vulnerability to sudden deterioration leads to uncertainty in recognising the timing and focus of advance care planning conversations.
Aim:
To understand how advance care planning can be better implemented for community-dwelling frail elders and to develop a conceptual model to underpin intervention development.
Design:
A structured integrative review of relevant literature.
Data sources:
CINAHL, Embase, Ovid Medline, PsycINFO, Cochrane Library, and University of York Centre for Reviews and Dissemination. Further strategies included searching for policy and clinical documents, grey literature, and hand-searching reference lists. Literature was searched from 1990 until October 2018.
Results:
From 3043 potential papers, 42 were included. Twenty-nine were empirical, six expert commentaries, four service improvements, two guidelines and one theoretical. Analysis revealed nine themes: education and training, personal ability, models, recognising triggers, resources, conversations on death and dying, living day to day, personal beliefs and experience, and relationality.
Conclusion:
Implementing advance care planning for frail elders requires a system-wide approach, including providing relevant resources and clarifying responsibilities. Early engagement is key for frail elders, as is a shift from the current advance care planning model focussed on future ceilings of care to one that promotes living well now alongside planning for the future. The proposed conceptual model can be used as a starting point for professionals, organisations and policymakers looking to improve advance care planning for frail elders.
Keywords
Frail elders are projected to become one of the largest future users of palliative care.
Advance care planning can improve person-centred end-of-life care quality; however, it is relatively uncommon in frail elders due to multiple complex challenges.
Behaviour change models can be used to identify relevant behaviours to inform the development of advance care planning interventions.
Implementing advance care planning for frail elders requires a system-wide approach that recognises the importance of living well now, relationality and early engagement.
All stakeholders (frail elders, families and professionals) have educational needs around the impact of frailty on the life course and why advance care planning is relevant for frail elders.
The proposed conceptual model can be used as a starting point for professionals, organisations and policymakers looking to improve advance care planning for frail elders.
Frail elders need to be engaged early with advance care planning to give them the greatest chance to engage physically and cognitively, at their own pace, and make and revise decisions.
Reframing advance care planning as something that promotes living well now as well as planning for the future would relate more readily to frail elders’ daily lives.
Professionals need to be given the opportunity to develop the skills and competencies required to recognise, proactively use and create advance care planning facilitation opportunities throughout frail elders’ end-of-life trajectories.
Background
Frailty is a syndrome of ageing affecting around 10% of those aged above 65, 1 increasing to around 65% of those aged 90 and above. 2 Characterised by a progressive, gradual decline in physical, psychological and social functions, 3 frailty increases vulnerability to sudden deterioration4,5 and reduces recovery potential. 6 Compared to fit older people, those with frailty are at greater risk of disability, care home admission, hospitalisation and death.7,8 Frail elders are projected to become one of the largest users of palliative care services, 9 although currently frail elders are often not recognised as having palliative care needs. 10
Conversations about end-of-life care, or advance care planning (ACP), are promoted in many high-income countries as a strategy to improve end-of-life care.11–15 However, ACP is relatively uncommon in frail elders.16–18 Priorities are often not discussed prior to significant deteriorations 19 when frail elders are unlikely to be able to voice their preferences. 20 Lack of engagement is due to multiple complex challenges.16–18 These include uncertainty of prognostication, therefore recognising when to initiate ACP,21,22 misunderstandings around what ACP means, 23 and frail elders and their families not wanting to discuss death and dying because the topic feels taboo or challenges the frail elders’ coping strategies.24,25
One previous review explored ACP in community-dwelling frail elders. 19 Sharp et al.’s 2013 review, 19 set within general practice, found that most frail elders would value discussing ACP and that general practitioners recognised ACP as part of their professional responsibility. However, conversations often did not occur due to multiple time pressures and barriers. This integrative review aims to understand how ACP can be better implemented for community-dwelling frail elders (frail elders whose main residence is home or a long-term care facility) and for all relevant multidisciplinary professionals. The review underpins a larger study to develop an intervention to facilitate ACP in this population using the COM-B behaviour change model. The literature analysis is mapped to key stakeholder groups: frail elders; families, including friends and significant others; and professionals, including health and social care professionals.
Behaviour change theory
To develop an intervention that successfully influences behaviours to bring about sustained change requires an understanding of current behaviours. 26 This review uses the COM-B 27 behaviour change model as a conceptual framework to support the identification of necessary ACP behaviours. COM-B 27 argues that for a person to change and sustain a change in behaviour, three interlinking elements are required (Figure 1). Capability relates to the physical and psychological knowledge and skills required to engage in a behaviour. Opportunity relates to physical and social opportunities that exist independently from the individual, such as the environment, resources and interpersonal influences that facilitate a behaviour. Motivation relates to an individual’s psychological processes that automatically, or reflectively, direct or encourage the behaviour, including conscious, analytical decision-making and unconscious or habitual responses. COM-B was selected as it is designed to be comprehensive and pragmatic so that it can be used with all behaviours in diverse settings,28–32 links to the taxonomy of existing behaviour change theories, 33 and maps to the larger Behaviour Change Wheel, 34 thus supporting the translation of behaviour identification into behavioural interventions. 31
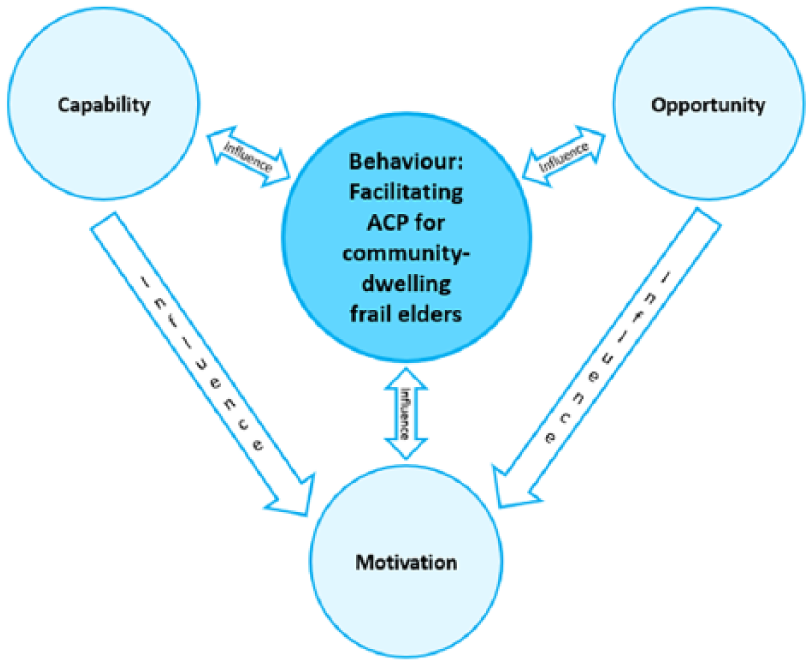
The interlinking elements of behaviour change as proposed by COM-B. 27
Method
Rationale
Whittemore and Knafl’s 35 systematic integrative review method enabled the synthesis of a wide range of experimental and non-experimental evidence from diverse sources36–39 including policy and theoretical documents alongside empirical studies. The narrative synthesis of findings enables a more comprehensive understanding of what is a complex, and at times nebulous, phenomenon. 39
Literature search
Multiple search methods were used (Supplementary Data 1). Search terms were developed and refined through a preliminary scoping review and by reviewing key words of relevant papers. The search strategy (Supplementary Data 2) was tailored to each database. Medical Subject Headings (MeSH) were used, where available, to efficiently identify the most relevant data, 40 alongside free-text synonyms and truncation. The Boolean term ‘OR’ was used to combine multiple terms within a concept and ‘AND’ to combine concepts. 41 The search, screening and selection, conducted by the first author (S.C.), were verified by the research team, and one author (C.J.N.) completed an independent screen of 10% of papers at both screening and selection stages. Following paper identification and de-duplication, titles and abstracts were screened, and full papers were assessed for eligibility guided by the inclusion criteria (Table 1).
