
Abstract
Background:
Patients with advanced diseases often experience deficient continuity of care. Although integrated palliative care promotes continuity of care, it is not clear how it can be optimized to improve continuity of care experiences.
Aim:
To examine how relational, informational and management continuity of care are experienced by patients with advanced diseases and their family caregivers receiving care from several integrated palliative care initiatives in five European countries.
Design:
We adopted a longitudinal qualitative study design including two interviews (interval 3 months) with patients and family caregivers focusing on how health care professionals responded to their needs. Interviews were audio-recorded and transcribed verbatim. Analysis involved a two-step qualitative content approach.
Setting/participants:
A total of 22 integrated palliative care initiatives (established local palliative care collaborations) were selected in Belgium, Germany, Hungary, the Netherlands and the United Kingdom. We recruited 152 patients (63% cancer, 24% chronic obstructive pulmonary disease, 13% heart failure; life expectancy <1 year; mean age 68 years, 56% female) and 92 family caregivers (mean age 61 years, 66% female).
Results:
Trusted relationships with a small number of key health care professionals to receive tailored care and easily access help were essential. Relational continuity was often deficient, especially with general practitioners. Although informational and management continuity was often lacking in care provision, collaborative integrated palliative care initiatives were related to consistent and coherent care.
Conclusion:
Patients and family caregivers most likely experience continuity of care by having a small number of trusted health care professionals who are available, provide multidisciplinary care and regularly transfer information to all health care professionals involved. Optimizing continuity of care requires further integration of integrated palliative care initiatives with other health care professionals involved in the patients’ care networks.
Keywords
Integrated palliative care has the potential to improve continuity of care experiences which are often at stake within the context of palliative care.
Collective team approaches have added value for patients’ and family caregivers’ experiences of security.
For patients and family caregivers, it is essential to have trusted relationships with a small number of key health care professionals in order to receive tailored care and easily seek help when needed.
Multidisciplinary care provision could jeopardize patients’ and family caregivers’ need to have trusted relationships with key health care professionals, particularly those with general practitioners.
Collaborative integrated palliative care initiatives are likely to improve patients’ and family caregivers’ experiences of informational and management continuity.
Integrated palliative care initiatives should identify a small number of trusted key health care professionals who are readily available and contactable by patients and family caregivers.
General practitioners should be more involved in leading multidisciplinary care provision for patients with palliative care needs.
Integration of integrated palliative care initiatives with health care professionals involved in patient’s care networks should be enhanced in order to optimize experiences of informational and management continuity.
Introduction
Continuity of care is associated with lower rates of emergency department visits,1,2 decreased hospital deaths3,4 and supportive needs being met. 5 It is a key issue in health care policy and organization6,7 and is crucial for patient experiences with health care.8,9 However, continuity of care is often at stake in care provision for patients with advanced diseases who usually receive care from multiple health care professionals.9–13 Lack of continuity of care can cause undesired experiences with palliative care provision, for example, feeling unsafe during illness transitions, 9 patients being transferred between multidisciplinary teams 11 and suboptimal support for problems and needs.12,13
Integrated palliative care has been increasingly proposed in order to achieve continuity of care for patients with advanced diseases.14,15 Integrated palliative care focuses on coordinating care around the needs of patients with advanced illnesses.16,17 Integrated palliative care approaches have shown promising results, not only in terms of continuity of care but also with regard to quality of life, survival rates and cost-effectiveness.15,18–20 However, it is not clear how integrated palliative care efforts improve outcomes such as continuity of care 21 making it difficult to inform health care policies. 22 Extensive research has been conducted on how continuity of care is achieved within chronic disease management and mental health.23–28 This has resulted in a widely recognized definition of continuity of care: ‘the extent to which a series of health care services is experienced as connected and coherent and is consistent with a patient’s health needs and personal circumstances’. 29 Three interrelated dimensions of continuity of care have been distinguished: (1) relational continuity referring to having ongoing therapeutic relationships with one or more providers, (2) informational continuity referring to the use of information about past events and personal circumstances to make current care appropriate for each individual and (3) management continuity referring to a consistent and coherent approach to the management of a health condition that is responsive to a patient’s changing needs. 29
As patients and family caregivers can have an important role in securing continuity,30,31 examining their perspectives on how continuity of care is achieved is essential. Furthermore, continuity of care is a complex multidimensional concept, and therefore obtaining insight into patients’ and family caregivers’ perspectives on this concept requires qualitative investigation.32,33 Limited qualitative research within the context of palliative care suggests that maximized continuity of care at all three levels relates to positive care experiences8,10 and that collective team approaches may have added value. 34 However, there is a need to further investigate how health care professionals can optimize integrated palliative care to improve continuity of care experiences. Therefore, this article examines how relational, informational and management continuity of care are experienced by patients with advanced cancer, chronic obstructive pulmonary disease (COPD) or heart failure and family caregivers receiving care from integrated palliative care initiatives in five European countries.
Methods
Design
We used a longitudinal qualitative study design which was part of a multiple embedded case study conducted by the European InSup-C project that aimed to identify prerequisites for integrated palliative care. 35 We choose this design in order to explore the in-depth views of patients and family caregivers about the care they receive from integrated palliative care services and other health care professionals involved over time.
