
Abstract
Background:
In cost-effectiveness analyses in healthcare, Quality-Adjusted Life Years are often used as outcome measure of effectiveness. However, there is an ongoing debate concerning the appropriateness of its use for decision-making in palliative care.
Aim:
To systematically map pros and cons of using the Quality-Adjusted Life Year to inform decisions on resource allocation among palliative care interventions, as brought forward in the debate, and to discuss the Quality-Adjusted Life Year’s value for palliative care.
Design:
The integrative review method of Whittemore and Knafl was followed. Theoretical arguments and empirical findings were mapped.
Data sources:
A literature search was conducted in PubMed, EMBASE, and CINAHL, in which MeSH (Medical Subject Headings) terms were Palliative Care, Cost-Benefit Analysis, Quality of Life, and Quality-Adjusted Life Years.
Findings:
Three themes regarding the pros and cons were identified: (1) restrictions in life years gained, (2) conceptualization of quality of life and its measurement, including suggestions to adapt this, and (3) valuation and additivity of time, referring to changing valuation of time. The debate is recognized in empirical studies, but alternatives not yet applied.
Conclusion:
The Quality-Adjusted Life Year might be more valuable for palliative care if specific issues are taken into account. Despite restrictions in life years gained, Quality-Adjusted Life Years can be achieved in palliative care. However, in measuring quality of life, we recommend to—in addition to the EQ-5D— make use of quality of life or capability instruments specifically for palliative care. Also, we suggest exploring the possibility of integrating valuation of time in a non-linear way in the Quality-Adjusted Life Year.
Medical (technological) progress and resulting competing alternatives increasingly raise the question “must everything that can be done, be done?” The Quality-Adjusted Life Year (QALY) is widely used as outcome measure for cost-effectiveness analyses in healthcare. However, there is an ongoing debate concerning the appropriateness of its use to inform decisions on resource allocation among palliative care interventions.
This paper offers the first systematic overview of pros and cons of using QALYs to inform decisions on resource allocation among palliative care interventions. It provides a critical appraisal of the arguments and discusses the QALYs’ value for palliative care. Furthermore, it explores whether difficulties are experienced in research practice and how they are dealt with, for example, are alternative approaches or outcome measures used?
Our review concludes that, despite criticisms, the QALY might be of value in informing decisions on resource allocation among palliative care interventions if specific issues are taken into account. Since standard quality-of-life measurement instruments (such as the EQ-5D) lack dimensions that are essential to palliative care, we recommend to add quality-of-life or capability instruments for economic evaluations in palliative care. Also, we suggest exploring the possibility of integrating valuation of time in a non-linear way in the QALY framework. However, to appropriately allocate scarce resources across healthcare, a common metric is needed. Therefore, the issues suggested should not remain restricted to palliative care, but be considered in the QALY conceptualization throughout healthcare.
Background
Patients are entitled to receive timely, acceptable, and affordable care of appropriate quality. 1 Due to new (expensive) drugs and treatments, and the fact that people live longer, the duration of intensive and costly care has increased. This puts pressure on the collective affordability of our healthcare. The question “must everything that can be done, be done?” is being asked more frequently, particularly in end-of-life care (EoLC). Palliative care also competes for limited healthcare resources. Since the number of patients in advanced stages of incurable conditions is increasing,2,3 expenditures in this field are likely to increasingly represent a bigger share of total spending.
Because of this, economic evaluations used when allocating resources are becoming increasingly important. 4 Insight into the effectiveness, its costs, and their incremental ratio (incremental cost-effectiveness) is important when allocating resources. It is frequently argued that the evaluation of palliative care interventions should also include cost-effectiveness.5–8 The Quality-Adjusted Life Year (QALY) is the predominant outcome measure for cost-effectiveness analyses (CEAs) in healthcare, and its use is recommended by both the National Institute for Health and Clinical Excellence (NICE) and the Dutch guideline for economic evaluation in healthcare.9–11 However, in the (scientific) palliative care community, a debate concerning the appropriateness of the QALY’s use as part of the efficiency decision rule in palliative care is taking place.6,7,12–14
The QALY takes into account two factors: the quality (of life; “Q”) and the quantity (life years gained; “LY”) generated by healthcare interventions. In the QALY, the length of time spent in a certain health state is weighed by the utility score given to that health state. 15 For instance, 1 year of perfect health is worth one QALY, a year of less than perfect health is worth less than one QALY, and death is considered to be equivalent to zero QALYs. Some health states may be considered worse than death and have negative scores. 15 By integrating Q and LY, the QALY provides a common metric to measure the added values from a variety of interventions, making it useful for budget allocation. In principle, deciding to allocate resources toward a specific intervention depends on the value for money question in terms of societal willingness to pay for a QALY gained.
This general application of the QALY, however, also contains a major objection. 16 Some think that the nature of palliative care makes it more difficult to provide evidence on efficiency, which puts palliative care in a disadvantaged position when competing for resources with other healthcare services that have better evidence.17–19 It is argued that other approaches, such as the capability approach, in which capabilities are considered rather than functioning, 14 might provide a richer evaluative space. The aim of this review is to systematically map pros and cons of using the QALY to inform decisions on resource allocation among palliative care interventions as brought forward in the debate and to discuss the QALY’s value for palliative care.
Methods
Rationale
In order to unfold the coherent body of knowledge, insights generated from separate studies were integrated using Whittemore and Knafl’s 20 methodology for integrative reviews. Both non-empirical (theoretical) and empirical (CEAs) literature was searched. Theoretical literature was analyzed from bottom-up to find and compare arguments regarding the appropriateness of using the QALY to inform decisions on resource allocation among palliative care interventions. All the pro- and con arguments were presented in their original form regardless of their strength. In the discussion, the various arguments were critically appraised and the value of QALYs for palliative care was discussed. Analysis of the CEAs focused on identifying whether the perceived difficulties are described in research practice.