Inclusion and exclusion criteria.
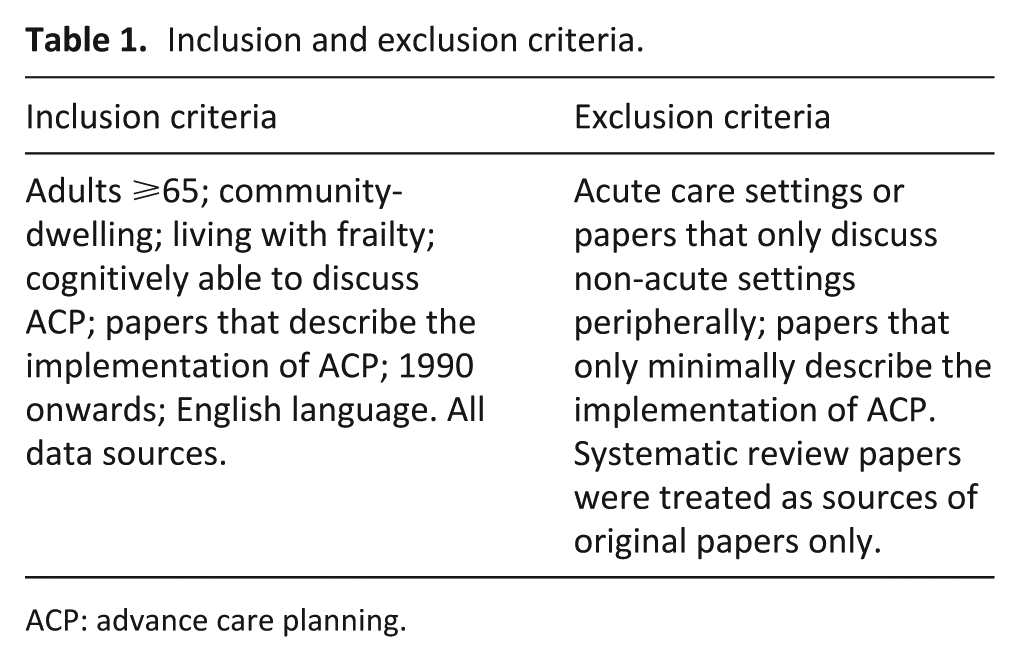
ACP: advance care planning.
Searches were limited to papers from 1990 when ACP first appeared in the literature 15 to October 2018, but not limited by source. The concept of, and process for, quality assessment is complex in integrative reviews with diverse sources, particularly when non-empirical sources are included. 35 The complexity of this review is increased as multiple conceptualisations of frailty and ACP exist internationally and over time. To ensure all relevant evidence was incorporated, papers were considered based on their relevance to the review’s aim, and so no quality appraisal was conducted. This enabled the inclusion of papers that discussed concepts in their broadest sense, for example, where authors described participants as frail, and residence in long-term care homes was used as a frailty proxy (Figure 2).
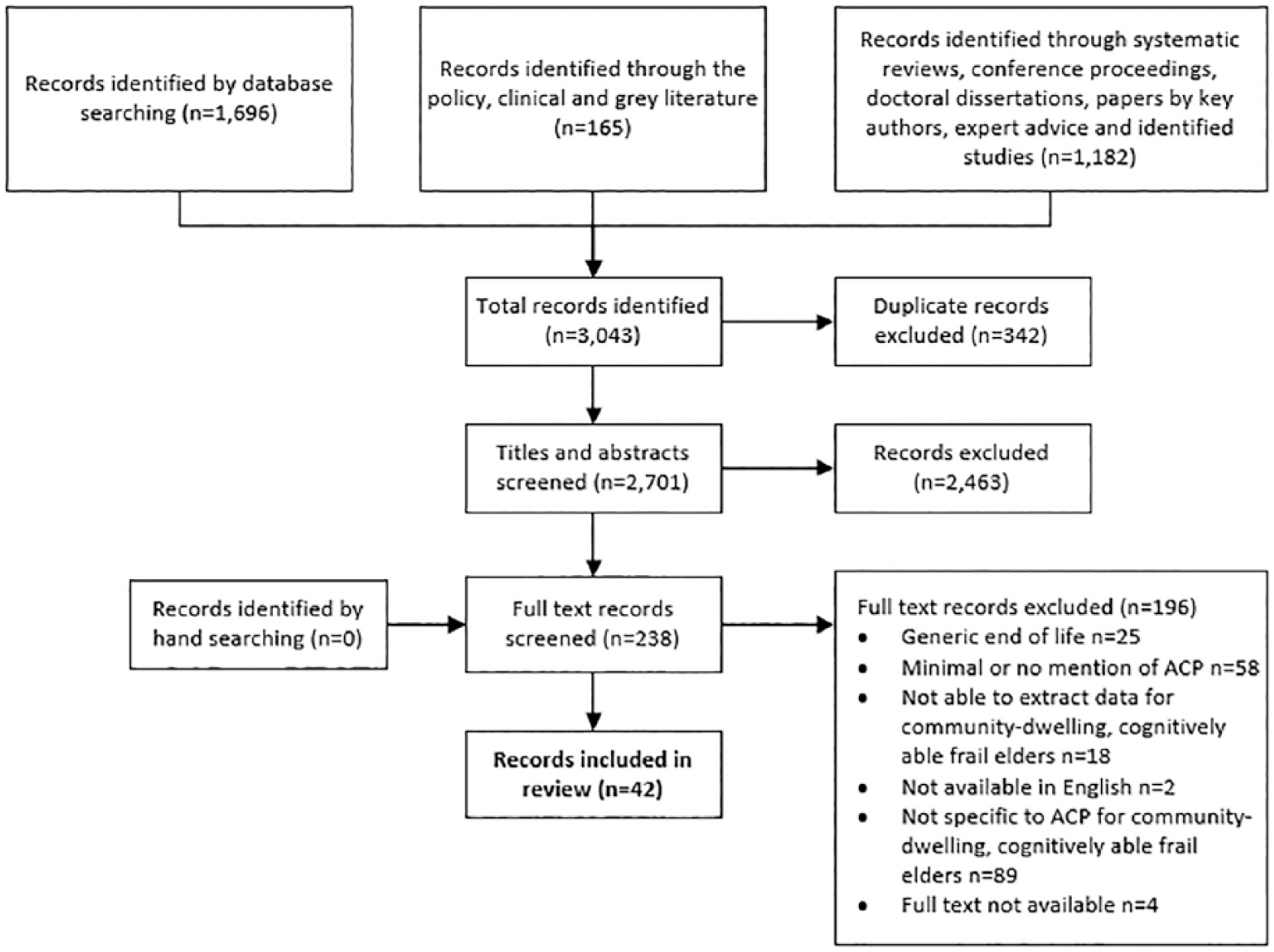
PRISMA: Flow of papers through the selection process.
