
Abstract
Background:
Healthcare providers working in hospitals have significant exposure to patients with palliative care needs. For many patients, these needs often reflect non-specialist rather than specialist palliative care needs. Embedding a palliative care approach in acute hospital-based care however is challenging.
Aim:
To identify core indicators for the integration of a palliative care approach in hospitals.
Design:
A Delphi technique used three sequential online survey rounds. Preliminary indicators were identified in a concept analysis of a palliative care approach, and a systematic review of hospital-based healthcare providers’ views of a palliative care approach.
Participants:
An international expert panel of three key stakeholder groups (clinicians, researchers, patients/family members) participated in each Delphi round.
Results:
The Delphi participants were recruited from 12 countries; 97 individuals responded to round 1, 78 to round 2 and 72 to round 3 (74% overall response rate). Consensus was achieved (defined a priori as >70%) on 32 core indicators of a hospital-based palliative care approach, with five structural indicators (relating to infrastructure and governance), 21 organisational indicators (relating to clinical care processes) and six staff indicators (relating to training and support for healthcare providers).
Conclusions:
This study offers multi-level guidance for clinical practice, policy and research related to integration of a palliative care approach in hospitals, based on evidence and international consensus from major stakeholder groups. These core indicators provide a means to assess, review and communicate the core elements of a palliative care approach in hospitals.
It is recommended that healthcare providers should have at a minimum, a basic knowledge of palliative care.
Healthcare providers working in hospitals care have significant exposure to patients with palliative care needs but meeting these needs remains a challenge.
The Delphi technique is a well-established method of eliciting the views of stakeholders and obtaining consensus.
This paper describes the identification of core indicators for the integration of a palliative care approach in hospitals using a Delphi technique.
Thirty-two core indicators were identified comprising 5 core structural indicators (relating to infrastructure and governance), 21 core organisational indicators (relating to clinical care processes) and 6 core staff indicators (relating to training and support for healthcare providers).
These core indicators can be used as a basis to support multi-level integration of a palliative care approach within acute hospital-based care.
Further research is needed on optimal approaches to implementing a palliative care approach in hospitals
Background
It is well established that the rapidly rising demand for palliative care globally will require optimal utilisation of all components of service provision within health systems.1,2 Healthcare providers working in acute hospital-based healthcare provision have an important role in the care of people with palliative care needs. 3 Estimates indicate that the likelihood of dying in hospital varies between countries but is generally high. 4 Acute hospital-based care however has occupied a relatively ambiguous position within the provision of palliative and end of life care,5,6 and there are mixed views whether this care environment is a preferential place to die. 7 Palliative care is an approach that improves the quality of life of people and families facing the problems associated with life-limiting illness. The palliative care approach focuses on the prevention and relief of suffering by means of assessing and treating pain and other physical, psychosocial or spiritual problems and all healthcare providers should have, at a minimum, basic knowledge of palliative care.8,9 Although competencies are available to support health care staff to self-assess, develop and maintain skills, knowledge and attributes required for the provision of palliative care, 10 the reporting of unmet palliative care needs in hospitals continues to be a concern where the momentum of care is towards rescue, resuscitation and lifesaving interventions.11 –14 Evidence, however, suggests that interventions which reflect a palliative care approach cannot be easily packaged and implemented within acute hospital-based care without careful attention being given to the complexities of the culture and context of that environment. 15 Studies of healthcare providers in hospitals working outside of specialist palliative care services have highlighted difficulties such as recognising those with palliative care needs and engaging in conversations with patients regarding poor prognosis,16 –18 complex and uncertain disease trajectories, 12 role uncertainty and integrating palliative care within an acute care workload,8,9 as issues which contribute to difficulties in providing palliative care in this setting. Increasing the capacity to support a palliative care approach for those with chronic and life limiting conditions, within acute hospital-based clinical practice necessitates a major change in core assumptions about the organisation and provision of acute care, requiring a multi-level approach to change.12,19
The term ‘integrated palliative care’ is described as bringing together aspects such as organisational, clinical and service elements to provide continuity of care between all those involved in the care network of patients receiving palliative care. 20 The body of evidence pointing to the integration of palliative care early within acute care largely emanates from intervention studies relating to the integration of specialist palliative care services.21 –23 Furthermore, although there have been calls to measure and evaluate the effectiveness of a palliative care approach,24 –26 in principle it is very difficult to evaluate quality of care without clear understanding as to what that care consists of in practice. Clinical indicators are a means to achieve this and are used for a variety of purposes to support the quality and safety of health services. 27 For the purposes of this study, an ‘indicator’ of a palliative care approach is considered a statement that describes an aspect of a palliative care approach which is relevant within the hospital care environment. The processes for developing previous indicators relating to palliative care were examined to identify areas for improvement and guide the development of indicators of a palliative care approach in hospitals in the current study. In a previously conducted review of palliative care quality indicators, 28 only one example of specialist palliative care hospital-based indicators was identified. 29 Most of the quality indicators of palliative care identified in this review reflected care processes and outcomes, with very few that reflected structural aspects which support quality palliative care provision. 28 Therefore, important contextual concerns such as infrastructure and resources which will affect the integration of palliative care were not considered. 30 Furthermore, it has long been established that the perspectives of patients and families should be encouraged in the definition and adoption of indicators of good palliative care from all dimensions of care.31,32 However there was little evidence of patient and/or family involvement in the development of previous hospital-based palliative care quality indicators, 29 and little attention has been given to the patient and family perspective in developing guidance for the integration of a palliative care approach in hospitals. 33 The aim of this study was to achieve consensus on essential (core) indicators which provides direction for hospital provision to integrate a palliative care approach within all levels of the organisation from the perspectives of all key stakeholders.
