
Abstract
Background:
To enable coordinated palliative care delivery, all clinicians should have basic palliative care skill sets (‘generalist palliative care’). Specialists should have skills for managing complex and difficult cases (‘specialist palliative care’) and co-exist to support generalists through consultation care and transfer of care. Little information exists about the actual mixes of generalist and specialist palliative care.
Aim:
To describe the models of physician-based palliative care services delivered to patients in the last 12 months of life.
Design:
This is a population-based retrospective cohort study using linked health care administrative data.
Setting/participants:
Physicians providing palliative care services to a decedent cohort in Ontario, Canada. The decedent cohort consisted of all adults (18+ years) who died in Ontario, Canada between April 2011 and March 2015 (n = 361,951).
Results:
We describe four major models of palliative care services: (1) 53.0% of decedents received no physician-based palliative care, (2) 21.2% received only generalist palliative care, (3) 14.7% received consultation palliative care (i.e. care from both specialists and generalists), and (4) 11.1% received only specialist palliative care. Among physicians providing palliative care (n = 11,006), 95.3% had a generalist palliative care focus and 4.7% a specialist focus; 74.2% were trained as family physicians.
Conclusion:
We examined how often a coordinated palliative care model is delivered to a large decedent cohort and identified that few actually received consultation care. The majority of care, in both the palliative care generalist and specialist models, was delivered by family physicians. Further research should evaluate how different models of care impact patient outcomes and costs.
Keywords
In a palliative care model where coordination of care exists between physicians, all clinicians (including family physicians, oncologists and other medical and surgical specialists) should have the basic palliative care skill sets to provide ‘generalist palliative care’. Specialists should have skills for managing more complex and difficult cases, providing ‘specialist palliative care’. Palliative care specialists should support generalists through consultation palliative care and transfer of care (i.e. care transferred prior to death to a specialist palliative care physician) where indicated.
Research using health administrative databases can provide important insights into the models of physician-based palliative care.
We operationalized a physician-based palliative care model as: low engagement (i.e. no physician palliative care services), generalist palliative care only, consultation palliative care (i.e. generalist and specialist palliative care) and specialist palliative care only.
In a large population-level decedent cohort (n = 361,951) in Ontario, Canada, we show that most decedents (53.0%) received no physician-based palliative care, while only 14.7% received consultation palliative care. Palliative care specialists reached only 25.8% of all decedents.
Only 37.5% of practicing physicians delivered palliative care. Nearly three-quarters (74.2%) of palliative care is provided by family physicians, who either have a generalist or specialist palliative care focus of practice.
A continued shift towards a public health approach in palliative care that emphasizes the importance of primary care – supported by consultation with palliative care specialists – will likely be needed to help increase the reach of physician-based palliative care services.
Further research is needed to evaluate how different models of palliative care impact patient outcomes, costs and system capacity.
Introduction
Palliative care is an approach to alleviate physical, psychosocial and spiritual suffering in patients and their families facing a life-threatening illness. 1 Despite the potential need for palliative care in our ageing population, a large proportion of decedents both in Canada and internationally may not be receiving these services.2,3 Quill and Abernethy 4 present a coordinated palliative care model to increase access: this model distinguishes primary-level palliative care (i.e. skills that all clinicians should have or ‘palliative care generalists’) from speciality-level palliative care (i.e. skills for managing more complex and difficult cases or ‘palliative care specialists’). Physicians delivering palliative care at a generalist or specialist focus of practice may be initially trained as family physicians or medical/surgical specialists. As patients progress closer to death, a patient’s growing needs may be met by shared care between palliative care generalists and specialists through consultation or through transfer of care to specialists for complex cases.4,5
In some countries like the United Kingdom, 6 the United States 7 and most European countries, 8 palliative care is a clearly defined physician speciality involving formal training and accreditation. Although advanced training for physicians who wished to develop speciality-level palliative care skills has existed in Canada for about 25 years and accredited programmes for the last decade or so, palliative care was only recently recognized as a formal sub-speciality by both the College of Family Physicians of Canada (CFPC) and the Royal College of Physicians and Surgeons of Canada (RCPSC). 9 The majority of physicians who practice palliative care in Canada today are certificants of the CFPC and hence often identified in administrative databases as family physicians.
