
Abstract
Background:
Red blood cell transfusions are commonly used in palliative care to treat anaemia or symptoms caused by anaemia. In patients with advanced disease, there is little evidence of benefit to guide treatment decisions in the face of increased risk of harms.
Aim:
To determine national transfusion practice in hospices and compare this against National Institute for Health and Care Excellence and British Society of Haematology guidelines to develop recommendations to improve practice.
Design and Setting:
Prospective data collection on red blood cell transfusion practice in UK adult hospices over a 3-month census period.
Results:
A total of 121/210 (58%) hospices participated. A total of 465 transfusion episodes occurred in 83 hospices. Patients had a mean age of 71 years, and 96% had cancer. Mean pre-transfusion haemoglobin was 75 g/L (standard deviation = 11.15). Anaemia of chronic disease was the largest cause of anaemia (176; 38%); potentially amenable to alternative treatments. Haematinics were not checked in 70% of patients. Alternative treatments such as B12, folate and iron were rarely used. Despite transfusion-associated circulatory overload risk, 85% of patients were not weighed, and 84% had two or more units transfused. Only 83 (18%) patients had an improvement maintained at 30 days; 142 (31%) had <14 day improvement, and 50 (11%) had no improvement. A total of 150 patients (32%) were dead at 30 days.
Conclusion:
More rigorous investigation of anaemia, increased use of alternative therapies and more restrictive approach to red cell transfusions are recommended. Clinicians should discuss the limited benefit versus potentially higher risks with patients in hospice services to inform treatment decisions.
Red blood cell transfusions are commonly used in palliative care to treat anaemia or symptoms caused by anaemia despite little evidence of benefit to patients and risk of harms.
A Cochrane review of 12 observational studies found limited benefits, and approximately one-third of patients died within 2 weeks of their transfusion.
Patients are not usually investigated for the cause of their anaemia, of those that were a significant proportion would have benefitted from B12, folate or iron supplementation, although these were rarely used.
Transfusion practice remains too liberal despite greater risks of transfusion-associated circulatory overload in patients with advanced disease.
Only 18% of transfused patients had an improvement maintained up to 30 days; 42% had no or very transient benefit, and 32% were dead at 30 days.
More rigorous investigation of anaemia, increased use of alternative therapies and a more restrictive approach to red blood cell transfusions are needed.
Clinicians should discuss with patients the limited benefit versus higher risks of red blood cell transfusion in this patient group to inform treatment decisions and ensure informed consent.
Introduction
Red blood cell transfusions are used to manage the symptoms caused by anaemia, with about 7% of patients admitted to palliative care units receiving a transfusion. 1 Three systematic reviews of international literature, which generally included similar studies all of which had small sample sizes1–3 have stated that the benefits of red blood cell transfusion in palliative care patients remain unclear and that risks of harm, although not common, may be underestimated.
There are no randomised trials comparing the efficacy of red blood cell transfusion to placebo or other alternative treatments in patients with advanced disease. 2 The challenges of researching this area (particularly high placebo response rate within first week post-transfusion and inability to blind) and the need for better evidence have been well described.4,5 This results in a lack of specific guidance for the use of red blood cell transfusions in patients with advanced disease. 2
In the United Kingdom, the National Institute for Health and Care Excellence (NICE) 6 has published red blood cell transfusion guidelines for adults and recommends the use of a restrictive approach: transfusing one unit when haemoglobin falls below 70 g/L to a target concentration of 70–90 g/L. The trigger threshold is raised to 80 g/L in those who are actively bleeding, have acute coronary syndrome or chronic anaemia (as the reason for their transfusion). 6 Recent guidance from the American Association of Blood Banks (AABBs) 7 also recommends a restrictive threshold but concluded that there is insufficient evidence in some patient groups. The European Society for Medical Oncology (ESMO) 8 advocates a threshold of 70–80 g/L and recommends that transfusions are only used in anaemic patients with severe symptoms in need of rapid haemoglobin improvement.
