
Abstract
Background:
Occupational therapists play an integral role in the care of people with life-limiting illnesses. However, little is known about the scope of occupational therapy service provision in palliative care across Europe and factors influencing service delivery.
Aim:
This study aimed to map the scope of occupational therapy palliative care interventions across Europe and to explore occupational therapists’ perceptions of opportunities and challenges when delivering and developing palliative care services.
Design:
A 49-item online cross-sectional survey comprised of fixed and free text responses was securely hosted via the European Association for Palliative Care website. Survey design, content and recruitment processes were reviewed and formally approved by the European Association for Palliative Care Board of Directors. Descriptive statistics and thematic analysis were used to analyse data.
Setting/respondents:
Respondents were European occupational therapists whose caseload included palliative care recipients (full-time or part-time).
Results:
In total, 237 valid responses were analysed. Findings demonstrated a consistency in occupational therapy practice in palliative care between European countries. Clinician time was prioritised towards indirect patient care, with limited involvement in service development, leadership and research. A need for undergraduate and postgraduate education was identified. Organisational expectations and understanding of the scope of the occupational therapy role constrain the delivery of services to support patients and carers.
Conclusion:
Further development of occupational therapy in palliative care, particularly capacity building in leadership and research activities, is warranted. There is a need for continuing education and awareness raising of the role of occupational therapy in palliative care.
The role of occupational therapy in palliative care service delivery has evolved over several decades.
The scope of this role is more established in some countries.
This is the first study to examine the provision of occupational therapy in palliative care in Europe.
This study provides evidence of the consistency of occupational therapy practice in palliative care between European countries, with an emphasis on physical, functional, psychological and social aspects of care.
There is a contrast between high levels of involvement in direct and indirect patient care and limited involvement in service development, leadership and research.
This study highlights the need for further development of occupational therapy in palliative care and capacity building in leadership and research activities.
Organisational expectations and understanding of the scope of the occupational therapy role constrain the delivery of services to support patients and carers.
There is a need for education and awareness raising of the scope of occupational therapy in palliative care.
Introduction
The European Association for Palliative Care (EAPC) White Paper on Standards and Norms for Hospice and Palliative Care in Europe includes occupational therapists (OTs) alongside doctors, nurses, physiotherapists and others as essential members of ‘the interdisciplinary team of health care professionals, who are both knowledgeable and skilled in all aspects of the caring process related to their discipline of practice’.1,2
Occupational therapy contributes to palliative care by enabling people to lead fulfilling lives within the constraints of their illness. It uses a structured process of assessment, activity analysis and goal setting with patients and carers to facilitate participation in essential and valued activities,3 –6 while acknowledging the practical and existential consequences of a deteriorating condition.7 –10 The ability to participate in everyday life and contribute to social relationships maintains a sense of competence, reciprocity and well-being for people with life-limiting illnesses and is highly valued.11 –13 It follows from this that suboptimal access to occupational therapy services limits patients’ and carers’ ability to manage daily activities in their preferred environments. While there are no formal data on the availability of occupational therapy services in palliative care in Europe, 14 anecdotal information shared at EAPC conferences and in online discussion forums (such as the Palliative Rehabilitation Facebook Group 15 ) indicates that provision of occupational therapy in palliative care varies widely, with services in the United Kingdom and Ireland being more established than in other European countries.
In order to investigate the reported variation in palliative care occupational therapy service provision across European countries, and to provide a forum for networking and exchanging information, an EAPC Task Force on Occupational Therapy was established in September 2010. The survey we report here was carried out by this task force. Its aims were to
Examine the scope and remit (i.e. specific interventions provided and therapists’ responsibilities) of occupational therapy in palliative care in Europe.
Explore any perceived differences in services provided between the United Kingdom/Ireland and other European countries.
Explore OTs’ perceptions of opportunities and challenges encountered in delivering and developing services.
Methods
An online questionnaire survey of OTs working full- or part-time in palliative care in European countries was conducted. The survey was presented in English as funding was not available for translation. Survey design, content and recruitment processes were reviewed and formally approved by the EAPC Board of Directors. Reporting of findings is informed by CHERRIES guidance for reporting Internet surveys. 16
Questionnaire design
The questionnaire followed the format of a previous survey successfully undertaken by the EAPC Task Force on Education for Psychologists in Palliative Care. 17 It comprised 49 items in four parts. Part 1 contained fixed response questions on the proportion of work time spent in palliative care, service type and main patient groups seen. Part 2 asked about frequency of engagement in occupational therapy interventions with patients and carers, multidisciplinary team (MDT) working, provision of education and training and participation in research and service development (very frequently/frequently/seldom/never). Items on interventions were derived from the UK College of Occupational Therapists’ Specialist Section in HIV/AIDS, Oncology and Palliative Care Guidance on Occupational Therapy in Cancer. 18 Space for free text responses was provided after each subsection. Part 3 covered respondents’ perceptions of occupational therapy in palliative care in their countries, with four free text and one fixed response question on their role, challenges and current and future contributions in palliative care. Part 4 collected demographic data on age, gender, qualifications and country. All questions except free text comment boxes were mandatory. The questionnaire was piloted with six palliative care OTs (working outside Europe) resulting in minor changes. It was reported to take about 20 min to complete. The full questionnaire is available in Supplementary Table 1.