Literature search and data extraction
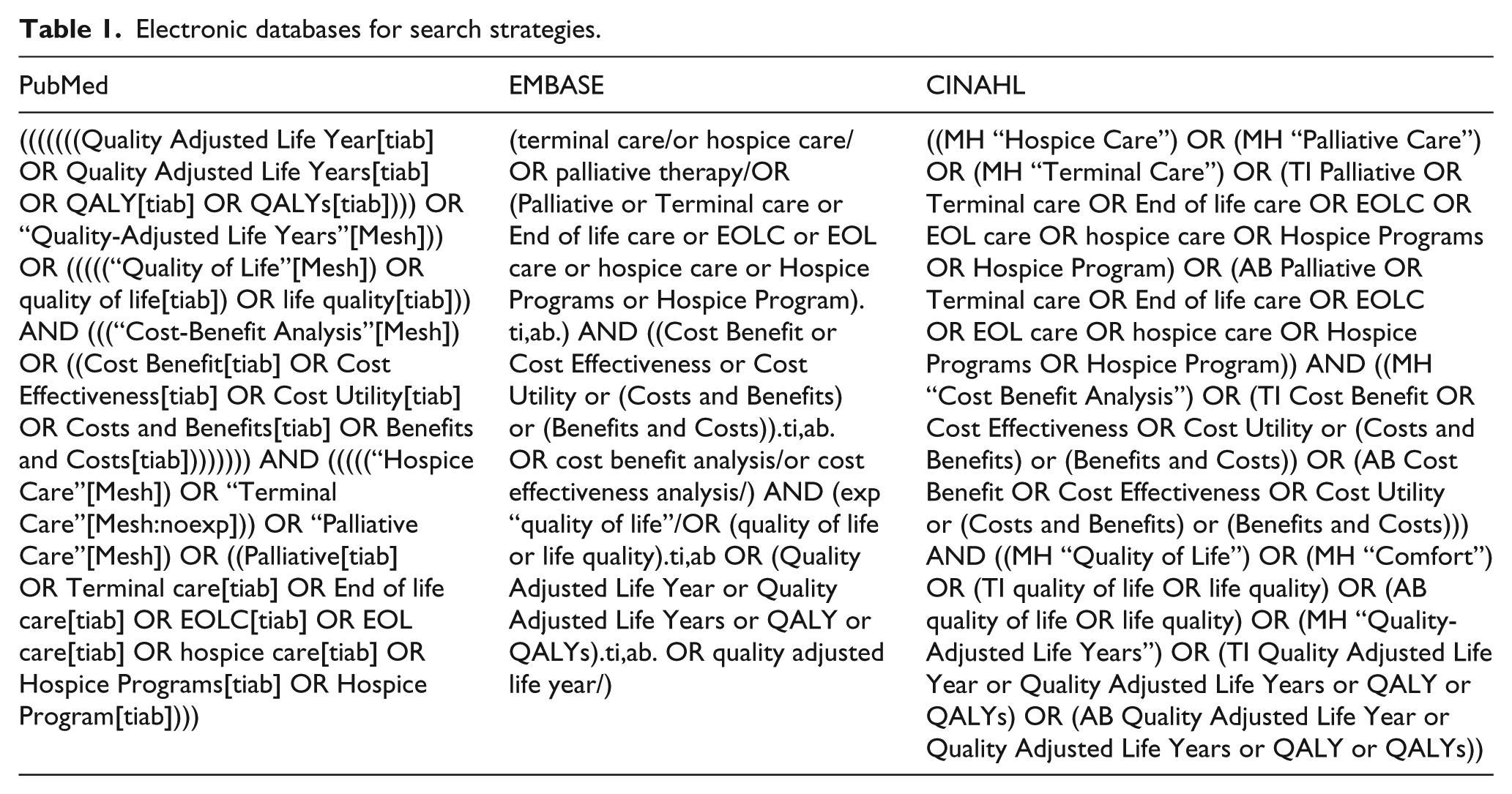
A literature search was conducted in the electronic databases PubMed, EMBASE, and CINAHL (Table 1). MeSH (Medical Subject Headings) terms in the search strategy were Palliative Care, Cost-Benefit Analysis, Quality of Life, and Quality-Adjusted Life Years. The search was limited to English-language articles published between 2000 and May 2015. In March 2016, a search update was done. Reference lists were scanned iteratively for supplementary publications.
Electronic databases for search strategies.
In assessing the records identified by the database search, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart was used (Figure 1). 21 After identification of the records and the removal of duplications, titles and abstracts were screened for their relevance. If the article did not concern our research question, for example, when the title or abstract not indicated the study concerned cost-effectiveness/utility analysis within the palliative care field, it was excluded. Then, full-text articles were read to evaluate their eligibility. Inclusion and exclusion (Tables 2 and 3) in both the screening and the eligibility rounds were independently done by two researchers (A.B.W. and S.K.). Since the emphasis was on finding various pros and cons of using the QALY in palliative care, an inclusive sampling approach was used. That is, all titles that seemed to be of interest were included. Primary sources were not assessed on their individual quality.