Methods
To achieve the study’s aim, a three-round international online Delphi survey was used. This is a well-established formal consensus method, which enabled the inclusion of international experts in a cost effective and efficient manner. 34 The Delphi method is especially useful where participants can express views anonymously in an iterative process, without being unduly influenced by Hasson and Keeney 35 and Vernon 36 In doing so the perspectives of multiple key stakeholders associated with a palliative care approach in hospitals could be ascertained efficiently, and over a relatively short duration of time. This study was guided by Conducting and REporting Delphi Studies (CREDES). 37
Identification of initial indicators
This study had three distinct, yet complimentary phases (see Figure 1). Phase I involved a principle-based concept analysis of a palliative care approach. This analysis of 124 sources of evidence yielded information about terminology associated with a palliative care approach, how this approach is currently understood and described the key attributes of a palliative care approach under the four broad philosophical perspectives of epistemology, pragmatism, logistics and linguistics. 9 Phase II involved a qualitative systematic review of 37 studies, 8 representing the views of 985 healthcare providers in hospitals which reported on the experiences, barriers and facilitators of integrating a palliative care approach to understand relevant contextual issues. 8
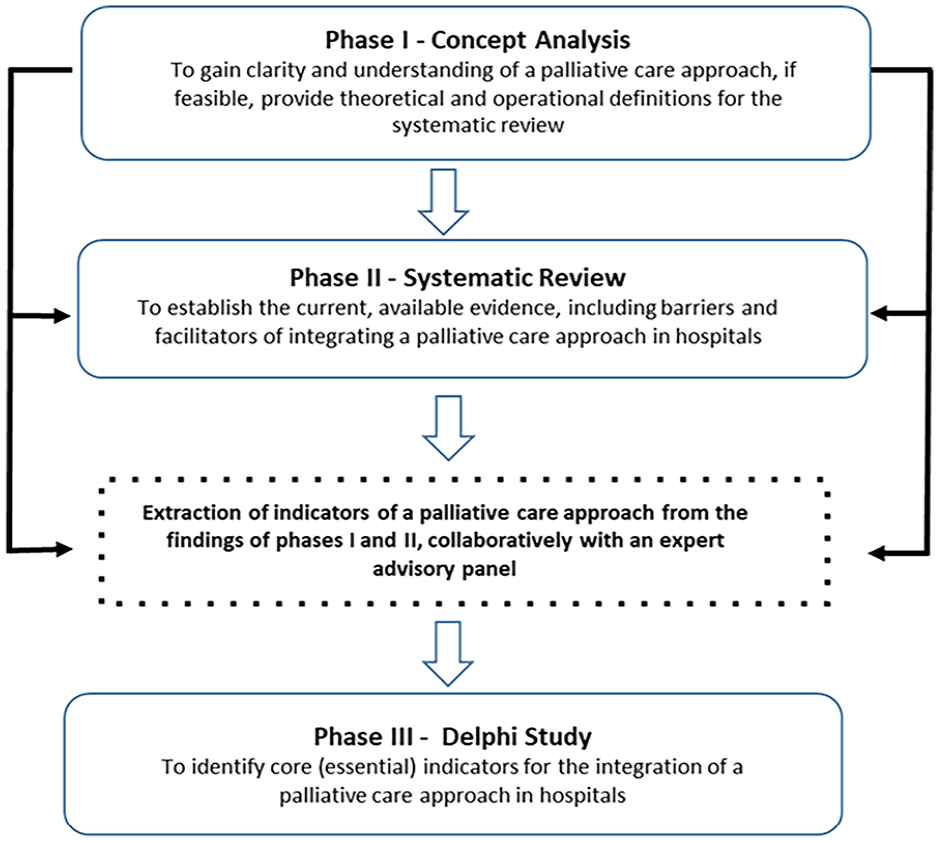
Research phases to identify core indicators for the integration of a palliative care approach in hospitals.
Phase III began by scrutinising the findings from phases I and II, separately, rewording the findings into short summary statements which relate to indicators of a palliative care approach in the hospital setting, and deriving clear, concise indicator statements to develop the initial indicators for use in a Delphi survey. After deriving the initial indicator statements, these were further scrutinised for similarity and overlap and combined, as appropriate to provide the complete list of preliminary indicators of a palliative care approach for hospitals. The indicators were then divided into three sections. Those indicators that related to the infrastructural or strategic governance systems within a hospital were combined into one category. Indicators related to clinical policies, guidelines or care processes were combined into a second category. Finally, any indicators that related to activities of individual hospital staff were categorised together.
To enhance rigor, an advisory panel was established to provide input and advice on the initial indicators and the round one Delphi survey instrument. The panel consisted of a hospital-based clinician, a palliative care researcher, a person with a chronic illness, a Delphi researcher, the medical director of a clinical audit department in a large acute care hospital setting, and an end-of-life care co-ordinator of a large acute care hospital setting. The role of the panel was to review the list of preliminary indicators and to provide feedback in accordance with their individual expertise in relation to their structure, clarity, appropriateness and readability. The development (extraction, scrutiny, categorisation, advisory and refinement) process culminated in the
Population, sample and recruitment
For the purposes of this study, the Delphi technique was used to elicit broad expertise and perspectives on the topic. It is advantageous to include heterogenous groups of experts with a wide understanding of the area in question. 36 Therefore, three stakeholder groups of experts were identified as; service users of a palliative care approach in hospitals, hospital-based healthcare providers and researchers/policy makers in palliative care. The Delphi survey was designed online and made available using SurveyMonkey©. Round 3 recruitment was completed in June 2019. Invitation emails, inclusive of a link to the online Delphi survey, were sent to the ‘contact us’ details of palliative care advocacy organisations, and chronic illness organisations internationally with a request to disseminate the invitation email to their members. Furthermore, the contact details of the first authors of all publications sourced for phases I and II, and any policy documents relating to a palliative care approach were identified, and an invitation email was distributed to these individuals. Snowball sampling was achieved by asking participants to forward the link to others who might have the necessary expertise to participate in the study. Informed consent was provided by participants by ticking the ‘I consent to take part’ box which was made available in each Delphi round. Ethical approval to conduct the study was granted by the Research Ethics Committee of the lead author’s University.