Data analysis
This focussed on the identification and synthesis of attitudes to, and necessary behaviours for, implementing ACP with community-dwelling frail elders. COM-B 27 was used as a theoretical framework to inform analysis. Using the constant comparison method, 42 codes and subthemes iteratively emerged within the three COM-B elements of Capability, Opportunity and Motivation. 27 Codes were then mapped to the three stakeholder groups (frail elders, families and professionals) to better target behaviours and intervention strategies. Analysis was conducted by S.C. and discussed and reviewed with the research team throughout the process, with final themes agreed by consensus.
Findings
Overview
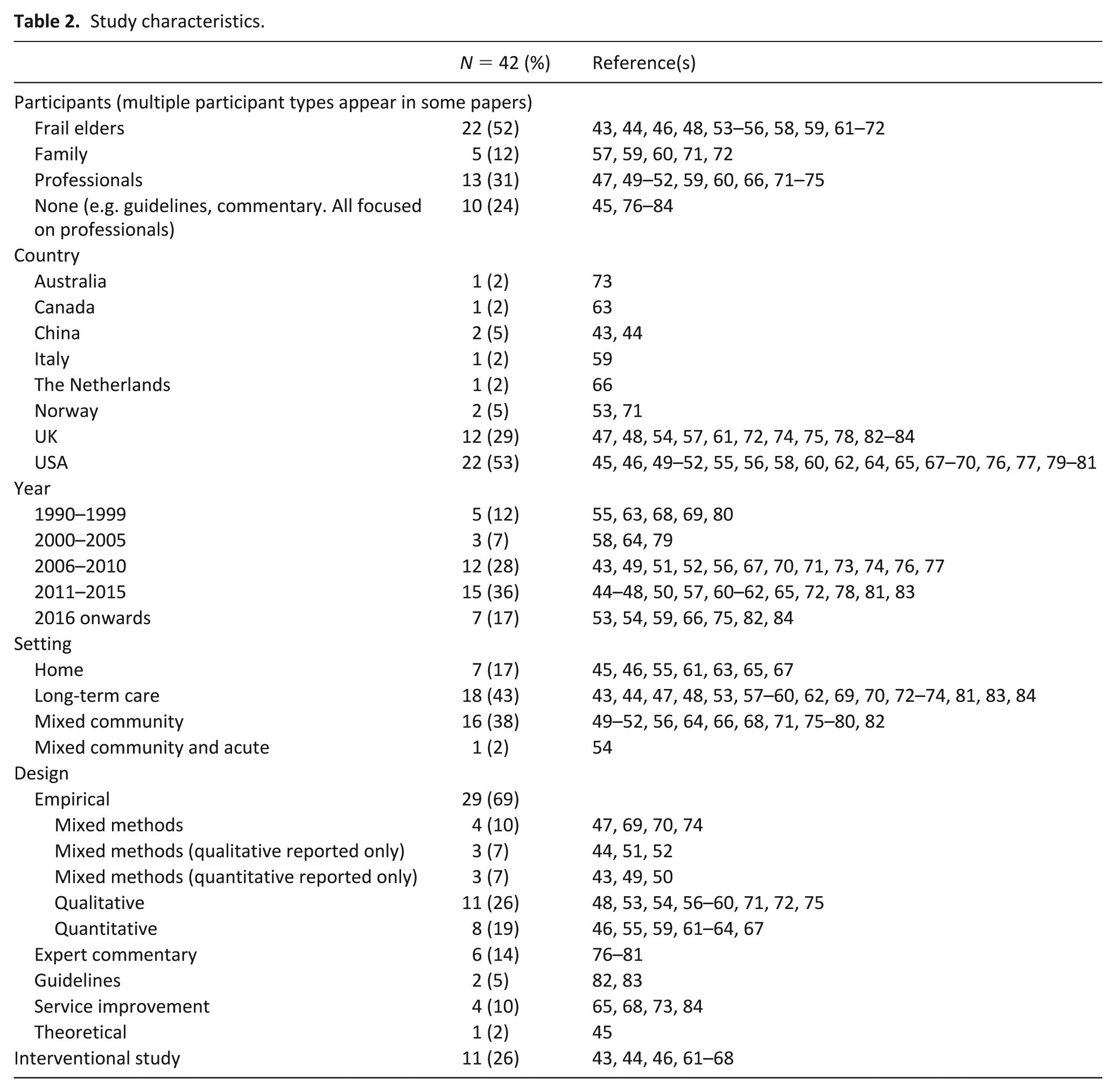
Forty-two papers were included. Ten papers discussed elements of five studies,43–52 leaving 37 unique records. Although 22 papers included frail elders as participants, only 10 focused on their views47,48,53–59 or those of family members;59,60 most focussed on professionals’ experiences and needs. The 29 empirical papers used a range of qualitative, quantitative and mixed methods, including interviews, focus groups, case studies, cohort design, record reviews, quasi-experimental, pilot and randomised controlled trials. Of the 33 empirical and service improvement papers, 11 discussed interventions (Supplementary Table 3). These included reactive case management, 61 storytelling incorporating reminiscence therapy,43,44 a video decision aid, 62 or versions of previously tested interventions: Let Me Decide, 63 PEACE (Promoting Effective Advance Care for Elders) 46 and Respecting Choices.64–66 The 42 papers are listed in Table 2.