Sampling and recruitment
Inclusion criteria required respondents to be qualified OTs, working in a European country, who saw palliative care recipients as part or all of their caseload. A convenience sample of OTs was invited to complete the securely hosted open survey online via the EAPC website. Email invitations were sent to all EAPC members, with one follow-up reminder. The initial invitation identified the investigators, the study purpose, the time the survey was open, which data would be stored and location of data storage (password-protected university computer). Given that very few OTs belong to the EAPC, members were asked to distribute the invitation as widely as possible through their networks. To further increase reach and participation, survey information, with a link to participate, was also disseminated by the Council of Occupational Therapists for the European Countries (COTEC), the EAPC Physiotherapy Task Force, the UK College of Occupational Therapists’ Specialist Section in HIV/AIDS, Oncology and Palliative Care, and to OTs attending past EAPC congresses as shown in EAPC records.
The survey ran from 20 March 2013 to 19 April 2013, and no incentives were offered for survey completion. Survey responses were anonymous unless respondents chose to provide email addresses to receive information when results were published. De-identified survey responses were entered automatically into a database, managed by EAPC.
Data analysis
Quantitative and qualitative data were collected simultaneously and were analysed using descriptive statistics and thematic analysis. Completed questionnaires were reviewed by investigators and duplicates eliminated prior to analysis. All questions were mandatory; therefore, all received questionnaires were complete. Descriptive statistics were prepared using Microsoft Excel on respondents’ characteristics and the frequency of occupational therapy interventions, tasks and roles. The proportions of people who endorsed an activity with ‘frequently’ or ‘very frequently’ were calculated. Free text data were organised and managed using QSR Nvivo. Analysis was informed by a pragmatic approach which entailed immersion in the data, coding and creation of categories and themes.19,20 Initial coding was undertaken by D.M., and themes refined by both D.M. and G.E. For the free text questions in Part 3, the UK and Ireland responses were separated from those of mainland Europe, and a content analysis was carried out to see whether any striking differences emerged.
Results
A total of 260 responses were received. After removing tests (2), non-Europe (14), non-OT (1) and duplicates (6), 237 responses from 21 countries remained for analysis, just over half of these from the United Kingdom (Table 1). In total, 14 EAPC member countries did not supply a response. They included Albania, Armenia, Croatia, Cyprus, France, Greece, Hungary, Iceland, Luxembourg, Poland, Slovakia, Spain, Switzerland and Ukraine.
Survey responses by country.
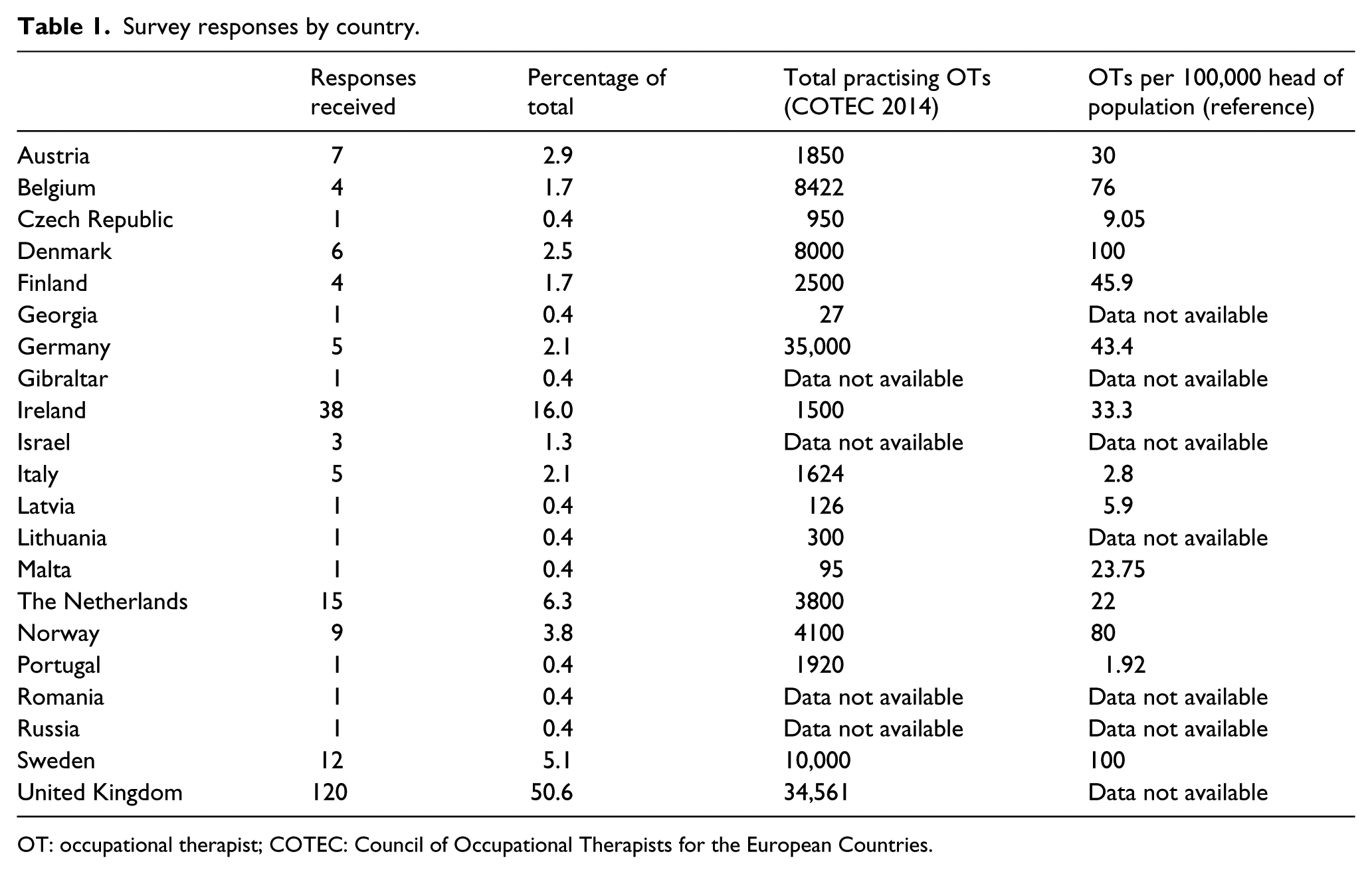
OT: occupational therapist; COTEC: Council of Occupational Therapists for the European Countries.
