
Abstract
Background:
Interprofessional specialized palliative care teams at home improve patient outcomes, reduce healthcare costs, and support many patients to die at home. However, practical details about how to develop home-based teams in different regions and health systems are scarce.
Aim:
To examine how a variety of home-based specialized palliative care teams created and grew their team over time and to identify critical steps in their evolution.
Design:
A qualitative study was designed based on a grounded theory approach, using semi-structured interviews and other documentation.
Setting/Participants:
In all, 15 specialized palliative care teams from Ontario, Canada, representing rural and urban areas. Data were collected from core members of the teams, including nurses, physicians, personal support workers, spiritual counselors, and administrators.
Results:
In all, 122 individuals where interviewed, ranging from 4 to 10 per team. The analysis revealed four stages in team evolution: Inception, Start-up (n = 4 teams), Growth (n = 5), and Mature (n = 6). In the Inception stage, a champion provider was required to leverage existing resources to form the team. Start-up teams were testing and adjusting care processes to solidify their presence in the community. Growth teams had core expertise, relationships with fellow providers, and 24/7 support. Mature teams were fully integrated in the community, but still engaged in continuous quality improvement.
Conclusion:
Understanding the developmental stages of teams can help to inform the progress of other community-based teams. Appropriate outcome measures at each stage are also critical for team motivation and steady progress.
Keywords
Community-based specialized palliative care has been shown to improve symptom management and quality of life, and reduce healthcare costs compared to usual homecare.
Existing validated frameworks on community-based palliative care teams describe theoretical phases and antecedent factors but lack operational and practical details required for team development.
Synthesizes experiences from 15 diverse specialized, community-based palliative care teams.
Details the characterizing features, activities, milestones, and challenges unique to each of four stages of team evolution evident: Inception, Start-up, Growth, and Mature.
Describes output and outcome measures that are appropriate to each stage.
Defining common stages in the evolution of community-based palliative care teams can inform the development of new teams.
Using stage-appropriate milestones and measures can gauge progress and set realistic expectations for team growth.
Introduction
An estimated 70% of the dying population in Canada, and other high-income countries, will require palliative care. 1 Developing these services in the community is important because many patients prefer to die at home, which can also be higher quality and less expensive than in hospital.2–5 Over a dozen randomized controlled trials and dozens more observational studies5–8 have shown that home-based palliative care can be effectively delivered using interprofessional specialized palliative care teams. These teams better managed symptoms, improved quality of life, and prevented late-life hospitalizations compared to usual care. Yet, community-based specialized palliative care teams are not commonplace. In part, this is because prior research has focused on demonstrating the health services outcomes of the teams, but has provided little description of how the teams developed and sustained themselves.6,9 As a result, we lack knowledge on effective strategies to build and replicate optimal models of teams in other regions.
A few evidence-based frameworks have been proposed that outline the development and growth of integrated palliative care programs in the community. Kelley’s Community Capacity-Building Model, based on research in rural areas, affirms that the initiation of a community-based palliative care program is founded upon four sequential phases or events: emergence of antecedent conditions, occurrence of a catalyst, creation of the team, and growing the program.10,11 Similarly, a grounded theory study by Ploeg et al. 12 on the adoption and scaling of best practices in home care for older adults identified five process phases: committing to change, implementing on a small scale, adapting locally, spreading internally to multiple users and sites, and disseminating externally. Together, these models contribute to the understanding of the theoretical stages of local program development. Still there remains little evidence on practical details, such as key milestones and outcome measures at each stage, that would guide providers wanting to replicate an effective team model in different contexts.
To address this gap in knowledge, we capitalized on a natural experiment existing in Ontario, Canada, where 15 regions independently developed their own community-based, specialized palliative care teams, hereafter referred to as “Teams.” These teams consisted of palliative care “specialist” physicians (who had completed a 1-year fellowship in palliative care, whose billings were > 50% for palliative care, and worked exclusively in the community) and nurses who completed additional training or a certification exam in palliative care. In a previous study, we found that exposure to any of the teams was associated with a 50% reduction in acute care use compared to usual care. 13 This cohort represents a unique opportunity to investigate and compare several diverse and efficacious teams within one healthcare system. We undertook a qualitative examination of these teams to understand the process of their development over time.
Methods
Design
We used a grounded theory approach to understand the milestones and stages in the evolution of creating a home-based team. Data were collected and analyzed between February and August 2013. The study was approved by Hamilton Health Sciences/McMaster University research ethics review board, Ontario, Canada (11-403). Written informed consent was obtained from each participant.