Study characteristics.
The main behavioural components from the narrative synthesis are presented within the three COM-B themes in Table 3 and discussed below. Themes are interrelated, and while they are presented separately here for clarity, they should be considered holistically.
Attitudes and necessary behaviours for ACP in frail elders.
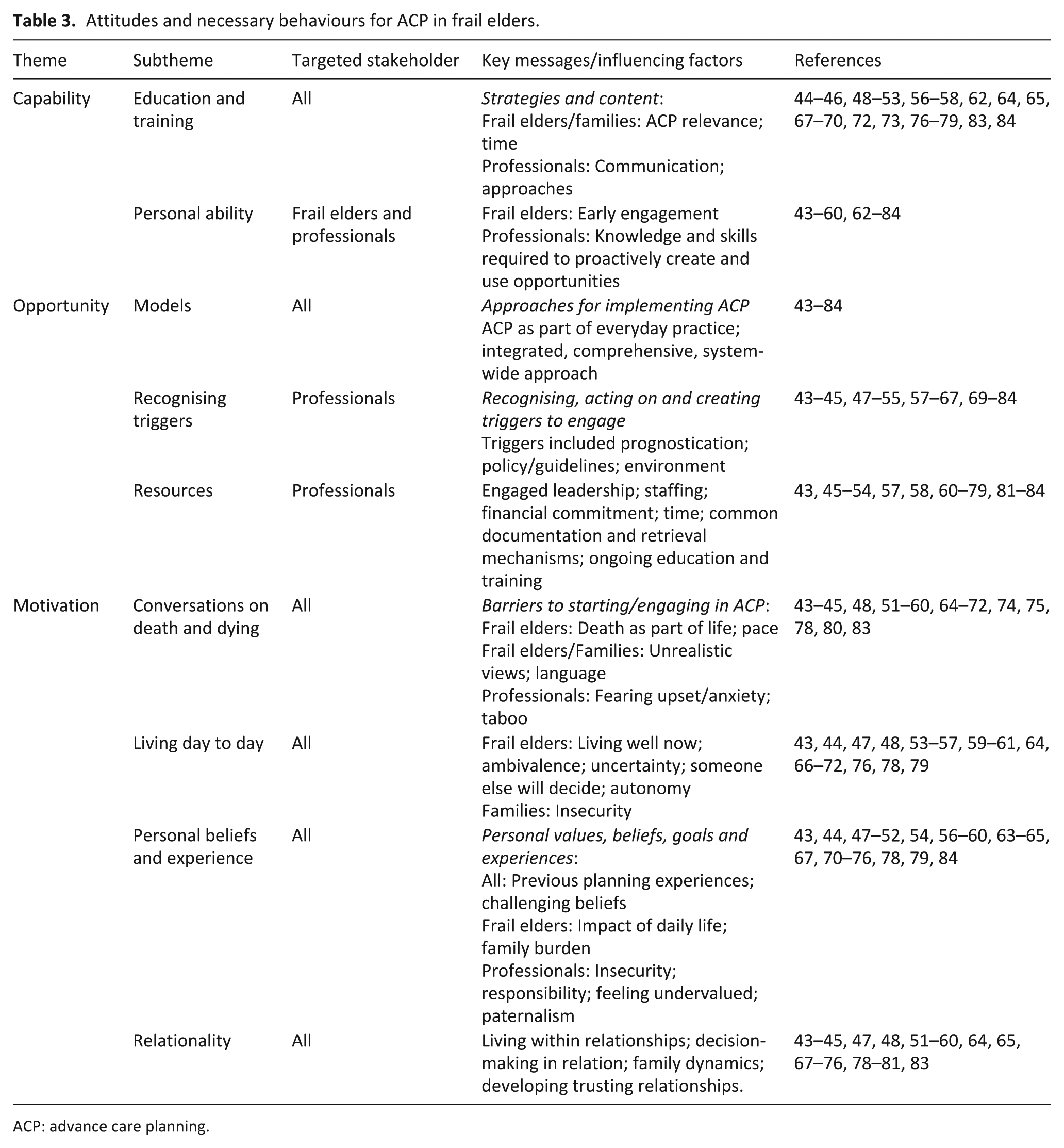
ACP: advance care planning.
Capability: physical and psychological capabilities that enable ACP engagement
Discussed by all but one paper, 61 this theme was the least nebulous of the three themes and is represented by two subthemes: (1) Education and training – packages to improve ACP engagement for all stakeholders, and (2) Personal ability – individual knowledge and skills to enable engagement with ACP.
Education and Training recommended multiple, diverse formal and informal education and training packages to support stakeholders to better understand, engage with and implement ACP. For frail elders and their families, this included education to improve understanding of ACP,44,64,69,72 how to complete documentation, 60 its relevance for frail elders 53 and their likely end-of-life trajectory.44,56,73 Time was recognised as important for education or training: time to understand necessary concepts and how they related to the frail elder, and time to make decisions.44,62,64,68,73 Strategies included making ACP part of routine practice,57,58,69,73,78 providing targeted materials,62,70 and preparing frail elders and families for potential future decision-making. 48 For professionals, educational packages focused on improving communication skills and their ability to sensitively engage frail elders with ACP.45,51,52,57,65,67,69,73,78,79,83,84 Various educational strategies were recommended, including role-play, online training, role modelling experts, and mentoring.49,50,72,73,84 Specific approaches were also discussed, including following a basic palliative approach,45,76,84 using core scripts,77,78 or attending formal programmes such as Respecting Choices.46,64
Personal ability related to both frail elders and professionals. For frail elders, it focussed on their physical and psychological ability to engage with ACP and how these would likely reduce with time.43,45,48–55,57–60,62–64,66,69–72,74–77,79–81,83 Abilities included difficulties reading and understanding documentation58,60 and remembering ACP decisions.59,60,66,70 The focus was on early engagement, prior to potential physical or cognitive deterioration43,45,48,51–55,57–60,62,64,66,71,72,74,75,77,79–81 where ‘… the person may already be too sick to interpret their treatment preferences’. 43 Early engagement meant ‘… meaningful plans could be put in place […] so that the patient’s quality of life could be enhanced …’ 80 and that decisions could be reassessed throughout the frail elders’ end-of-life trajectory.45,48,52,57–59,62–64,69,76,81,83 For professionals, personal ability related to the knowledge and skills they required to proactively use and create ACP opportunities. Recommendations ranged from needing a greater understanding of what ACP meant, 72 to the ability to address cultural, socio-demographic and educational influences, 76 answer existential questions, 65 help frail elders connect ACP with their own values and beliefs, 56 and cross-sectoral liaison. 73
Capability: key messages
Early engagement means frail elders are most likely to be able to engage with ACP. This is supported by ACP becoming part of everyday practice and the provision of targeted materials. In addition, all stakeholders require access to relevant ongoing education and training. For frail elders, this should focus on understanding what ACP means for them and their likely end-of-life trajectory. For professionals, the focus is on developing the knowledge and skills required to proactively create and use opportunities to engage frail elders in ACP throughout their end-of-life trajectory.