Red blood cell transfusion carries risks of harm.9–11 Complications include acute transfusion reactions, bacterial contamination and transfusion-associated circulatory overload (TACO). TACO is cardiogenic pulmonary oedema caused by the infusion of blood products. Prospective and retrospective active surveillance studies have shown the incidence of TACO to be between 1% and 6% of patients undergoing a transfusion10,12–15 with a mortality of 6%–10%. 16
NHS Blood and Transplant (NHSBT) manages the largest programme of clinical audits in the United Kingdom which reviews the use and administration of blood components in hospitals. We aimed to describe current practice regarding red blood cell transfusion in advanced disease within UK hospices, compare current practice against NICE standards on red blood cell transfusion and make recommendations for palliative care practice.
Method
Sampling
All 210 adult hospices in England, Scotland, Wales and Northern Ireland were invited to participate in this prospective observational audit of current practice.
Data collection
Each hospice that consented to contribute was asked to nominate a clinician to collect prospective data during the 3-month observation period (September 2016–December 2016) in specifically designed audit booklets available on paper or online. These booklets requested anonymised information on patients, pre-transfusion investigations, process of transfusion, and patient outcomes at 30 days post-transfusion. A transfusion episode was defined as each patient receiving a unit(s) of red blood cells within a 24-h period.
Anonymised data were collated by the audit project manager after the closing date for data entry and prior to issuing a national report to participating sites. No patient-identifiable data were recorded on the website, so auditors were recommended to keep an audit linkage record to assist in review of cases and validation of data. Hospices were asked to validate the audit results and were given the opportunity to contact the audit project manager with details of any data entry/data transmission errors or any missing data so that the database could be corrected prior to statistical analysis for the final report. The database was amended accordingly, mainly to rectify instances of missing data.
Ethics
This audit involved the collection of routine data and no additional tests or information was requested; therefore, anonymised routine data were collected without individual patient consent (as per all NHSBT audits).
Analysis
We undertook descriptive analyses to examine pre-transfusion treatments, transfusion process and outcomes at 30-day follow-up.
Results
A total of 139/210 hospices (66%) agreed to contribute to the audit but 18 subsequently withdrew before data collection. We received data from 121 (58%) UK adult hospices, of which 83 (69%) administered at least one red blood cell transfusion during the 3-month data-collection period.
We analysed data on 465 red blood cell transfusion episodes administered at 83 sites; 38 sites confirmed they did not perform a transfusion in the audit period.
Patient characteristics
Mean patient age was 71 years and 53% were men. A pre-transfusion performance status score was recorded in 194 (42%) episodes. Australian Karnofsky Performance Scale (AKPS) was the most common scale used where maximum score is 100. Median AKPS score was 60 which represents ‘able to care for most needs; but requires occasional assistance’. Nearly all patients (448; 96%) had a cancer diagnosis, Table 1.
Cancer type breakdown (n = 448).
