
Abstract
Background:
The anticipatory prescribing of injectable medications to provide end-of-life symptom relief is an established community practice in a number of countries. The evidence base to support this practice is unclear.
Aim:
To review the published evidence concerning anticipatory prescribing of injectable medications for adults at the end of life in the community.
Design:
Systematic review and narrative synthesis. Registered in PROSPERO: CRD42016052108, on 15 December 2016 (https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=52108).
Data sources:
Medline, CINAHL, Embase, PsycINFO, Web of Science, Cochrane Library, King’s Fund, Social Care Online, and Health Management Information Consortium databases were searched up to May 2017, alongside reference, citation, and journal hand searches. Included papers presented empirical research on the anticipatory prescribing of injectable medications for symptom control in adults at the end of life. Research quality was appraised using Gough’s ‘Weight of Evidence’ framework.
Results:
The search yielded 5099 papers, of which 34 were included in the synthesis. Healthcare professionals believe anticipatory prescribing provides reassurance, effective symptom control, and helps to prevent crisis hospital admissions. The attitudes of patients towards anticipatory prescribing remain unknown. It is a low-cost intervention, but there is inadequate evidence to draw conclusions about its impact on symptom control and comfort or crisis hospital admissions.
Conclusion:
Current anticipatory prescribing practice and policy is based on an inadequate evidence base. The views and experiences of patients and their family carers towards anticipatory prescribing need urgent investigation. Further research is needed to investigate the impact of anticipatory prescribing on patients’ symptoms and comfort, patient safety, and hospital admissions.
Keywords
The anticipatory prescribing of injectable medications for adults at their end of life is recommended practice in a number of countries.
Practitioners believe that anticipatory prescribing has a key role in ensuring patients receive effective and timely symptom control and in avoiding crisis inpatient admissions.
Practice and policy are based on healthcare professionals’ views that anticipatory prescribing is reassuring to patients and their family carers and is clinically effective in providing effective symptom control.
No studies have explored patients’ views and experiences of anticipatory prescribing
Anticipatory prescribing is a low-cost intervention, but there is inadequate evidence to allow conclusions to be drawn about its cost-effectiveness, safety, impact on patient-reported symptoms, and comfort or prevention of crisis hospital admissions.
Research is needed to investigate the impact of anticipatory prescribing on patient-reported symptom control and comfort, patient safety, and crisis hospital admission avoidance.
The acceptability of anticipatory prescribing for patients and their family carers requires urgent investigation.
Introduction
The management of pain, distress, and other symptoms at the end of life is a shared goal for patients, their family carers, and healthcare professionals.1–5 To meet the needs of patients approaching the end of their lives in the community, anticipatory prescribing has been promoted to optimise symptom control and prevent crisis hospital admissions.6–10 Anticipatory prescribing is the prescription and dispensing of injectable medications to a named patient, in advance of clinical need, for administration by suitably trained individuals if symptoms arise in the final days of life.6,11 Injectable medications are typically prescribed for four common symptoms: pain, nausea and vomiting, agitation, and respiratory secretions.7,11,12
Community-based anticipatory prescribing practices vary between countries based on local healthcare conventions, financial costs, legislation surrounding controlled drugs, and the availability of healthcare professionals to administer medications when needed.9,13–15 Studies in the United States of America15–17 and Singapore 9 report on schemes where drugs are prescribed in oral, sublingual, or rectal forms for family members to administer. In the United Kingdom7,8 and Australia, 18 it is considered good practice to prescribe and dispense injectable medications that offer reliable and rapid symptom relief when patients can no longer manage oral medications during the dying phase. 11 They are typically administered by nurses or general practitioners (GPs) based on their clinical assessment that the person is dying and has irreversible symptoms.3,7,19,20
Anticipatory prescribing of injectable medication in the community first appeared in the literature by Amass and Allen 6 and has subsequently been adopted as a central component of good end-of-life care planning in the United Kingdom, Australia, and New Zealand.7,10,11,18,21 Anticipatory prescribing is recommended to follow an individualised approach after assessment of a patient’s particular needs and situation.7,22 It ensures rapid access to medications, particularly out-of-hours when sourcing medication can be delayed22–25 and enables rapid administration of drugs when out-of-hours clinicians may have limited knowledge of a patient’s situation. 26
However, prescribing strong injectable medications ahead of need has potential risks. Appropriate prescribing relies on GPs correctly identifying that patients are approaching their last days of life.3,24,27 Appropriate administration is dependent on nurses correctly diagnosing that symptoms are not reversible and that the patient is dying; a skilled judgement requiring multidisciplinary discussion with senior colleagues in the hospital setting. 19 The prescriber remains accountable for the drugs, including strong opioids, which may be in the home for weeks 7 and are open to misuse by visitors and family members.3,28 In the United Kingdom, the critical review of the Liverpool Care Pathway found that the use of anticipatory prescribing without adequate explanation or justification led to families being concerned about over-sedation and drugs hastening death. 29
Despite these concerns, subsequent UK end-of-life care guidance continues to advocate individualised anticipatory prescribing as best practice.7,8 However, the same guidance 7 highlighted the limited evidence base concerning anticipatory prescribing practice and the risk that drugs are sometimes prescribed in a ‘blanket-like fashion’ rather than tailored to patients’ needs.
In summary, it is unclear whether anticipatory prescribing is acceptable to all involved, clinically effective or cost-effective.