Opportunity: physical and social opportunities that facilitate ACP
This theme, discussed by all papers, regards the implementation and sustainability of ACP for frail elders. In addition to factors related to the stakeholders, it encompasses organisation and system influences and requirements. The theme represents three subthemes: (1) Models – approaches to implementing ACP; (2) Recognising triggers – the importance of professionals recognising and utilising ACP triggers; (3) Resources – the multiple and diverse resources required for professionals to implement ACP with frail elders.
Models related to the various recommended approaches for implementing ACP with frail elders. While it related to all stakeholders, recommendations focussed on professionals, organisations and systems. Several papers focussed on how ACP should be conducted,45,51,52,58,59,61,64,73,75,77,78,80 for example, conversations should be ‘… focussed and brief …’, 78 use open questions ‘what things are most important to you, now and in the future?’, 75 be held in conducive environments 64 and include after-death arrangements. 59 Other papers recommended specific approaches. The recommended palliative, holistic approach45,46,48,53,54,56,59,60,71,72,76,79 recognised the importance of relationality (discussed further in Motivation), promoted hope, and focussed on living well now rather than planning for dying and death.53,54,60,72,75 The storytelling approach included life therapy or using hypothetical scenarios and was promoted as a strategy to support frail elders to clarify their views and beliefs as regards end-of-life wishes.43,44,48,56,58,62,69 Integrated and comprehensive system-wide models were seen as important in facilitating ACP.43,45,53,54,60,64–66,70–75,78 Recommendations included developing and maintaining cross-sectoral relationships,47,59,75,84 ensuring key people, particularly families, were available,51,52,81 enabling documentation access,54,64,65,75 particularly during care transitions,60,70,81 and community-wide support and education.43,64,66,70,72,74,75 Almost two-thirds of papers suggested successful ACP necessitated a cross-sectoral, multidisciplinary approach,45,47,51–54,57,58,60,61,63–65,68–70,73–75,77,80–84 with the overall recommendation that ACP became ‘… woven into the fabric …’ 65 of everyday practice43,45,54,58,63,65,73,75,77–79,81 ‘… as normal as discussing smoking cessation’. 78
Recognising triggers related to professionals recognising, acting on and creating opportunities to engage frail elders.43,44,47,48,53,54,58–60,62,64,66,67,69–72,75,78,83 Triggers included recognising poor prognostic indicators,54,58,61,66,72,77,78,82,83 transitions, such as admission to homecare services,45,58,63,67 and environment, particularly living in long-term care,43,47,48,53,57–59,72–74,81 which ‘… allows for continuity of end-of-life care discussion …’ 43 Policy and guidelines that promoted ACP were also triggers,54,60,67,72–75,78,79,81,83 particularly when linked to funding or accreditation. 72 However, there were also multiple barriers. Frailty prognostication is difficult.47,48,60,75,78,80,83 The lack of a terminal diagnosis means frail elders ‘… are not identified as being, or do not see themselves as being, at the “end-of-life”’, 48 especially when they present with ‘… apparent wellness […] during initial consultations …’ 47 Opportunities provided by frail elders were also not always recognised, for example, when a frail elder ‘… refused a percutaneous endoscopic gastrostomy tube and had indicated that he wanted to die …’. 72 Furthermore, policies and guidelines regarding ACP responsibility were often unclear,47,51,52,65,71,73,78 not relevant to frail elders lives,48,54 could potentially undermine frail elders’ strategies ‘… to maintain positivity and motivation’, 54 and often focused on institutional admission with no motivation for ongoing review or relevance to those living in domestic settings. 67
Resources related to the multiple resources required for successful ACP implementation and sustainability, with most discussions including leadership, finance, staffing, time and documentation. Engaged leaders, from commissioners to colleagues, were recognised as important ACP drivers.48–50,53,63–65,72–74,78,84 This included supporting professionals to overcome ACP challenges,49,50,65,72–74,78,84 enabling resources including funding initiatives and training,46,47,49–53,57,64,72–74,84 and employing ‘… a critical mass …’ 73 of trained staff.43,45,46,54,61,68,71,73,76,78,79,83,84 Specific professional groups were promoted as ACP facilitators due to their knowledge, skills and responsibilities, for example, nurses,43,58,63 general practitioners,78,81,83 palliative specialists, 46 and social workers.51,52,76 Other papers suggested successful ACP required round-the-clock community-based exacerbation management teams.45,61,78 Time was discussed as a resource by over half the papers.43,46–53,57,58,63,64,67,69,70,72–75,77,78,81 For frail elders, this included time to get to know and trust professionals,48,51,52,57,58,68,69,83 and ‘… to make the decision, … get information’. 58 Professionals also required relationship-building time,51,52,58,76 and several papers46,48,51,52,63,70,73 recommended that organisations allocate staff ‘… the time and skills needed to realistically plan for the future’, 52 although this was often difficult due to competing priorities.47,49–52,64,67,72,74,78 Documentation and the process of completing it was discussed by almost two-thirds of papers.43,45,47,48,51–54,58,60–65,69,70,72–75,78,79,81–83 Most recommended ‘… common documents, a common storage and retrieval mechanism …’, 65 within and across care settings, including frail elders and their families.45,54,60–62,64,65,69,70,73,75,81–83 Document contents were also discussed by most authors,48,51,52,62,63,69,72,74,75,79,81–83 although there was lack of consensus around whether the document should focus solely on specific treatments69,79,81 or recognise personal goals.43,54,60,72,82
Opportunity: key messages
Frail elders are more likely to engage with ACP if it becomes part of everyday practice as part of an integrated, comprehensive, system-wide approach that occurs over time, rather than as a one-off event. Professionals need to recognise, act on, and create opportunities for frail elders to engage with ACP throughout their end-of-life trajectory. To enable this, professionals need support from engaged leaders within their organisations and the wider system, including the provision of all necessary resources such as staffing, finances, education and common documentation.