Data collection
For rounds 1 and 2, a 5-point categorical rating scale ranging from Strongly Agree to Strongly Disagree was utilised to ascertain participants’ level of agreement as to whether each indicator statement presented was considered essential (core) for a palliative care approach to occur in hospital. Consensus in rounds 1 and 2 was based on ⩾70% of the participants in at least two of the three stakeholder groups indicating either strongly agree or agree to each indicator statement. This was to ensure that one stakeholder group did not dominate the consensus. 38 This definition of consensus (⩾70%) is also consistent with previously conducted Delphi studies in palliative care.39,40 Participants were also offered the opportunity, in round 1 to propose additional core indicators not already in the list. Any newly suggested indicators were added to round 2. To determine ‘new indicators’ suggested in round 1, the suggestions were read and re-read to identify overlap and potential duplication of content and words, and terms that conveyed similar meaning were grouped. 41 Respondents to round 1 were sent the round 2 survey and were invited to re-rate all indicators provided to them in round 1, and rate any newly added indicators using the same round 1 rating scale. The opportunity to revise previous scores in light of previous ratings is an important element in consensus in a Delphi study.42,43 Therefore, in round 2 participants were presented with a table alongside each indicator with each group’s round 1 percentage level of agreement. Aligning with consensus methods, only those indicators that reached at least 70% agreement, in at least two participant groups at the end of round 2, were sent forward to