Aim
It was, therefore, decided to undertake a systematic literature review concerning anticipatory prescribing for adults at the end of life in the community. The focus is exclusively on injectable medications, as this is the most widespread form of anticipatory prescribing, requires specific training, and has been highlighted to have potential for misuse.7,29
Review questions
With regard to anticipatory prescribing of injectable medications for adults in the community approaching the end of their lives:
What is current practice?
What are the attitudes of patients?
What are the attitudes of family carers?
What are the attitudes of community healthcare professionals?
What is its impact on patient comfort and symptom control?
Is it cost-effective?
Methods
Eligibility criteria
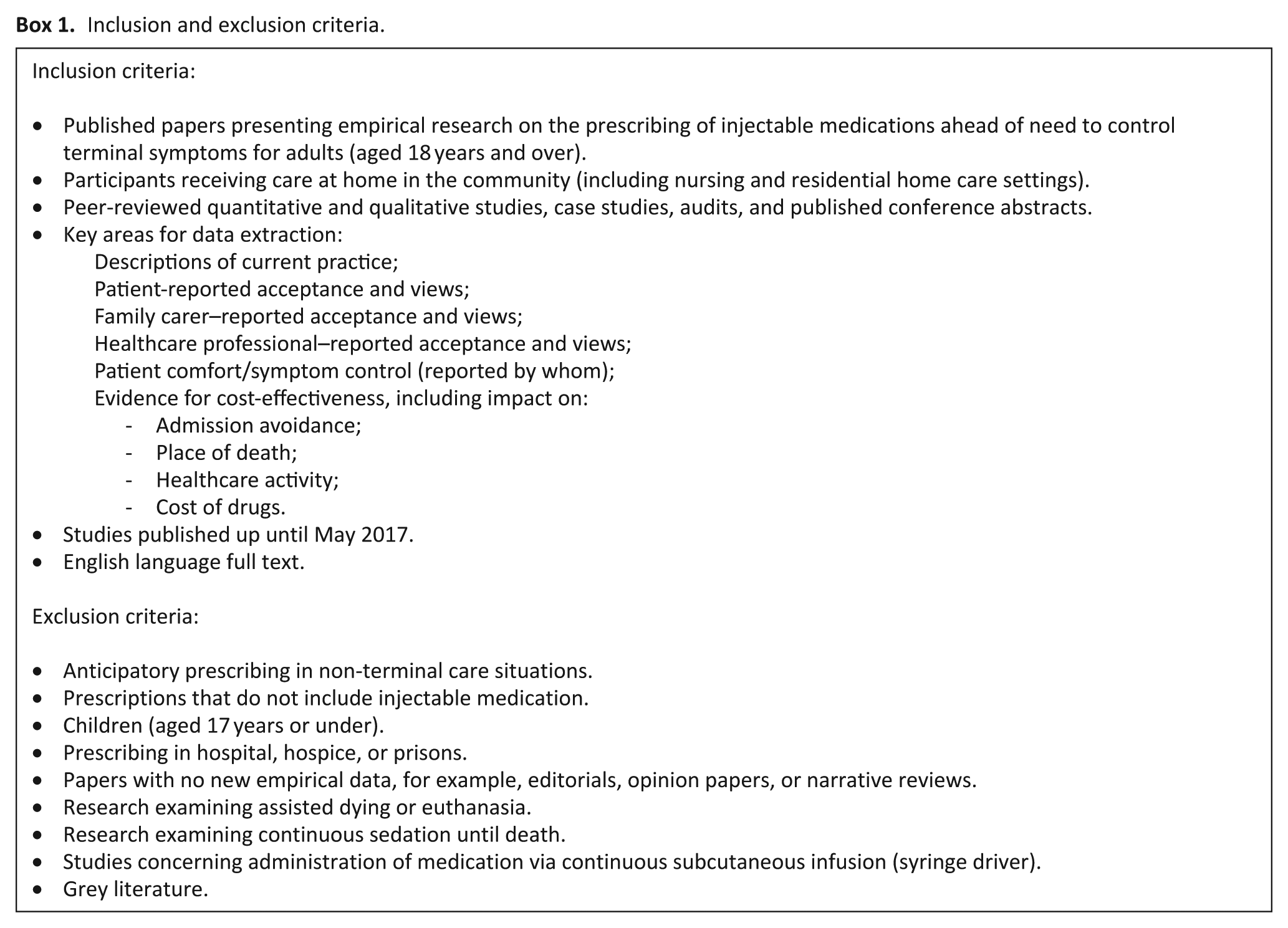
Papers were included if they presented empirical research on the anticipatory prescribing of injectable medications for symptom control in adults (aged 18 years and over) at the end of life in the community. Box 1 presents detailed inclusion and exclusion criteria.
Inclusion and exclusion criteria.