The World Health Organization (WHO) 10 has recommended that specialist palliative care to be only one component of palliative care service delivery. Approximately three-quarters of all decedents can benefit from a palliative care approach, 11 yet not all dying individuals require a specialist. To improve its reach and sustainability, palliative care needs to be integrated into primary care services, which includes a wide range of providers such as nurses, personal support workers, social workers, primary-level palliative care physicians and other allied health professionals. While non-physician health professionals internationally play varying important roles for the provision of palliative care, in Canada during our study period, only physicians could prescribe regulated medications such as opioids and benzodiazepines for relief of symptoms such as pain and nausea. They also often act to coordinate care. Physicians are thus often integral members of the palliative care team as death approaches.
In order to maximize constrained health care resources and to provide high-quality care for our increasingly ageing population, public payers (such as the provincial governments in Canada) must be knowledgeable about the types of physician palliative care delivery models available, as well as their effectiveness. Little population-level information exists, however, about the mixture of generalist and specialist palliative care, including what levels of palliative care (i.e. primary-level vs specialist-level) physicians are actually delivering such care.
This study operationalizes a theoretical coordinated palliative care model, such as one presented by Quill and Abernethy, 4 to describe how palliative care is being delivered by physicians in Ontario, Canada. It can be used as a reference to other countries to compare palliative care physician models and to inform access and human resources planning activities. It builds upon previous work done in this area by three of the authors, 12 and it is also partially inspired by previous research on developing a shared care typology for people living with HIV. 13
Methods
Operationalization of a physician-based palliative care model
To establish an operational model of physician-based palliative care, we conducted interviews with palliative care experts in Ontario, Canada, who represented clinical, research and advocacy aspects of care delivery. We prompted discussion on the current organization of physician-based palliative care models. Specifically, we discussed aspects of physician practice focus (i.e. palliative care specialists and generalists), physician medical speciality (i.e. family physician vs medical or surgical specialist), setting of care (i.e. hospital versus office vs patient’s home) and timing of care in relation to death.
We identified eight experts representing palliative care providers (both physicians and nurses) and researchers as well as a ninth expert in developing models of shared care using health administrative databases. This was a purposive sample representing diverse expertise from Ontario, Canada, the province of our decedent and physician cohort. Eight of the nine invited experts (88.9%) participated. Three teleconference interviews (n = 7), which lasted approximately 60 min each, were conducted and one set of written feedback (n = 1) was received between 20 January and 3 February, 2017.
Until 2014, the identification of physicians with advanced palliative care training in Canada was complex as there was no formal designation of palliative care as a unique speciality.9,14 As such, there is no ability to identify ‘palliative care specialists’ through administrative databases. The majority of palliative care specialists in Canada often pursue formal fellowship training in palliative care (e.g. 1-year training following completion of family medicine residency), and a minority obtain informal training through electives and/or continuing medical education. Our palliative care experts recommended using a previously validated algorithm for Ontario, Canada, 15 to identify ‘palliative care specialists’, defined as physicians with a focussed practice in palliative care with greater than 10% of total billings as palliative care. This billing-based definition has previously been found to be 76.0% sensitive and 97.8% specific to self-identification as a physician with a specialized palliative care focus in practice, many of whom have advanced training in palliative care. 15 All other physicians providing palliative care services, but whose total billings as palliative care was less than 10% was considered a ‘palliative care generalist’. This included both family physicians as well as medical and surgical specialists (e.g. medical oncologist or internist).
The model parameters evolved in an iterative fashion, as we modified the contents and inclusion criteria based on the experts’ feedback. After each feedback session, the draft model was revised before being shared with the next panel of experts. The purpose of this exercise was to balance face validity (i.e. attempts to reflect what is actually happening for palliative care service) and generalizability (i.e. sacrificing overly complex subgroups, such as settings and temporality of care).
The operationalized palliative care model represents the tenth iteration (Figure 1). It broadly outlines four major models of physician-based palliative care:
Low engagement. No physician palliative care services received prior to death.
Generalist palliative care. Palliative care provided only by physicians with a generalist palliative care focus of practice.
Consultation palliative care. Palliative care received from both generalist and specialist palliative care physicians.
Specialist palliative care. Palliative care provided only by physicians with a specialist palliative care focus of practice.