Respondent characteristics
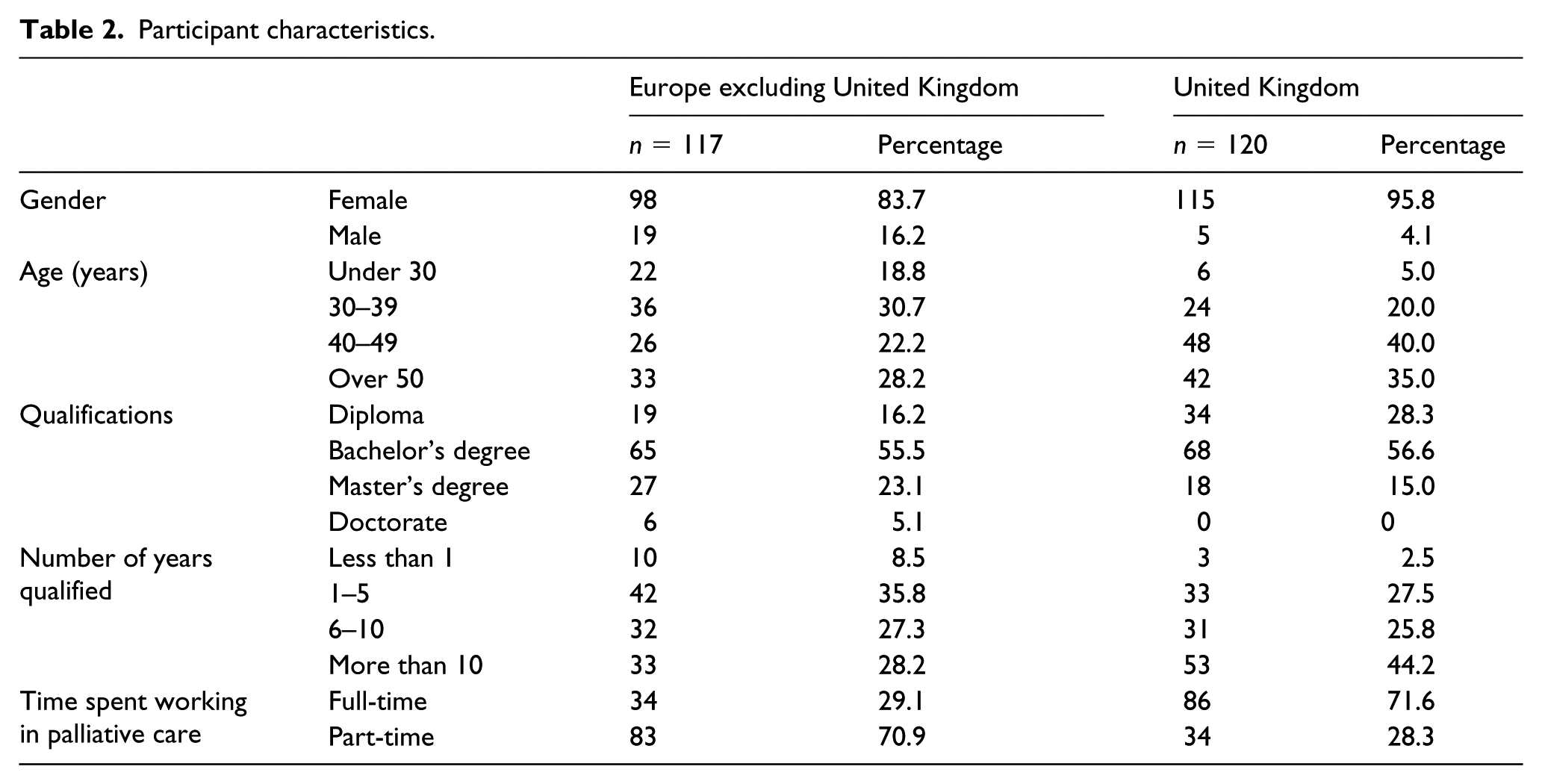
Respondent characteristics are summarised in Table 2. The majority of respondents were female (95.8% in the United Kingdom; 83.7% in the rest of Europe). UK therapists tended to be older (75% over 40 years compared with 50.4% in Europe) and more experienced (70% in practice more than 5 years compared with 55.5% in Europe). More European therapists had master’s and doctoral-level qualifications (28.2% in Europe compared with 15% in the United Kingdom). A total of six therapists in Europe had a doctorate compared with none in the United Kingdom. The proportion of therapists working full- or part-time in palliative care was exactly reversed between the United Kingdom and the rest of Europe, with 71.6% of UK therapists working full-time and 70.9% of European therapists working part-time.