Setting
Teams from Ontario, Canada, were examined. The majority of community-based palliative care is delivered by homecare providers (e.g. nurses and personal support workers). 14 Ontario has a few dozen residential hospices (i.e. free-standing, home-like facilities in the community) but only about 4% of patients die in this setting. 15 Some communities have a visiting hospice volunteer program and a small proportion have a hospital palliative care unit (19 units in ON).
To improve palliative care delivery and address the fragmentation between primary care and homecare, some communities developed interprofessional specialized palliative care teams. 13 These teams provide services similar to the visiting hospice service under the United States’ Medicare Hospice Benefit or palliative homecare provided by MacMillan nurses in the United Kingdom. Patients referred to the Ontario teams are usually in the last months of life and are followed until death. The teams’ services are offered at no cost to patients, although the funding sources vary for the providers involved. Physicians are reimbursed through fee-for-service and/or salary arrangements, while homecare nurses are covered by homecare funding. Some of the teams also rely on fundraising to cover infrastructure costs.
Participants
In all, 15 teams and team members across Ontario were selected using a purposive sampling process, aimed at achieving a variety of profiles. The teams selected represent a diverse geography, including rural and urban communities. These teams met the study inclusion criteria of multidisciplinary team, having specialized palliative care expertise and training, providing care to patients in their homes, and having a focus on pain and symptom management.
The team models vary in the extent that the physicians consult or take over care.16,17 The “specialist” physicians sometimes worked in a consultative manner to family physicians, generalist homecare nurses and personal support workers, and other allied health providers to care for seriously ill patients in the home (consultation model). 18 Other times, the “specialist” physicians would assume primary ownership of the patients (take over model). 7 Eleven of the teams were previously studied as exemplars of specialized palliative care teams serving patients in their homes. 13 The remaining teams were newly formed and in the initial stages of organizing a collaborative practice to serve palliative care patients in their area.
The researchers were known to the team leads through prior activities/events. Team leads introduced the study to their members, who were then approached by the researchers for participation using email and/or phone contacts. In teams with less than six members, all team members were interviewed. In larger teams, a purposive sample was taken to include interprofessional representation and those with the most experience with the team, until data saturation was reached. Core team members interviewed included palliative care specialist physicians, palliative care nurses, allied health professionals (e.g. generalist homecare nurses), homecare case managers, and team administrators. We did not interview family physicians who were supported by the teams. The lead from each team also provided formative information, team documents, and subsequent information requested for clarification by the research team.
Procedure
In-person semi-structured interviews were conducted with team members using an interview guide (Appendix 1). The guide was developed by the research team based on the relevant literature, existing palliative care provision frameworks,19–21 and expert opinion. The guide was designed to explore participants’ perspectives on the process of building a team to provide community-based palliative care. Based on responses, the trained interviewers followed up with additional or clarifying questions.
Interviews were conducted in the participants’ workplaces and took approximately one hour each. Each interview was lead jointly by a primary (H.S., D.Ba., D.Br., S.T.T. (see acknowledgements)) and a secondary interviewer who served as a note-taker. Interviews were audio taped and transcribed by the primary interviewer. Documents describing the history of the teams, relevant administrative data, and process data, that is, briefings, characteristics of caseload, tools incorporated into practice, were also compiled for the teams.
Data analysis
In accordance with Corbin et al.’s 22 grounded theory approach, data analysis proceeded through stages of open, axial, and selective coding. Data for each participant were first coded by the primary interviewer, then reviewed by the secondary interviewer and discussed. Resulting codes and supplementary document data from the teams were then examined by the four primary interviewers together, to determine similarities, divergences, and associations. Codes, themes, and categories were generated first by individual respondent, then by each team, and then across all teams. A constant comparative method was used throughout the analytic process to compare new data to existing codes. 23 To reduce analysis bias, we maintained an audit trail of decisions, used an external peer review process to substantiate the research process, and shared back preliminarily findings with the respondent teams for comment. 23
Results
A total of 122 palliative care providers and administrators involved in 15 home-based teams were interviewed (Table 1). Each team had a mean of seven providers interviewed (range of 4–10). The most common profession interviewed were nurses (37%). Almost a quarter (23%) of participants had 11 or more years of experience in their current role in the team. The 15 teams had characteristics that varied by geography, caseload size, number of physician and nurse providers on team, and year of inception (Table 2). For instance, the palliative care physician full time equivalent (FTE) varied from 0.5 to 11.5 between teams. Overall, 80% of the patients had cancer and were seen by the teams for a median of 1 to 2 months before death. The median patient age was 75 years. A specialist palliative care physician working with a team would typically have 50–100 patients under their care at one time, and see 125–175 new patients each year.