Recruitment
We selected integrated palliative care initiatives in five European countries (Belgium, Germany, Hungary, the Netherlands and the United Kingdom) using uniform selection criteria (Table 1) and an integrated palliative care working definition:
Bringing together administrative, organisational, clinical and service aspects in order to realise continuity of care between all actors involved in the care network of patients receiving palliative care. It aims to achieve quality of life and a well-supported dying process for the patient and the family in collaboration with all the caregivers, paid and unpaid.
36
Selection criteria for integrated palliative care initiatives.
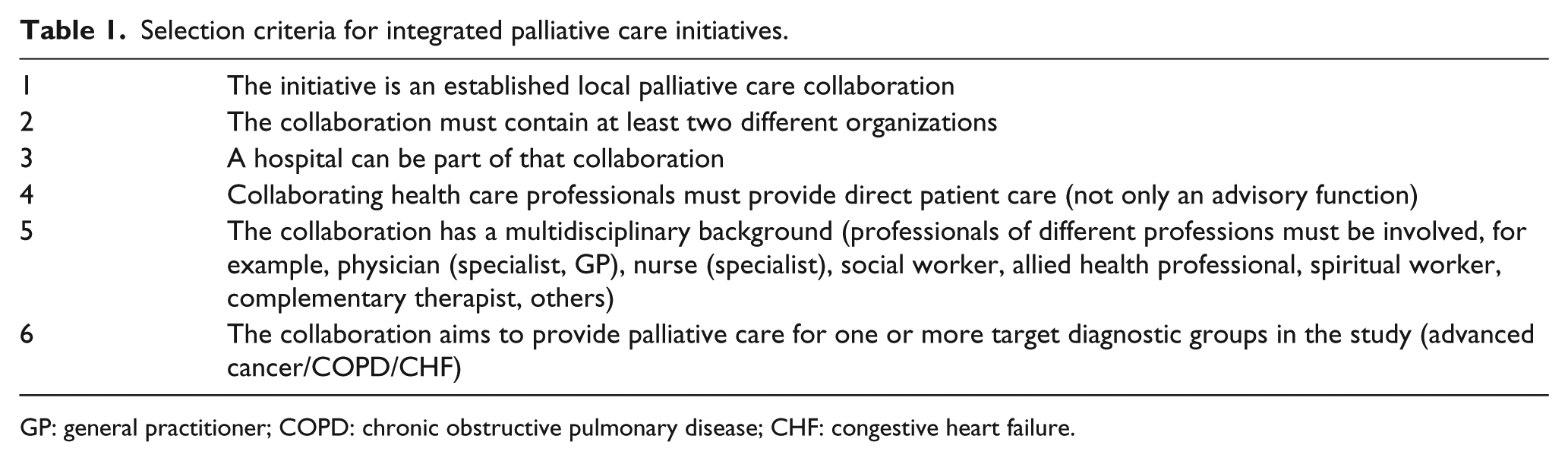
GP: general practitioner; COPD: chronic obstructive pulmonary disease; CHF: congestive heart failure.
We developed these criteria in order to have initiatives that would reflect the cross-sector and multidisciplinary nature of integrated care. From the integrated palliative care initiatives, we recruited patients and their family caregivers using inclusion criteria (Table 2). Respondents were informed about the study by their treating health care professionals. If they expressed interest in participation, they received further information and a consent form from the researcher who would conduct the interview.
Inclusion criteria for patients and family caregivers.
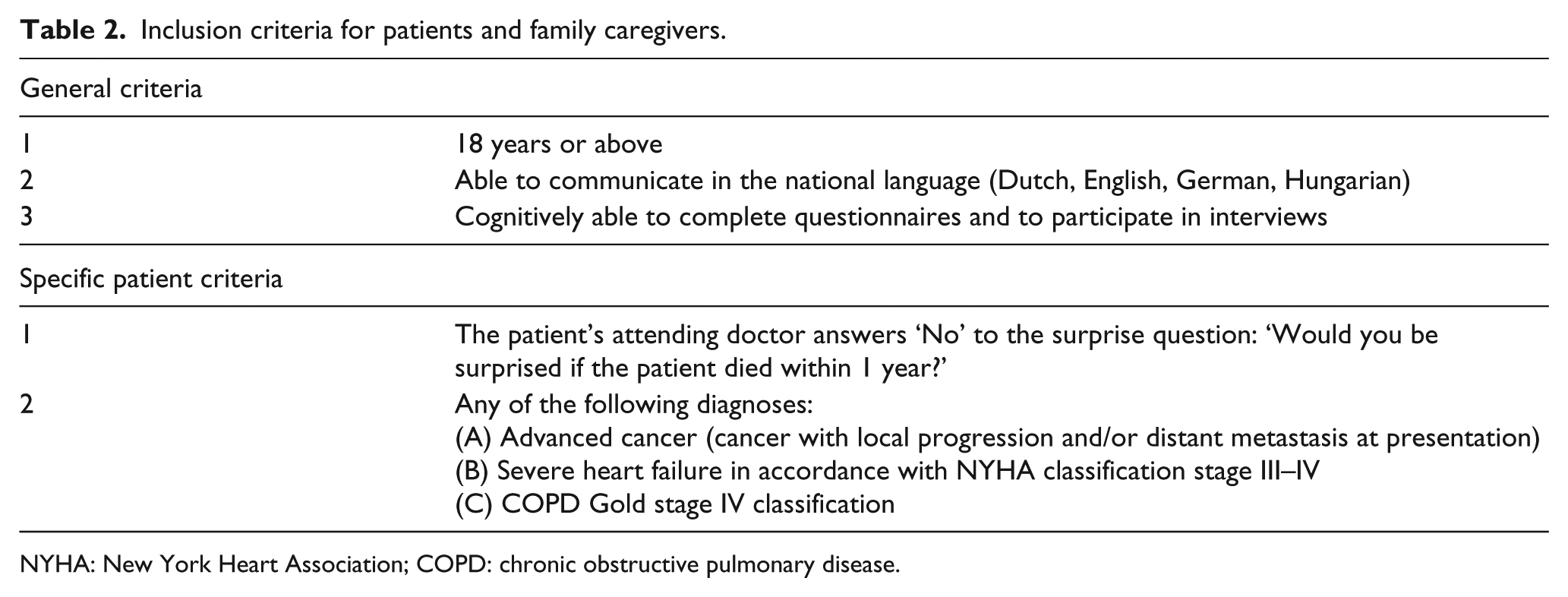
NYHA: New York Heart Association; COPD: chronic obstructive pulmonary disease.