Participant characteristics.
Frequency of occupational therapy interventions, tasks and roles
Frequency of occupational therapy interventions, tasks and roles was identified from responses to Part 2 of the survey. Figures 1–3 show the frequency with which occupational therapy interventions, tasks and roles are undertaken. Interventions undertaken directly with patients are shown in Figure 1. The most commonly undertaken interventions, carried out frequently/very frequently by >80% of European and UK OTs, include prescription/provision of assistive equipment to optimise patients’ independence in activities of daily living and assessing patients’ functional capacity, positioning, postural and comfort needs. With the exception of vocational rehabilitation, all of the interventions listed are carried out by more than 60% of UK OTs and are more frequently carried out by UK than European OTs. Interventions where there is a substantial difference between the frequency with which they are carried out by UK OTs compared to European OTs (>25 percentage point difference) include fatigue, breathlessness and anxiety management and supporting patients’ adjustment to disability, loss and dying. Of note, very few OTs either in Europe or in the United Kingdom are providing vocational rehabilitation.
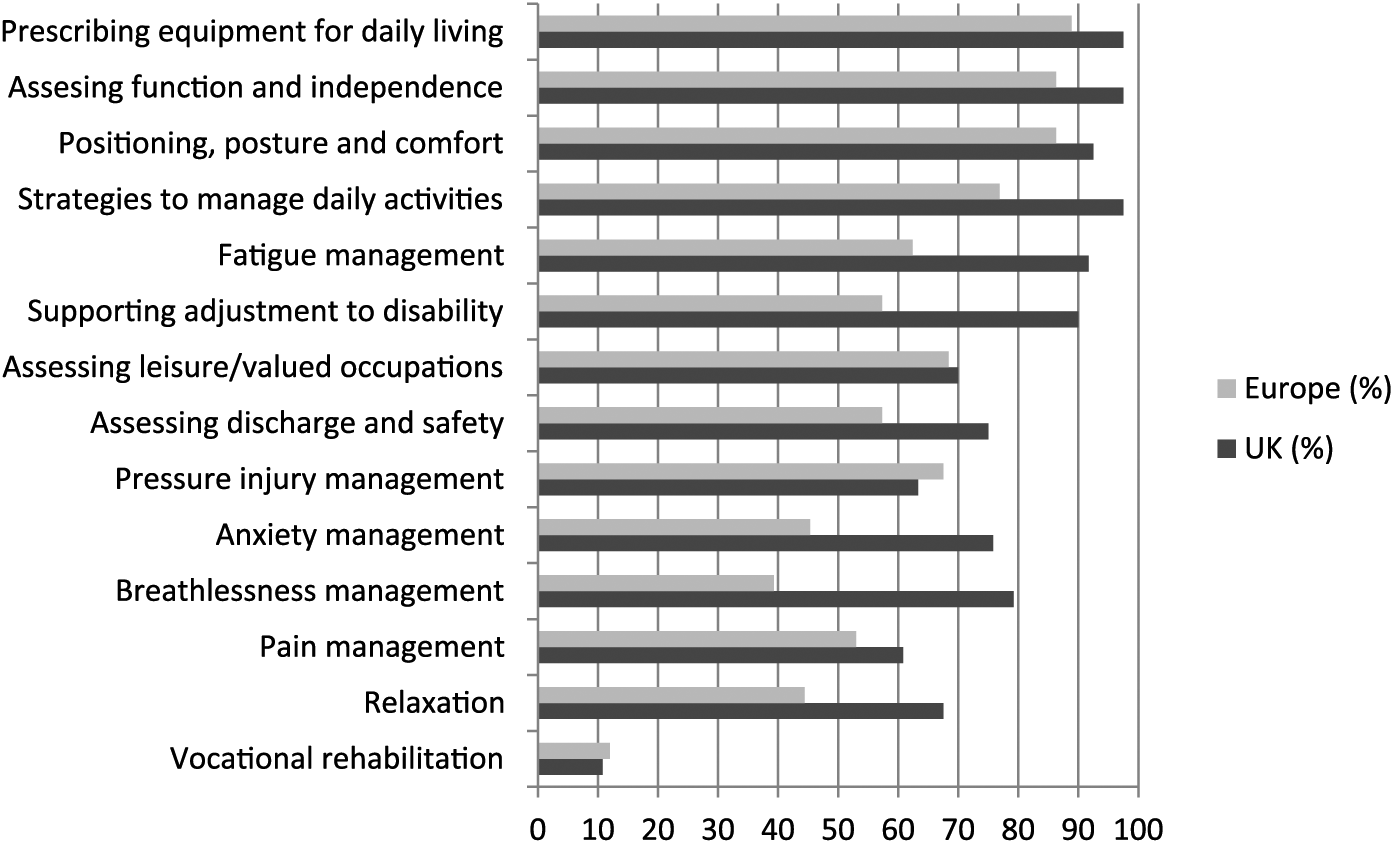
Interventions undertaken with patients frequently/very frequently.