Participant Demographics (N = 122).
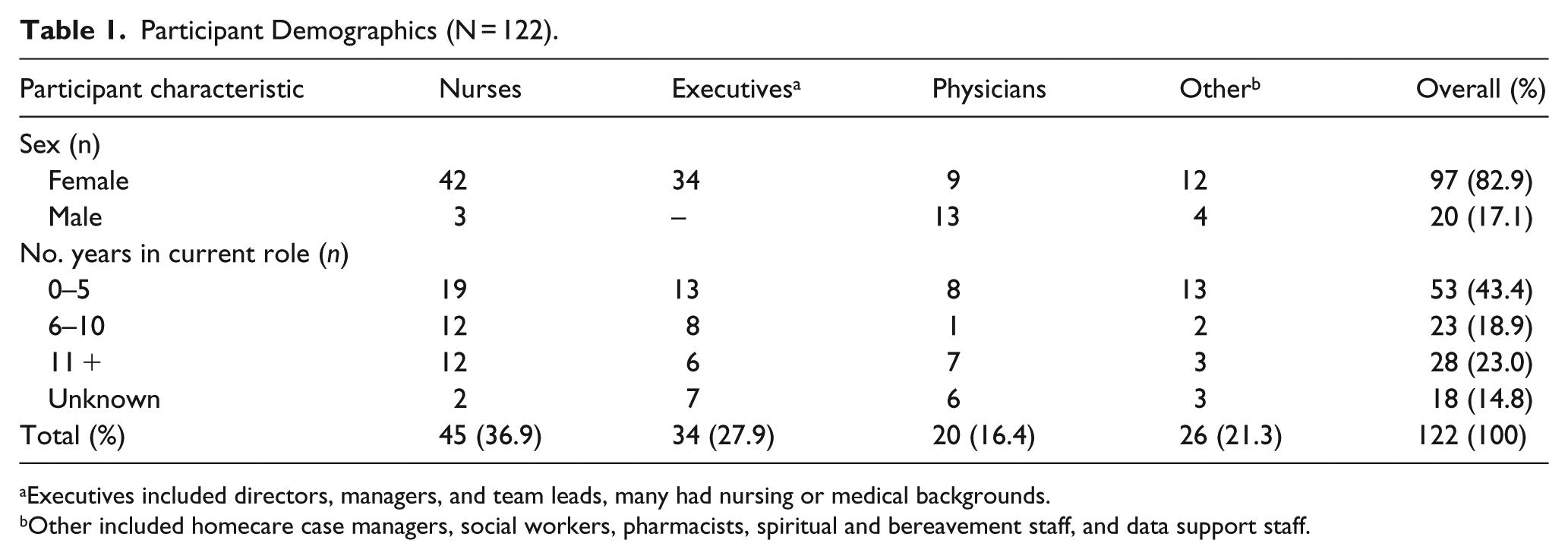
Executives included directors, managers, and team leads, many had nursing or medical backgrounds.
Other included homecare case managers, social workers, pharmacists, spiritual and bereavement staff, and data support staff.
Characteristics of specialized teams.