Motivation: psychological processes that encourage or direct individual ACP engagement
Discussed by all but four papers,46,62,77,82 this theme related to all stakeholders. It is represented by four closely related subthemes: (1) Conversations on death and dying – difficulties inherent in engaging with ACP conversations; (2) Living day to day – frail elders’ focus on living in the moment rather than planning for the future; (3) Personal beliefs and experience – how these influence ACP engagement; (4) Relationality – the impact of living within relationships.
The subtheme Conversations on death and dying, discussed by almost two-thirds of all papers, raised important barriers around starting conversations and engaging in informed decision-making.43–45,48,51–60,64–72,74,75,78,80,83 Frail elders and families held wide-ranging ACP views from rejection to full engagement,44,48,59,66 with many frail elders viewing death as part of life.43,44,53,55,69,72 While ACP had the potential to cause distress or make frail elders initially ‘… slightly uncomfortable …’, 53 most saw ACP as ‘… a welcome intervention …’, 59 as long as conversations were at the frail elder’s pace.48,59,66,68,83 For professionals, barriers included struggles discussing a taboo subject44,51–53,57,71,72 and fear of causing suffering or anxiety.43,53,55,57,67,69,71,72,75,80 Informed decision-making could also be challenging. Language could be confusing for frail elders and families, notably legal requirements, documentation54,58,60,64 and language around ACP, particularly what it meant,45,58,59,67,69,78 with many fearing ACP was ‘… irrevocable…’ and led to professional ‘… abandonment …’ 69 Informed decision-making was also impacted by unrealistic views, including misunderstanding what medical treatments or palliative care would likely achieve,48,55,67,71 the availability of services and support,48,54,75 the frail elder’s ability to recover, and denial that the frail elder was nearing the end of life.51,57,59,71 Families found this particularly difficult when they felt they had been given ‘… irrational optimism …’ regarding prognosis. 60
Living day to day, discussed by over half the papers, related to how frail elders focussed on living well now, maintaining quality of life, rather than on future planning.43,44,47,48,53–57,59–61,64,66–72,76,78,79 While some frail elders appreciated ACP as a way to ‘… express their opinion …’, 59 there was an ambivalence around ACP. Frail elders often did not see how ACP could be relevant when likely rapid physical or psychological deterioration ‘… meant that any plans may become obsolete quite quickly’. 54 Frail elders often trusted family or professionals to make future care decisions in their best interests,43,44,48,53,54,56,59,68,69,72,78 as these ‘others’ knew what they wanted, challenging the concept of autonomy as a motivating factor for ACP engagement. In reality, while some families felt they knew the person’s preferences, 71 most felt insecure making decisions as preferences had not been discussed:44,48,53,54,60,68,69,72,78 ‘It’s hard to be the healthcare proxy […] you say, “Am I doing the right thing?”’ 60
Personal beliefs and experiences discussed how ACP motivation largely related to personal beliefs, values, goals, and experiences and how these, and therefore motivation to engage with ACP, can change over time. For all stakeholders, previous future planning experiences, such as helping others make end-of-life decisions, 56 facilitating ACP,49,50,58,75 or having experience with the dying process,60,72 could encourage or discourage engagement. For frail elders, personal beliefs included whether they believed decisions would impact their day-to-day life,48,59 distrusting the proxy process, 59 or a desire not to burden their family. 56 For professionals, papers mainly discussed demotivating beliefs, including that ACP conversations were ‘… undervalued …’ 72 by colleagues or managers, that professionals lacked the confidence to manage complex, often upsetting conversations,51,52 and concern that ‘… lack of services’ would impact ACP implementation. 75 Many professionals expressed paternalism, wishing to make decisions themselves as they feared ACP conversations would upset frail elders,43,67 burden families, 71 or challenge their sense of patient responsibility.54,64,78 Responsibility for ACP was unclear,47,51,52,57,59,73,74 with many professionals reluctant to assume responsibility,51,52,57 believing ACP was within another professional’s remit. 57 This highlighted the need to be ‘… more discriminating about who is responsible for which elements of ACP practice …’ 74
Relationality, discussed by almost three-quarters of papers, related to how frail elders live within relationships, whether family, friends, professionals or cultures,43–45,47,48,51–60,65,67–69,71–76,78–81,83 and the impact relationality had on ACP decision-making. Relationality included frail elders wanting to make decisions within relationships43,48,54,56–59,75 and being more concerned with how ACP decisions may affect others than themselves.48,56,58 Developing trusting relationships, particularly the frail elder/professional relationship,43,44,47,48,51–58,60,64,68–72,76,78,80,81,83 was recognised as important, with the development of rapport and trust between all stakeholders cited by many as ‘… the cornerstone …’ 44 of ACP engagement. Long-term care homes were considered excellent environments for this. However, opportunities for professionals to build trusting relationships with frail elders living at home were less promising due to the ‘… erosion of personal continuity between a doctor and their patient …’. 75 Other challenges included disagreements within families,65,67,71 between the frail elder and their family43,47,51,52,58,65,71,74,80 or between families and professionals. 57 Further difficulties were caused by lack of or limited family involvement45,47,48,51,52,59,60,72,74,76,79,81 and limited social networks.51,52,79
Motivation: key messages
The importance of relationality and living well now should be recognised by all stakeholders, with frail elders supported to make decisions within relationships should they wish. Professionals should attempt to build trusting relationships with frail elders and their families as appropriate. In addition, professionals should assess frail elders’ readiness to engage, clarify misunderstandings, and work with them at their own pace. To enable this, professionals need greater clarity around ACP responsibilities and require support to challenge any stakeholder’s negative personal beliefs.
Discussion
Main findings
The main behavioural components, factors and requirements necessary to conduct successful ACP with community-dwelling frail elders are represented conceptually below (Figure 3). This proposed conceptual model includes the interrelated stakeholder behaviours and factors as well as the organisational and system requirements found to be important influencers particularly in enabling professional’s opportunity behaviours.