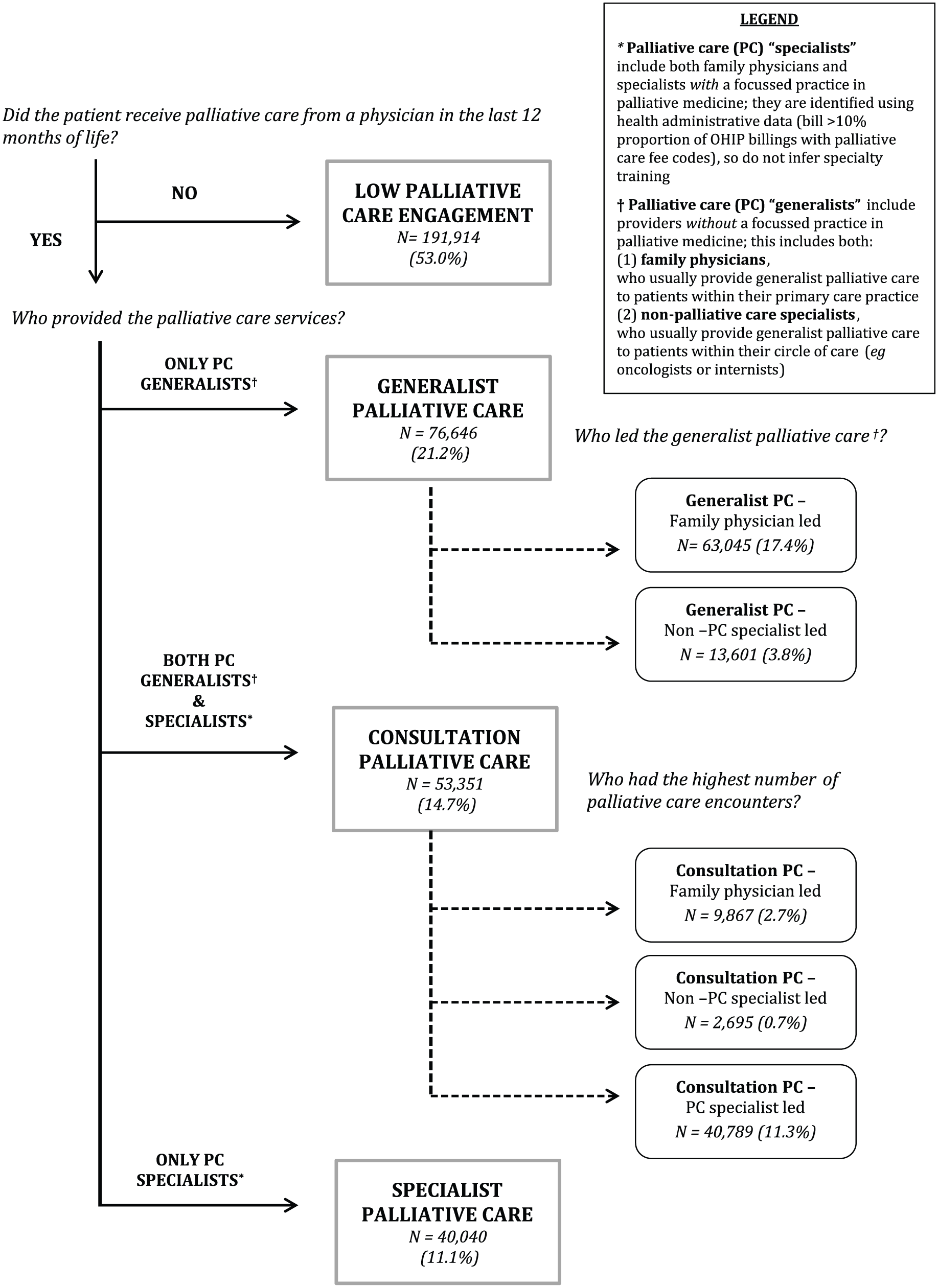
Typology of physician-based palliative care services with decedent population in Ontario, Canada from April 2011 to March 2015.
Retrospective cohort study characterizing physician-based delivery of palliative care
We examined how the operationalized palliative care model is actually being delivered in a population with universal health care coverage for physician services.