round 3. To further channel participants into deciding whether an indicator was considered core or not, in round 3, the 5-point Likert scale was replaced by YES/NO response options whereby YES is chosen if a participant deems this absolutely essential as a core indicator for the integration of a palliative care approach in acute hospitals. Consensus on the final core indicators was ⩾70% agreement ‘YES’ in at least two participant groups.
Data analysis
To maintain momentum in the process, and guard against participant apathy, the results for each round were analysed and the links for access to the rounds 2 and 3 surveys were circulated to those participants who participated in the previous round one week after the official close of that round. Two reminder emails were sent to non-responders during rounds 2 and 3 1 week apart. SPSS® version 25 was used to analyse the data in each round which included the response rates for each round (counts), percentages for each level of agreement, at group level, for each indicator (i.e. strongly disagree to strongly agree), and median scores, which are recommended to be reported in Delphi studies. 44
Results
Participation in the study
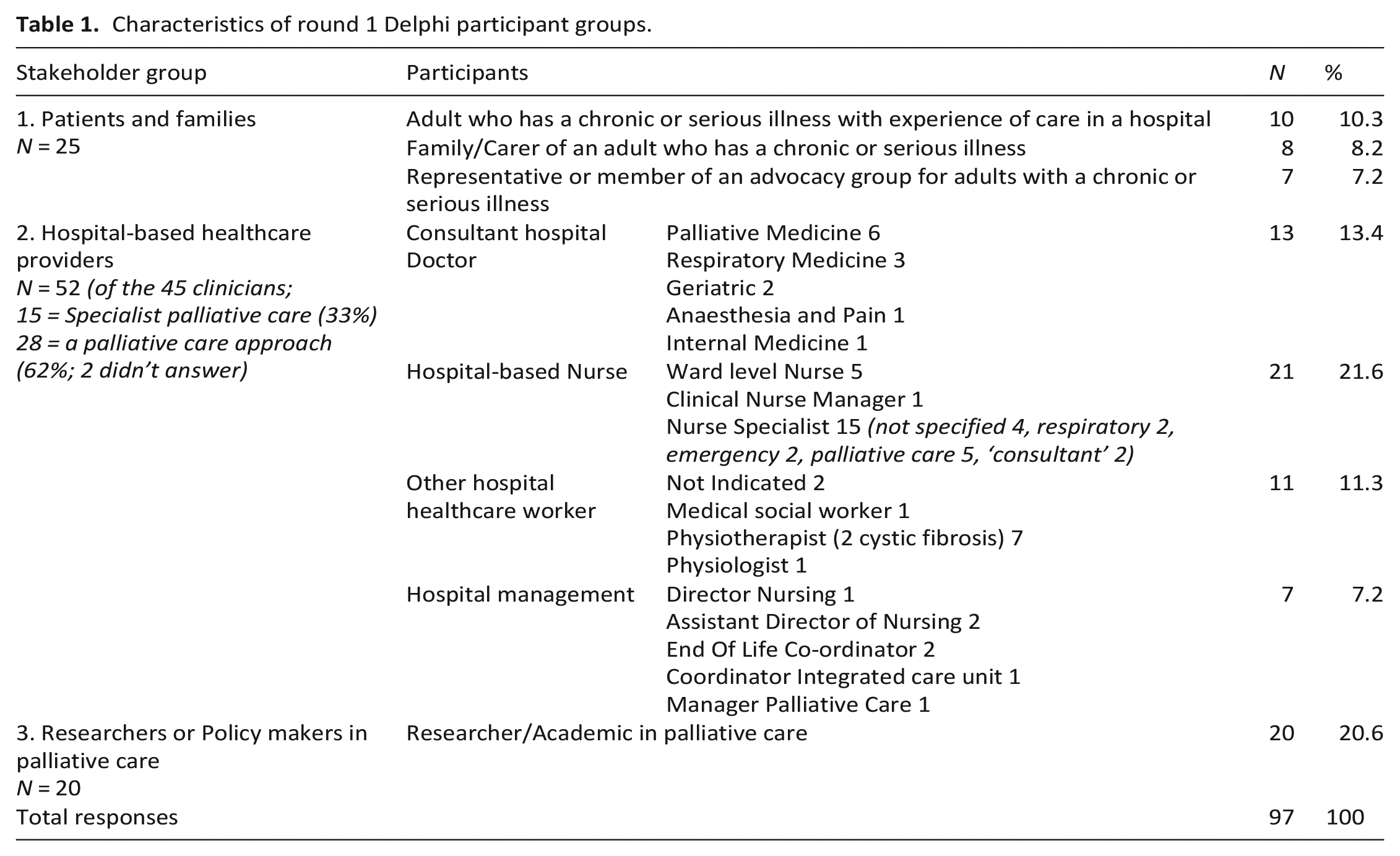
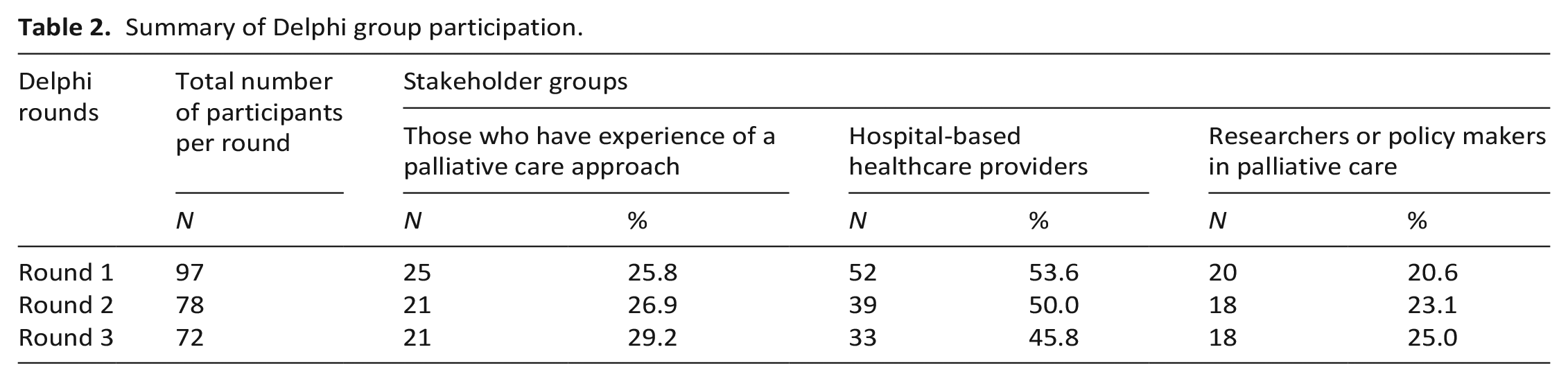
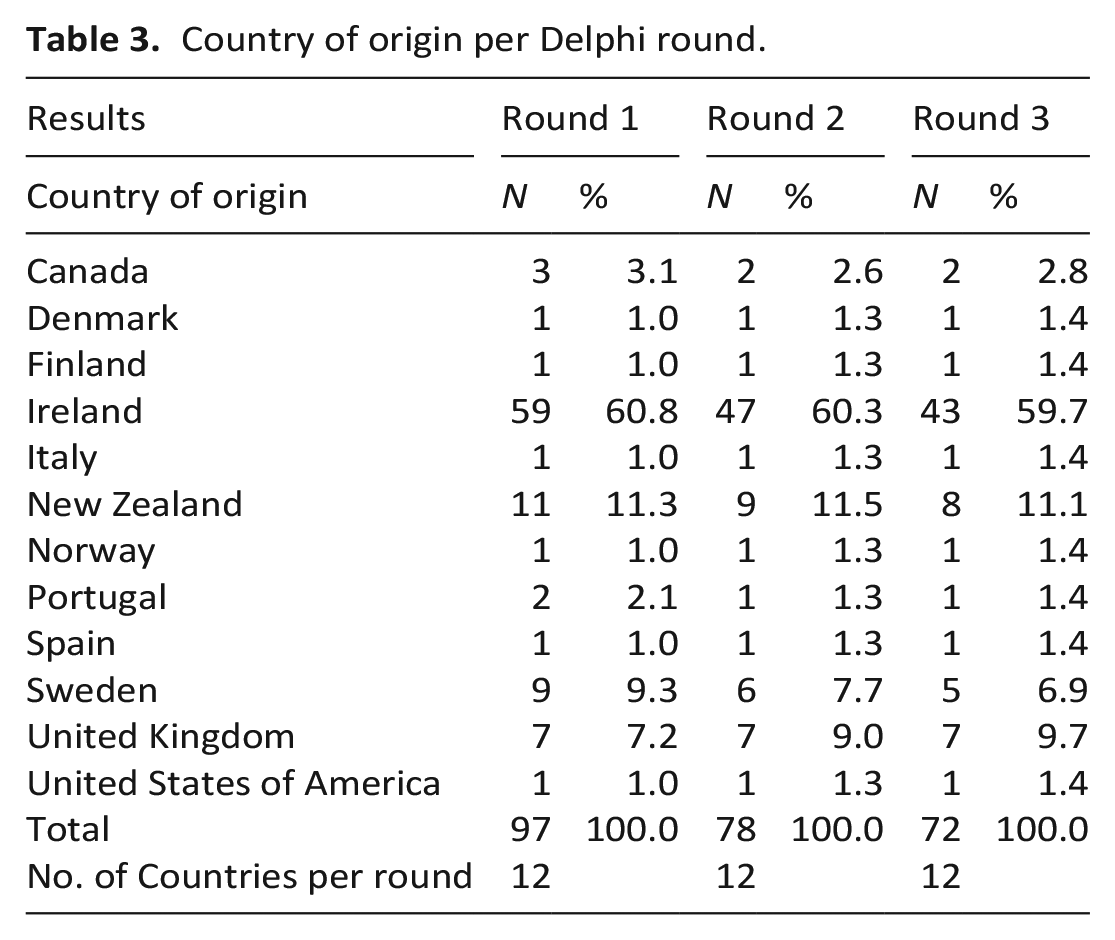
Ninety-seven individuals from 12 countries responded to round 1. Of these, 78 (82%) responded to round 2, and of these 72 responded in round 3 (overall response rate of 74%). The characteristics of the respondents in round 1 are presented in Table 1. The breakdown of each expert group over the three rounds is provided in Table 2, while Table 3 provides details of the countries of origin in each round of this Delphi study.