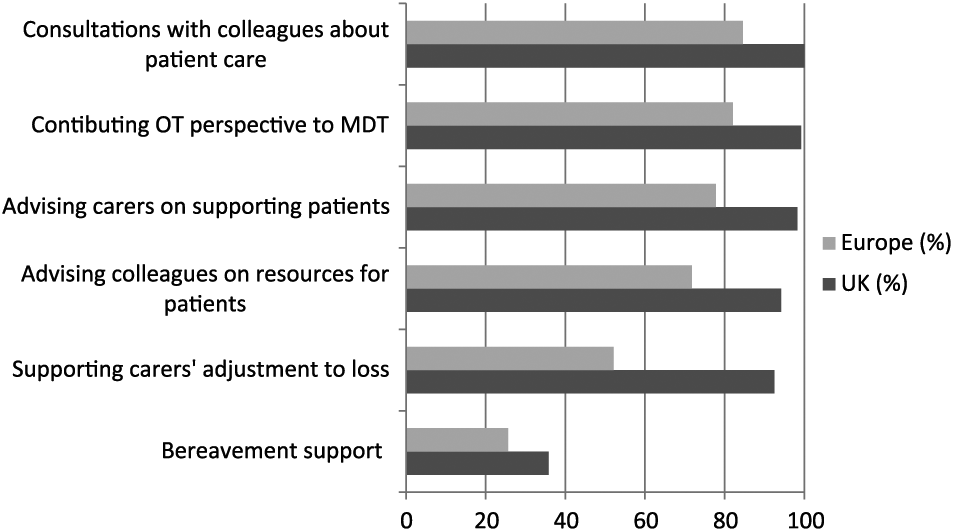
Supporting carers and colleagues undertaken frequently/very frequently.
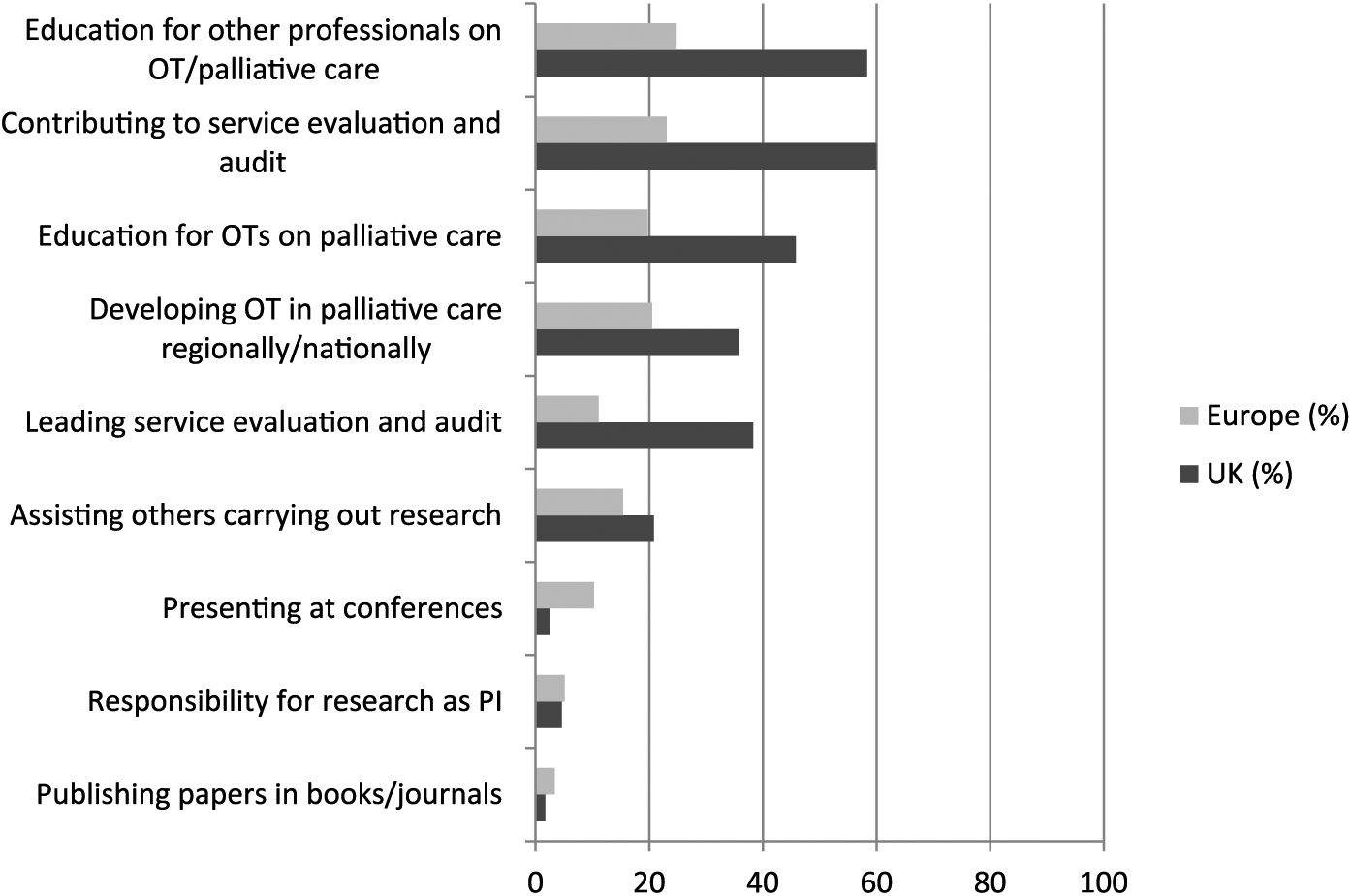
Involvement in education, service development and research frequently/very frequently.