Study population
Our study relied on linked, administrative health data held at the Institute for Clinical Evaluative Sciences (ICES). Within ICES, encrypted health card numbers were used to link patient-level information across several health administrative databases, which contains service encounter information from primary, secondary and tertiary care settings.
We included all adult decedents (18+ years) in Ontario, Canada, over a 4-year period (1 April 2011 to 31 March 2015). Decedents were excluded if they were younger than 18 years or older than 105 years, or if they were ineligible for coverage under the provincial health insurance plan (i.e. the Ontario Health Insurance Plan (OHIP)) in the last year preceding death. As a universal health system, all Canadian citizens, permanent residents or landed immigrants living in Ontario are eligible for coverage under the provincial health plan. Subsequently, we identified all physicians who provided palliative care services to each decedent in this period.
Data sources
We used the Ontario Registered Person’s Database (RPDB) – a registry of all Ontarians who are eligible for OHIP coverage, containing birth and death dates – to identify decedents. We used the OHIP database to capture physician care to our decedent cohort during their last 12 months of life. OHIP contains billing data for all services covered under the provincial health insurance programme (including all palliative care services) and captures the vast majority of all physician services. It excludes physicians at community health centres, who are salaried and provide primary care to about 2% of Ontario’s population 16 and services provided by nurse practitioners and physician assistants.
Physician characteristics were identified from the Physician Database and Corporate Provider Database (CPDB). First, we categorized physicians by medical speciality type as either ‘family physician’ (i.e. family physician or general practitioner) or ‘specialist’ (i.e. medical or surgical specialist). Second, we classified physicians by their palliative focus of practice as ‘palliative care generalists’ or ‘palliative care specialists’. Given that no codes to identify formally designated palliative care physicians existed during our study cohort, we used Barbera et al.’s 15 previously validated algorithm to identify ‘palliative care specialists’, defined as those with a focussed practice in palliative care with greater than 10% of total billings as palliative care. ‘Palliative care generalists’ are physicians who provide palliative care services, but this is not a major focus (<10% of total billings) of their practice. We further subdivided ‘Palliative care generalists’ into ‘family physicians’ (i.e. family physicians and general practitioners certified through the CFPC) and ‘non-palliative care specialists’ (i.e. medical and surgical specialists certified through the RCPSC).
We categorized individual encounters as palliative care services if the billing code was considered a physician palliative care service (Appendix 1). This included direct patient care such as palliative care encounters in acute care hospitals, nursing and chronic care hospitals, community outpatient clinics and home visits as well as indirect patient care such as counselling a relative, telephone management and weekly palliative care case management. All home visits in the last 3 months prior to death, regardless as to whether billed specifically as a ‘palliative’ service, were considered to be a physician palliative care service given these are patient-centred care provision usually to individuals with a life-threatening illness.
Data analysis
These datasets (RPDB, OHIP, CPDB) were linked using unique encoded identifiers and analysed at the ICES. We determined whether a decedent received palliative care services from a physician during the last 12 months of life. If so, we determined the physician’s palliative care focus and medical speciality (see Appendix 1 for details). We then sorted decedents into one of the four main models described in our framework: low engagement, generalist palliative care, consultation palliative care or specialist palliative care.
We describe characteristics of physicians delivering palliative care – including age, sex, rurality, year of graduation, country of medical school graduation and speciality – from the time of latest record of contact with a decedent in our study cohort. As the validated algorithm depends on the proportion of palliative care billing claims over a 2-year period, 15 we applied a 2-year look-back window from each health care encounter to determine a physician’s palliative care focus at each encounter. As a physician’s practice is likely to evolve over time, their palliative care focus could differ between different palliative care encounters. For this analysis, physicians who transitioned between a generalist and specialist palliative focus of practice during the observation period were counted with the group with their greatest proportion of contacts. We reported descriptive data, including means and standard deviations, across all physician-based variables. Statistical significance was set a priori at p < 0.05. All analyses were conducted using SAS Enterprise Guide 7.1 (SAS Institute Inc., Cary, NC).
Ethical approval, consent and reporting
This study received ethical approval from the Sunnybrook Health Sciences Centre (Toronto, Canada) and the Ottawa Hospital Research Institute (Ottawa, Canada). Given this study used health administrative data, no consent was required from individual decedents or physicians. To ensure the protection of the patients’ identity, cells that contain six or fewer observations were not reported.