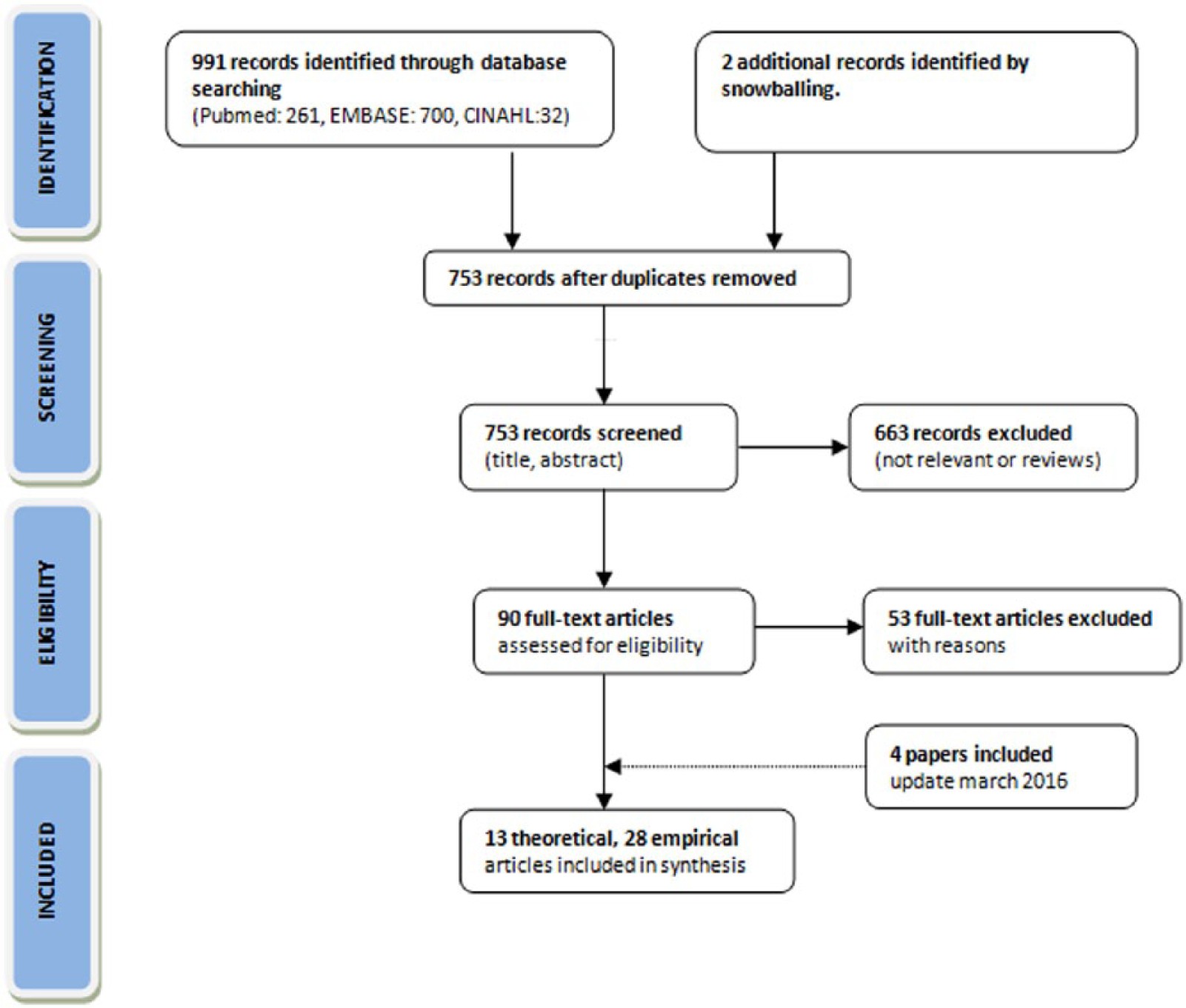
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. 22
Inclusion and exclusion criteria of theoretical papers.
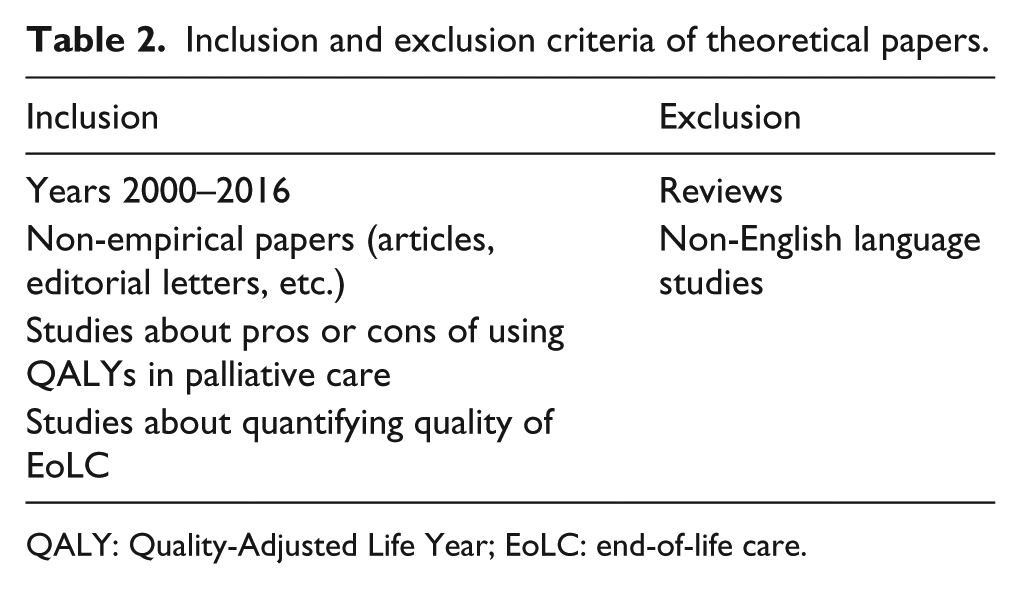
QALY: Quality-Adjusted Life Year; EoLC: end-of-life care.
Inclusion and exclusion criteria of empirical (CE) papers.
