
Abstract
Background:
Holistic breathlessness services have been developed for people with advanced disease and chronic breathlessness, leading to improved psychological aspects of breathlessness and health. The extent to which patient characteristics influence outcomes is unclear.
Aim:
To identify patient characteristics predicting outcomes of mastery and distress due to breathlessness following holistic breathlessness services.
Design:
Secondary analysis of pooled individual patient data from three clinical trials. Our primary analysis assessed predictors of clinically important improvements in Chronic Respiratory Questionnaire mastery scores (+0.5 point), and our secondary analysis predictors of improvements in Numerical Rating Scale distress due to breathlessness (−1 point). Variables significantly related to improvement in univariate models were considered in separate backwards stepwise logistic regression models.
Participants:
The dataset comprised 259 participants (118 female; mean (standard deviation) age 69.2 (10.6) years) with primary diagnoses of chronic obstructive pulmonary disease (49.8%), cancer (34.7%) and interstitial lung disease (10.4%).
Results:
Controlling for age, sex and trial, baseline mastery remained the only significant independent predictor of improvement in mastery (odds ratio 0.57, 95% confidence intervals 0.43–0.74; p < 0.001), and baseline distress remained the only significant predictor of improvement in distress (odds ratio 1.64; 95% confidence intervals 1.35–2.03; p < 0.001). Baseline lung function, breathlessness severity, health status, mild anxiety and depression, and diagnosis did not predict outcomes.
Conclusions:
Outcomes of mastery and distress following holistic breathlessness services are influenced by baseline scores for these variables, and not by diagnosis, lung function or health status. Stratifying patients by levels of mastery and/or distress due to breathlessness appears appropriate for clinical trials and services.
Holistic breathlessness services for people with advanced disease and chronic breathlessness can improve psychological aspects of their breathlessness and health.
Outcomes within and between trials show inconsistencies, which may relate to patient characteristics.
Baseline mastery and distress due to breathlessness predict outcomes following holistic breathlessness services.
Diagnosis, lung function and health status do not influence outcomes following holistic breathlessness services.
Patients should be considered as candidates for holistic breathlessness services regardless of their diagnosis, lung function and health status.
Where trials and clinical services face limited resources, prioritising patients with low levels of mastery and/or high levels of distress due to breathlessness appears appropriate.
Introduction
Holistic breathlessness services have been developed for people with advanced disease and chronic breathlessness (i.e. breathlessness that remains persistent despite optimal treatment of the underlying disease 1 ). These typically combine input from multiple-specialities (e.g. palliative care, respiratory care) and professions (e.g. medicine, nursing, physiotherapy) to offer comprehensive assessment of patient and carer needs, and tailored pharmacological and non-pharmacological breathlessness management. 2 In chronic respiratory disease, such services represent an evidence-based means for early integration of palliative care based on need rather than prognosis. 3
Overall, holistic breathlessness services lead to improvements in mastery (i.e. patients’ feeling of control over their disease 4 ), distress due to breathlessness and psychological health. 2 However, treatment outcomes across and within trials is inconsistent, 2 and the extent to which patient characteristics influence this is unclear. Breathlessness itself is associated with poor physical and mental health, 5 which may influence how patients interact with services. Other factors including health status, exercise capacity, anxiety and depression may also influence outcomes, as they can for pulmonary rehabilitation.6–9 We aimed to identify patient predictors of outcomes from holistic breathlessness services, focusing on improved mastery and reduced distress due to breathlessness.
Methods
Design
We conducted a secondary analysis of pooled individual patient data from three trials of holistic breathlessness services for patients with advanced malignant and non-malignant conditions, delivered over 2–6 weeks.10–12 The original data were collected between 2008 and 2012. Our methods built on those in an analysis of patient predictors of response to opioids. 13
Analysis
Our primary analysis considered improvements on the Chronic Respiratory Questionnaire (CRQ) mastery domain, defined as a 0.5 point increase in line with the minimum clinically important difference. 14 This outcome was measured in all trials and was the primary outcome in the Higginson et al. 10 trial. A secondary analysis considered improvements on Numerical Rating Scale (NRS) distress due to breathlessness (NRS distress), defined as a 1-point reduction. 15 This was the primary outcome in the two Farquhar et al.11,12 trials but was not measured in the Higginson et al. 10 trial.