Results
Retrospective cohort study characterizing decedents and palliative care physicians
We identified 361,951 adult decedents in Ontario between 1 April 2011 and 31 March 2015. Over half (53.0%, n = 191,914) received no physician services billed as palliative care in the last 12 months of life, 21.2% (n = 76,646) received only generalist palliative care, 11.1% (n = 40,040) received only specialist palliative care and 14.7% (n = 53,351) received consultation palliative care. Within the generalist palliative care, more family physicians led care (i.e. had more palliative care encounters) than non-palliative care specialists. Within consultation palliative care, palliative care specialists led care in 76.4% of decedents receiving such care. Figure 1 shows the final model with decedent population distribution.
Table 1 describes the characteristics of physicians providing palliative care services in Ontario, Canada, broken down by focus of practice and physician speciality. Of the 29,343 practicing physicians in Ontario over our study period, 11,006 (37.5%) delivered palliative care services to our decedent cohort. In total, 95.3% of physicians delivering palliative care had a generalist palliative care focus and 4.7% had a specialist palliative care focus. Among physicians who provided palliative care, nearly three-quarters are family physicians (74.2%) and the remainder are from a broad spectrum of specialties including general internal medicine (8.3%), medical and radiation oncology (3.1%) and general surgery (2.1%).
Characteristics of physicians providing palliative care services to adult decedents in their last year of life (n = 361,951) in Ontario, Canada, April 2011 to March 2015.
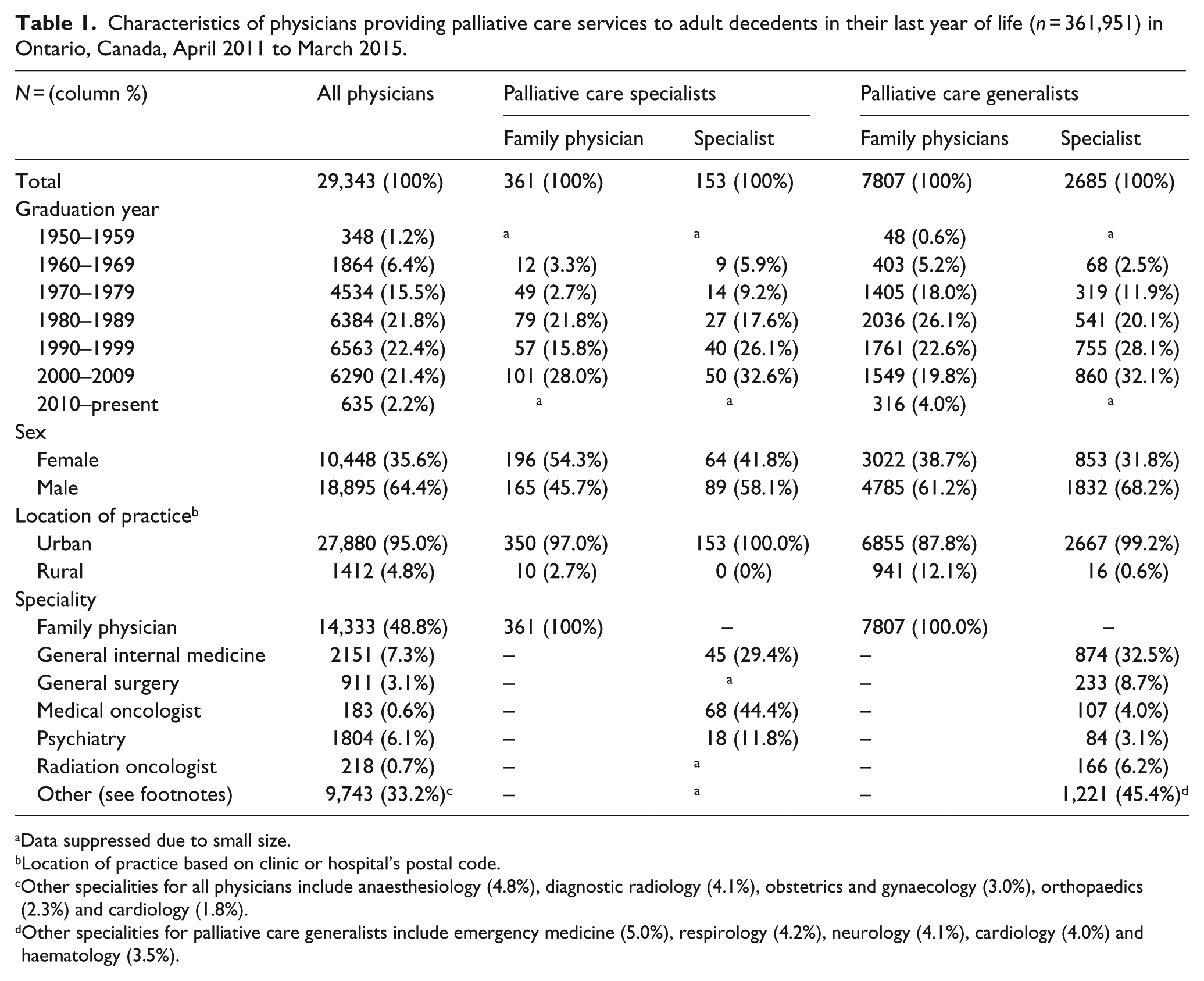
Data suppressed due to small size.