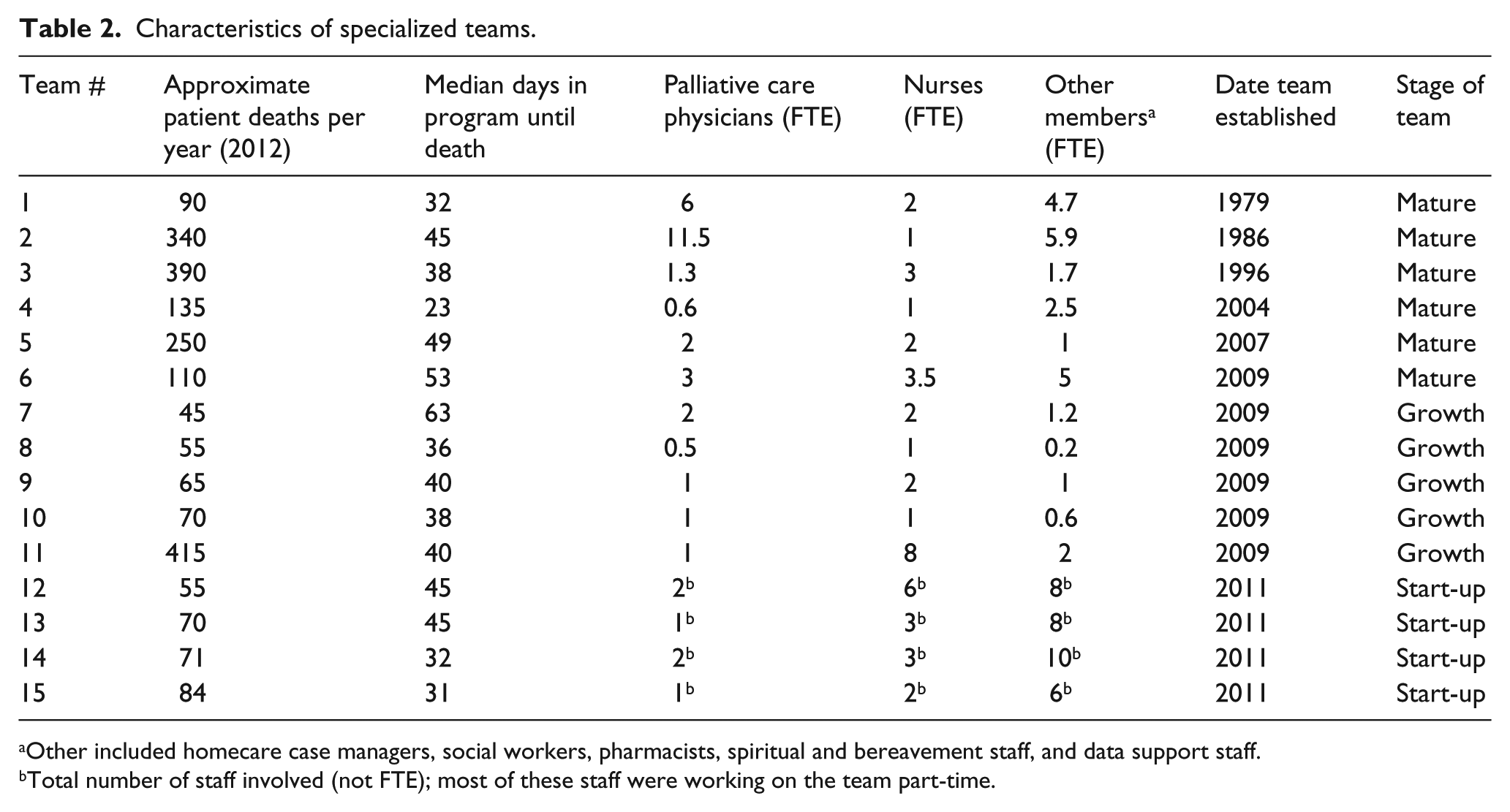
Other included homecare case managers, social workers, pharmacists, spiritual and bereavement staff, and data support staff.
Total number of staff involved (not FTE); most of these staff were working on the team part-time.
Stages of team evolution
Despite differences in characteristics, the analysis revealed that team development underwent a process of evolution that took time and determination: It’s a gradual evolution, you can’t do it all at once, you have to be patient and learn from your mistakes. It’s very “two steps back and three forward,” hopefully in a way that improves the program. As we’ve run into barriers we problem solve and try to bring it back to the team meetings and go forward one by one. (Interviewee 1–Team 11)
The thematic analysis of our data revealed four stages of team evolution: Inception, Start-Up (4 teams), Growth (5 teams), and Mature (6 teams). All teams in the study had evolved past an initial Inception stage. Characterizing features, milestones, challenges, and outcome measures of each stage are described below and summarized in Table 3.
Evolution framework by stage.