Characteristics of round 1 Delphi participant groups.
Summary of Delphi group participation.
Country of origin per Delphi round.
Delphi rounds
Round 1 Delphi results
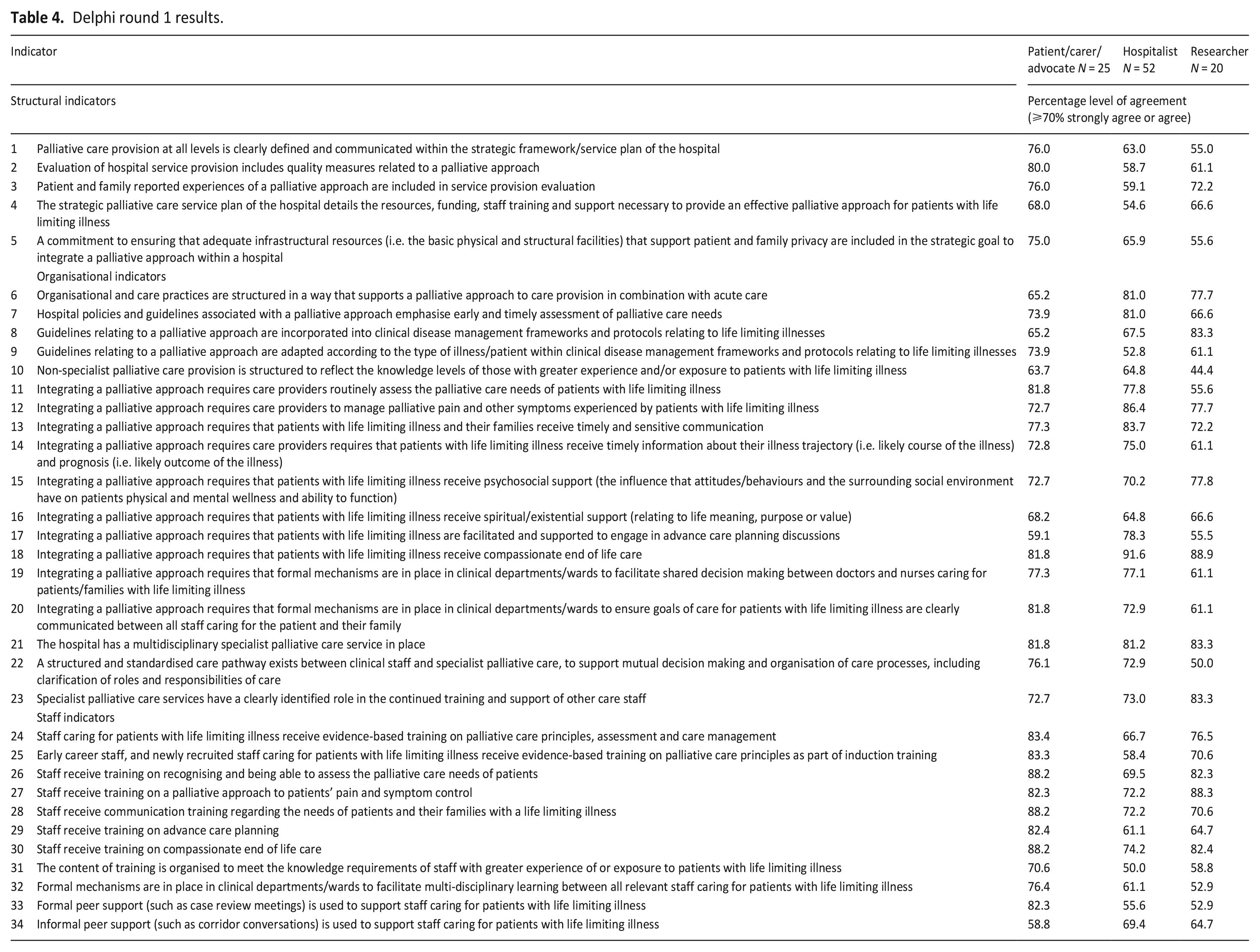
Table 4 presents the results of the 34 indicators rated in round 1. Indicators that achieved ⩾70% agreement (either strongly agree or agree) in at least two participant groups were deemed to have achieved consensus. Consensus was achieved for 20 of the 34 round 1 indicators, specifically 1 of the 5 structural indicators, 13 of the 18 organisational indicators and 6 of the 11 staff indicators.
Delphi round 1 results.