Data collection
After obtaining written consent, patients and family caregivers participated in two semi-structured interviews with an interval of 3 months. Longitudinal interviewing allowed us to explore care experiences over time and confirm findings from the first interview. We developed a uniform interview protocol for patient and family caregiver interviews that was used by all researchers performing the interviews (Supplementary file 1). The protocol for the patient interviews focused on how health care professionals in patients’ care networks responded to their needs and included three sections: (1) problems and needs, (2) relationships with health care professionals in the patient’s care network and (3) collaboration between health care professionals. For family caregiver interviews, we used the same protocol, but we asked them to answer the questions about the patient’s care from their own perspective. In order to support respondents in reporting their experiences with care provision in a structured way, we used a prompt card method. 37
The first two patient interviews were regarded as a pilot study. Since there was no need to change the content of the interview guide, these patients were included in the final sample. Interviews were mainly conducted at home and also at the place where patients resided at that moment (e.g. hospice or rehabilitation department). Interviews took on average 1 hour. If possible we tried to interview patients and family caregivers separately. However, when participants wished the family caregiver or patient to be present when they were interviewed, we asked the one who accompanied the interviewee to respect their perspective. Data were collected between June 2014 and August 2015. Interviews were audio-recorded and transcribed verbatim. Field notes were made during data collection and stored in the national research team’s qualitative databases.
Before starting the interviews, one group training was organized for the interviewers to enable them to collect reliable and valid data and to ensure consistency of methodology among countries. Furthermore, to reflect on the data collection and preliminary analysis, monthly Skype meetings were held with the international research team. Research ethics committee approvals were obtained in all countries (Medical Ethics Committee UH Leuven, Belgium S56893/ML11187; NRES Committee North West, Lancaster, United Kingdom 14/NW/0140; Medical Faculty Ethics Committee Rheinische Friedrich-Wilhems-Universität, Bonn, Germany 014/14; Medical Research Council Scientific and Research Committee, Hungary 21005-2/2014/EKU (194/2014)). However, in the Netherlands the study did not fall within the remit of the Medical Research Involving Human Subjects Act (WMO) and so did not require approval from an ethics committee (Medical Research Ethics Committee Arnhem-Nijmegen, The Netherlands 2013/538).
Data analysis
Interview data were analysed using qualitative content analysis 38 and comprised two steps: (1) a general analysis of the national data resulting in an international code book and (2) an in-depth analysis on continuity of care.
Step 1: general analysis
Two researchers in each country deductively coded 10 (patient, family caregiver and bereavement) interviews using a priori main themes derived from the interview protocol (Figure 1). Then the same researchers inductively coded these interviews using line-by-line coding. Line-by-line codes were clustered into sub-themes which were compared in a face-to-face meeting. A code book was created during this meeting based on the consented sub-themes. Then all interviews were coded using the code book. Regular Skype meetings were held and electronic correspondence took place in order to refine the code book until no new sub-themes emerged. Qualitative Data Software Nvivo 10 was used in order to support the coding process.