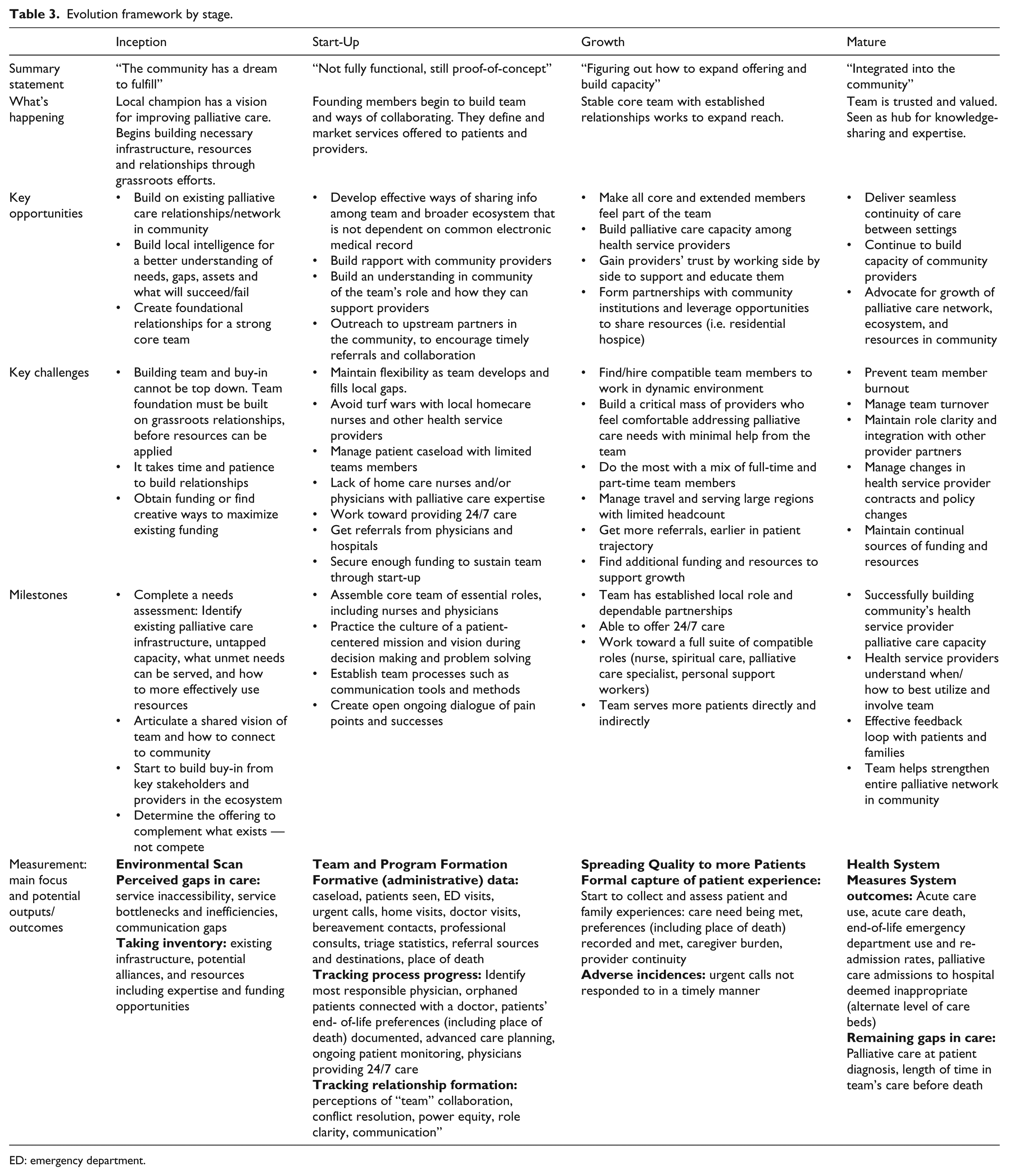
ED: emergency department.
Stage 1: inception
Most of the teams were initially spearheaded by a provider champion, usually a nurse or physician, rallying members of the local community to improve access to palliative care. The champion was able to leverage funding and/or obtain in-kind support from organizations and providers interested in fulfilling this “dream.” The existence of at least one person to champion the cause and a community that perceives the value of palliative care, were seen as critical to the genesis of the team: Without local champions and leaders, nothing would happen. (2–Team 12)
The teams built upon existing services when possible rather than duplicate those already in place. Many preliminary teams conducted some form of needs assessment to obtain a sense of what support is available for dying patients, what is needed, and who are the current “players.” Most teams first worked with local primary care physicians who were amenable to receiving support from the team for their dying patients. The teams gradually developed a reputation for expert care, which encouraged other primary care physicians to either work with or refer patients to the team: Complete a needs assessment. Begin with existing teams and experts. Develop a small team of interested and committed experts with a common goal and identify the critical roles and responsibilities of team members. Networking and profiling the program as it was developed was a key to our success. (4–Team 11) When starting a palliative care team you have to look at your own community and see who’s there and where the interest lies. Look into which physicians in your community are doing palliative care, and then think how can you support that physician trying to do this work so they aren’t doing it alone. That is how our team evolved. (1–Team 6)
One of the most crucial pieces of advice offered by the teams was to begin small and build relationships; proceed even if the plan is not perfect: Start somewhere, don’t wait until the pieces of the puzzle fit together—don’t be afraid. Just start and learn from your mistakes and then change and adapt. Start somewhere, because this person is dying now and they won’t be here tomorrow. If we wait until all the stars are aligned we will miss helping all those people who die while we wait around. Has it been perfect? No, probably some of my most difficult cases have been our greatest learning opportunities. (1–Team 6)
Stage 2: start-up
The teams in the Start-up stage were not fully functional and still in a proof-of-concept phase. They were caring for some patients in the community but still trying to solidify the team’s staff complement and test different care processes to improve the efficiency of their practice, the quality of care for dying patients, and access to the service. Approaches to care at this point were neither standardized nor consistent, but the teams had developed a clear mission of what they wanted to achieve. They remained adaptive since not everything they tried would work. Building a small team of capable core providers and further advancing working relationships with generalist and specialized providers in the community were essential to progressing through this stage: Then you just start and you gain experience and confidence by doing the work and working through and solving the problems. Make a path with the help of team support and tapping into some external consultants you can call as you need, and by working very closely with community groups like hospice volunteers, church volunteers, and neighbours. You will quickly gain confidence that you can actually do this work very well. (2–Team 1)
Informal communication internally and externally to the team was integral for building rapport, improving care continuity, and establishing the team’s presence in the greater community. Many of the teams tested processes for the transfer and discussion of patient information between providers, to determine which methods worked best. Some of these strategies, for example, chart-in-the-home, worked well for some teams but not others. Core providers tended to communicate with one another by phone, and also offered their number to external providers to call the team for assistance or patient referral. Through the teams’ offering to collaborate, they strove to spread a culture of patient-focused practice. This including reaching out to “upstream” partners in the community, to encourage earlier referrals to palliative care: Relationship building has happened informally [through] encouraging the nurses to take initiative to call and discuss if they think something’s missing and we work together. We are able to communicate and deal with things quickly. (1–Team 14)