Round 2 Delphi results
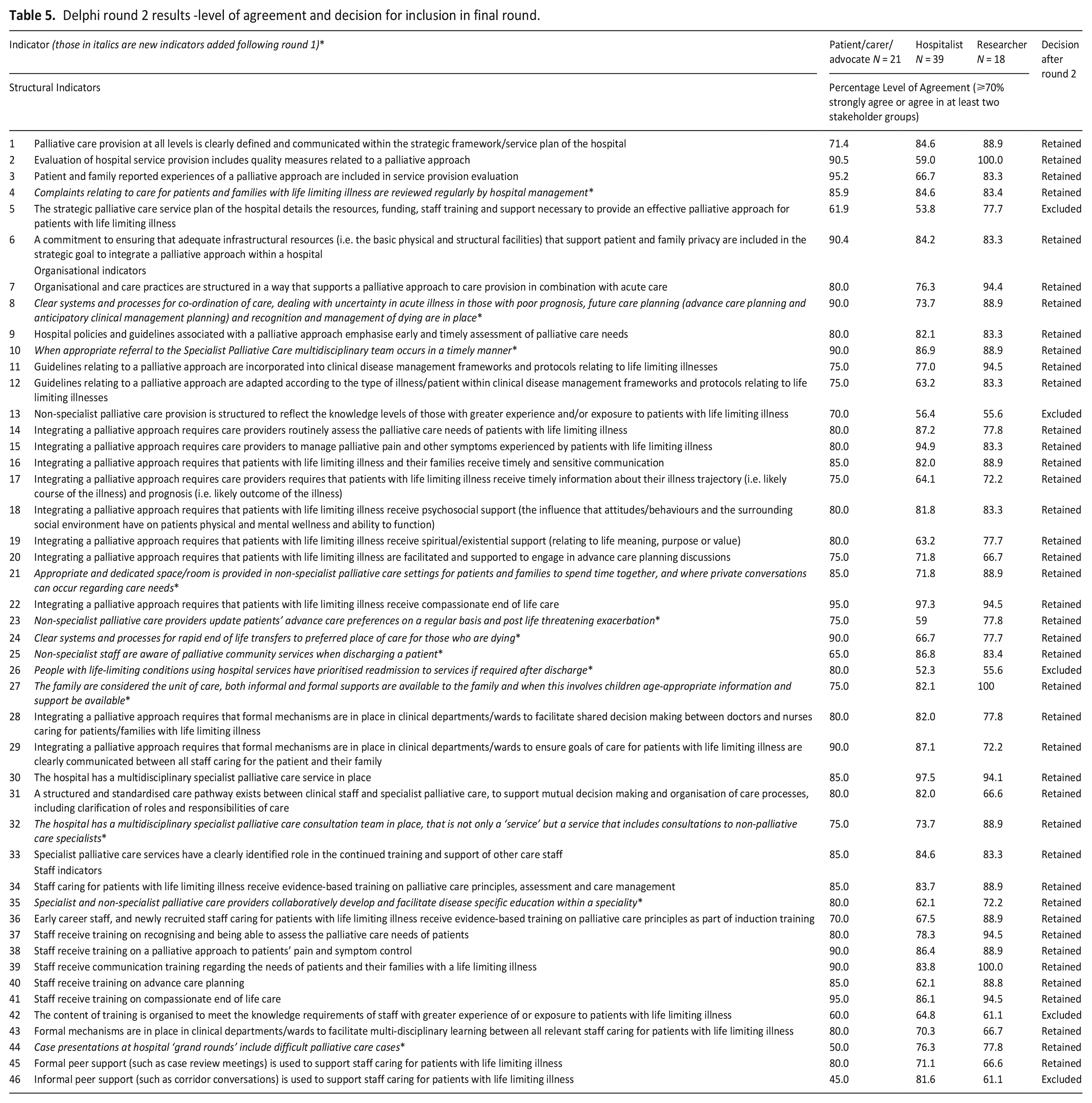
Participants were provided with the results of round 1 for review and re-rating. From the ‘additional indicators’ section of round 1, 12 new indicators were identified and aligned to the relevant indicator category. This produced one structural, nine organisational and two new staff category indicators, providing, overall, a list of 46 indicators for rating in round 2 (6 structural, 27 organisational and 13 staff indicators). In round 2, 41 of the 46 indicators achieved consensus and were thus retained for re-rating in round 3. The five indicators that did not achieve consensus were excluded from round 3. Table 5 provides the results of round 2. Indicators in italics are the 12 new indicators identified from round 1.
Delphi round 2 results -level of agreement and decision for inclusion in final round.
Round 3 Delphi results
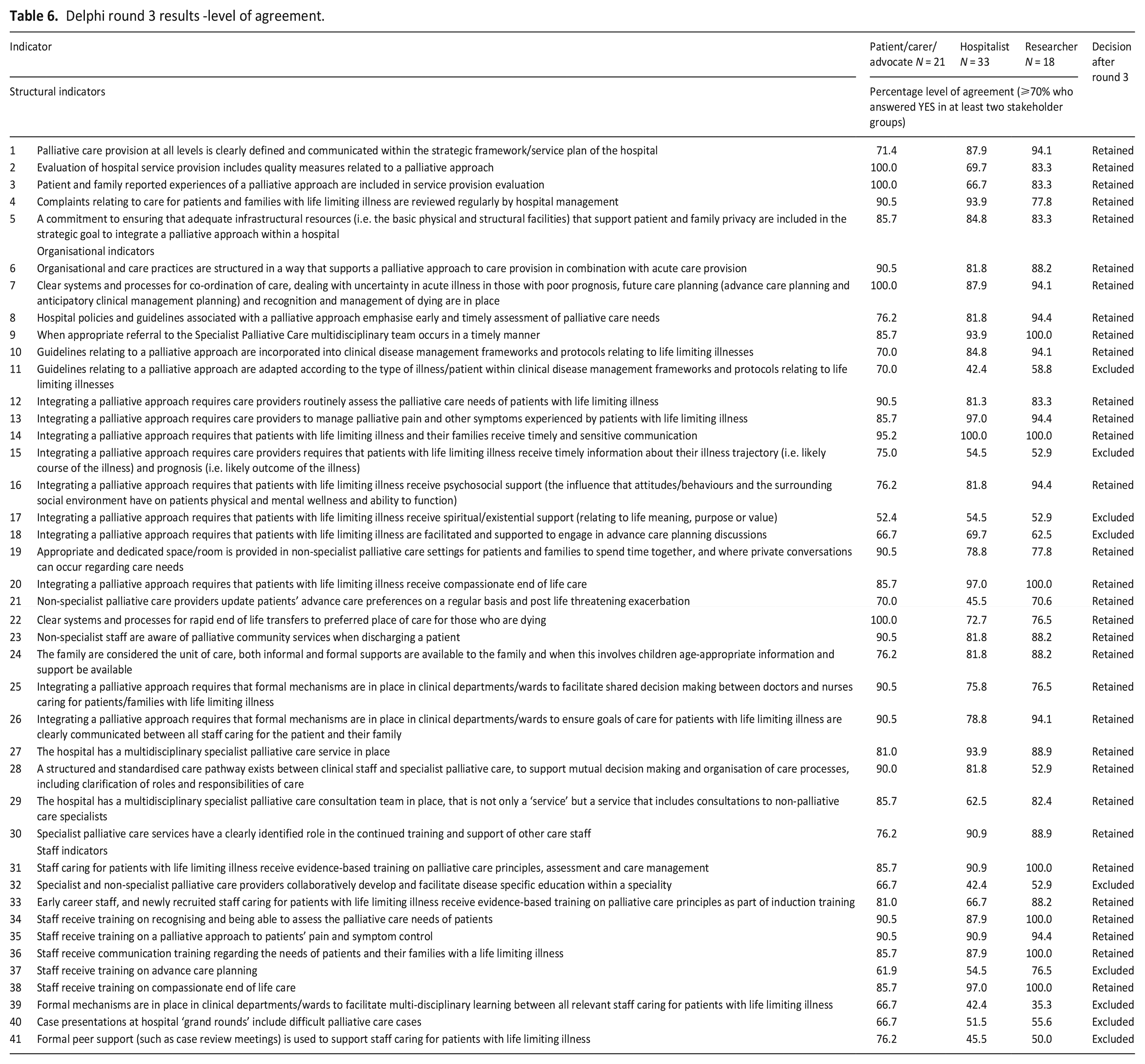
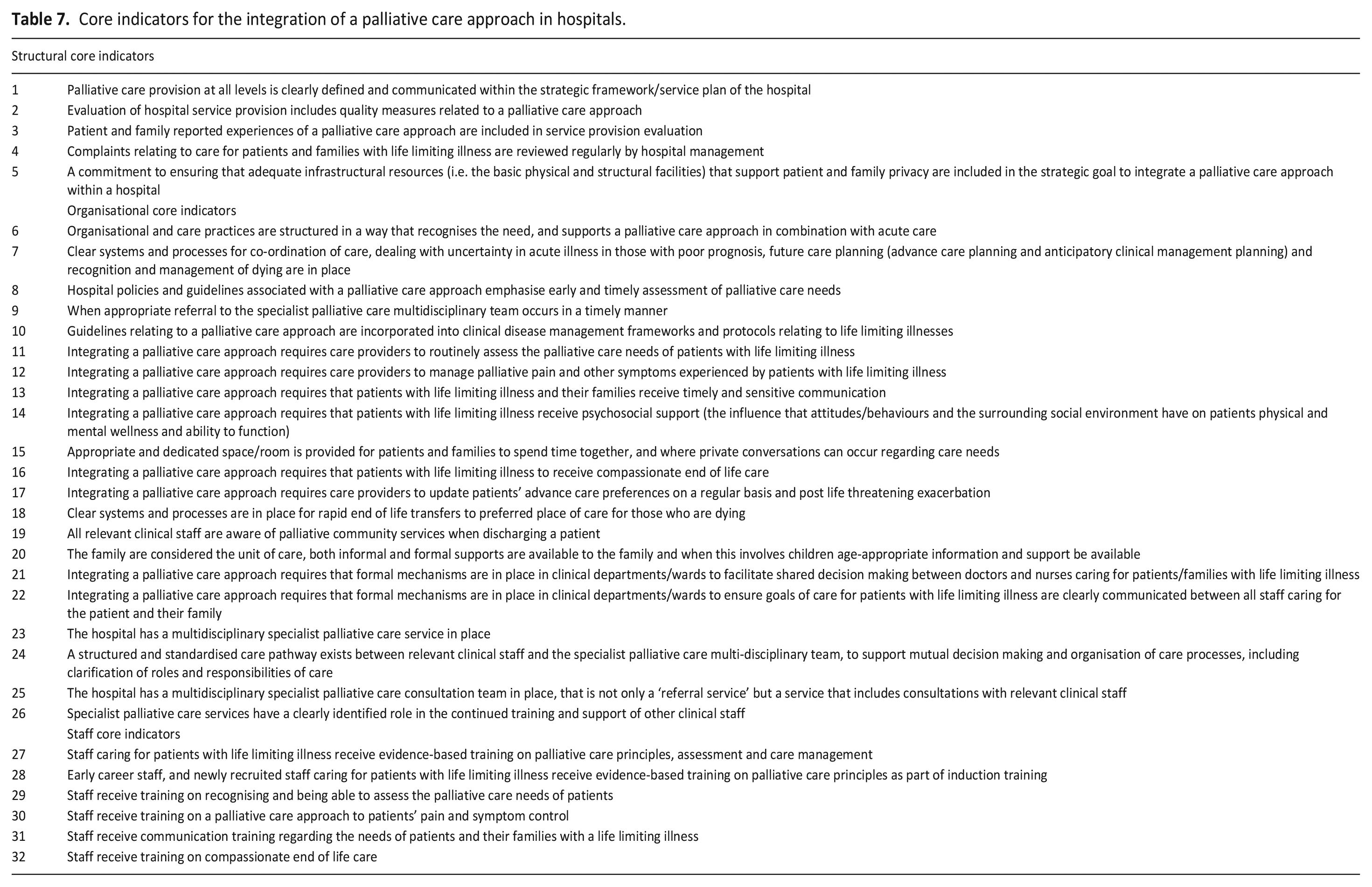
Table 6 provides the results of round 3. In round 3, the 41 indicators retained from round 2 were re-rated whereby participants were asked to indicate either ‘yes’ or ‘no’ if the indicator should be included in the final core set. Consensus (⩾70% agreement ‘yes’ in at least two participant groups) was achieved for 32 of these reflecting the final core indicators for the integration of a palliative care approach in acute hospitals (5 structural, 21 organisational and 6 staff indicators; Table 7). All 32 core indicators achieved consensus in the patient/carer/advocate stakeholder group. While 26 of the 32 core indicators achieved consensus in all three stakeholder groups. Furthermore, of the 34 indicators that were presented for rating in round 1, 21 were retained following the final round indicating a high degree of stability between Delphi rounds.
Delphi round 3 results -level of agreement.
Core indicators for the integration of a palliative care approach in hospitals.