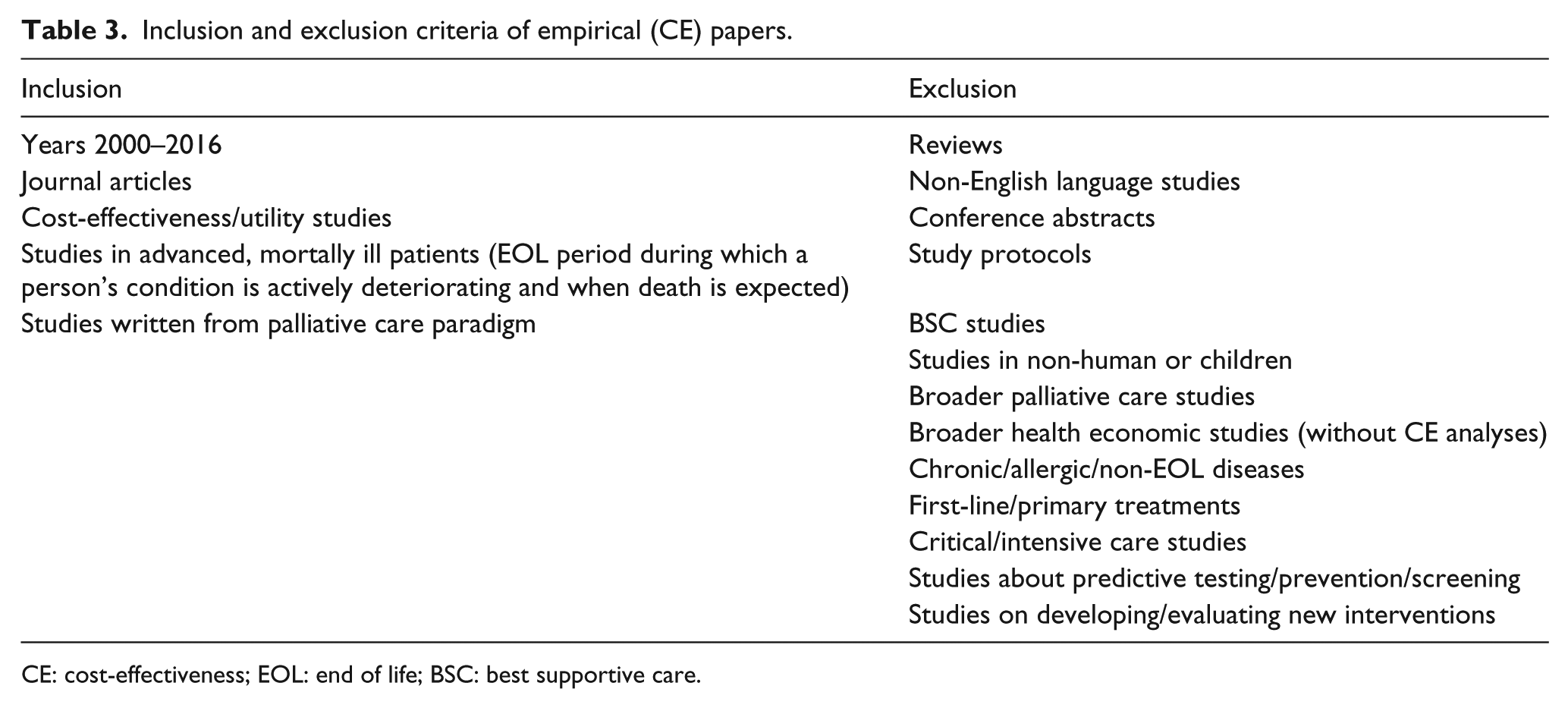
CE: cost-effectiveness; EOL: end of life; BSC: best supportive care.
Data analysis
In order to provide a comprehensive understanding of pros and cons of using QALYs to inform decisions on resource allocation among palliative care interventions, the storyline of the coherent body of knowledge was unfolded. Heterogeneous literature (Tables 4 and 5 in Appendix 1) was explored and analyzed. The research strategy for integrative reviews was used for data analysis. 20 Two subgroups consisting of theoretical and empirical literature were analyzed separately (see the following subsections). Subsequently, the theoretical and empirical subgroups were integrated. 23
Theoretical literature
Pros and cons of using the QALY in palliative care, as well as alternative outcome measures and approaches, were inferred from the theoretical literature. All arguments from primary sources were coded, ordered, and clustered to identify patterns that could be translated into themes (Table 6 in Appendix 1). To meaningfully analyze the arguments, it was done in chronological order.
Empirical literature
Empirical CEAs were studied to find out whether perceived difficulties are experienced in research practice in the theoretical literature and how they are being dealt with, for example, are alternative approaches or outcome measures used? A data extraction form was used to systematize all findings. The empirical studies were ordered alphabetically, by author name, and on methodological characteristics (Table 5 in Appendix 1).
Findings
Of the 993 publications initially identified through database searching and snowballing, 753 studies of potential interest were left after removal of duplications (Figure 1). A total of 13 theoretical and 30 empirical CEAs were included. The theoretical literature encompassed clinical, economic, policy/management, and philosophical studies. Tables 4 and 5 in Appendix 1 show the characteristics of the included studies.
Interpretation and integration
After ordering all arguments regarding the use of the QALY to inform decisions on resource allocation among palliative care interventions—as they were originally brought forward in the literature—three themes were identified from bottom-up (Table 6 in Appendix 1). These themes concern groups of arguments about the “life years gained,” “conceptualization of quality of life (QoL) and its measurement,” and the “valuation and additivity of time” elements of the QALY. Some of these arguments could also be found in the empirical literature (Table 7 in Appendix 1), and some were supported by alternative outcome measures or approaches such as the “PalY” and the “Peak End Rule.” In the discussion, we critically appraise the main arguments and the value of QALYs for palliative care.
Theme 1. Life years gained
Low life expectancy is considered to be a problem (con)
Some authors view the LY component of the QALY as problematic. It is argued that the main objective of palliative care is to improve QoL and enable people to opt for a dignified death 14 and not (necessarily) prolonging survival.5,14,18 Egan, 5 for example, argues that the QALY has the implicit and flawed assumption that interventions should prolong survival to be valuable. He states that since patients eligible for palliative care have a relatively low life expectancy, any life-saving therapy will result in potentially higher QALY gains. 5 A consequence of this assumption, it is posed, is that even when costs are quite modest, palliative care interventions cannot prove themselves to be cost-effective, as there is no enough time for them to generate QALYs.5,12 This difficulty is also encountered in empirical studies.24,25,26 For instance, Stevenson et al. 24 state that “any survival advantage has a marked effect on the cost-effectiveness, which reflects the frequent issue that it can be more cost-effective to let patients die rather than to use relatively costly treatments.”