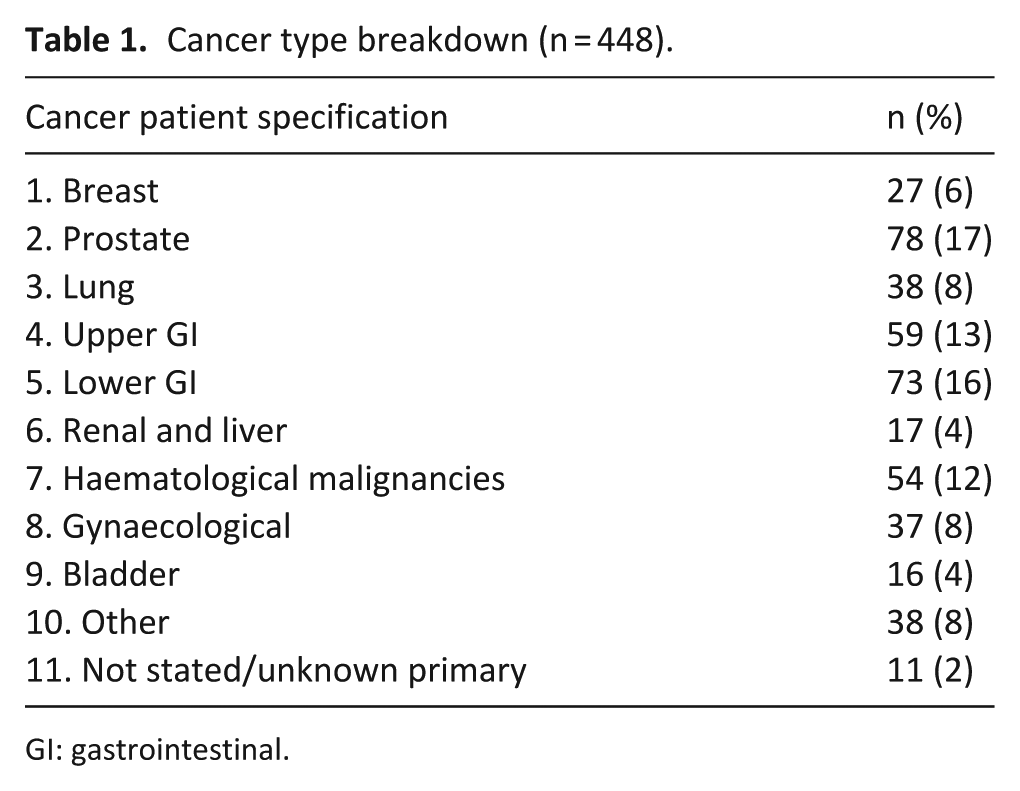
GI: gastrointestinal.
Predominant causes of anaemia were functional iron deficiency (FID; 176, 38%), active bleeding (112, 24%) and bone marrow failure (99, 21%). Causes of anaemia differed among cancer types. Blood loss was the largest cause of anaemia associated with gastrointestinal (43%), renal and bladder (44%) and gynaecological malignancies (38%). Bone marrow failure was more commonly associated with prostate (42%) and haematological malignancies (82%). A total of 326 (68%) did not receive chemotherapy, radiotherapy or immunotherapy in the previous 2 months before transfusion.
Pre-transfusion parameters
Mean pre-transfusion haemoglobin was 75 g/L (SD = 11.15 g/L); 325 (70%) patients had a haemoglobin above the trigger threshold of 70 g/L recommended by NICE (Table 2). Pre-transfusion investigations and treatments were limited. Investigations for iron deficiency or FID included ferritin (checked in 122 (26%) patients), percent hypochromic red cells (checked in 64 (14%)) and transferrin saturation (checked in 43 (9%)).
Pre-transfusion Hb (n = 465).