Importantly, at this stage, most teams had not built enough capacity to offer around-the-clock-access to palliative care. However, they had begun proactively addressing potential crises among their patients to reduce the need for after-hours care. Part of this plan was being explicit with patients about the support they could depend upon from the team and from other community services. The development of role clarity and open communication, to facilitate collaboration of care, were key tenants of this stage.
Stage 3: growth
Teams in the Growth stage were figuring out how to both expand the offering and build capacity in supporting generalist providers. The teams had established dependable partnerships, including those with community institutions, to share information, resources, and responsibility for addressing palliative care needs. The teams, in conjunction with their partners, were able to provide 24/7 care in the home and help transfer patients to appropriate, more intensive, care settings if required. Growth teams made concerted efforts to promote their service among local health professionals and the larger community: Knowing that there is this 24/7 service in place has enticed some [primary care] physicians. We went out to different family practice groups and provided presentations and offered our consultants to work collaboratively with them. There is still a lot of resistance but we’ve capitalized on the physicians that have shown interest in trying to make referrals to them. (1–Team 11)
At this point, most of the teams had implemented formal interprofessional platforms such as case rounds, as opportunities to plan and learn together. The teams had a desire to prove their worth and value to patients, funders, and their community; as a result, they continually strived to improve the patient and family experience: The community nurses know we are here, we meet every two weeks as a broader team for rounds, we also meet with hospital discharge planners and have collaborated with the ER [emergency room] to avoid admissions and facilitate continuity of care. (1–Team 8)
The teams incorporated more formal quality improvement into their practice, eliciting patient feedback and reflection on adverse incidents. Team members spread their expertise and gained trust by supporting, working with, and educating a growing number of generalist providers in the community to build their capacity for palliative care: We have heard of nurses approaching the [primary care] physician and telling them that they are solely responsible for their patients. Usually this scares them [the physician] and if given an out to transfer care they will. We approach it differently and try to meet the physician where they are at and as a result have a much better response rate of them remaining involved. We don’t give them an out but work with them. (3–Team 14)
In the Growth stage, the core and extended members of the team constituted a full suite of compatible roles (nursing, personal support, therapy, primary care, emotional support, spiritual care), toward serving more patients collectively and initiating palliative care earlier in patient trajectory. Challenges such as turf wars with other organizations, prevailing bureaucracy, and ensuring the sustainability of the team were still being resolved. The teams stayed the course by reminding themselves and others of the ultimate goal of providing quality palliative care experiences for patients. A non-punitive environment which celebrates wins but also views failures as learning opportunities was regarded as key to growing the program while avoiding members becoming discouraged: You need to name the problem, or at least someone needs to have the courage to name it. You need to be professional, gracious and clear. Transparency and clarity on an issue is important for trust. These “elephants in the room,” in my experience, are never one-offs so you need to develop a safe space to hash out the common ground and common vision. (1–Team 4) The focus needs to stay on what we’re trying to do; provide the best care for someone at end of life. If there is something that is a consistent problem, that keeps on coming up, we have to be able to say it. (6–Team 6)
Stage 4: mature
The teams considered at the Mature stage were fully integrated into the community. They were recognized as a center of excellence for knowledge-sharing, expertise, and patient care. The contributions of these teams were both trusted and valued, which granted them authority in advocating for their palliative care patients and system: The team is well known in the community and is very well respected. It [the team] is promoted by a number of organizations that help to fundraise. The turf wars may have happened in the early days but it is now well know that everyone plays an important role in the care of palliative patients and their families. All providers work together and I do not think there is any overlap or redundancy. (3–Team 1)