Search strategy
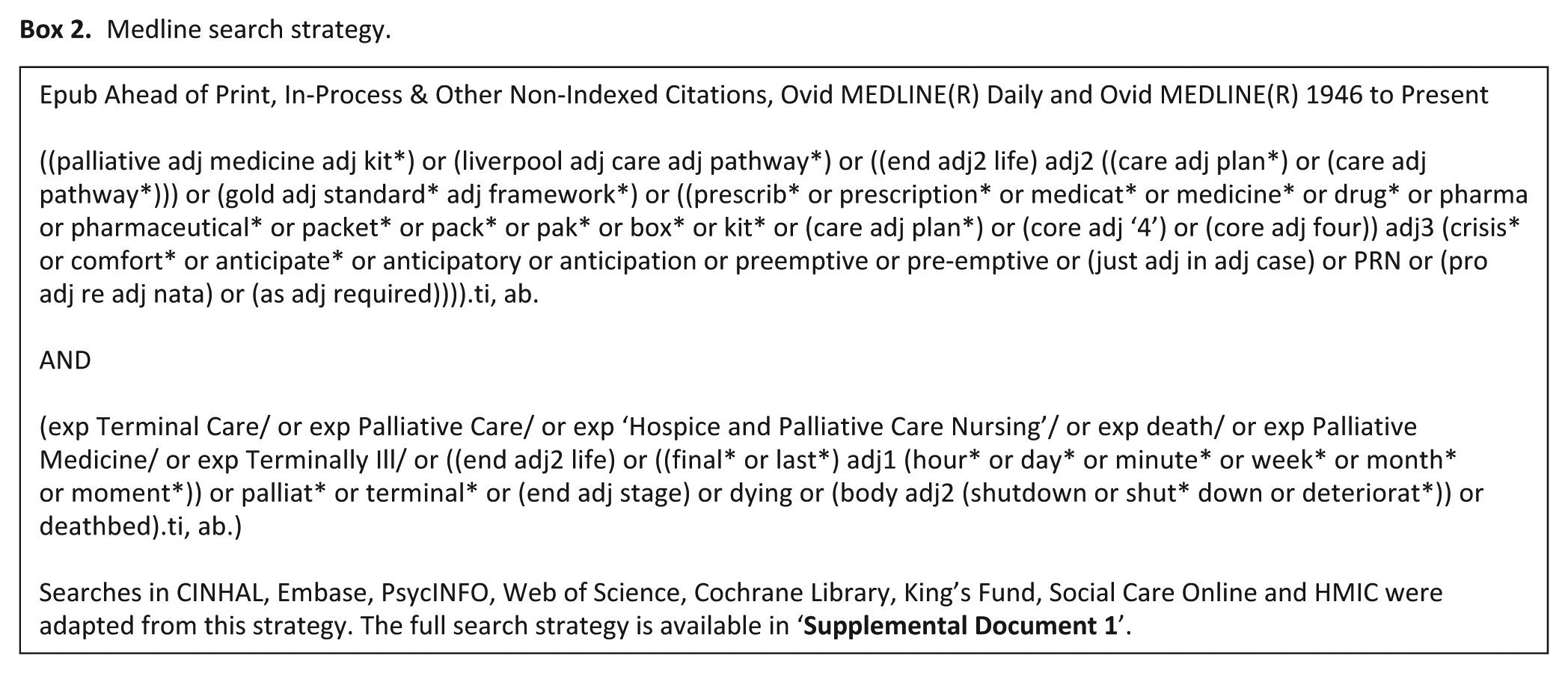
The search strategy was developed in collaboration with a specialist information technologist (I.K.). The search strategy in Medline is presented in Box 2 and was adapted for each subsequent database (CINAHL, Embase, PsycINFO, Web of Science, Cochrane Library, King’s Fund, Social Care Online and Health Management Information Consortium (HMIC);
Medline search strategy.
Study selection
After exclusion of irrelevant and duplicate titles, abstracts were screened for eligibility independently by two reviewers (B.B. and R.R.) with disagreement between reviewers resolved by consensus. Full-texts of all potentially relevant papers were then assessed for eligibility by B.B. and with a second review by R.R. where eligibility was uncertain (Figure 1).
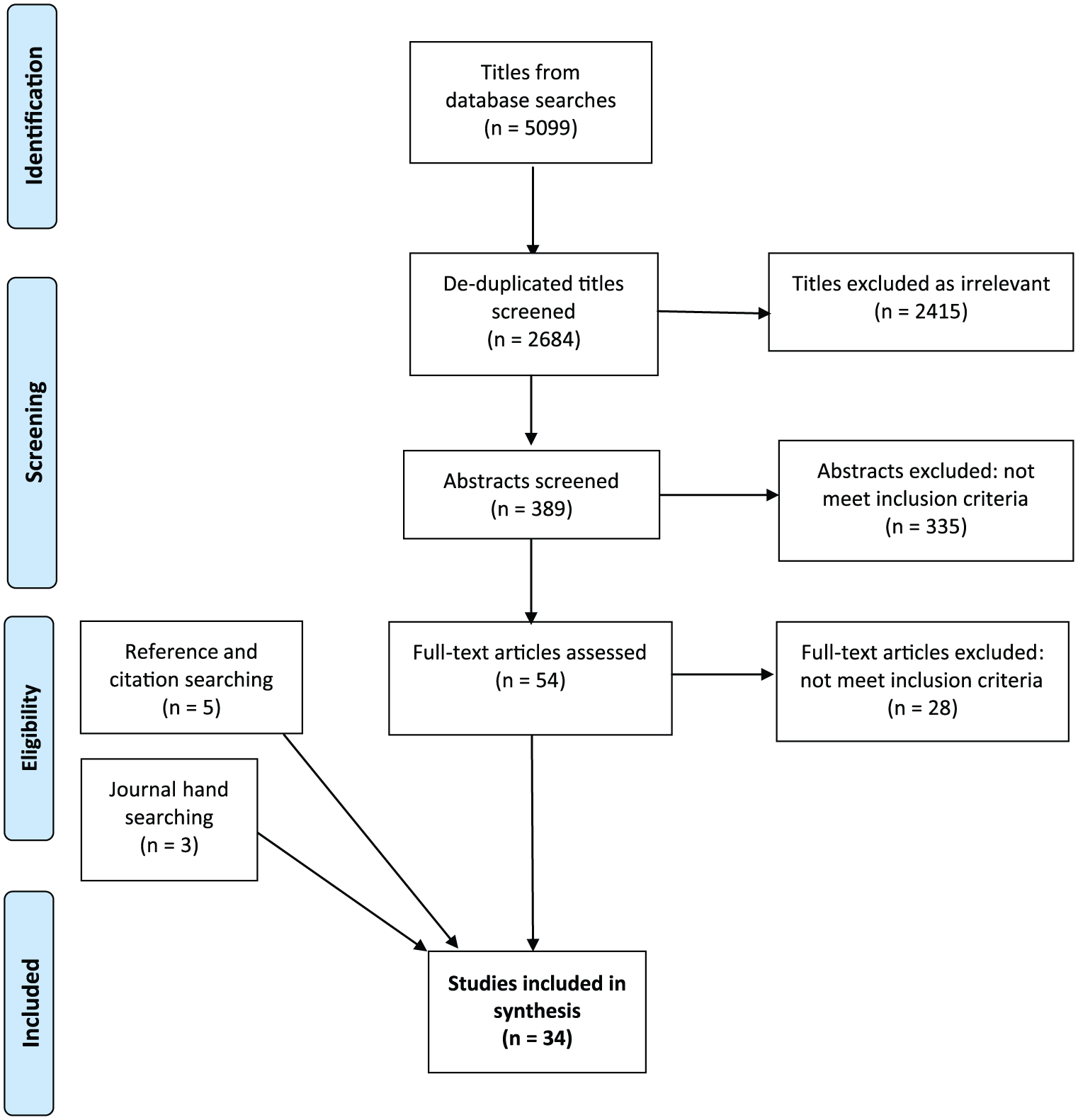
PRISMA flow diagram.
Data extraction, quality appraisal, and data synthesis
A review-specific data extraction form was designed and piloted on five papers. Two reviewers (B.B. and R.R.) then independently extracted data from each eligible paper: publication details, study aims, participants, methods, and results relevant to each of the six review questions (
Two reviewers (B.B. and R.R.) then independently critically appraised the quality and relevance of each included study using Gough’s ‘Weight of Evidence’ (WoE) framework 30 (Table 1). This framework rates both the quality and relevance of included studies using four domains of assessment concerning the internal validity of the study (WoE A), the appropriateness of study design to the review aims (WoE B) and the focus or relevance of the study to the review aims (WoE C). These three domains were then combined into an overall judgement of study quality and relevance (WoE D). Where the reviewer was also an author of a selected study, a third reviewer (S.B.) conducted the quality assessment. Discrepancies in quality appraisal decisions were discussed and consensus achieved.
Review-specific Gough’s ‘Weight of Evidence’ criteria.
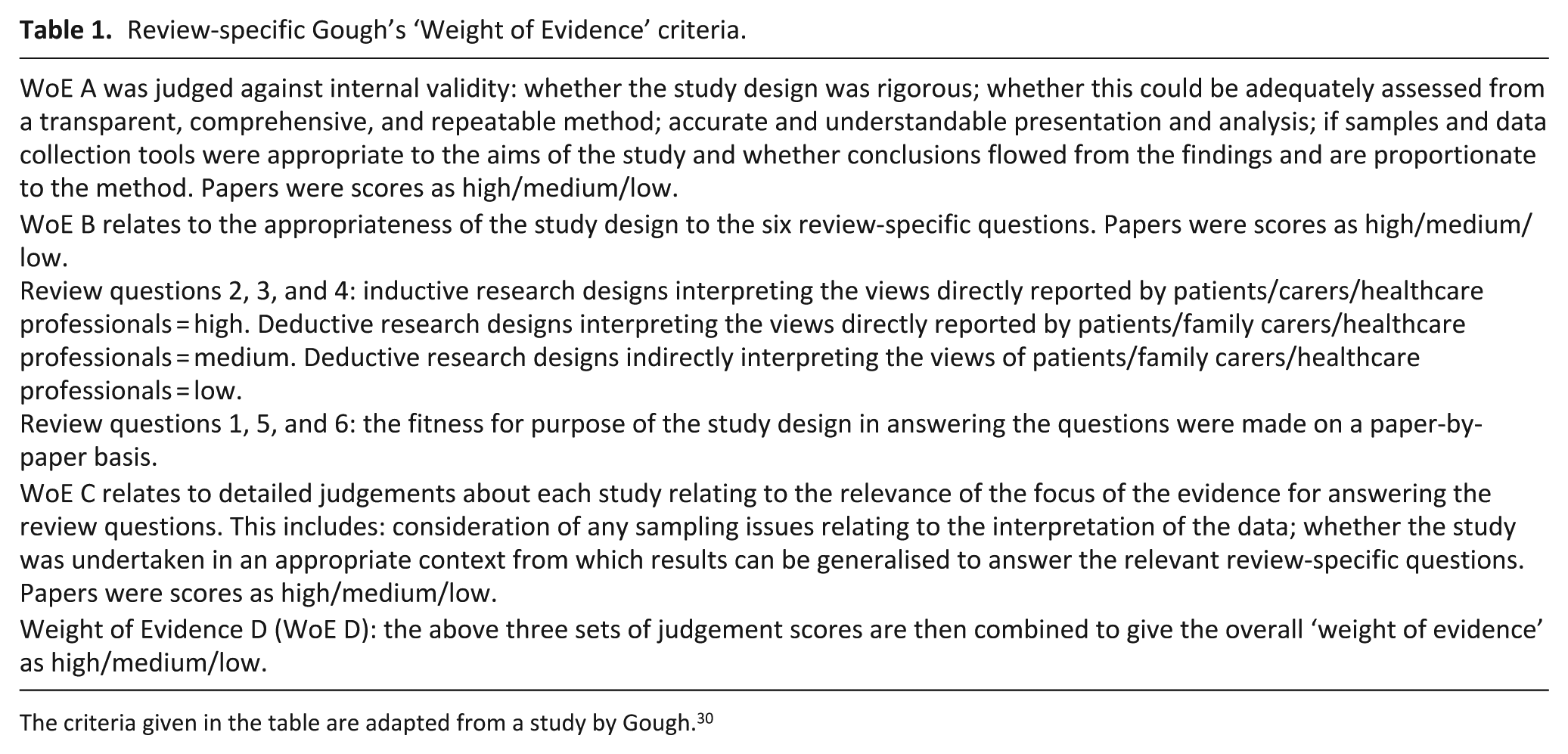