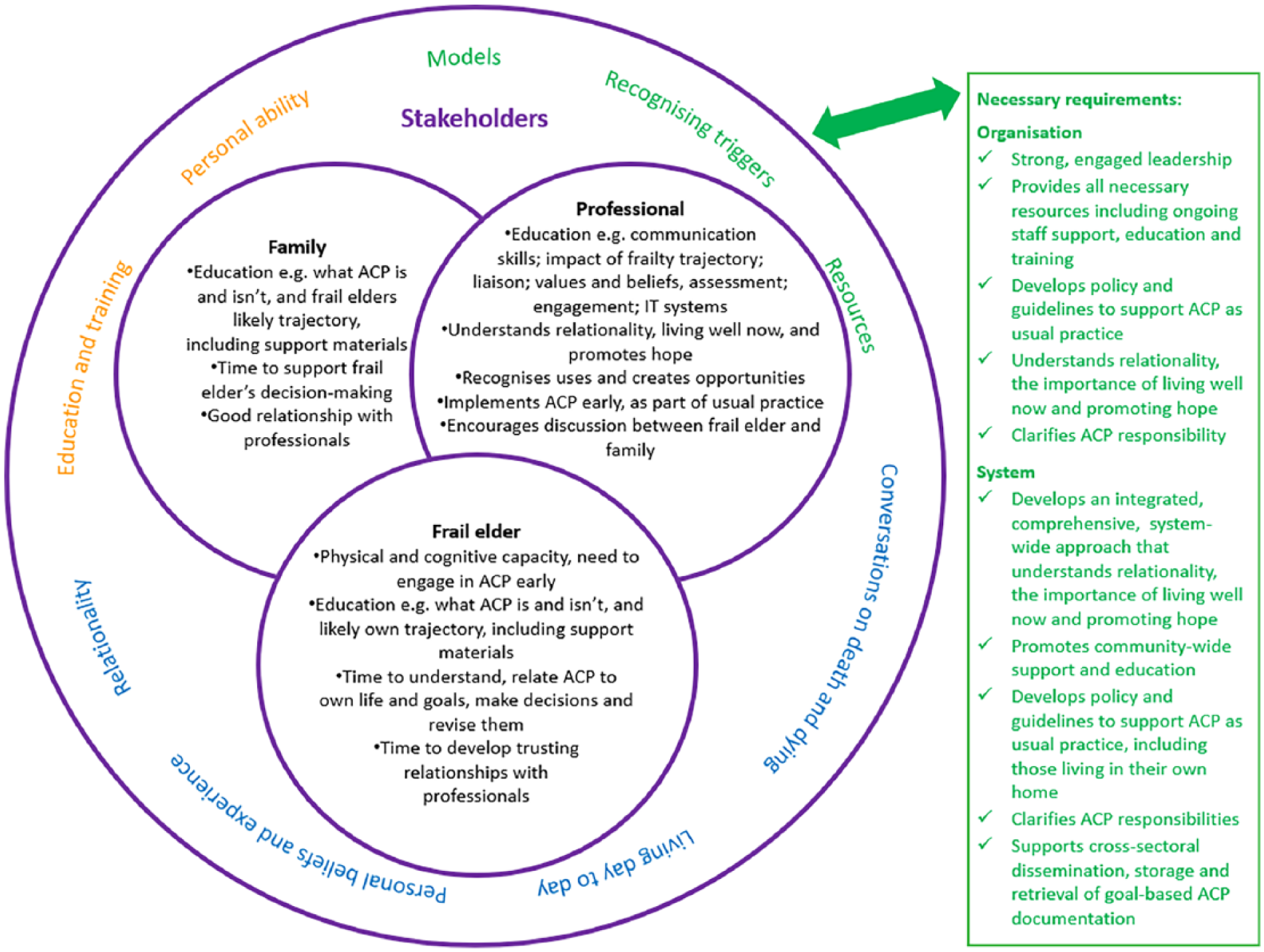
Conceptual model of the behaviours, factors and requirements necessary to conduct successful ACP with community-dwelling frail elders.
The model demonstrates the complexity inherent in ACP facilitation for community-dwelling frail elders, with all elements required for successful ACP implementation. It recommends an approach that recognises the importance of early engagement, relationality, living well now, and stakeholder education, particularly educating professionals to develop the knowledge and skills required to recognise, create and use ACP facilitation triggers throughout frail elders’ end-of-life trajectories. These core recommendations are discussed further below.
Capability
Early engagement, which provides frail elders the greatest chance of being able to engage physically and cognitively with ACP, is the key Capability. If successful, early engagement enables frail elders to engage at their own pace, to understand necessary concepts and how these relate to them, to put meaningful plans in place, to revise decision-making, and to develop trusting relationships with professionals. While finding the ‘right time’ to start ACP is difficult,6,21 early engagement promotes the concept of ACP as an ongoing process that takes place over time and is revisited regularly throughout the frail elders’ life course.85,86 To enable early engagement, all stakeholders require ongoing education. Notably, professionals needed to develop the knowledge and skills required to recognise, create and use triggers to facilitate ACP throughout frail elders’ end-of-life trajectories. Evidence suggests that professionals often require knowledge and communication-based training to enable ACP 85 as conversations can be challenging. 87 The requirement to create and use triggers is also strongly influenced by Opportunity, as frail elders often have little professional contact and few perceived end-of-life needs.16,88
Opportunity
ACP as part of everyday practice and something that occurs over time, rather than a single event, is the key Opportunity. This is reflected in the model’s recommendation of the vital necessity of a system-wide approach, and with it, the necessary resources to support it at every level. This takes forward Sharp et al.’s 19 review which suggested policymakers and healthcare professionals need to address multiple issues to promote personal autonomy, such as informed decision-making, within healthcare systems with limited resources. The concept of an integrative, comprehensive, system-wide approach to ACP for frail elders supports the call for more integrated care systems to better meet the needs of older people. 89 The model also aligns with the public health palliative care approach, which raises community awareness and engagement with end-of-life issues and influences social views of death and dying. 90 This approach presents an opportunity for behavioural change in ACP and may help challenge the conceptualisation of ACP as a failure of medical care by some. 91 As with this public health palliative movement, to effect long-term ACP change requires a system-wide approach, incorporating national campaigns and policy, through to the involvement and commitment of multiple community leaders, organisations and individuals. 92
Motivation
Relationality and living well now are the key Motivations. Individual autonomy is promoted throughout current ACP policies and literature and the current measurable activities system of incentivising health and social care. 91 However, the model challenges the concept of autonomy as the sole motivating factor for frail elders’ ACP engagement. The findings demonstrate the importance frail elders place on living and making decisions within relationships, sometimes choosing that others will make ACP decisions for them. This review demonstrates that often frail elders focus on maintaining current quality of life rather than on ACP, with future planning seen as irrelevant for some within the context of their uncertain physical and psychological trajectory. This links strongly with Capability and Opportunity, emphasising the need to start conversations early and continue them over time, providing frail elders opportunities to change their views as their trajectory changes. These findings are supported by much of the ageing literature which suggests that many older people prioritise trusting relationships and relational decision-making over autonomy,85,93,94 valuing living well now above future planning.23,95 Reframing ACP for frail elders to become something that promotes living well now in addition to future planning and recognising the importance of relational autonomy by supporting frail elders to make decisions within relationships would relate more readily to their daily lives. This reframing may be key to successful ACP implementation in this population.