Gains in QALYs are possible even if life expectancy is low (pro)
Hughes 6 contends against this argument by citing Keynes’ “in the long run we are all dead.” This fact, he argues, does not make QALY analysis inapplicable across the board. After all, our QoL matters while we are alive, and this is what the QALY seeks to capture, too. 6 This view is supported by Round, 7 who by means of an illustration shows that increases in QALYs are possible even if life cannot be lengthened. This is also backed by empirical studies that found that their results were most sensitive to changes in utilities, 27 and that palliative therapies began to gain very high QALY values with only modest decreases in QoL. 28 This implies that the Q weight significantly influences the QALY, and that survival advantage even seems to be undermined by declines in QoL. Moreover, Hughes 6 poses the objective of improving QoL (or limit its potential loss, red.) rather than increasing life expectancy is true for other non-life prolonging interventions which can be measured in QALYs, such as hip operations. In other words, gains in QALYs are possible even if one of its components does not change significantly, since improvements can be made in the other component. 7
Theme 2. Conceptualization of QoL and its measurement
Health-related domains are less relevant in palliative care (con)
Other arguments concern the Q weight of the QALY. One of the main arguments is about its conceptualization and measurement. The instrument predominantly used to measure the Q weight is the EuroQol instrument (EQ-5D). However, the health-related QoL (HR-QoL) dimensions—pain/discomfort, anxiety/depression, mobility, self care, and usual activities—that are covered by this instrument are often seen as less relevant in the context of palliative care, in which values such as patient dignity, spiritual and psychosocial well-being, and bereavement support are central. These rather broad, multidimensional, complex, and holistic intentions of palliative care are said to be lacking in HR-QoL measurement instruments such as the EQ-5D.12,29 In other words, the authors argue that the EQ-5D is mainly concerned with health and the recovery of health, and not with the quality of end of life (EoL) or dying.
Do not dismiss the framework: develop valid measurement instruments (pro)
Yang and Mahon, 30 however, argue that palliative care and the QALY are compatible. They state that “like QALY and cost-utility calculations, palliative care involves a benefit-burden analysis for optimal treatment recommendations.” However, they argue that palliative care must be optimally integrated in QALY calculations. 8 Other authors are also convinced that, despite current difficulties, the champagne should not be thrown out with the cork. Improper measurement (as of yet) of the Q weight of the QALY should not result in a relinquishment of the whole outcome measure.6,7,31 Hughes 6 argues, what should be done is develop the best ways for estimating QoL. According to Chochinov, 29 in palliative care, this means measurement should embrace a perspective as broad as the notion of QoL itself. With further refinements of analytical instruments, the conviction is that palliative care can be optimally integrated in the QALY calculation. 30 Coast, 14 with the capability approach, argues for a richer evaluative space when measuring QoL.
… this flexibility is offered in the extra-welfarist framework (pro)
Round 7 agrees that instruments could be developed that take account of the domains of relevance to a certain population. This flexibility of preference-based measurement is said to be offered within the extra-welfarism framework. In this (conceptual) approach, non-health domains next to or instead of health-related domains, or capabilities instead of functioning, 14 can or should preferably be considered when estimating QALYs. It is argued that accepting some degree of heterogeneity in QoL measurement may be less detrimental than squeezing all evaluation activity into standard instruments. 18 This flexibility, however, is said to be rarely applied in research practice, 7 and “the fact that researchers have not taken advantage of this flexibility is not a criticism of the framework itself.” 7
An extra-welfarist capability approach (con)
Coast and colleagues,14,32 inspired by the work of Amartya Sen,33–35 make the case for the capability approach. In this approach, interventions are not based solely on functioning but are assessed based on their impact on what a person is able to do or be—in terms of capabilities that allow a person to have a good EoL. 14 Although there is disagreement on the scope to which these capabilities can differ,36,37 Coast 14 advocates for different sets of capabilities in different contexts.
The Palliative Care Yardstick as alternative approach (con)
An alternative approach also using this flexibility is suggested by Normands’ 12 Palliative Care Yardstick (PalY). By adding items to the QALY, the PalY would incorporate dimensions of palliative care (i.e. caring externalities) that are not considered when calculating QALYs. 12 This approach, however, has not yet been studied in practice.
(Availability of) instruments not known (con)
In the empirical literature, mostly (standard) HR-QoL measurement instruments—such as the EQ-5D, EORTC QLQ-LC13/30, and SF-36—were used (Table 5 in Appendix 1). In one of these CEAs, it is noted that standard HR-QoL instruments were used that do not include QoL domains specifically relevant for the valuation of EoLC, due to the assumption that “unfortunately, no valuation instrument exists that incorporates such issues.” 38 In the empirical literature, some authors look for intermediate solutions for this problem by taking into account aspects of HR-QoL that have the largest impact on general QoL in palliative patients. Barton et al. 39 for example, use response to pain treatment in their utility calculations, since “chronic pain has an enormous effect on QoL of patients with bone metastases.” Pace et al. 40 measure rehospitalization, as this is correlated with a lack of symptom control, worsening patient QoL.
Linear continuum and the narrative approach (con)
Another main argument against the use of the QALY in palliative care is its assumption of a mathematical linear continuum between death (0) and excellent health (1).5,12 Authors specifically have a problem with the fixed valuing of zero for death, due to which the benefits of a good or desired death currently cannot be captured.12,41 Normand 12 argues that the non-linearity could be “accepted” by putting a value on components of a good death, and that this non-linear valuing would be separate from the days that led up to it (We will come back to the valuation question in theme 3.). The linear continuum assumption is challenged by the narrative approach. 6 This theory describes that the manner in which a life ends impacts the overall value of that life. In this approach, the benefit of good EoLC is independent of any particular time-slice and thus cannot be captured by the QALY. 6 Hughes 6 and Cowley 42 are in favor of this approach, as good terminal care adds greater meaning to the past life, and “the increase in rediscovered meaningful years can be measured backwards rather than forwards.” Cowley argues that this increase in rediscovered life years can even constitute new quality life years, since quality is retrospectively added to lived years.
Theme 3. Valuation and additivity of time
Valuation of time increases as time is running out (con)
As briefly mentioned above, the QALY assumes that preferences on time are stable. Therefore, in the QALY methodology, it is common practice to weight each year of added life equally. That is, time for any individual at any point in time is treated as being constant, making it additive. 18 By some, this feature of additivity is seen as problematic,5,12 since valuation of time might not be fixed.12,29,43 It would increase as time itself runs out.29,41 Chochinov 29 describes it as follows: “Each moment becomes increasingly precious as death draws near, while for the rest of the world, the clock marks time at its usual pace, with its usual indifference.”
Adding the Valuation Index Palliative to the PalY (con)
Normands’ previously introduced PalY not only suggests adding items to the QALY, but also deals with the valuation problem. For example by allowing a value to be put on components of a “good death,” which is separate from the days that led up to it. Chochinov further explores the PalY suggestion by adding the Valuation Index Palliative (VIP). In the VIP, the supposed increasing value of time as death gets closer is taken into account by ascribing a higher value to time in proximity to death.