Indirect patient activity is shown in Figure 2. This includes supporting and advising carers and colleagues on resources and strategies to enable patients to manage daily activities and/or to be cared for in the place of their choosing. The majority (over 60%) of OTs in the United Kingdom and Europe carry out such interventions frequently or very frequently. Fewer OTs in Europe than in the United Kingdom (52.1% compared with 92.5%) support carers’ adjustment to disability, dying and loss frequently or very frequently. Only a quarter (Europe) to a third (United Kingdom) of OTs are frequently or very frequently involved in providing bereavement support.
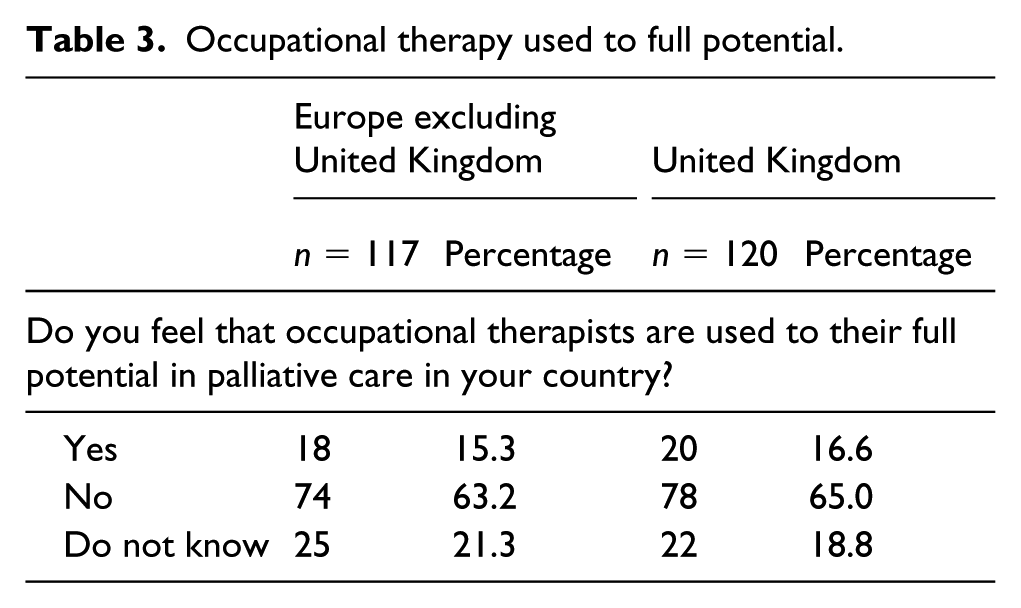
Figure 3 indicates the extent to which OTs participate in education, service development and research activities. There is a noticeable contrast between the high levels of involvement in direct and indirect patient care shown in Figures 1 and 2, and their limited involvement in activities – such as teaching, research and dissemination – designed to build services, develop the evidence base and provide strategic vision and leadership. The majority of respondents (65% in the United Kingdom, 63.2% in Europe) felt that occupational therapy was not used to its full potential in their country (Table 3).
Occupational therapy used to full potential.
Free text responses
A total of three free text questions asked respondents to comment on the scope of their role, ways in which they felt they could make a greater contribution and the key challenges that made this contribution to clinical care difficult. There was also a free text option to record relevant issues not covered by other questions. A total of three main themes with subthemes (in italics) were identified. Further detail and supporting quotations can be found in Supplementary Table 2.
Theme 1: enabling active living while dying
Respondents emphasised the importance of identifying meaningful activities and working with patients and families to adapt these to enable continued participation. Setting realistic and meaningful goals served as the foundation for this: The OT role is most valuable in the support of patients and their families to achieve important goals towards the end of their lives. Whether this is remaining in their familiar home environment for their end of life care, or attending their children’s communion when they cannot sit up for more than an hour. The holistic nature of our role enables us to really listen to a patient’s goals and our problem-solving skills enable us to assist in achieving them for our patients.