Candidate variables (and their reference group/possible score ranges) for the primary and secondary analysis were selected based on availability within the dataset. They included age, sex, diagnosis (reference: COPD), FEV1 % predicted and baseline scores for CRQ dyspnoea, fatigue, mastery and emotional domains (1–7), EuroQol-5D (EQ5D) Utility Index (–1 to 1) and Visual Analogue Scale (VAS; 0–100), Hospital Anxiety and Depression Scale (HADS) anxiety and depression scores (0–21), and NRS average breathlessness in the previous 24 h (NRS average; 0–10). Baseline NRS distress (0–10) was included only in the secondary analysis. For all variables, the timepoint immediately pre-intervention for each group was treated as ‘baseline’ (e.g. in the Higginson trial, fast-track participants’ baseline was week 1, wait-list participants’ baseline was week 6).
Variables significantly related to improvements by the minimum clinically important difference (p < 0.05) in univariate logistic regression models were considered in separate multivariate analyses for CRQ mastery and NRS distress. We used backwards stepwise logistic regression modelling, with sequential removal of variables with the largest non-significant (p > 0.05) p value in each model. Age, sex (reference: male) and trial (reference: Farquhar et al. 2016) were forced into both models to control for these clinically relevant variables. This secondary analysis of anonymised data did not require ethical approval (references for each contributing study: King’s College Hospital 10/H0808/17; Cambridgeshire 2 NHS 08/H0308/157).