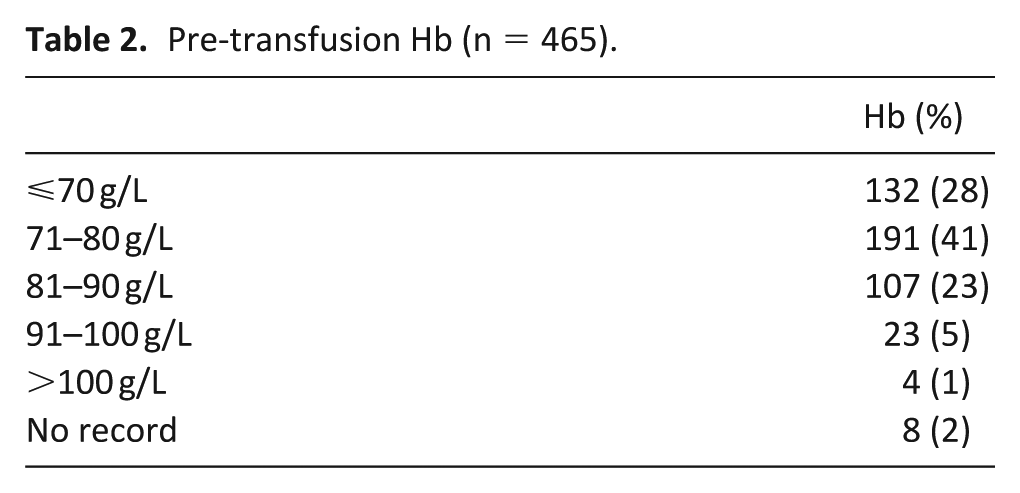
In total, 76 patients had iron deficiency or FID. This was defined as ferritin <30 ng/mL or at least 6% hypochromic red cells, or ferritin 30–100 ng/mL and estimated glomerular filtration rate (GFR) less than 45 or transferrin saturation less than 20%. 17 A further 73 patients had possible iron deficiency or FID, defined as ferritin 30–100 ng/mL or transferrin saturation less than 20% or mean corpuscular volume (MCV) <78. Iron status was not assessed in 67% (310/465) of patients. Of the 76 patients who had iron deficiency or FID, 20 were on iron and 2 were intolerant of iron. Of the 73 patients with possible iron deficiency, 17 were on iron and 2 were intolerant of iron.
Of the 102 (22%) patients who had a B12 level checked, 12% (12/102) would have benefitted from B12 injections (B12 <200 ng/L). Of the 105 (23%) patients who had a folate level checked, 41% (43/105) may have benefitted from folic acid (folate <4.5 µg/L). However, only 8% (1/12) of patients with a low B12 were on treatment with B12 injections, and only 23% (10/43) of patients with a low folate level were on treatment with folic acid.
Three patients were treated with erythrocytosis-stimulating agent therapies, despite the fact that 66 patients had a moderate or severe reduction in renal function. Five patients were treated with tranexamic acid which is known to reduce blood loss, 18 despite 25% (117/465) of patients having active or recent blood loss.
Transfusion process
Most (301; 65%) transfusion episodes were performed as in patients, and the majority of patients were transfused for low haemoglobin (237; 51%) or a combination of breathlessness and low haemoglobin (182; 40%). Fatigue (75; 16%) was the third most common indication. The mean and median number of units of blood transfused was two.
Despite a national recommendation that all patients are weighed, 6 only 68 (15%) of patients were weighed before transfusion; 44 (64%) of patients weighed less than 70 kg. Most patients (390; 84%) were transfused two or more units of red cells and 333 (72%) did not have their haemoglobin checked in between units or post-transfusion. Clinical observations were undertaken in 95% of patients before, within 15 min of transfusion commencement and at 60 min post-transfusion.
Patient outcomes at 30 days post-transfusion were reported by clinicians (Table 3). Performance status was not measured in 399 (86%) patients. A total of 53 (14%) patients had a pre- and post-transfusion performance status recorded. A variety of performance status scales were used, but overall, 9 (17%) had an increase in performance score, 23 (43%) had no change and 21 (40%) had a lower score; in total, 83% showed no improvement in performance status within the 30-day post-transfusion period.
30-day outcome (n = 465).