29
Although these concepts did not (yet) reach research practice, Furlan et al., in their empirical study, theorize about this idea:
… patients at the EoL tend to have low QALYs because of very poor health status […] This raises the question of whether economic evaluations […] ought to use some adjustment that would give additional weight to gains to health occurring at the EoL.
Billingham et al. 44 may have used the VIP. They state that their CEA takes no account of the diminishing marginal utility, but that “an extra 2 months of good QoL to a life-expectancy of 6 months is potentially more valuable than an extra 2 months to a much better average life-expectancy.”
And: the willingness to pay for it increases (con)
When following this line of reasoning, a QALY gained at the EoL would not be equivalent to a QALY gained earlier in life. 41 Moreover, a rising willingness to pay for time gained at the EoL is assumed. 29 This line of reasoning can also be found in empirical studies. Arguedas et al. 45 state that in their CEA, “a value closer to $100,000 per QALY [instead of the regularly cited threshold of $50,000 46 ] might more accurately reflect societal preferences.” Furlan et al. 47 argue that their results “indicate that increased expenditures are needed to impact patients’ QoL for such morbid clinical conditions.” According to Haycox, 41 society indeed appears to show a willingness to pay for palliative care that lies above the level that would be considered “rational.”
Or doesn’t it? (pro)
Hughes 6 though, objects to this reasoning since, according to him, it is not clear that palliative patients have greater needs than others. So, it cannot be the sole criterion for distribution of resources. He poses it should be combined with some measure of benefit. 6 Round 7 agrees that equity issues arise when resource allocation decisions are made based on situations that are no more unique to patients at the EoL than they are at any other life stages. Round 43 puts forward that, as patients themselves are willing to spend increased sums on their care at the EoL, it may not be that the value of time to the individual increases but that the value of alternative uses of the individual’s resources decreases.
The Peak End Rule as alternative approach (con)
When following the non-linear rationale, periods of time cannot be added up at different points in time. Not even after adjusting for quality, since the value behind different time-slices may differ.6,12 Normand 12 even states that when adding up benefits for (different) individuals, theorems in welfare economics are violated. This is why it is argued that Kahneman et al.’s 48 Peak End Rule theory is applicable. The idea that there are circumstances where people put more or less value on time is supported by this theory. It describes that the way people evaluate past experiences tends to be based on the most intense points (best or worst) and how they end. Authors using Kahnemans’ theory argue that people caught in the gravity of approaching death encounter a profound distortion of how time is experienced and valued. 29
But … in what direction does it change? (pro)
Others, however, argue that the assumption that time spent in the terminal phase of life is valued more highly is currently without empirical support. 7 It is stated that even if valuation of time changes throughout life, it is not clear in which direction. 43 Furthermore, the valuation of time objection is stated to ignore the option of weighing health gains differently for different populations. 7
Discussion
We integrated theoretical and empirical literature on arguments concerning the appropriateness of using QALYs to inform decisions on resource allocation among palliative care interventions. 20 A total of 13 theoretical and 30 empirical CEAs were included. The theoretical literature encompassed studies from various theoretical bases and perspectives (Table 4 in Appendix 1), which made the juxtaposition of all arguments challenging. Nonetheless, three themes regarding the pros and cons of using the QALY, as well as difficulties concerning its use in research practice (CEAs), were identified: (1) life years gained, (2) QoL measurement and conceptualization, and (3) valuation and additivity of time. Below, we iterate the main arguments theme by theme, critically appraise them, and discuss the QALY’s value for palliative care and potential implications for practice or policy.
Theme 1. Life years gained
In this theme, the main argument against the use of the QALY is that not enough can be gained in its LY component.5,18 This allegedly results in disadvantageous cost-effectiveness ratios in palliative care compared to other healthcare fields. 5 Others object that, since the Q weight significantly influences the QALY outcome,6,7 increases in QALYs are possible even if life is not lengthened. Indeed, QALY gains have been reported in empirical studies.27,28
Appraising the above argument, it is clear that—mathematically—improvements in QoL can and will generate QALYs. However, given the short survival, the scope for this (but; also for rises in costs) is clearly limited. Also, higher thresholds for diseases with a high disease burden can be used. Moreover, we want to emphasize that the discussion on the appropriateness of using the QALY in CEAs in palliative care takes place in the narrow context of economic evaluation, where new interventions are compared to a “best alternative,” mostly standard care. 49 This means that in research practice, comparators are faced with the same context and constraints. Research has even shown that early palliative care and symptom control not only improve QoL but also, without the use of aggressive medical care, translate into prolonged survival.50–52 So, when calculating QALYs in palliative care, there is a fair competition between competing interventions. Nevertheless, when using the QALY for the allocation of financial resources on a macro level, other very relevant questions—such as how much may a QALY cost? 53 —are in play that deserve thorough exploration.
Theme 2. QOL measurement and conceptualization
A major perceived objection regarding the use of the QALY in palliative care is that it takes into account health-related domains, which are considered less relevant than other dimensions of QoL. Therefore, it is argued that alternative QoL measurement instruments should be developed that embrace a perspective as broad as the notion of QoL itself 29 and that the flexibility as offered in the extra-welfarist framework even makes it possible to use other QoL concepts broader than HR-QoL—such as the capability approach.14,31,54 This flexibility, however, is seldom used according to some.7,18 Moreover, several authors mentioned that standard HR-QoL instruments were used because of the assumption that no valuation instrument exists that incorporates EoLC issues.
However, to appraise these arguments, there are several instruments taking into account EoLC values such as peace, emotions, and spiritual and psychosocial well-being (e.g. the ICECAP-SCM—measuring capabilities—the POS, and the FACIT-Pal).55,56 Probably, they are hardly used as they are not suggested in CEA guidelines; the EQ-5D is the norm.10,11 But in the QALY framework, deviation from this norm is legitimate with solid arguments. Therefore, we recommend researchers in palliative care to, in the first place in addition to the EQ-5D, use these alternative instruments.