The criteria given in the table are adapted from a study by Gough. 30
Data synthesis used a narrative approach.31,32 This was chosen for its applicability to the synthesis of a range of qualitative and quantitative evidence. 32 The narrative synthesis involved the following three iterative stages:
Developing a preliminary synthesis: B.B. created a textual description of each study from the data extraction forms. Study descriptions were grouped together and tabulated based on the sample population and the research questions the results answered. B.B. carried out an inductive thematic analysis to identify the main, recurrent, and important data across the studies in answering each research question.31,32
Exploring relationships in the data: B.B. (a nurse researcher) and R.R. (a palliative doctor and clinical academic) constructed the interpretive synthesis by independently reviewing the thematic analysis and exploring heterogeneity across studies.31,32 Particular attention was placed on the differences and similarities between the studies, including methodological approaches, context, the characteristics of the populations being studied, and results. The results which emerged from studies conducted by researchers from different disciplinary and epistemological positions were debated and consensus in the synthesis was reached. 32 The synthesis was further refined through discussion of the review results and their implications with clinicians, interdisciplinary academic audiences, and S.B. (a GP and clinical academic).
Assessing the robustness of the synthesis: the quality and relevance assessment using Gough’s WoE framework 30 informed each stage of the synthesis. Papers judged as being of high quality using Gough’s WoE framework were considered more credible and relevant than medium quality papers throughout data synthesis.30,32 Conclusions drawn only from papers assessed under WoE D to be of low quality were deemed inadequate unless they supported the findings of high or medium quality papers. 32 The reviewers decided to include low quality evidence in the synthesis to demonstrate that current anticipatory prescribing practice is largely based on low and medium quality evidence, highlighting the gaps in knowledge and the need for future research (Table 2).