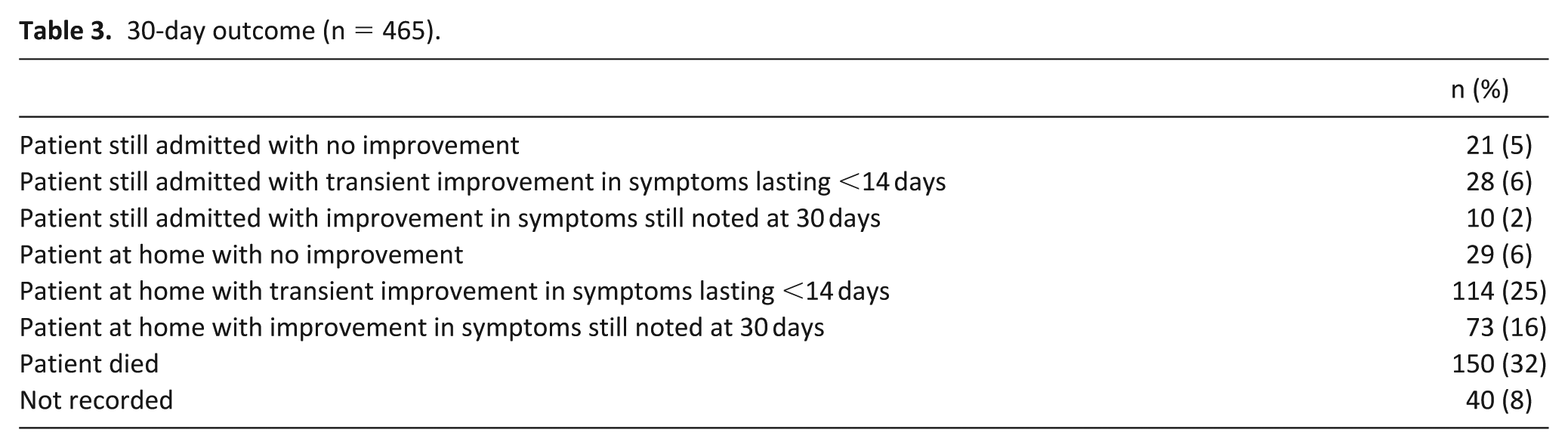
Overall, 83 (18%) of patients were considered to have experienced sustained benefit for up to 30 days after red blood cell transfusion (Table 3); 142 (31%) had a transient improvement (<14 days) and 50 (11%) had no improvement; 150 patients (32%) were dead at 30 days. Benefit was assessed by the clinician or by change in performance status score; however, post-transfusion performance status was only recorded in 53 patients. Patient-reported benefit could not be ascertained, as we could not request that patients were asked additional questions.
Discussion
This is the largest prospective observational cohort of red blood cell transfusion in palliative care published to date, and representative of UK hospice practice. A recent multinational prospective observational study included 101 cases with a 7day follow-up; 19 we include 465 cases with a 30-day follow-up. The participation of 121 (58%) UK hospices demonstrates how pertinent this topic is to palliative care physicians. While the data were collected in hospices, we believe that the results are generalisable to other general medical patients with advanced disease.
Overall, we found that patients had inadequate investigation and treatment before transfusion. If anaemia is poorly investigated, it is unlikely that alternative and more targeted treatments will be explored. B12 or folate deficiency that is associated with a severe anaemia also causes a cardiomyopathy. A red blood cell transfusion in this situation can cause life-threatening TACO, whereas treatment with B12, folate or both can cause a rise in the haemoglobin within 7–10 days. 20 Treating iron deficiency with intravenous iron in people with heart failure can significantly increase quality of life, exercise capacity and symptoms of heart failure. 21 Intravenous iron is recommended within ESMO guidelines; 8 however, local availability, local guidance and the appropriateness of this therapy should be considered.
Many patients had anaemia due to ongoing blood loss. Tranexamic acid has been shown in other patient groups to reduce blood loss without increasing the risk of thrombosis, 18 though its use in urinary blood loss is less strongly evidenced and not recommended. 22 Alternative treatments to red blood cell transfusion in patients with blood loss may be more clinically cost-effective, with reduced risk of harm. It has been estimated that a unit of red blood cells costs £170, 23 with an additional cost of £49 to administer the unit. 24 A study looking at the clinical and financial impact of using alternative treatments for anaemia is needed.
Transfusion practice was more liberal than evidence-based guidelines suggest is effective and safe.6,25 For example, we found that the mean pre-transfusion haemoglobin was 75 g/L; 82% had haemoglobin above the 70 g/L threshold recommended by NICE, and 32% had haemoglobin above 80 g/L (the NICE recommended threshold for patients with acute coronary syndrome).