Moreover, a strict weighing of HR-QoL leads to unfavorable QALY results for healthcare domains that do not primarily focus on improving HR-QoL (but, for example, on improving autonomy, social well-being, or capabilities). In these domains, standard HR measurement tools are biased estimators as benefits (other than the EQ-5D dimensions) are missed. Therefore, we suggest to move to a broader concept of QoL. The time for doing this is right, since the new concept of health—in which health no longer refers to a state of complete well-being (WHO definition 1948), but to the ability to adapt and self-manage—more or less closes the gap between HR-QoL and QoL. 57
Theme 3. Valuation and additivity of time
In the third theme, it is argued that time episodes throughout life may be valued differently, and that this should be taken into account when making budget allocation decisions. The Peak End Rule theory is invoked to back the argument of varying valuations of time. To deal with the increasing valuation of time as death gets closer, the PaLY and VIP are introduced as alternative approaches. Others pose that it is not clear in which direction time preferences act. 43
Appraising these arguments, we note that there is no scientific consensus on the idea of the increasing valuation, and thus additivity, of time. However, more voices are heard on the non-linearity and changing valuation of time in proximity to death,48,58 while in the normative framework of the QALY, valuation of time is considered linear. Other descriptive models on valuation of time—such as the Peak End Rule, 48 maximal endurable time, 59 and lexicographic preferences, for example, the primacy of the “Q” over the “LY” weight—may be alternatives. We suggest further exploring the possibility of integrating valuation of time might be in a non-linear way in the QALY framework, for example, by operationalizing the VIP. If it is not legitimate to add up quality-adjusted time periods, it might be worthwhile to consider “whole experiences” and determine how these are valued.48,60
Strengths and limitations
Our integrative review offers the first systematic overview of pros and cons for using the QALY to inform decisions on resource allocation among palliative care interventions, adding new insights to the broader topical issue of whether everything that can be done or must be done. In our review, however, we focused on “technical” efficiency, informing allocation decisions among palliative care interventions only. Although this information is of importance, it cannot be used to inform on resource allocation throughout healthcare. 61 Moreover, because of controversy about the definition of “palliative care” in the field, we might have missed studies of importance. Furthermore, since we choose to bundle arguments in pros and cons, and analyzed them from bottom-up, our presentation might not have captured every link, making the discussion seem more black-and-white than it actually is. For example, the link between themes 1 and 3 (if you agree that time may not be additive, then the problem of short time horizons is less of an issue) was not reflected in the bottom-up analysis. Finally, although important for the QALY discussion across the entire width, the debate around QALY issues on a macro level, preferences in relation to health, and who should value these preferences was put aside.53,62,63
Conclusion
Three themes regarding the appropriateness of using QALYs to inform decisions on resource allocation among palliative care interventions were identified. The debate as identified in theoretical literature is recognized in the empirical literature. However, alternative outcome measures are not used. Despite criticism, concerning theme 1, the limited gain in LY in palliative care, QALYs can be gained, despite the fact that palliative care itself not primarily aims at this weight. Moreover, in the (narrow) context of economic evaluation, new interventions face the same context and constraints as their competitors, making the limited-scope issue less of an issue. In theme 2, it was argued that standard measurement of the Q weight of the QALY—for example, based on the EQ-5D or measuring functioning (instead of capabilities) at all—does not fit the palliative care context. We recommend making use of the possibility to use additional QoL or capabilities measurement instruments that incorporate important values for palliative care patients. As for theme 3, we suggest exploring whether valuation of time might be integrated into the QALY framework in a non-linear way. In short, the QALY might be more valuable when informing decisions on resource allocation among palliative care interventions, when specific issues related to the above-mentioned themes are taken into account.
Footnotes
Appendix 1
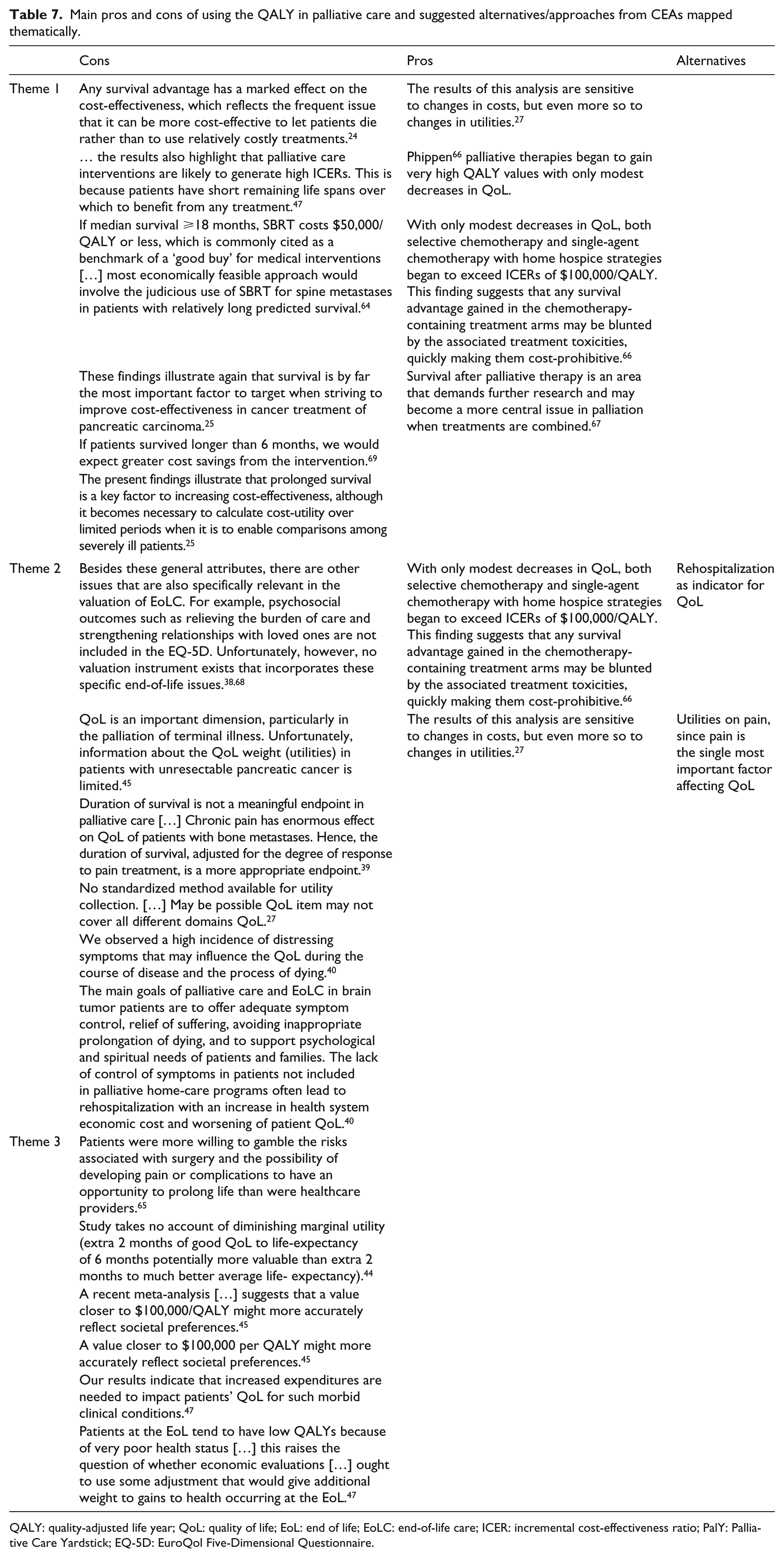
Main pros and cons of using the QALY in palliative care and suggested alternatives/approaches from CEAs mapped thematically.