Results
Participants
The pooled dataset comprised 259 participants (118 female) with a mean (SD) age of 69.2 (10.6) years (Table 1). The most common primary diagnosis was COPD (49.8%), followed by cancer (34.7%) and interstitial lung disease (10.4%).
Sample characteristics.
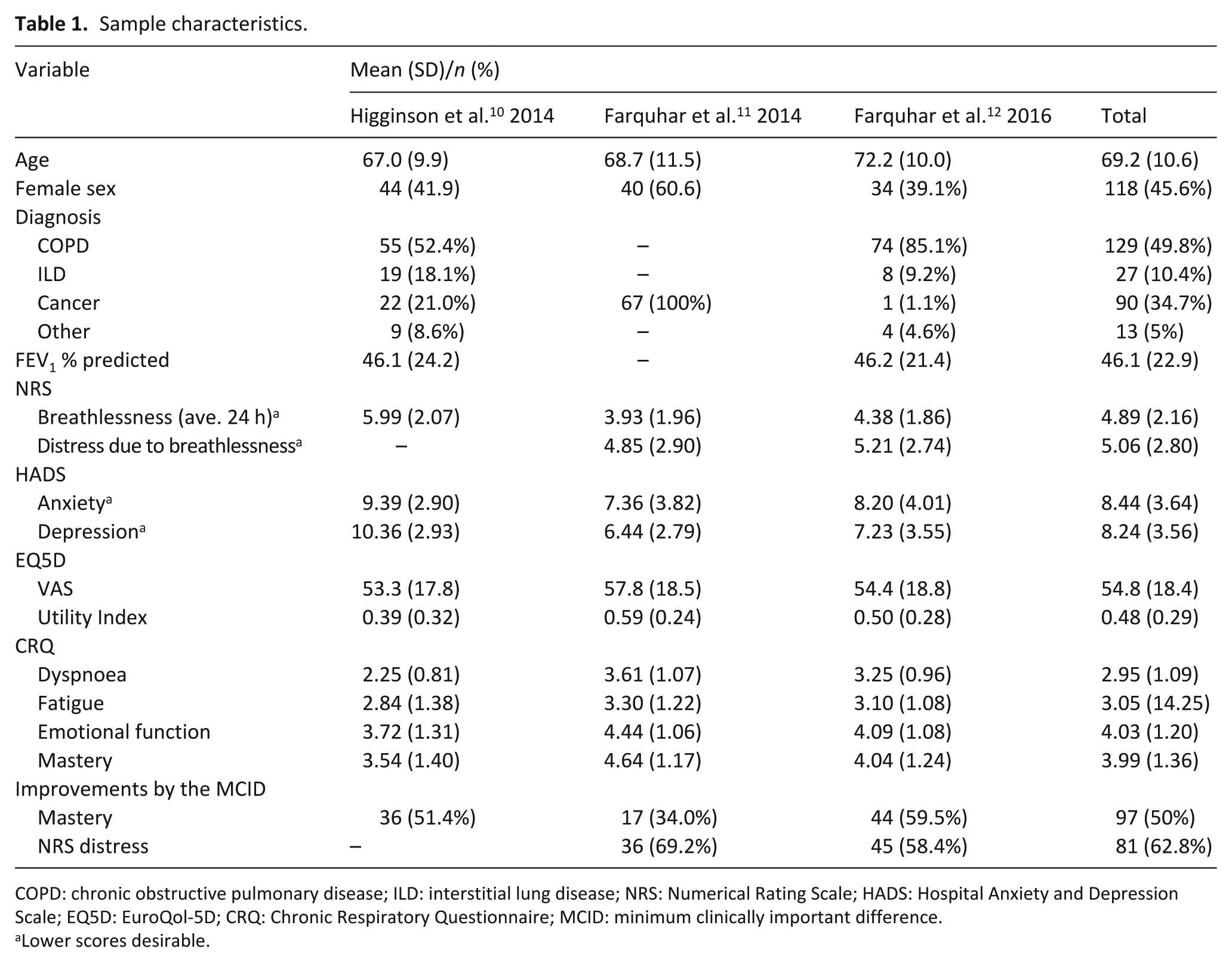
COPD: chronic obstructive pulmonary disease; ILD: interstitial lung disease; NRS: Numerical Rating Scale; HADS: Hospital Anxiety and Depression Scale; EQ5D: EuroQol-5D; CRQ: Chronic Respiratory Questionnaire; MCID: minimum clinically important difference.
Lower scores desirable.
CRQ mastery
Of the participants for whom CRQ mastery outcomes could be calculated, 97/194 (50%) were classified as improving by the minimum clinically important difference. In univariate analyses, baseline variables significantly associated with improvements in CRQ mastery were baseline CRQ mastery (p < 0.001), dyspnoea (p = 0.008) and fatigue (p = 0.009); EQ5D Utility Index (p = 0.007) and VAS (p = 0.014); and NRS average (p = 0.039). Controlling for age, sex and trial in the multivariate modelling, baseline CRQ mastery remained the only significant predictor of outcomes. Participants with higher CRQ mastery scores at baseline (i.e. better mastery) were less likely to improve by the minimum clinically important difference, with a 43% decrease in odds for a 1-point increase at baseline (odds ratio (OR) 0.57, 95% confidence interval (CI) 0.43–0.74; p < 0.001; Table 2).
Predictors of outcomes in multivariate logistic regression.