Number of papers included in the synthesis.
The review protocol was registered with PROSPERO (reg. no. 42016052108).
Results
The paper identification process is summarised in Figure 1. Database searches identified 2684 titles after de-duplication: journal hand searches identified three conference abstracts with five papers from reference and citation searching. A total of 34 papers, reporting on 30 studies, were included in the synthesis: 24 research papers and 10 conference abstracts. Two studies were reported in two papers33–36 and one study in three papers: 19,20,37 as each paper presented different findings, they were treated as individual study units in the synthesis. Papers reported on practice in the United Kingdom (n = 28), Australia (n = 5), and Canada (n = 1). Published papers’ methods included qualitative interviews with healthcare professionals (n = 15), qualitative interviews with family carers (n = 2), retrospective patient notes reviews (n = 7), staff or family carers questionnaires (n = 6), and clinical audits (n = 4). Table 3 summaries the included papers and their weighting on Gough’s WoE framework: 30 3 were rated high quality, 22 medium quality, and 9 low quality.
Summary of included studies.
Care home: a community residence without trained nurse on site; nursing home: a community residence with trained nurses on site; GP: family doctor; H: high; M: medium; L: low.
Quality of the evidence was assessed using Gough’s Weight of Evidence framework: 30 (A) coherence and integrity of the evidence in its own terms; (B) appropriateness of the study design in answering the review questions; (C) relevance of the evidence for answering the review questions; and (D) overall assessment of the quality and relevance of the study, derived by combining judgements (A), (B), and (C).
What is current practice?