We identified that risk factors for TACO appeared not to be considered prior to transfusion such as patients’ weight and other biochemical parameters (Appendix Serious Hazards of Transfusion (SHOT) TACO risk assessment 9 ). TACO is more common with rapid or large volume infusions but can be triggered by less than one unit. 9 Patients treated in hospices commonly have risk factors for TACO which include hypo-albuminaemia, low body weight, being physiologically compromised by cardiac, respiratory or renal insufficiency, as well as older age.9–11 Symptoms of TACO are non-specific and include dyspnoea, cyanosis and tachycardia which can be mistaken for deterioration of underlying advanced disease. 11 One study across 157 UK hospitals showed that 4.3% of inpatients aged over 60 years developed increasing respiratory distress after transfusion, but only one-third of patients who were diagnosed with TACO by the hospital were reported to the SHOT Haemovigilance Group. 26 Patients should therefore receive a weight-related transfusion which may be less than one unit if the patient weighs less than 70 kg. Recent international guidance 7 advises that ‘if there is no substantial benefit associated with the transfusion, it is best not to expose the patient to rare but potentially serious risks associated with red cell transfusion’ a sentiment echoed by NICE 6 who states that ‘some patients are transfused unnecessarily, which is wasteful of a scare and costly resource and put patients at unnecessary risk’.
Most (392; 84%) patients had more than one unit given in the transfusion episode and without checking haemoglobin after each unit, which is recommended to reduce risk of complications. 9 NICE 6 recommends monitoring for effect by checking haemoglobin post-transfusion and restricting transfusion rate to no more than one unit per 24 h. Few patients had a post-transfusion assessment of haemoglobin (28%) or performance status (14%), and no standardised symptom assessment scales were used.
Most importantly, we found evidence that benefits of red blood cell transfusion appear to be very limited in this population of patients with advanced disease; at 30 days post-transfusion, only 18% appeared to have sustained benefit, while 32% had died indicating poor patient selection or increased mortality from blood transfusion. These findings are consistent with a Cochrane review of red blood cell transfusion in advance, 1 which found that subjective response rate varied between 31% and 70%; fatigue improved initially but deteriorated by day 14.27–30 Similar results were found for breathlessness. A significant proportion of these participants (23%–35%) died within 2 weeks of their transfusion. 1
Audit feedback
Each hospice was sent the report which is also published on the NHSBT website. We have developed a piktograph which will be available via the NHSBT website to disseminate audit recommendations. We have presented the findings at a national palliative care conference and are currently developing further educational tools with NHSBT specifically for hospices as part of a national education programme. We aim to re-audit hospices after implementation and disseminating of the education plan.
Limitations
Participation was voluntary, and each site had a designated data collector whom we relied on for correct reporting. This in turn depends on good documentation in clinical notes. We provided a data-support officer during the data-collection period to try and ensure that the most correct and complete data were gained and to validate their final audit data and resolve missing data queries. Data were only collected in hospices; therefore, there may be aspects of transfusion practice in palliative care that we have not captured. For pragmatic reasons, we limited our census to a 3-month period; a larger response rate and a longer census period might have captured a larger sample though it is unclear whether this would substantially alter our findings. We collected outcomes at 30 days post-transfusion because we considered this would provide sufficient time to observe benefit. However, outcomes were based on subjective clinical opinion and not patient-reported outcome measures. We did not collect data on complications or adverse events following blood transfusion, so we cannot draw conclusions about whether actual harm came to any of our cohort. We did not record cardiac comorbidities so cannot estimate which NICE threshold would apply in individual cases.
Implications for practice
Our large prospective study confirms the conclusions of previous systematic reviews1–3 and demonstrates that practice remains too liberal when judged against international evidence-based guidelines, which in turn exposes patients to an increased risk of harm and consumes more resources. In addition, inadequate investigation of underlying causes of anaemia and the poor response rate to red blood cell transfusion should prompt a reconsideration of the need for, and practice related to, red blood cell transfusion practice in palliative care contexts.