Enabling participation through symptom management and education was seen to be achieved through gentle rehabilitation. Patients and families were included in education about practical ways to manage symptoms such as fatigue. Skilled assessment of the impact of symptoms on function, and the provision of assistive equipment or home modifications where required, enabled participation: Through correct posture, seating and mobility advice, we can contribute towards easing symptoms of pain. OTs are well-placed to offer advice on fatigue, anxiety and breathlessness which is commonplace in palliative care. I provide practical support to enable people to be as independent as they can be with either equipment, home adaptations, changes to the way they do things or help from carers.
While facilitating adjustment to deterioration and dying might be an atypical role for an OT, it was perceived to be a core role in palliative care. Respondents sought to optimise patients’ independence wherever possible but at the same time supporting patients to relinquish activities that became impossible as they deteriorated: I believe my role fundamentally is about working with a person to bridge the gap between the past into the short-term future. I do this by focussing on someone’s innate desire to be productive, allowing him/her to reprioritise, adapt and adjust so the quality of life of the person (and the people they love) becomes the main priority. My role is to work with the activities that the patient needs to do and wants to do. It’s not only about being independent and do as much as you can on your own, but also figure out when it’s time not to do some activities or take help from someone else, or compensate with devices.
Theme 2: roles informed by resources and expectations
Resources and expectations were seen to restrict the scope of occupational therapy practice. Limited resources and a lack of others’ knowledge about the potential contribution of occupational therapy were barriers to service delivery. Respondents expressed frustration with their role being limited to that of equipment provider, expediting discharge from in-patient units. However, they were cautious about communicating their role, fearing that limited resources would prevent them from meeting potential demand: At present, occupational therapy resources in palliative care are often limited and stretched meaning it is the patients’ basic needs, occupations and safety which are often addressed as a priority. This makes it difficult to address all occupations such as leisure and work equally, to spend time on research, service development and other interventions due to time constraints. By knowing more about what my contribution could be [patients and carers] would probably include me more. Limited resources in occupational therapy has made me choose not to inform them.
Conversely, the scope of practice was expanded when the OT was an integral part of the MDT: I work closely with the MDT in order to provide the best care e.g. joint assessments with the clinical nurse specialists, joint home visits with the palliative care social workers, joint consultations with the palliative care consultant.
In these settings, issues beyond basic activities of daily living could be addressed: I feel well supported to develop the service as needed for the patient population and can include anything from basic functional assessments to community-based activities that increase quality of life. My current role with the Specialist Palliative Care Team … is quite novel in that I aim to deliver the ‘hospice ethos of care’ as an OT on the acute wards [including] clinical interventions to a small complex caseload, provision of advice for professional colleagues, plan and deliver palliative education … and service development to include audit and research.
Theme 3: mapping a future
Respondents described the importance of promoting occupational therapy in palliative care, both to ‘generalist’ OTs and the wider MDT team: Profile needs to be raised to ensure that other professionals/commissioners fully recognise what skills occupational therapists possess and how we can provide to their patients. Often OTs do not realise they have a role in supporting people at this time.
There was a need for palliative care learning outcomes to be embedded in pre- and post-registration education: [There is a] lack of under-graduate and post-graduate training [in palliative care] for OTs. We lack support in education and career progression. Most courses are run for doctors and nurses and we have a very limited budget for training which means we can really only attend free courses. [Some OTs] would feel they do not have adequate training or counselling skills to deal appropriately with these issues.
Finally, despite challenges, respondents emphasised the importance of contributing to, and implementing, evidence in practice: I also consider research and service development to be an integral part of my role. Interventions need to be based on current evidence and best practice. We have contributed to articles in the past and would relish continuing to do so as well as continuing to participate in research.
In addition to the thematic analysis, the free text responses from the United Kingdom and Ireland and those from mainland Europe were separated and examined to see whether any differences emerged. In fact, more similarities than differences were observed with respondents in both groups identifying similar issues and challenges. The emerging nature of palliative care in some European countries was noted; however, respondents from these countries commented on the need for improvement in the provision of basic palliative care services before occupational therapy could be further developed.
Discussion
This is the first survey of European OTs that examines the scope of occupational therapy in palliative care. Although palliative care is a small clinical speciality for OTs, there were a substantial number of respondents (N = 237). Similar to UK respondents in this study, an Australian occupational therapy workforce profile of clinicians working in palliative care (N = 171) found that the majority of clinicians were female (93%) in full-time employment. 21 However, only 49% had worked in this field for more than 5 years, which is more aligned to respondents from the rest of Europe.
Significance of the findings
Findings of this study are consistent with two Australian studies that examine the occupational therapy role 8 and barriers to clinical practice. 22 Barriers include a limited understanding of the scope of the occupational therapy role; limited resources; and few OTs engaged in service development, leadership and research. A number of national position statements on occupational therapy offer further agreement on the core aspects of the role.23 –27
The free text responses in the survey enabled respondents to explain their role in more detail. The important contribution made by occupational therapy in enabling people to participate in valued activities while managing and adjusting to deterioration and death was consistently highlighted, again in consensus with international literature.3,5,6,21,28 Respondents felt that they had key roles in facilitating discharge home and helping patients and caregivers manage self-care through education, symptom management and equipment prescription and provision, but at the same time expressed frustration that their role was ‘limited’ to this. Respondents commented that they could contribute more to supporting patients fully in all aspects of life-limiting illness if they were given the opportunity to do so. They routinely adopted an holistic and client-centred approach to goal setting and problem solving and attending to daily occupations that people found fulfilling and enjoyable (creative and leisure occupations and work), going beyond those which were necessary for basic survival (eating and keeping clean). This is a common frustration for OTs in palliative care8,10,22 and is perceived to be influenced by other health professionals’ limited understanding of the full range of occupational therapy interventions.8,11,22 Paradoxically, however, respondents also reported reluctance to publicise the scope of their role for fear of being not being able to meet the anticipated need.