The sustainability of these teams was secure in tapping continual sources of funding but also in adaptability to top-down policy changes. The team’s role was clearly understood, and as such, external health service providers knew when/how to best utilize and involve the team. Established channels of formal and informal communication existed within the team, with external providers, and with relevant community organizations, to facilitate continuity and comprehensiveness of care in an efficient manner: We talk to each other daily, sometimes even on weekends. We relay information to one another so nothing falls through the cracks. We have a great system. (2–Team 5)
Generally, teams evolved their model of care over time. At start-up, they worked more in a take-over model, as they were learning how to work together to provide comprehensive palliative care. However, over time, they realized the community’s need was too great for their team alone, and began to deliberately focus on building capacity of other primary care physicians and nurses. Thus, the majority of the mature teams did not assume full responsibility for most of the palliative care patients referred to them (take over model), but rather supported the primary care provider to remain significantly involved (consultation model). Teams had increased palliative care capacity through training other providers to the extent that often only the more complicated patients required team involvement and some of these other providers had become capable mentors themselves: My mantra is that, first and foremost, we [the team] are here to serve primary care. I am here to put myself out of business. The more we are in a relationship with a family physician, the less they need us [the team]. We help them grow their skills. We remain engaged in care but may do very little—we hover but don’t do ongoing care. (1–Team 4)
Stage appropriate measurement
Outcome measurement was important to all the teams. The newer teams felt pressure to show patient and system improvements and were eager to do so quickly, resulting in frustration. In contrast, the more established teams had come to realize that expecting great impact too early can set the initiative up for failure. Mature teams emphasized that measurement needs to start simple, such as counting the number of patients seen (Table 3). Informal mechanisms of immediate feedback were often utilized: We know we’re doing a good job because of the feedback that we get from not only families, but from each other working together as a team. It is very important to have that feedback from one another. Sometimes when we’re having a bad day or a bad week or we’re about to lose one of our precious patients, we need feedback from each other to know that we’ve done a good job. (5–Team 5)
At formation, most teams had a sense of the local state of palliative care, that is, present gaps and assets. This knowledge of the environment is critical to build upon existing capacity and align the service to the needs of the community. Once the team had started serving patients, the primary focus of measurement was understanding how and why the team is contributing to the care experiences of dying patients. Outcomes at this Start-up stage were more like outputs: tracking patients, including the number and characteristics of patients seen; process counts, such as number of patients with a most responsible physician identified; and monitoring and reflecting on the team climate. Measurement becomes more sophisticated at the Growth stage to formally capture the patient and caregiver experience of care and examine adverse incidents, using these findings to improve care quality. Finally, at the Mature stage, health system outcomes were measured as evidence of effectiveness, as well as, patterns of care data to improve earlier and more inclusive patient access to the team: Now we know the team is doing a good job based on some big measures such as reducing emergency visits or reducing time in the hospital and so on. (4–Team 2)
In the beginning of team development, measurement was more purposeful than perfect. They made sure to celebrate small successes at each stage, to help them to stay motivated, build momentum, and grow their program. As the teams matured, measurement became more formalized, structured, and integrated into the broader system. There is no formal system of palliative care measurement in Ontario, thus the teams had to measure their own outcomes using local data. By partnering with the authors in a related study, the Mature stage teams demonstrated significant patient and system impact, including increased home death rates and reduced emergency department and hospital use.