Behavioural change theory
The model calls for system-wide, multi-level implementation, the recommended approach for successful behaviour change interventions, 96 but current health and social care resource limitations mean this is challenging. While policy, for example, the UK long-term care plan, demonstrates the importance of personalised care at end of life, the UK community sector is experiencing increasing workloads, patient complexity, and lack of funding.97,98 This has led to the prioritisation of core care, such as diagnosis and treatment, over more holistic needs 99 such as ACP. The global picture is similar, particularly regarding end-of-life and palliative care, 100 with priorities often focussed on more fundamental needs such as access to analgesia. 101 However, an incremental approach, making pragmatic decisions by focussing on fewer behaviour changes and building on the success of these, 34 can also be used to facilitate ACP with frail elders. This strategy can be demonstrated by the concept of early engagement, which could be supported by making ACP part of everyday practice and providing targeted materials for frail elders to read in their own time. This would reduce the need for professional involvement at every step of the decision-making process, thus minimising the use of health and social care resources, and as a by-product could promote trusting relationships and relational decision-making.
Strengths and limitations
The proposed conceptual model is limited by the literature. The study exclusion criteria may have meant some relevant papers were missed, particularly papers prior to 1990, those not in English, and those where older participants self-identified as healthy. The use of a proxy for frailty, particularly the proxy of residence in long-term care homes, may have skewed the data away from the needs of frail elders living in domestic settings. The voices of frail elders and families were reduced as literature mainly focussed on behaviours and factors influencing professionals. Furthermore, minimal literature explored early engagement, public health models or moving beyond professional responsibility for ACP within this population. The strength of the review, and therefore the proposed conceptual model, is its rigorous methods; use of a research team to discuss, review and verify the process; and the use of a theoretical model. Using COM-B 27 as a framework ensured a focus on implementation throughout the review and synthesis, and that individual- and system-level behaviours were considered. While some behaviours were influenced by more than one COM-B element, this demonstrates the complexity of the topic and the multidimensional, interdependent behaviours that require targeting for the success of any whole-system intervention.
Implications for clinical practice and research
The conceptual model can be used as a starting point for professionals, organisations and policymakers when looking to improve ACP for frail elders. The themes and key necessary requirements are displayed at stakeholder, organisation and system levels to help target relevant behaviours or requirements depending on the reader’s purpose. This is demonstrated above with the example of early engagement. Further targets that do not require significant health and social care resource but are likely to have a significant impact on successful ACP facilitation are providing opportunities for professionals to develop skills to recognise, proactively use and create facilitation opportunities; professionals’ understanding and working with relationality, including developing trusting relationships and enabling relational decision-making; and reframing ACP for frail elders to focus on living well now as well as future planning.
Conclusion
This review is the first to define the necessary requirements to enable ACP for community-dwelling frail elders and synthesise these into a proposed conceptual model. The model can be used as a starting point for professionals, organisations and policymakers looking to improve ACP for community-dwelling frail elders. Key messages are that frail elders should be engaged early in the process of ACP, that ACP should be reframed as a discussion of current care goals as well as future planning, and that professionals need the opportunity to develop the skills and competencies required to recognise, proactively use and create ACP opportunities throughout frail elders’ end-of-life trajectories. Further research will focus on refining and testing the model in practice, prior to collaborative intervention development with stakeholders.
Supplemental Material
845804_Supplementary_Data_1_-_22.03.19_(1) – Supplemental material for Implementing advance care planning with community-dwelling frail elders requires a system-wide approach: An integrative review applying a behaviour change model
Supplemental material, 845804_Supplementary_Data_1_-_22.03.19_(1) for Implementing advance care planning with community-dwelling frail elders requires a system-wide approach: An integrative review applying a behaviour change model by Sarah Combes, Caroline Jane Nicholson, Karen Gillett and Christine Norton in Palliative Medicine
Supplemental Material
845804_Supplementary_Data_2_-_28.10.18_(1) – Supplemental material for Implementing advance care planning with community-dwelling frail elders requires a system-wide approach: An integrative review applying a behaviour change model
Supplemental material, 845804_Supplementary_Data_2_-_28.10.18_(1) for Implementing advance care planning with community-dwelling frail elders requires a system-wide approach: An integrative review applying a behaviour change model by Sarah Combes, Caroline Jane Nicholson, Karen Gillett and Christine Norton in Palliative Medicine
Supplemental Material
845804_Supplementary_Data_3_-_18.03.19_(1) – Supplemental material for Implementing advance care planning with community-dwelling frail elders requires a system-wide approach: An integrative review applying a behaviour change model
Supplemental material, 845804_Supplementary_Data_3_-_18.03.19_(1) for Implementing advance care planning with community-dwelling frail elders requires a system-wide approach: An integrative review applying a behaviour change model by Sarah Combes, Caroline Jane Nicholson, Karen Gillett and Christine Norton in Palliative Medicine
Footnotes
Author contributions
S.C., C.J.N., K.G. and C.N. made substantial contributions to the study design. The search, screening and selection of papers was conducted by S.C., verified by the research team, with C.J.N. completing an independent screen of 10% of papers at both screening and selection stages. Data analysis and synthesis was conducted by S.C. and discussed and reviewed with C.J.N., C.N. and K.G. throughout the review. Final themes and the conceptual model were agreed by consensus. S.C. prepared the manuscript and C.J.N., C.N. and K.G. revised it critically for important intellectual content. All authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article presents independent research funded by the National Institute for Health Research (NIHR) and Health Education England. The views expressed are those of the author(s) and not necessarily those of the National Health Service (NHS), the NIHR or the Department of Health.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.