| Cons | Pros | Alternatives | |
|---|---|---|---|
| Theme 1 | Any survival advantage has a marked effect on the cost-effectiveness, which reflects the frequent issue that it can be more cost-effective to let patients die rather than to use relatively costly treatments. 24 | The results of this analysis are sensitive to changes in costs, but even more so to changes in utilities. 27 | |
| … the results also highlight that palliative care interventions are likely to generate high ICERs. This is because patients have short remaining life spans over which to benefit from any treatment. 47 | Phippen 66 palliative therapies began to gain very high QALY values with only modest decreases in QoL. | ||
| If median survival ⩾18 months, SBRT costs $50,000/QALY or less, which is commonly cited as a benchmark of a ‘good buy’ for medical interventions […] most economically feasible approach would involve the judicious use of SBRT for spine metastases in patients with relatively long predicted survival. 64 | With only modest decreases in QoL, both selective chemotherapy and single-agent chemotherapy with home hospice strategies began to exceed ICERs of $100,000/QALY. This finding suggests that any survival advantage gained in the chemotherapy-containing treatment arms may be blunted by the associated treatment toxicities, quickly making them cost-prohibitive. 66 | ||
| These findings illustrate again that survival is by far the most important factor to target when striving to improve cost-effectiveness in cancer treatment of pancreatic carcinoma. 25 | Survival after palliative therapy is an area that demands further research and may become a more central issue in palliation when treatments are combined. 67 | ||
| If patients survived longer than 6 months, we would expect greater cost savings from the intervention. 69 | |||
| The present findings illustrate that prolonged survival is a key factor to increasing cost-effectiveness, although it becomes necessary to calculate cost-utility over limited periods when it is to enable comparisons among severely ill patients. 25 | |||
| Theme 2 | Besides these general attributes, there are other issues that are also specifically relevant in the valuation of EoLC. For example, psychosocial outcomes such as relieving the burden of care and strengthening relationships with loved ones are not included in the EQ-5D. Unfortunately, however, no valuation instrument exists that incorporates these specific end-of-life issues.38,68 | With only modest decreases in QoL, both selective chemotherapy and single-agent chemotherapy with home hospice strategies began to exceed ICERs of $100,000/QALY. This finding suggests that any survival advantage gained in the chemotherapy-containing treatment arms may be blunted by the associated treatment toxicities, quickly making them cost-prohibitive. 66 | Rehospitalization as indicator for QoL |
| QoL is an important dimension, particularly in the palliation of terminal illness. Unfortunately, information about the QoL weight (utilities) in patients with unresectable pancreatic cancer is limited. 45 | The results of this analysis are sensitive to changes in costs, but even more so to changes in utilities. 27 | Utilities on pain, since pain is the single most important factor affecting QoL | |
| Duration of survival is not a meaningful endpoint in palliative care […] Chronic pain has enormous effect on QoL of patients with bone metastases. Hence, the duration of survival, adjusted for the degree of response to pain treatment, is a more appropriate endpoint. 39 | |||
| No standardized method available for utility collection. […] May be possible QoL item may not cover all different domains QoL. 27 | |||
| We observed a high incidence of distressing symptoms that may influence the QoL during the course of disease and the process of dying. 40 | |||
| The main goals of palliative care and EoLC in brain tumor patients are to offer adequate symptom control, relief of suffering, avoiding inappropriate prolongation of dying, and to support psychological and spiritual needs of patients and families. The lack of control of symptoms in patients not included in palliative home-care programs often lead to rehospitalization with an increase in health system economic cost and worsening of patient QoL. 40 | |||
| Theme 3 | Patients were more willing to gamble the risks associated with surgery and the possibility of developing pain or complications to have an opportunity to prolong life than were healthcare providers. 65 | ||
| Study takes no account of diminishing marginal utility (extra 2 months of good QoL to life-expectancy of 6 months potentially more valuable than extra 2 months to much better average life- expectancy). 44 | |||
| A recent meta-analysis […] suggests that a value closer to $100,000/QALY might more accurately reflect societal preferences. 45 | |||
| A value closer to $100,000 per QALY might more accurately reflect societal preferences. 45 | |||
| Our results indicate that increased expenditures are needed to impact patients’ QoL for such morbid clinical conditions. 47 | |||
| Patients at the EoL tend to have low QALYs because of very poor health status […] this raises the question of whether economic evaluations […] ought to use some adjustment that would give additional weight to gains to health occurring at the EoL. 47 |
QALY: quality-adjusted life year; QoL: quality of life; EoL: end of life; EoLC: end-of-life care; ICER: incremental cost-effectiveness ratio; PalY: Palliative Care Yardstick; EQ-5D: EuroQol Five-Dimensional Questionnaire.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the EU 7th Framework Programme, grant agreement 6031111.