Based on our data, we developed practice guidelines for red blood cell transfusion in conjunction with NHSBT which are consistent with guidance from NICE 6 and from the British Committee for Standards in Haematology 25 (see Appendix 1). We propose that these are adopted by hospice and palliative care units to encourage alternative strategies for managing patients with anaemia and reducing risk of harm from red blood cell transfusions.
Footnotes
Appendix
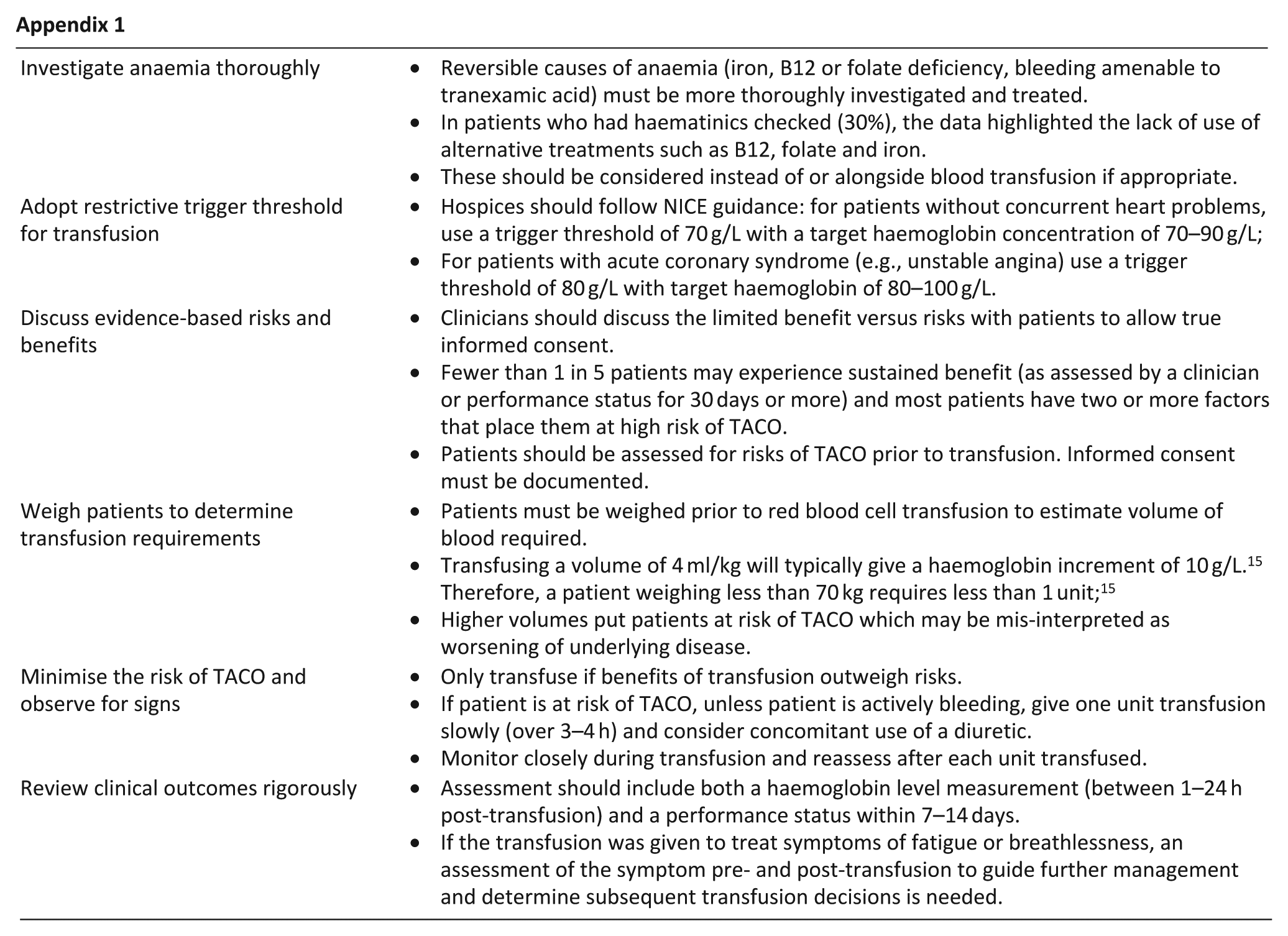
| Investigate anaemia thoroughly | ● Reversible causes of anaemia (iron, B12 or folate deficiency, bleeding amenable to tranexamic acid) must be more thoroughly investigated and treated. ● In patients who had haematinics checked (30%), the data highlighted the lack of use of alternative treatments such as B12, folate and iron. ● These should be considered instead of or alongside blood transfusion if appropriate. |
| Adopt restrictive trigger threshold for transfusion | ● Hospices should follow NICE guidance: for patients without concurrent heart problems, use a trigger threshold of 70 g/L with a target haemoglobin concentration of 70–90 g/L; ● For patients with acute coronary syndrome (e.g., unstable angina) use a trigger threshold of 80 g/L with target haemoglobin of 80–100 g/L. |
| Discuss evidence-based risks and benefits | ● Clinicians should discuss the limited benefit versus risks with patients to allow true informed consent. ● Fewer than 1 in 5 patients may experience sustained benefit (as assessed by a clinician or performance status for 30 days or more) and most patients have two or more factors that place them at high risk of TACO. ● Patients should be assessed for risks of TACO prior to transfusion. Informed consent must be documented. |
| Weigh patients to determine transfusion requirements | ● Patients must be weighed prior to red blood cell transfusion to estimate volume of blood required. ● Transfusing a volume of 4 ml/kg will typically give a haemoglobin increment of 10 g/L. 15 Therefore, a patient weighing less than 70 kg requires less than 1 unit; 15 ● Higher volumes put patients at risk of TACO which may be mis-interpreted as worsening of underlying disease. |