Location of practice based on clinic or hospital’s postal code.
Other specialities for all physicians include anaesthesiology (4.8%), diagnostic radiology (4.1%), obstetrics and gynaecology (3.0%), orthopaedics (2.3%) and cardiology (1.8%).
Other specialities for palliative care generalists include emergency medicine (5.0%), respirology (4.2%), neurology (4.1%), cardiology (4.0%) and haematology (3.5%).
Male physicians provided the majority of palliative care services, with the exception of family physicians who have a specialist focus of palliative care. Only 12.1% of palliative care generalists and 2.7% of palliative care specialists worked in a rural practice. Predominantly, family physicians with both a generalist and specialist focus of palliative practice delivered rural palliative care as over 99% of medical and surgical specialists provided palliative care in an urban practice.
Discussion
Main findings
We operationalized a physician-based palliative care delivery model and described its application to a population-based decedent cohort. We identified four models of physician-based palliative care: low engagement, generalist palliative care, consultation palliative care and specialist palliative care. The vast majority of physicians who provide palliative care services had a generalist palliative care focus, with fewer than 5% having a specialist palliative care focus. Not surprisingly, although they may have received other physician services, more than half of the Ontario decedent population (53.0%) did not have a single palliative care encounter with a physician. As underlined by Quill and Abernethy, 4 all physicians should be able to deliver primary-level palliative care to increase the reach of these services. We have also shown that family physicians, with either a generalist or specialist palliative focus of practice, delivered the vast majority of palliative care, which likely reflects in part how palliative care was historically delivered in Canada.
A gap in physician palliative care services exists between urban and rural populations, with only 10 out of 514 palliative care specialists practicing in rural communities, where about 1 in 7 decedents reside. 17 Furthermore, care delivered in a rural location is nearly exclusively being delivered by family physicians, a finding also noted in Australia, a country that shares with Canada having its population spread across a large geographical landmass. 18 In our study, less than 1% of medical or surgical specialists have a rural location of practice. Previous analyses of a similar population cohort demonstrated that being older, living in poorer and rural neighbourhoods and having a non-cancer diagnosis were all associated with a lower odds of palliative care receipt. 2 The average age of both palliative care generalists and specialists was over 50 (data not shown), which underscores the need to ensure physician trainees and young physicians develop competence in palliative medicine.
This study demonstrates that generalists palliative care providers currently play a key role in the provision of these services in Ontario, Canada. There is limited human resource capacity to deliver physician palliative care through a specialist-only model, given that palliative care specialists in Ontario, Canada, see 25.8% of all decedents, of which a majority (14.7% in consultative care vs 11.1% in specialist only care) was done in conjunction with a generalist. Ideally, all physicians should have primary-level palliative care skills such as basic management of pain and symptoms; basic management of depression and anxiety; basic discussions about prognosis, goals of treatment and suffering.4,19,20 Only 37.5% of all physicians, however, who cared for our decedent cohort delivered palliative care services. There is certainly scope to increase the reach of physician palliative care services by encouraging all physicians, including medical and surgical specialists, to provide primary-level palliative care (e.g. cardiologists for end-stage heart failure or medical and radiation oncologists for metastatic cancer). Family physicians and nurse practitioners, who are often already providing years of primary care for their patients, are uniquely positioned to provide continuous care as a patient faces a life-threatening illness. For more complex cases, this care can be supplemented with expertise from palliative care specialists.