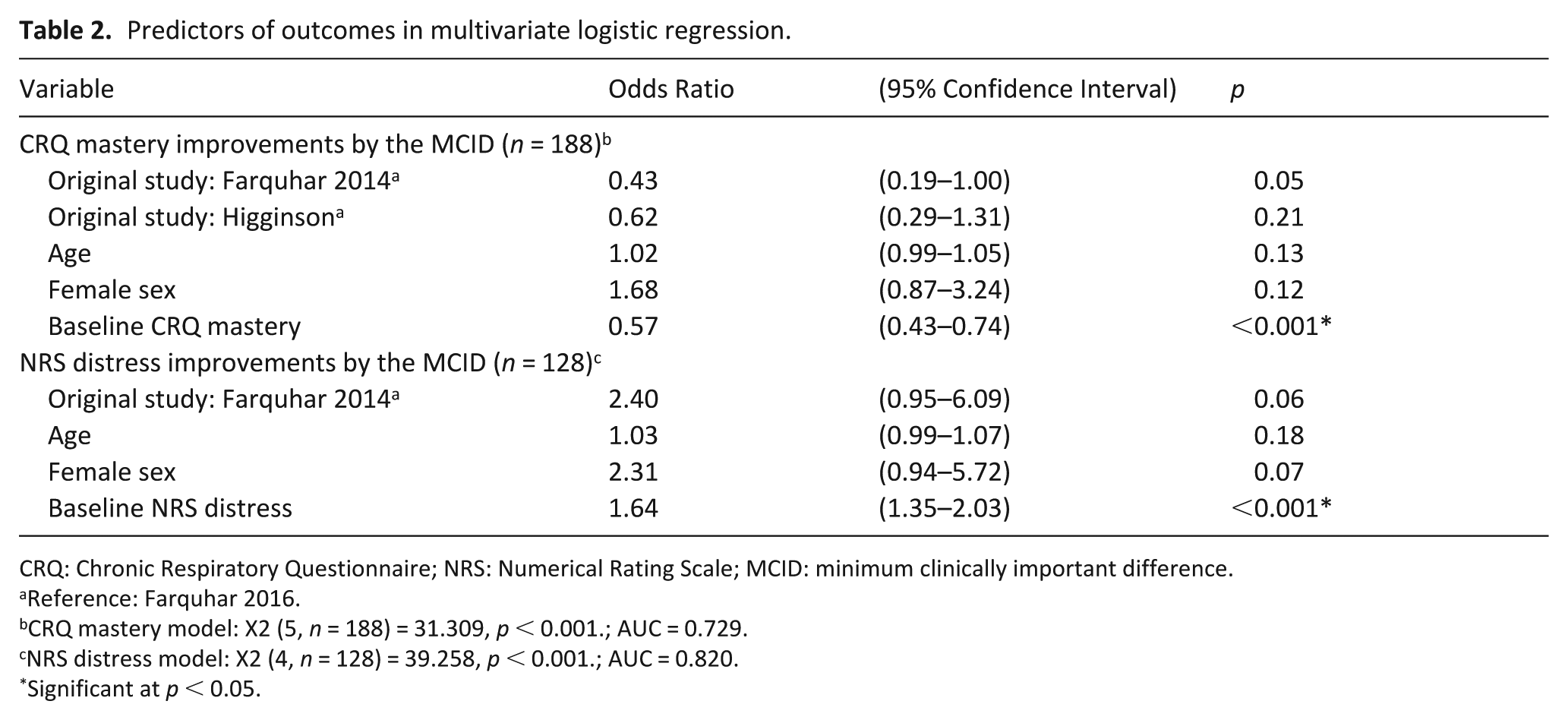
CRQ: Chronic Respiratory Questionnaire; NRS: Numerical Rating Scale; MCID: minimum clinically important difference.
Reference: Farquhar 2016.
CRQ mastery model: X2 (5, n = 188) = 31.309, p < 0.001.; AUC = 0.729.
NRS distress model: X2 (4, n = 128) = 39.258, p < 0.001.; AUC = 0.820.
Significant at p < 0.05.
NRS distress due to breathlessness
Of the participants for whom NRS distress outcomes could be calculated, 81/129 (62.8%) were classified as improving by the minimum clinically important difference. The only variable significantly associated with NRS distress outcomes in the univariate analysis was baseline NRS distress (p < 0.001). This remained significant in the multivariate model controlling for age, sex and trial. For every 1-point increase in baseline NRS distress the odds of improving by the minimum clinically important difference increased by 64% (OR 1.64; 95% CI 1.35–2.03; p < 0.001; Table 2).