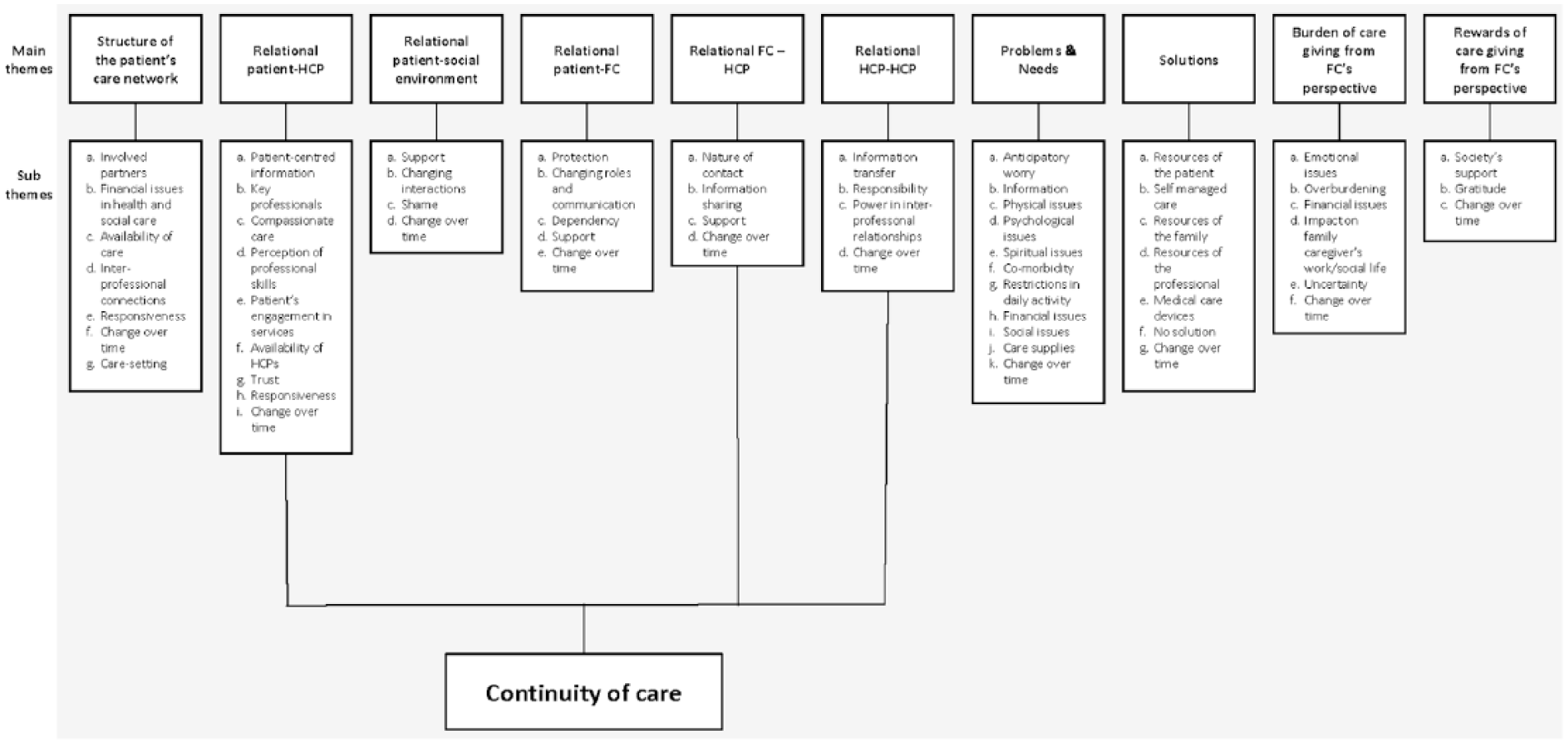
International code book.
Step 2: in-depth analysis of continuity of care
Since continuity of care emerged as an important theme explaining patients’ and family caregivers’ experiences with care provision provided by health care professionals we decided to explore this theme in depth. We used Haggerty et al.’s 29 continuity of care definition including its three dimensions as described in the introduction as a theoretical framework to allow uniform analysis and enable international comparison. Based on this framework, research teams in each country further analysed the main themes in the code book that were relevant in the context of continuity of care (main themes: relational patient–health care professional, relational family caregiver–health care professional and relational health care professional–health care professional). Quotes were added by the national teams in order to illustrate the findings. The resulting five country-specific analyses were subsequently analysed and compared by the first author and then aggregated into an overall analysis. The interpretations in the overall analysis were verified within the international research team. Due to the general vulnerability of our sample and the complex international context of our study, we did not undertake a member check of our findings.
We used the consolidated criteria for reporting qualitative studies (COREQ) checklist 39 as far as this was applicable to our study.
Results
A total of 22 integrated palliative care initiatives were included mainly involving hospital- or hospice-based services in conjunction with home care services (Table 3). In all, 152 patients participated in the study: 15 in Belgium, 34 in Germany, 37 in Hungary, 31 in the Netherlands and 35 in the United Kingdom. The mean age was 68 years, the majority were female (56%) and had cancer (63%). Most patients had their partner (59%) as family caregiver. The majority of patients (62%) also took part in the second interview. A total of 92 family caregivers participated in the interviews, 15 in Belgium, 16 in Germany, 26 in Hungary, 22 in the Netherlands and 13 in the United Kingdom. The mean age was 61 years old and the majority were female (66%). Just over half of the family caregivers (54%) also took part in the second interview, due to loss to follow-up (Table 4).
Integrated palliative care initiatives recruited.