Few studies investigated the frequency of anticipatory prescribing in the community: these were primarily limited to the United Kingdom, and patient samples do not accurately represent the general population. 38,40,42,43,47,50 Reported figures varied greatly across studies which may relate to differences in study design, context, and denominators used.38,40,42,43,47,50 A study of 12 GP practices in one UK county reported that anticipatory prescribing occurred in 16% of all predictable deaths in the community (home or care home). 42 By contrast, a retrospective case note review of 150 consecutive deaths managed by a specialist palliative care team indicated that 63% of the sample had anticipatory prescribing in place at the time of death. 40 One Australian nursing home study reported a low rate of anticipatory prescribing but provided no figures. 50 Three retrospective studies in UK nursing home settings reported anticipatory prescribing rates varying from 37%, 43 28%–62%, 47 to 13–100%. 38 Although the data are limited by inadequate definitions of anticipatory prescribing,43,47 patients at home or in care homes appear less likely to be prescribed drugs than those in nursing homes.38,42,43,47 Surveys of community healthcare professionals suggest that anticipatory prescribing is widespread in the United Kingdom.13,20
There is wide variation in the timing of anticipatory prescribing prior to death, ranging from a few days3,49 to several weeks.3,5,40 Difficulties are encountered in predicting when patients are likely to die3,24 with GPs and community nurses frequently recalling situations where drugs were not issued in a timely manner.3,39,48 Nurses often initiate the process by alerting the GP to a patient’s changing condition and requesting an anticipatory prescription.5,20,24,37,49 One study reported nursing home staff would request anticipatory prescriptions weeks ahead of need to mitigate the difficulty of timely GP reviews. 5
Decisions regarding which anticipatory medications are issued are often shared between GPs and nurses.24,37 In most cases, only the GP can issue the prescription: the small number of UK nurse-prescribers still prefer to share decision-making with the GP. 24 There is considerable variability in the terminal symptoms prescribed for and anticipatory drugs prescribed. There are very limited data about anticipatory drugs prescribed.20,38,55 One study, 38 rated as medium quality, indicates that there was variability in the number and type of terminal symptoms prescribed for across eight nursing homes; 54% of patients had at least one drug prescribed (most commonly for pain and least commonly nausea and vomiting), but only 15% had drugs prescribed for all four recommended indications. A local service evaluation, 55 rated as low quality, lists the most commonly prescribed drugs but did not provide frequencies.
There is limited literature concerning the relationship of anticipatory prescribing to diagnosis. Cancer was predominant in two studies of anticipatory medication kit implementation48,49 (84% and 91.5%), with 79% of community nurses reporting their last experience of anticipatory prescribing was with cancer patients. 20 Conversely, one retrospective study of 150 consecutive deaths under a community specialist palliative care service found that anticipatory medications were in place at the time of death for 78% of non-cancer deaths (n = 50) but only 55% of cancer deaths (n = 100). 40 No other data are provided to allow assessment of the comparability of these diagnostic subgroups. Anticipatory medication timing decisions are perceived to be more challenging in the less predictable dying trajectories of non-cancer illnesses. 3
The literature concerning the use of anticipatory medications after prescription is also limited. Use in nursing homes appears to be less common: one retrospective study reported that ‘less than a third’ of patients required the administration of prescribed medications, 43 and a qualitative study of nursing home nurses reported that very few dying patients required the administration of prescribed drugs. 5 Much higher proportions of use have been reported at home, ranging from 70%–77%.6,48 The sedative anxiolytic midazolam is identified in three studies as the most frequently administered drug.20,43,46 However, two of these studies20,46 relied on healthcare professionals recalling the drugs they gave and did not detail actual practice.
The literature suggests that decision-making concerning anticipatory medication administration is often undertaken by nurses without consultation with a doctor.5,19,20,45,54 In some situations, a range of doses are prescribed on drug charts, allowing nurses discretion on the dose administered. 19 In contrast, one Canadian study reported nurses to have a less independent role, needing to gain authorisation from a doctor before administering the drugs. 49 UK nurses identify four conditions that all need to be met before they administer medication: symptoms are irreversible and due to the dying phase; inability to take oral medication; patient consent where possible; and decisions made independent of influence from family carers. 19 Nurses often work in pairs when making this assessment or check their decisions with nursing colleagues. 19 In some areas, family carers have been trained to assess symptoms and give injectable drugs, with or without direct clinical guidance, in Australia14,22,23 and United Kingdom.53,56
What are the attitudes of patients?
No studies have investigated patients’ experience of or views towards anticipatory prescribing. One audit, 6 rated as medium quality, and one service evaluation, 55 rated as low quality, report anticipatory prescribing to be well received by patients. Both studies were based on practitioner interpretations of patient views rather than patient self-reports.
What are the attitudes of family carers?
Family carer attitudes have been explored within studies of initiatives to train them to administer anticipatory medications,14,22,23,56,53 a context which does not reflect standard practice in most countries. Five UK and Australian studies, of low to medium quality, reported that family carers selected for participation in initiatives found the experience of administering anticipatory medications to be acceptable,14,22,23,56,53 although an unreported proportion in one study felt overwhelmed by this expectation. 22 Family carers reported that anticipatory medications were beneficial to patient comfort14,22,23 and enabled patients to remain at home until death.22,56,53 One Australian study, of medium quality, reported on family carer administration of anticipatory medications in the context of limited access to trained nurses. Family carers felt they had no option but to administer drugs, were uncertain about the timings of medications, and feared causing an overdose or hastening death. 23 If symptoms remained uncontrolled post drug administration, family carers felt disempowered and distressed. 23 All five studies reported only on the attitudes of family carers who were willing to take on the role of administering drugs. No studies have investigated the experience of family caregivers when not involved in administering medications, which is standard practice in most countries.
What are the attitudes of community healthcare professionals?
The range of views of healthcare professionals towards anticipatory prescribing are reported in 21 studies of community, palliative care, and nursing home nurses, care home staff, pharmacists, GPs, and palliative doctors in limited geographical areas (3 rated as high quality, 13 as medium quality, and 5 as low quality).3,5,14,19,20,24,33–37,39,41,44–46,48,51,52,54,55 The majority of the studies focussed on the views and experiences of nurses.5,19,20,24,35,36,41 Only two studies explored the views of GPs in detail.3,37 The views of emergency ambulance paramedics have not been studied.