On the face of it, this leaves therapists in a ‘Catch 22’ situation: they feel unable to develop their role without the understanding of others in the MDT but cannot raise awareness of their potential for fear of being overwhelmed by the demand. The implications here are twofold. OTs could recognise that demand outstripping supply is a persuasive argument for increasing resources and use this as the basis for a business case to increase resources for services. Furthermore, managers and advocates of occupational therapy in palliative care could recognise the dilemma and support their occupational therapy staff and colleagues to identify unmet need to promote their services. However, two further issues should be noted here. First, the dynamics around the provision of occupational therapy in palliative care are likely to be more complex than expanding other professionals’ perception of the role. Second, the ability to simply provide basic services would be welcomed by therapists in countries with less well-developed palliative care services or where there were very few OTs working in palliative care.
Some challenging issues alluded to in free text survey responses warrant further exploration in future research. Ensuring that services are relevant to service users and make the best use of available resources requires clear knowledge of the needs and priorities of both service users and service providers. Therapists must ensure that therapy needs and client goals are elicited from clients themselves and not assumed by therapists. Systematic screening for these needs is one way to ensure that both expected and unanticipated needs are identified, and respondents highlighted the importance of timely referral and assessment. A number of articles support the importance of optimising function from both clinician5,28,29 and patient standpoints,6,30 emphasising the need to take a holistic approach to enabling normal routines and participation in everyday activities.5,31 For example, support for patients to remain in work or achieve a positive withdrawal from work has received limited attention in palliative care, but as people with advanced disease survive longer, employment support becomes more important. This is an emerging area in palliative care that warrants focused attention. 32
Survey results showed a marked contrast in time allocated to patient care versus research and service development. The World Federation of Occupational Therapists (WFOT) 2013–2018 Strategic Plan identifies capacity building in research, education and support of emerging areas of clinical practice as a worldwide priority. 33 Development of collaborative and creative relationships between researchers, clinicians and employers is essential to support this in occupational therapy in palliative care. 34
Limitations of this study
A number of factors must be taken into consideration when interpreting findings. It is not possible to estimate the response rate, as there are no data available for the number of OTs working in palliative care in Europe. More survey respondents came from the United Kingdom and Ireland, and more of these respondents reported working full-time in palliative care. They were also older and more experienced than respondents from other European countries. This was due in part to limited palliative care services and small numbers of OTs in a number of countries. All survey questions were in English, and no funding was available for translation which may have influenced responses from countries where English was a second language. Free text survey responses in this study provide context to Likert-type scale questions, but they do not provide an in-depth exploration of issues identified. It is also possible that free text responses may come from a self-selecting group of respondents so may not be representative of the survey population and therefore not generalisable.
Conclusion
This study is the first to examine the provision of occupational therapy in palliative care in Europe. It shows that there is a shared core content of occupational therapy services in direct and indirect patient care and that priority is given to clinical care activities over teaching, service development or research. OTs understand and value their role in making it possible for people facing dying to participate as fully as they wish and are able in their everyday lives – from managing the basic fundamentals of personal hygiene to digging the flowerbeds or continuing to work – but do not feel that this role is used to its full potential. The ability of OTs to use the full range of their skills and expertise to support patients to live well while dying appears to be significantly influenced by their colleagues’ and employing organisations’ expectations and understanding of the scope of their role. This needs to be addressed in partnership between OTs, patients and carers, the MDT and palliative care service providers. A continual reframing of professional roles must occur within the context of ever-changing local and global resources and constraints. This will require targeted occupational therapy research to evaluate clinical practice which can inform clinical care.
Supplemental Material
Supplementary_Table_1_Survey_questions_Final – Supplemental material for Mapping the scope of occupational therapy practice in palliative care: A European Association for Palliative Care cross-sectional survey
Supplemental material, Supplementary_Table_1_Survey_questions_Final for Mapping the scope of occupational therapy practice in palliative care: A European Association for Palliative Care cross-sectional survey by Gail Eva and Deidre Morgan in Palliative Medicine
Supplemental Material
Supplementary_Table_2_Free_text_thematic_analysis_Final – Supplemental material for Mapping the scope of occupational therapy practice in palliative care: A European Association for Palliative Care cross-sectional survey
Supplemental material, Supplementary_Table_2_Free_text_thematic_analysis_Final for Mapping the scope of occupational therapy practice in palliative care: A European Association for Palliative Care cross-sectional survey by Gail Eva and Deidre Morgan in Palliative Medicine
Footnotes
Acknowledgements
We wish to acknowledge the invaluable support of the EAPC Board of Directors and the occupational therapists who participated in this survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.