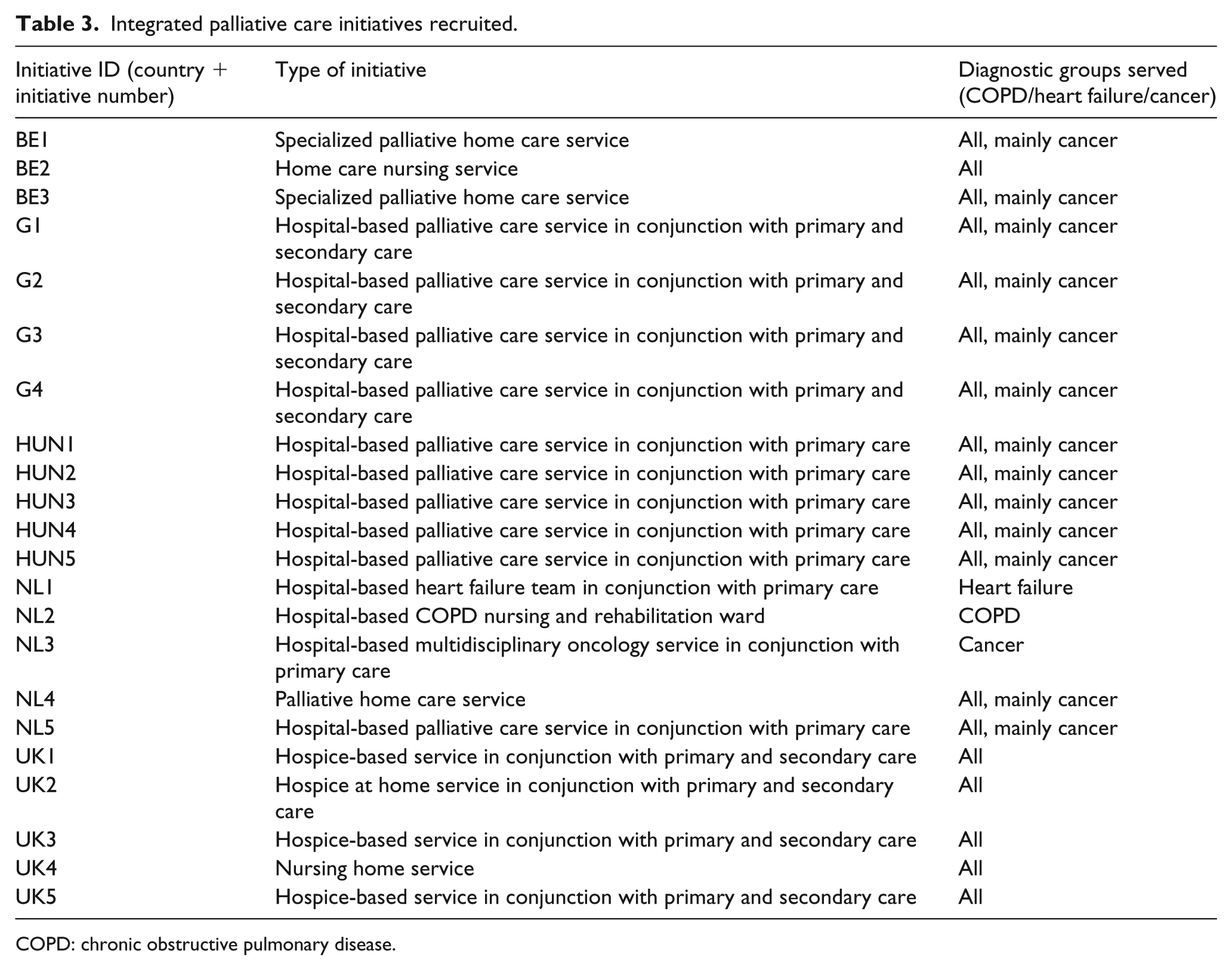
COPD: chronic obstructive pulmonary disease.
Respondent characteristics by country.
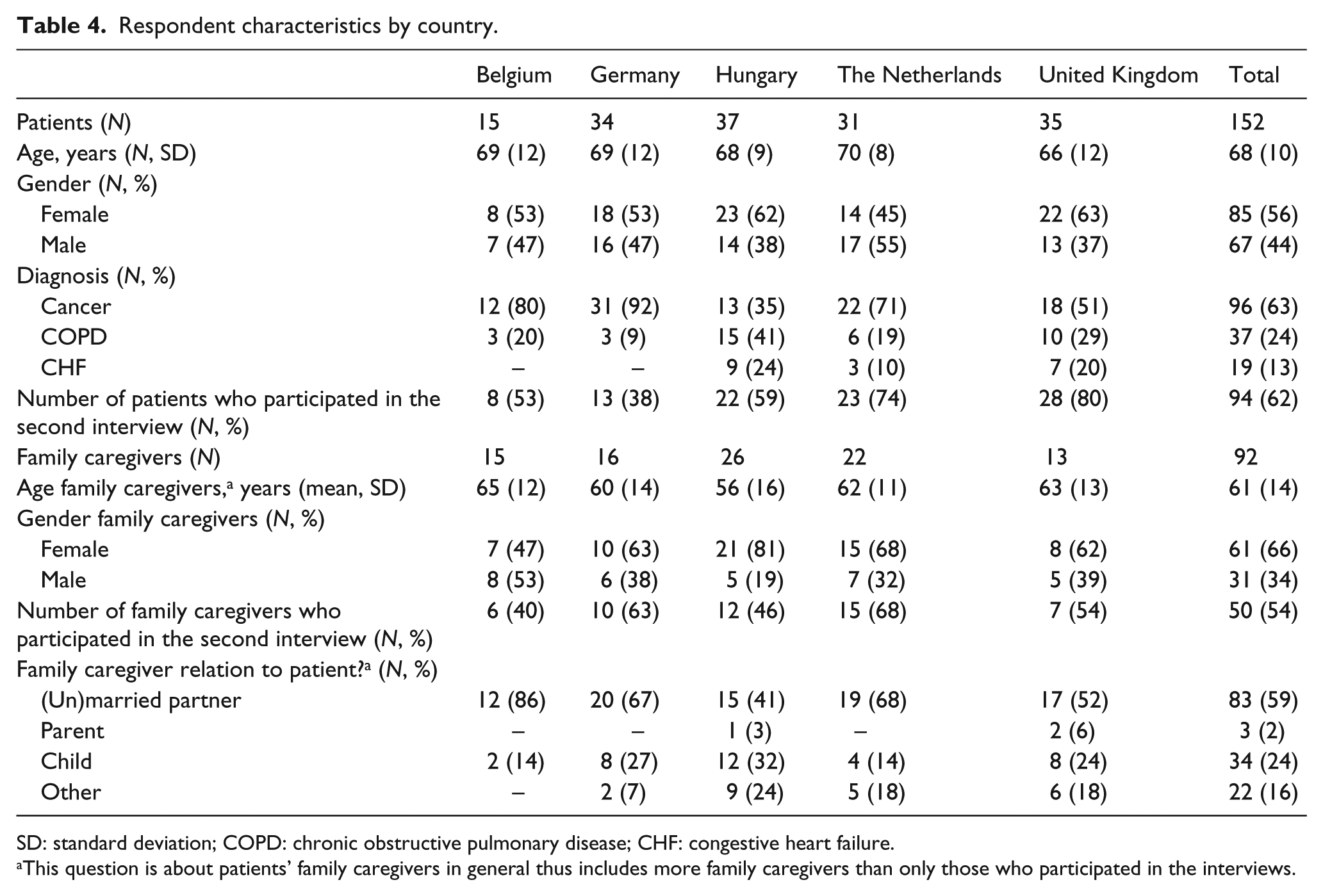
SD: standard deviation; COPD: chronic obstructive pulmonary disease; CHF: congestive heart failure.
This question is about patients’ family caregivers in general thus includes more family caregivers than only those who participated in the interviews.
Relational continuity
Relational continuity appeared prominent in all countries. Both positive and negative experiences related to having or not having close relationships with a small number of health care professionals (e.g. hospital specialists, general practitioners (GPs), nurses, physiotherapists or hospice care professionals) and seeing them on a regular basis. These health care professionals paid attention to the person behind the illness and took time to talk about respondents’ personal lives, rather than only about the illness. It provided trust when respondents were known to health care professionals, so that these could take their needs and wishes into account to tailor care:
Well, he promised me to die in a decent way. What she meant by that, I am not sure […]. But she has promised: ‘You can count on me’. (B1P3, cancer)
Also, these health care professionals were always available and responded adequately in case of needs, as perceived by respondents:
I call my carers [hospice staff] if I need and I get immediate help. They are available all day and night, my GP also gave me his private phone number. (HU2P2, COPD)