These studies suggest that healthcare professionals’ views are largely positive towards anticipatory prescribing. GPs and nurses believe it offers reassurance to patients, family carers, and healthcare professionals; provides timely and effective symptom control; and helps prevent crisis hospital admissions.5,19,24,34,39,44,48,46,52,55 The one exception is in terminal haemorrhage when specialist palliative care doctors and nurses believe anticipatory prescribing has limited value, as patients often die before medication can be given or take effect.35,36,46
Facilitators of successful anticipatory prescribing are identified in several studies. GPs and nurses generally report working well together;5,20,24 partnership is perceived to be vital, with trust between the two parties, mutual respect for each other’s expertise and ease of access to each other essential.3,24,33,37,39 GPs who are familiar with end-of-life drugs appear to be more confident about anticipatory prescribing,24,37,51,54 finding it easier to prescribe for patients they have known for some time, 3 and appear to be more likely to prescribe in a timely fashion when receiving regular updates from nurses about a patients’ changing condition. 24 The development of a rapport with patients and their families is perceived to enable sensitive anticipatory prescribing conversations to take place at an appropriate time.3,24
Negative healthcare professional views were also articulated in several studies. GPs are wary about the safety of prescribing strong injectable forms of medications ahead of need, since they are accountable for drug errors or misuse.3,24,44 Prescribing decisions were perceived to be harder when the GP does not know the patient’s situation well or there are concerns about possible drug misuse within the home.3,51 GPs also express concern about the cost of unused medications.3,5,51 Despite these potential barriers, nurses perceive that only a small proportion of GPs are reluctant to prescribe anticipatory medications.20,24,37,41,48
The administration of anticipatory medications also raises safety concerns for nurses. They do not want to administer the drugs unless it is clear that the patient is dying, and are conscious of the need to balance the achievement of effective symptom control with the avoidance of over-sedation. 19 If a patient dies soon after drug administration, particularly of opioids, less experienced nurses worry that the ‘last injection’ may have hastened their death.5,19,54 Some nurses think it too burdensome on family carers to train them to administer the injectable drugs. 14
What is its impact on patient comfort and symptom control?
Evidence of the impact of anticipatory prescribing on comfort and symptom control is limited to three observational audits and surveys of low to medium quality, none of which used symptom assessment scales. No intervention trial of clinical effectiveness has been conducted to date. One small-scale audit of family carer administration (n = 5) found carers to report that their administration of anticipatory medications had facilitated a peaceful death at home. 53 One large-scale survey of palliative care, community, and nursing home nurses found 89.6% to report that anticipatory prescribing had helped provide successful symptom relief in the cases they recalled. 20 Similarly, in a very small pre–post implementation study, 88% (n = 7) of surveyed palliative care nurses reported improved outcomes following the introduction of anticipatory prescribing. 45
Is it cost-effective?
The literature to date suggests that anticipatory prescribing is a low-cost intervention when compared to the cost of an inpatient hospital or hospice stay. 51 The typical cost of supplying 2–3 days’ medication to cover the symptoms of pain, nausea and vomiting, agitation, and breathlessness in the United Kingdom is between £22.12 48 and £30.26 per patient. 51 The net cost of unused prescribed medications is estimated to be between £10 6 and £14.61 48 per patient. Studies calculating costs derived estimates from incomplete prescribing and administration data,6,48,51 limiting the accuracy of findings.
Seven studies of low to medium quality have examined the relationship between anticipatory prescribing and service use. One study of 12 GP practices found anticipatory prescribing to be associated with an increase in GP contacts and a lower risk of hospital admission in the last month of life. 42 Two small-scale audits6,53 and one service evaluation 55 identified that most patients with an anticipatory medication prescription were not admitted to hospital for symptom control at the end of life. These studies do not report the outcomes for patients not prescribed anticipatory medications. One Canadian service evaluation 49 and three United Kingdom–based retrospective notes reviews40,42,43 identified a positive correlation between anticipatory prescribing and the proportion of patients dying at home. None of these studies accounted for confounding variables, such as the level of support from healthcare services.
Discussion
Main findings
This systematic literature review addressed six questions and identified the following findings with regards to anticipatory prescribing in the community:
Current practice varies both across countries and within the United Kingdom. There are no reliable data on how often drugs are prescribed or subsequently used in the community. In the United Kingdom, where the majority of data were identified, anticipatory prescribing appears to be widespread. Practice varies in relation to community setting, proximity of prescriptions to death, patient populations, and frequency of administration.
No studies have directly investigated the experience or views of patients.
Studies of family carers’ attitudes have been limited to evaluations of family carer administration of injectable medications. Although family carers appreciate being able to provide symptom relief, some struggle with the responsibility of assessing patient needs and administering medications. No studies have investigated family carers’ views and experiences of standard UK practice.
A large proportion of the published literature focuses on the attitudes and experience of healthcare professionals. GPs and nurses believe that it is reassuring to patients and their family carers, enables better symptom control and helps to prevent crisis hospital admissions. In addition to broadly positive professional experience, GPs and nurses also express safety concerns.
Robust evidence of clinical effectiveness is absent, as no intervention trial has been undertaken. Observations from qualitative interviews and retrospective audits suggest it may contribute to symptom relief.