We are not aware of existing population-based studies within or outside of Canada looking at the mixture of physician-based palliative care services, including a breakdown of primary-level and specialist-level palliative care. Given that increasing access to palliative care is a priority in many countries, these data can serve as a reference for other countries. Replicating this study’s methods in other countries will allow them to compare how the physician-based model is associated with patient access to palliative services. Future studies can evaluate the effectiveness of these physician-based models on health care costs and health care outcomes, such as emergency room visits or hospitalizations in the last month of life, as well as other models of community-based palliative care, such as services provided by nurse practitioners and physician assistants. With an ever-growing demand for increased palliative care services in all countries, there is an urgent need to implement shared care models that align with WHO recommendations. This approach has the greatest potential to increase reach of physician palliative care services to the widest number of individuals.4,19,20
Limitations
First, the model we have described may not accurately reflect other jurisdictions with vastly different health care systems, health human resources and infrastructure for palliative care. Nevertheless, we would expect that most developed countries and many developing countries would have physicians with primary-level and speciality-level palliative care expertise. Second, while palliative care is increasingly being delivered through inter-professional teams, the datasets used in this study do not capture care provided by non-physician providers such as registered nurses and nurse practitioners. In our study, decedents in the ‘low engagement’ model may have received nursing palliative care support including home care, despite not receiving any physician palliative care.
Third, formal designation of palliative care physicians in Canada was only implemented recently, after the years included in our decedent cohort. As such, our study used proportion of total billings to identify palliative care specialists. While Barbera et al.’s 15 algorithm is very specific (97.8%), it is only moderately sensitive (76%) and may have underestimated the number of physicians providing speciality-level palliative care. Fourth, given that data used were collected for administrative rather than clinical purposes, we have limited information regarding a patient’s palliative care needs and how they evolve over time and the quality of care being delivered. For example, the administrative data cannot inform us on whether the palliative care physicians with a specialist focus of practice are providing primary-level palliative care along with specialist-level palliative care. For the consultation palliative care model, we also do not have information about which physician is truly leading the majority of care, and there may be undocumented or informal interactions between health care providers such as telephone or e-mail consultations.
Finally, other studies have shown administrative data may be influenced by under-coding of palliative care services rendered. 21 As we used billing codes specific to palliative care, patients may have received physician palliative care services that fell under another billing code and are therefore not captured in the database (e.g. a family physician bills an intermediate assessment as multiple issues are addressed at an outpatient community visit, which could include palliative care), so we may have underestimated these services.
Conclusion
We operationalized a physician-based palliative care model that can be used to understand how generalist and specialist palliative care physicians deliver services at a population level. We demonstrate how routinely collected, health administrative databases can be used for these purposes. This model has already been useful to understand the types of physician palliative services decedents in Ontario, Canada, are receiving during their last 12 months of life, and importantly, where the gaps in care may lie. Future research should evaluate whether the physician-based model of palliative care described here impact health care outcomes, including health care costs, number of emergency room visits or hospitalizations in the last few weeks of life.
Footnotes
Appendix 1
Acknowledgements
We appreciate the expert advice provided by Drs Lisa Barbera, Michelle Howard and Ahmed Jakda in the operationalization of the physician-based palliative care model. C.R.L.B. and P.T. are the co-lead authors; the other authors are involved with all stages in the conceptualizing and editing of this article. This includes design and conception or analysis and interpretation of the data, drafting or revising for intellectual content, and final approval of the version submitted for publication.
Data management and sharing
All our data are held at the Institute for Clinical Evaluative Sciences (ICES).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by the Institute for Clinical Evaluative Sciences (ICES), which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). We also received an additional research grant from the MOHLTC to perform this work. The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred.
Research ethics and patient consent
This study received ethical approval from the Sunnybrook Health Sciences Centre (Toronto, Canada) and the Ottawa Hospital Research Institute (Ottawa, Canada). Given this study used health administrative data, no consent was required from individual decedents or physicians.