Furthermore, continuing relationships with certain health care professionals enabled monitoring of the patient’s illness progress: ‘They actually know each other very well. In the way he is sitting [the heart failure nurse] can see how he is’ (NL1C1, heart failure). For a number of respondents in Belgium and the Netherlands, this monitoring function was the reason that they wanted to continue their relationship with their oncologist.
However, lack of relational continuity was often experienced as well and meant that respondents needed to spend a lot of energy in building new relationships, reiterating their histories and that they did not know what they could expect from health care professionals:
[…] it’s hard because, you know, really you should be building a rapport up with the GP [so that] when you are ill he comes out, he knows you, you’re not convincing him. But the one that I have been going to for years is leaving now as well. (UK2P4, cancer)
More specifically, experiences of relational continuity with GPs varied widely across countries. Many respondents highly valued longstanding relationships with their GPs and GPs’ comprehensive knowledge of them: ‘And then I talked to him [GP], because he knows me for a long time’ (G2P12, COPD). Also, GPs often had an important role in coordinating care, prescribing medication and making referrals. However, at the same time many respondents in all countries, but predominantly in Hungary, Germany and the United Kingdom, experienced a lack of involvement of their GPs:
Our GP didn’t come at all. He [the patient] is at home since September, but the doctor didn’t visit him … When we need something, for example tube or catheter, I’ve to spend hours making phone calls. (HU4C1, cancer)
Many GPs seemed to take the backseat when patients were (still) treated by hospital specialists, or specialized palliative care teams. Consequences were that respondents did not receive the support they needed and/or expected from their GPs.