Robust evidence of cost-effectiveness is also absent, although it is a low-cost intervention.
In summary, this review demonstrates a paucity of high-quality research concerning anticipatory prescribing. Most studies investigate healthcare professionals’ views or provide limited insights through retrospective case note reviews. No study has prospectively investigated the clinical effectiveness or cost-effectiveness of anticipatory prescribing. Most studies were limited to single sites, evaluated new initiatives or had selected participants, limiting their generalisability.
What this review adds
This review brings together the diverse literature in regard to anticipatory prescribing, clarifying the current knowledge base and the priority areas for future research.
Current practice is based primarily on GPs’ and nurses’ perceptions and experiences that anticipatory prescribing offers reassurance to patients and family carers and provides effective symptom control in the home setting.5,19,24,33,34,39,44,48,52,55 Although the rationale for this practice appears strong intuitively, it is unwise to base end-of-life care practice on healthcare professionals’ views alone. The views of patients and family carers must also be taken into account; 57 some may view anticipatory prescribing as an unwelcomed indicator of impending death. 24 Concerns have been raised that prescribing and administration can be paternalistic or service driven rather than tailored to patients’ wishes.7,58 Having medication at home places a significant responsibility on family carers to assess symptom control and decide when to request a healthcare professional to administer drugs.57,59,60 This responsibility is much greater when family carers are expected to administer injections:14,22,23,53 some worry that this might hasten death.22,23 Conversely, many family carers value being able to do something to relieve pain and distress.22,23,61 Patient and family carer views and experiences of anticipatory prescribing need urgent investigation.
It appears that anticipatory prescribing policies and practice are running ahead of the evidence base. There is a lack of robust evidence for its clinical effectiveness in optimising symptom control and in preventing crisis hospital admissions, alongside the lack of high quality evidence of patient and family carer experience and views. The recent call in UK end-of-life care guidance for a cluster-randomised control trial 7 may be challenging in countries such as the United Kingdom, where anticipatory prescribing is already a widespread and established practice. However, there is a clear need for well-designed clinical trials investigating the intervention’s impact on patients’ symptom control and crisis hospital admissions.
Patient safety concerns were a recurrent theme in the papers exploring the attitudes of community healthcare professionals. There is a potential for drug errors or misuse3,24,44 and recent guidance reiterates the risks of prescribing and administration being standardised rather than individualised to a patient’s needs. 7 When drugs are prescribed in hospital or hospice prior to discharge, this is not always clearly communicated with community healthcare professionals. 62 When drugs remain in the home for long periods they may no longer be appropriate. There is also the risk that immediate access to medications reduces out-of-hours doctor visits which may disadvantage patients with potentially reversible problems in need of careful medical assessment. 28 Research investigating the safety of anticipatory prescribing is urgently needed.
Limitations and strength of the review
This review sought to systematically identify and synthesise the published evidence. Supported by a professional medical librarian (I.K.), the literature search strategies covered nine pertinent databases using the majority of terms used internationally. Journal hand searches and reference and citation searches identified a further eight papers, four of which were not registered on the electronic databases searched.
The review team included published conference abstracts to ensure comprehensiveness, although all abstracts scored medium or low on Gough’s ‘WoE’ framework due to limited information on their methods.
At times, it proved difficult to separate anticipatory prescribing before symptoms arise from reactive prescribing after symptoms occur in papers describing end-of-life care practice.3,23,41 Two reviewers systematically applied the definition of ‘the prescribing of injectable medications ahead of need to control terminal symptoms’ 11 and reached consensus by discussion.
The review findings are limited to the United Kingdom, Australia, and Canada, countries whose similar healthcare systems permit synthesis of data. Although anticipatory prescribing is considered good practice internationally, published empirical research from a number of countries is scant and refers largely to the prescribing of orally and rectally administered medications.9,15–17,60
Conclusion
Anticipatory prescribing is a recommended and widespread practice in many countries, despite an inadequate knowledge base. Policy and practice are running ahead of the evidence, based largely on the belief of healthcare professionals that it reassures patients and their family carers, effectively controls symptoms and prevents crisis hospital admissions. The views and experiences of patients and their family carers have not been adequately investigated; nether has clinical effectiveness, cost-effectiveness, and safety. Our research group is planning a programme of research to help address these knowledge gaps
Supplemental Material
Supplemental_Document_1_Search_strategy_19.10.18 – Supplemental material for Anticipatory prescribing of injectable medications for adults at the end of life in the community: A systematic literature review and narrative synthesis
Supplemental material, Supplemental_Document_1_Search_strategy_19.10.18 for Anticipatory prescribing of injectable medications for adults at the end of life in the community: A systematic literature review and narrative synthesis by Ben Bowers, Richella Ryan, Isla Kuhn and Stephen Barclay in Palliative Medicine
Supplemental Material
Supplemental_Document_2_Data_Extraction_Tool_19.10.18 – Supplemental material for Anticipatory prescribing of injectable medications for adults at the end of life in the community: A systematic literature review and narrative synthesis
Supplemental material, Supplemental_Document_2_Data_Extraction_Tool_19.10.18 for Anticipatory prescribing of injectable medications for adults at the end of life in the community: A systematic literature review and narrative synthesis by Ben Bowers, Richella Ryan, Isla Kuhn and Stephen Barclay in Palliative Medicine
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: B.B. and S.B. are funded by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care (CLAHRC) East of England. R.R. is funded by the Eastern Deanery of the National Health Service. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.