Discussion
Consensus was achieved on 32 core indicators for the integration of a palliative care approach in hospitals. These reflect core activities at structural, clinical governance and individual practitioner level within this care environment. The need for multi-level engagement in the hospital setting in order to recognise and integrate palliative care has been identified in previous literature.12,45 –48 The core indicators also reflect the need for a multidisciplinary approach to incorporate palliative care principles, with the adoption of clear care co-ordination, communication structures and shared decision making between care providers. These 32 indicators have broadened our understanding of what, at its core, access to and interaction between non-specialist and specialist palliative care providers should entail to support the integration of a palliative care approach in hospitals. This suggest that hospitals at a minimum should have a specialist palliative care team in place, which facilitates fluid and timely referrals and provides support, consultation, mentorship and training for staff. This reaffirms the perceived importance of specialist palliative care services for the effective integration of a palliative care approach in hospitals highlighted in previous literature.49 –51 The importance of training on the recognition of those patients who may have palliative care needs, palliative care principles, assessment and care management for all care providers and in particular newly recruited staff and early career staff also emerged in the consensus process.
The integration of a palliative care approach, and the 32-core indicators within acute care provision in hospitals faces different challenges to that of specialist palliative care service integration. In models that focus on specialist palliative care integration 52 the palliative care input is provided by those with a shared philosophy of palliative care working within the boundaries of specialist palliative care services and units, where the main palliative care role of healthcare providers working outside of specialist palliative care is considered referral to specialist palliative care. However, increasing the capacity of healthcare providers outside of specialist palliative care services to provide palliative care, as reflected in these core indicators, care providers within the acute biomedical ‘cure’ focused service provision in hospitals must assume a duality of roles by also integrating the fundamentally different view of ‘heal’ into their practice. The concern about whether it is feasible to incorporate a palliative care approach within hospitals has been raised by several authors.12,53,54 Adopting a whole system approach through the identification of structural, organisational and staff indicators may provide a means to recognise the need and support this integration in clinical practice.
The acute care environment however is a complex ecosystem. 55 Even though individual hospital departments may serve separate functions in acute patient care, recognising that all healthcare providers working in hospitals have a role to play in the provision of a palliative care approach is essential. 10 Exploration of a palliative care approach in previous studies within hospital departments such as the emergency department56,57 and intensive care48,53 support this, and highlight that while specific clinical priorities may occur between hospital departments, there is consistency in the fundamental palliative care philosophical approach to the patient. Consensus in this study was achieved on ‘what’ the core aspects of integrating a palliative care approach in hospitals requires through the identification of 32 core indicators. Further inquiry is required to establish ‘how’ they can be operationalised for use. This will likely require multi-level engagement involving rigorous examination of the core indicators within hospital structures, services and departments to ascertain how they may be integrated into a hospitals quality improvement system and quality standards reviews. Thus the 32 core indicators can be used as a basis to establish key outcome measures and quality indicators that could be used to evaluate the effectiveness and quality of an integrated palliative care approach in hospitals.
While 26 of the final 32 core indicators achieved consensus in all three stakeholder groups, indicating a high degree of consensus, 5 of the final core indicators did not achieve ⩾70% Agreement in the hospitalist stakeholder group and 1 did not achieve ⩾70% Agreement in the researcher stakeholder group. This suggests that differences exist between key stakeholders about the meaning and value of a palliative care approach in hospitals. The clinical application of these core indicators should be explored further from the perspective of how care is provided, and experienced by patients and families, recognising the variations and diversity that exists in palliative care provision in hospitals not only between countries, but also within-countries. 58
Strengths and limitations
The strengths of this study include the rigorous completion of two initial phases to identify a preliminary list of indicators of a palliative care approach.8,9 Also, of the 34 indicators that were presented for rating in round 1, 21 were retained following the final round indicating a high degree of stability between Delphi rounds. The inclusion of three diverse groups of international stakeholders’ views which included patients and families, and the overall retention rate of 74% represents further strengths of the findings. Several limitations are identified; participants were overwhelmingly from Ireland, and the findings are representative of the twelve countries who participated and may not be representative of other countries. Furthermore, the survey was only available online and in English, which may have limited the scope of participation.
What this study adds?
These core indicators provide multi-level guidance to support the recognition and integration of a palliative care approach in hospitals. They provide a basis to assess, review and communicate the essential elements required to integrate a palliative care approach within hospitals. Contextual factors such as national palliative care policy, funding and organisation culture 58 for example must be considered in relation to the clinical applicability and operationalisation of these core indicators in practice.
Conclusions
The core indicators of a palliative care approach identified in this study reflect the fundamental palliative perspective of total pain and whole person care, highlighting the importance of a multidisciplinary palliative care approach in hospitals and the importance of the interface between non-specialist and specialist palliative care. One of the fundamental challenges for healthcare providers is recognition of the importance and value of integrating a palliative care approach within acute care. This study has established consensus on what the core aspects of a palliative care approach in acute care hospitals are. Further research is needed to understand how these core indicators of a palliative care approach can be operationalised for use in clinical practice.
Footnotes
Acknowledgements
We are grateful to all respondents who participated in the Delphi study. We acknowledge the important intellectual contribution of Prof Geralyn Hynes during the initial phases of this research project.
Author contributions
Mary Nevin and Valerie Smith made substantial contributions to the concept and design of the study. Mary Nevin undertook data collection and analysis, drafted the article and approved the final version for publication. Valerie Smith and Sheila Payne critically revised the article for intellectual content and approved the final version for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Health Research Board Ireland, Research Training Fellowship for Healthcare Professionals (Reference HPF/2015/968) awarded to the lead author Mary Nevin.
Ethical approval and consent
Ethical approval to conduct the Delphi study was obtained from the School of Nursing and Midwifery Research Ethics Committee, Trinity College Dublin (Ref: 18052018).
Availability of data and materials
All data are archived at Dublin City University and may be obtained from the corresponding author