Informational continuity
Respondents found it very important that health care professionals were well informed as they felt it prevented them from repeating their histories and provided trust that health care professionals had the right information to make correct treatment decisions:
If you all know the same things then you’ve a better quality of treatment and more chance of success. (UK3P1, COPD)
However, in all countries informational continuity seemed to be a weak point in care provision. This was revealed in situations in which many different health care professionals were involved, within the hospital, between hospital specialists and GPs, between hospitals and during acute (out-of-hour) situations. At these moments, it became apparent that health care professionals were often badly informed about the patient’s history, did not have access to other health care professionals’ patient records or did not have regular contact:
My impression is that they [hospital physicians] do not always read the record accurately, and that they do not know the whole thing about me. (G2P4, cancer) The GP, since half a year I think, he receives a little letter about what was done. […] I had been with the oncologist for two years. […] I was being treated and I was coming back twice a month to make a photo or CT-scan. The GP didn’t know anything … So I’m visiting the GP one time for another little thing and: ‘Cancer?’ he says. I say: ‘Yes, cancer’. (NL5P2, cancer)
Negative consequences resulting from this according to respondents included the need to reiterate medical histories several times, receiving contradictory information, worries about the quality of care and becoming agent of information transfer between health care professionals, while many respondents did not want to have this responsibility:
P: […] the GP prescribed antibiotics. Then we went to the hospital day clinic […]: ‘oh no, she cannot take these antibiotics with her liver’. And then we had to contact the GP and tell the GP what the hospital had said … those things! (B1P1, cancer) […] So you need to take control while you actually want to give it away. (NL3C2, cancer)
In contrary to the above-mentioned, in all countries respondents provided examples of health care professionals who worked closely together in teams or networks and were often well informed about respondents’ medical histories and personal circumstances. Respondents appreciated that they did not have to ensure information transfer between health care professionals anymore. Interestingly, we observed that these health care professionals were often involved in collaborative integrated palliative care initiatives:
There is a close relationship between them [hospice team], daily contact … All professionals share the information with others. (HU4P1, cancer) Yes, they are in constant touch. That’s why I don’t have to explain the medication to the qualified palliative physicians … (G3C2, cancer) I think [the network works together] now a lot more because everything’s on the computer […] when I go to my GP, you don’t have to have the letter with you that’s come from the hospital … (UK5P1, cancer)
Management continuity
Respondents wanted to be seen as a person with multidimensional needs rather than a medical subject. This required that health care professionals viewed respondents with a holistic lens and provided multidisciplinary care in order to support their multidimensional needs:
I understand that doctors at the Pulmonology [department] treat my lungs, but I also have constriction of the arteries in my legs … (HU4P9, heart failure) I: What do you think about all these different persons who are dealing with this [illness]? FC: Well, I think that is […] very good. It cannot be done by one single person. That seems nearly impossible. […] I do assume that there are all kind of connections [between HCPs] going up and down. I do perceive this as well. (NL5C6, cancer)
The importance of this became clear with several examples provided by respondents in which multidisciplinary care was absent or obstructed. Many respondents experienced that health care professionals worked in a fragmented fashion and only dealt with their own medical specialty. We found this fragmented care mainly among individual hospital specialists and between hospital specialists and GPs. Consequences for respondents were that problems were inadequately addressed, remained unaddressed or were discovered too late:
[GP and oncologist] … sometimes, they think only inside their box. […] The GP has been looking on his computer for 20 minutes which antibiotics he could give […] He should be able to just grab his phone and say: ‘listen I have that patient, that medical file number, she has these symptoms, what can I give?’… (B1C1, cancer) [About missed diagnosis of broken leg]: … he [urologist] kept persisting that he wasn’t able to see anything on the screen. […]. But, […] if he is not able to see it, he could have passed that on to another physician like: ‘this madam complained a little about her leg’. Then he could have send her [patient] to Orthopaedics. Then we would have been much further and earlier than [now] that we had to stay with him having done nothing about it. (NL5C9, cancer)
In contrast, several respondents clearly perceived the differences when multidisciplinary care was provided:
… the advantage of [care networks] being connected is that you get the optimum care […] Now that I’ve had lots of referrals and I’ve been able to access some exercise, a dietician, hospice workers to help with my will or thinking about a funeral, psychology to help me and to give me advice … (UK5P8, heart failure)
Respondents often did not know how health care professionals exactly worked together and many were not particularly interested in this, as long as they received multidisciplinary care. However, in all countries some respondents appreciated that health care professionals formed small collaborative groups in which they consulted each other and provided referrals to other health care professionals. For example, a number of respondents in Germany, the Netherlands, Belgium and the United Kingdom knew that health care professionals came together in meetings, resulting in impressions that care was connected and coherent. These collaborative groups often seemed relevant for health care professionals involved in integrated palliative care initiatives:
I know that they have like a big … a big meeting about my Mam’s care […] I’m sure it’s like [Breast Care Nurse Specialist], the Oncologist, and it might even have been [the Bone Specialist] as well. (UK2C3, cancer) … with those [palliative care and radiology] I have the feeling that it all fits together like cogwheels. (NL5P2, cancer)
Discussion
This article examined how relational, informational and management continuity of care are experienced by patients with advanced cancer, COPD or heart failure and family caregivers receiving care from several integrated palliative care initiatives in five European countries. Concerning relational continuity, respondents found it very important to have trusted relationships with a small number of key health care professionals in order to receive tailored care and easily access help when needed. GPs had an essential role for many respondents across the five countries, because of their established relationships with patients. However, as multiple health care professionals were involved in order to meet respondents’ needs, relational continuity was often at stake. This was especially the case with GPs who appeared to take the backseat when hospital/palliative care specialists were involved. As a result, patients and family caregivers felt abandoned by their GPs and sometimes lacked the support they needed.