Discussion
Our findings reveal that baseline CRQ mastery and NRS distress are strong predictors of outcomes from holistic breathlessness services; other patient characteristics we considered, including diagnosis, are not associated with treatment outcome. Clinical services and future trials may therefore consider focusing efforts on patients with poor psychological health relating to their breathlessness, based on screening questions. To illustrate this, in a post hoc analysis of outcomes according to unadjusted baseline CRQ mastery, 75% of patients with a score of ⩽2 improved by the minimum clinically important difference, while just 28% of those with a score of ⩾5 did so. For NRS distress, 89% of patients with a ‘severe’ score (⩾7) improved by the minimum clinically important difference compared with 39% of those with a ‘mild’ baseline score (⩽3). With high levels of health service use in breathless patients and limited resources, factors to inform prioritised access to holistic breathlessness services based on likelihood of benefit may be useful.
It is notable that outcomes were not influenced by breathlessness severity, patient diagnosis, lung function, overall health status, anxiety or depression. In some instances, this finding may relate to baseline scores within our sample. For example, baseline scores indicated only mild anxiety and depression; 16 higher levels of psychological distress were therefore not considered within our analyses. However, this finding could also be a product of the tailored nature of these services, whereby individual clinical and demographic characteristics should be addressed.
This work has strengths and limitations. We combined individual patient-level data from three high-quality randomised controlled trials, resulting in a more powerful analysis than would be possible with any single trial. This approach meant our analyses were limited to variables common across the datasets. Potentially important patient factors (e.g. multi-morbidity, functional status) were not tested as they were not measured across all three trials, and fewer cases were available for our secondary analysis around distress. It is also important to acknowledge that there is no consensus on the optimal outcomes of holistic breathlessness services. While we have focused on mastery and distress due to breathlessness, another trial comparing one versus three sessions of a breathlessness service focused on worst breathlessness over the previous 24 h as a primary outcome. Future work may benefit from establishing a core set of clinically relevant patient characteristics and outcomes from breathlessness services, and consistently including these when assessing interventions. Our findings may reflect regression to the mean, 17 however, the magnitude of effects observed and consistent benefit across the controlled trials 2 suggest that this is not the only contributing factor. Finally, these data are limited to holistic breathlessness services trialled in the United Kingdom and may not transfer to international services.
Conclusion
Outcomes of holistic breathlessness services in terms of improved mastery and reduced distress due to breathlessness are influenced by baseline scores for these variables, but not breathlessness severity, patient diagnosis, lung function, overall health status, or mild anxiety or depression. In future trials, and where clinical services face limited resources, selecting or prioritising patients with low levels of mastery or high levels of distress appears appropriate.
Footnotes
Acknowledgements
Thank you to our team of service-user representatives who have provided their reflections and feedback throughout this project. M.M. and I.J.H. designed and obtained funding for the study. L.J.B. conducted data cleaning and analysis, with statistical guidance from G.W. and M.M. L.J.B. drafted the original version of the short report with supervision from M.M. All the authors contributed to interpretation of the data and critical revisions to the final manuscript.
Data management and sharing
Requests for access to anonymised data should be directed to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
This secondary analysis of anonymised data did not require ethical approval. Each contributing study obtained appropriate ethical approvals: King’s College Hospital 10/H0808/17; Cambridgeshire 2 NHS 08/H0308/157.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was conducted as part of a project funded by an NIHR Health Services and Delivery Research Grant (NIHR HSDR 16/02/18). M.M. and G.W. are supported by the NIHR Collaboration for Leadership in Applied Health Research and Care (CLAHRC) South London; M.M. is supported by an NIHR Career Development Fellowship (CDF-2017-009); W.M. is supported by the NIHR CLAHRC Northwest London, and I.J.H. holds an NIHR Emeritus Senior Investigator Award and is supported by Cicely Saunders International. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health and Social Care.