| Minimise the risk of TACO and observe for signs | ● Only transfuse if benefits of transfusion outweigh risks. ● If patient is at risk of TACO, unless patient is actively bleeding, give one unit transfusion slowly (over 3–4 h) and consider concomitant use of a diuretic. ● Monitor closely during transfusion and reassess after each unit transfused. |
| Review clinical outcomes rigorously | ● Assessment should include both a haemoglobin level measurement (between 1–24 h post-transfusion) and a performance status within 7–14 days. ● If the transfusion was given to treat symptoms of fatigue or breathlessness, an assessment of the symptom pre- and post-transfusion to guide further management and determine subsequent transfusion decisions is needed. |
Acknowledgements
K.N. participated in the initial concept of audit, design of project, interpretation of data, first draft of paper and revision and approved the version to be published. R.G. participated in the design of project, analysis and interpretation of data, revision of paper and approved the version to be published. J.G.-C. participated in the design of project, analysis and interpretation of data, revision of paper and approved the version to be published. L.E. participated in design of project, interpretation of data, revision of paper and approved the version to be published. C.M. participated in the design of project, interpretation of data, revision of paper and approved the version to be published. J.W.B. participated in the design of project, interpretation of data, revision of paper and approved the version to be published. M.I.B. participated in the initial concept of audit, design of project, interpretation of data and revision of paper and approved the version to be published.
Data management and sharing
Data can be obtained from J.G.-C., the Programme Manager for the National Comparative Audit of Blood Transfusion. He can be contacted by email at
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by the National Comparative Audit in Blood Transfusion which is funded by NHSBT; however, there was no specific grant or award associated with the audit.
Research ethics and patient consent
As this was an audit-specific study, patient consent was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.