Thus, although adequately supporting multidimensional needs of patients with advanced illnesses and family caregivers requires multidisciplinary care, 40 it can jeopardize relational continuity. Such impact of structure and organization of services on the involvement of valued key health care professionals and experiences of patients has been described elsewhere. 27 These findings highlight the need of patients and family caregivers to maintain relational continuity, especially when multiple health care professionals are involved. Our results suggest that in order to maintain relational continuity, multidisciplinary collaboration could be enacted by health care professionals behind the scenes, but at service level respondents may only need a small number of key health care professionals who are readily available without exactly knowing how health care professionals collaborate. Additionally, GPs need to be more involved in multidisciplinary care provision for patients with advanced illnesses. Both hospital/palliative care specialists and GPs should take that responsibility.
Furthermore, our findings demonstrated that although patients and family caregivers needed and expected to receive multidisciplinary collaboration, informational and management continuity were still 11 a weak link in care provision. Many health care professionals seemed to lack a collaborative attitude in which they focus on the needs of patients and family caregivers and work closely together with other health care professionals by consultation and information transfer. As a result, many patients and family caregivers did not find adequate support for their needs and were burdened with information transfer between health care professionals. This is in line with the study of Seamark et al. 10 who found that information transfer between primary and secondary care often does not take place, according to experiences of bereaved caregivers in the United Kingdom. Moreover, Richardson et al. 11 showed that even if consultation and referral does take place between multidisciplinary teams, it is not clear who is responsible for treatment; this could still disrupt and delay care.
In contrast, similarly to findings from previous studies,24,34 we found that where collaborative initiatives between health care professionals existed, multidisciplinary care and information transfer did take place and patients and family caregivers felt that care provision was connected and coherent. Respondents in our study often referred to health care professionals involved in integrated palliative care initiatives. Thus, integrated palliative care initiatives that particularly focus on the needs of patients and family caregivers and use a person-centred collective team approach can have an important role in improving informational and management continuity. However, our study additionally suggests that as informational and management continuity was deficient despite the existence of collaborative integrated palliative care initiatives, fuller integration of these initiatives with other health care professionals is necessary to optimize continuity of care.
Strengths and limitations
The international context of the study enabled collection of rich data. However, data collection and analysis were done by different researchers in each country with a potential risk of methodological inconsistencies. We have limited these as much as possible using uniform interview protocols and training on data collection and analysis, regular support via Skype and face-to-face meetings and electronic correspondence to reflect on findings and prevent inconsistencies. Furthermore, in order to limit the likelihood of interpretation bias for the cross-country comparison, the data were peer reviewed with the researchers in each country in order to ensure correct interpretations. We aimed for theoretical sampling with the aim of attaining a balanced sample of patients with cancer, COPD or heart failure in all five countries and to compare experiences for patients with different diseases. However, in practice it appeared challenging to recruit the intended sample, especially for patients with COPD and congestive heart failure (CHF) as these are in the minority within integrated palliative care initiatives.
Some aspects seemed to be more an issue in some countries than in others, such as the role of the GP. However, a nuanced interpretation of these international data is difficult to achieve and requires understanding of the particular country context, including health care system and funding mechanisms. Notwithstanding, we found many common aspects that contributed to continuity of care suggesting that health care professionals and policy makers across countries can learn from each other in finding successful solutions for improving continuity of care experiences.
Conclusion
This international qualitative study showed that patients and family caregivers are most likely to experience continuity of care by having a small number of health care professionals who are available, who provide multidisciplinary care and who regularly transfer information to all health care professionals involved. Collaborative integrated palliative care initiatives could optimize continuity of care experiences and thus improve quality of palliative care in Europe. However, further integration of these initiatives with other health care professionals involved in the care networks of patients with advanced diseases and their family caregivers is needed. Researchers, clinicians and policy makers could use these insights in order to enhance integrated palliative care and improve experiences of patients with life-threatening diseases and family caregivers.
Supplemental Material
sj-docx-1-pmj-10.1177_0269216317697898 – Supplemental material for How continuity of care is experienced within the context of integrated palliative care: A qualitative study with patients and family caregivers in five European countries
Supplemental material, sj-docx-1-pmj-10.1177_0269216317697898 for How continuity of care is experienced within the context of integrated palliative care: A qualitative study with patients and family caregivers in five European countries by Marlieke den Herder-van der Eerden, Jeroen Hasselaar, Sheila Payne, Sandra Varey, Sven Schwabe, Lukas Radbruch, Karen Van Beek, Johan Menten, Csilla Busa, Agnes Csikos, Kris Vissers and Marieke Groot in Palliative Medicine
Footnotes
Acknowledgements
The authors would like to thank all the participants for their valuable contributions to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The research leading to these results has received funding from the European Union’s Seventh Framework Programme (FP7/2007–2013) under grant agreement no. 305555.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.