13
Teams also sustained an informal feedback loop with patients and families to continually fine tune the care process: We follow up with the families afterward and they tell us things went as well as could be expected. If the opposite is true, we ask how things could have been improved, and thank them for the opportunity to learn. (1–Team 8)
Discussion
Key findings
Our qualitative examination of 15 specialized palliative care teams at various degrees of development revealed four main stages of evolution: Inception, Start-up, Growth, and Mature. With each consecutive stage, the teams demonstrated more capacity to advise and educate providers external to the team; offer around-the-clock access to care; impact patient and system outcomes; work in a collaborative, interprofessional model; engage primary and tertiary care, incorporate quality improvement and measurement into practice; and influence the local palliative care system. Even though the teams represent different models and staff complements we observed the same patterns in evolution. Prior frameworks have proposed the essential elements to building quality palliative care provision19,24–26 but have not suggested how these features emerge over time. To our knowledge, this is one of the first studies to report on an in-depth analysis of the natural progression of palliative care teams, based on a large number of diverse examples.
Implications for policy and practice
The findings from this study are relevant for the many countries that utilize home-based palliative care, such as visiting hospice service teams in the United States or palliative care community provider teams in Australia or the United Kingdom.27–30 Although community-based palliative care services have expanded, consistency in access and quality remain variable, meaning teams have room to improve over time.31–33 Regardless of how teams are funded in different countries, the steps of how teams evolve and which challenges arise over time likely hold true. Initiating the team programs examined was dependent on a few individuals with the vision to work with others to provide better palliative care in the community. Many of the team founders reported that they did not wait for an external catalyst or the perfect opportunity, plan, or resources, but rather perceived a local need and started with small changes; leveraging available capacity—becoming the catalyst themselves. In the early stages, the teams placed less priority on choosing the best measures and collecting data, than serving the needs of patients who needed support at that moment. While growing, team attention was on implementing and adjusting their service. Simple forms of quality improvement measures were incorporated into practice. As teams matured, measurement became more formalized and directed at more ambitious outcomes. Most of the teams had taken a long time to mature; this evolution was directly related to the activities partaken and measures of success used, along the way.
What this study adds
The stages of evolution we identified among the teams share commonalities with the phases of palliative care development described in Kelley’s10,11 Capacity-Building model and those in Ploeg et al.’s 12 model of scaling of best practices in home care programs. All three models describe an iterative, non-linear process and emphasize the critical role of leaders to drive forward the vision for change. The models are different yet complementary in that the Capacity-Building Model focuses on teams in the earlier stages of evolution, while the scaling model conceptualizes the spread of standardized practices in general home care. In comparison, our model covers the progression from newly formed to well-established teams, across different geographies, and predicated on the formation of interprofessional collaborative partnerships.
Study limitations
A limitation of our study is that all the teams were from one province in Canada, possibly restricting the global applicability of the findings. However, our study sample includes a large and diverse number of teams, who face system challenges common to many countries (e.g. shortage of expertise, fragmentation of services, uncoordinated communication, lack of standardized outcome measurement, etc.). 34 Another limitation is that we interviewed relatively few providers external to the teams, who may have a different perspective of team evolution and impact.
Conclusion
We found that specialized palliative care teams go through distinct stages of evolution, each with unique sets of opportunities and challenges. Despite each team being different in initial and present structures for palliative care delivery, four stages of development were evident across the team histories. Team establishment was an iterative process, largely based on relationships. Time was required to build the long-term trust, communication channels, and authority necessary to render the teams successful and sustainable. The teams learned and adapted as they grew, refining ways of working together and serving patients and their families. Understanding the steps that are associated with the developmental stages of these teams can help to inform the progress of other community-based teams. This information also assists planners to better anticipate and set expectations for how teams may advance toward strengthening the palliative care system.
Footnotes
Appendix 1
Indicative script for interviews
Acknowledgements
The authors gratefully acknowledge funding received for this study from the Ontario Ministry of Health and Long Term Care (Contract No. 2011-0006) and the Canadian Institutes of Health Research (Grants No. 115112 and No. 148997). Dr. Seow is supported by the Canada Research Chair program. We also wish to thank Ms. Deanna Bryant (MPA) and Ms. Sue Tan Toyofuku (MSc) for their assistance in data collection and analysis. Hsien Seow contributed toward the study design, data collection, data analysis, writing of draft manuscript, and review of draft and final manuscript. Daryl Bainbridge contributed toward study design, data collection, data analysis, writing of draft manuscript, and review of draft and final manuscript.
Data management and sharing
The confidential nature of the qualitative data prohibits them from being released publicly.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was received for this study from the Ontario Ministry of Health and Long Term Care (Contract No. 2011-0006) and the Canadian Institutes of Health Research (Grants No. 115112 and No. 148997).
Research ethics and patient consent
The study was approved by Hamilton Health Sciences/McMaster University research ethics review board, Ontario, Canada. Written informed consent was obtained from each participant.