
Abstract
Background:
Patients with palliative care needs do not access specialist palliative care services according to their needs. Clinical Nurse Specialists working across a variety of fields are playing an increasingly important role in the care of such patients, but there is limited knowledge of the extent to which their interventions are cost-effective.
Objectives:
To present results from a systematic review of the international evidence on the costs, resource use and cost-effectiveness of Clinical Nurse Specialist–led interventions for patients with palliative care needs, defined as seriously ill patients and those with advanced disease or frailty who are unlikely to be cured, recover or stabilize.
Design:
Systematic review following PRISMA methodology.
Data sources:
Medline, Embase, CINAHL and Cochrane Library up to 2015. Studies focusing on the outcomes of Clinical Nurse Specialist interventions for patients with palliative care needs, and including at least one economic outcome, were considered. The quality of studies was assessed using tools from the Joanna Briggs Institute.
Results:
A total of 79 papers were included: 37 randomized controlled trials, 22 quasi-experimental studies, 7 service evaluations and other studies, and 13 economic analyses. The studies included a wide variety of interventions including clinical, support and education, as well as care coordination activities. The quality of the studies varied greatly.
Conclusion:
Clinical Nurse Specialist interventions may be effective in reducing specific resource use such as hospitalizations/re-hospitalizations/admissions, length of stay and health care costs. There is mixed evidence regarding their cost-effectiveness. Future studies should ensure that Clinical Nurse Specialists’ roles and activities are clearly described and evaluated.
Keywords
Resource use and costs tend to increase for patients with advanced disease and at the end of life.
Palliative care improves quality of life while reducing health care costs.
It is difficult to assess the effectiveness of Clinical Nurse Specialists (CNSs) working as individual providers.
CNSs have an important role in palliative care provision, but this is a role that is currently poorly recognized and not articulated.
CNS interventions are effective in reducing health care resource use such as admissions, re-hospitalization, length of stay and health care costs.
CNSs may have the potential to enhance quality at neutral or lower costs to health care system while enhancing or delivering similar clinical or patient-reported outcomes but that new studies are necessary that address characteristic methodological shortcomings.
The inclusion of CNSs in national strategies to improve palliative care and enable more people to benefit from a palliative care approach at all stages of illness is recommended
Introduction
There is some evidence that specialist palliative care (SPC) improves quality of care and reduces health system costs and resource utilization,1,2 but few who could benefit are likely to access SPC services (such as hospice care). 3 The Worldwide Palliative Care Alliance 3 estimated in 2014 that 20 million people require palliative care (PC) at the end of life, with another 20 million needing PC support earlier in the disease trajectory. Such patients may have their PC needs met to varying degrees by a variety of providers, but there is a lack of evidence about this, especially where multiple professionals are involved and among patients with conditions other than cancer. 4
Clinical Nurse Specialists (CNSs) play an increasingly prominent role in the support of people with PC needs, even if they do not have the term ‘palliative care’ in their job description or role title. The CNS role as an expert in evidence-based nursing practice in various fields is internationally recognized, although there are a wide variety of professional titles in use. 5 While there is no universally agreed definition of CNS, there is an international consensus that CNSs are nurses who have additional education, preferably at degree level or beyond. 6 An example of a widely accepted definition comes from the International Council of Nurses, which defines the nurse specialist as ‘… a nurse prepared beyond the level of a nurse generalist and authorized to practice with advanced expertise in a nursing field. Specialist practice includes clinical, teaching, administration, research and consultant roles’. 7
The extent to which CNSs focus on any of the latter areas either singly or in combination varies greatly. 8 CNSs frequently work as part of multidisciplinary groups; this makes it difficult to evaluate their effectiveness as individual providers. There is a risk that interventions that are difficult to evaluate such as those provided by CNSs may have less opportunities in the competition for resources compared to those with higher levels of evidence, 9 meaning that patients with PC needs may be unable to access any potential benefits.
Interventions delivered by CNSs can be described as ranging across several levels, from single patient contacts or advice provided to another staff member, through short-term involvement for multiple problems (such as provision of support and information at the time of diagnosis), and finally long-term involvement with patients with rapidly changing or deteriorating conditions. 10 All interventions delivered by CNSs are complex, 11 comprising several interacting components and with sensitivity to contextual conditions; this makes their evaluation challenging. Despite this, there is some existing research on CNS-led interventions in different settings and with a variety of patient groups showing evidence of clinical and cost-effectiveness. For example, a systematic review of the effectiveness and cost-effectiveness of CNS interventions in outpatient care settings shows reduced costs and resource use compared to usual care, together with consistent evidence of improved patient outcomes and largely similar health care system outcomes. 12 One evaluation of advanced nursing roles in 12 countries shows that CNSs improve access to services, reduce waiting times and, in some contexts, deliver quality of care equivalent to that provided by doctors, with high satisfaction rates among the patients and informal carers. 6 However, there are no systematic reviews of the cost-effectiveness of CNS-led interventions for patients with PC needs despite calls for greater understanding of the contribution that CNSs may be able to make to the quality and delivery of PC at scale. 13 Reasons for the lack of evidence relate in part to the conceptual challenges surrounding the assessment of cost-effectiveness of interventions for PC populations. 2
This article presents a systematic review of international evidence on the costs, resource use and cost-effectiveness of CNS-led interventions of different types for patients with PC needs.
Objectives
The objectives of the review were to
Examine the available international evidence on the cost or resource use of CNS-led interventions in patients with PC needs.
Examine the available international evidence on the cost-effectiveness of CNS-led interventions in patients with PC needs.
Describe the range of CNS-led interventions in patients with PC needs, within the identified international evidence
Methods
Protocol and registration
The protocol for this study was registered in the Prospero register of systematic reviews.
Eligibility criteria
Type of study
This review considered quantitative studies addressing cost-effectiveness of CNS interventions including randomized controlled trials (RCTs), quasi-experimental, before and after, prospective and retrospective cohort studies, case control studies, analytical cross-sectional studies, service evaluations and economic analyses.
Type of participants
We included adult patients (>18 years) with a clinical diagnosis of a life-limiting or life-threatening illness, who were unlikely to be cured, recover or stabilize; 4 please see Box 1.
Type of interventions
For the purpose of this review, interventions led by CNS (e.g. the CNS had an autonomous and clearly defined role) were included. Studies in which the training or level of education of the nurse was not clear, or in which the nurse was part of a multidisciplinary team (and thus their specific role cannot be established), were excluded.
Type of outcomes
Economic outcomes included the following: (1) costs; (2) objective measures of health system utilization such as length of stay (LOS), hospitalizations/readmissions or health resource use (e.g. medications); and (3) cost-effectiveness measures (e.g. incremental cost/effectiveness ratios). In order for studies to be included, they had to have at least one economic outcome.
Exclusion criteria
Articles were excluded if they were written in languages other than English or Spanish. Other exclusion criteria were as follows: studies published prior to 2000, unpublished or incomplete papers (e.g. conference abstracts or letters to the editor) and systematic reviews or descriptive articles; studies published that included interventions which were not directed exclusively to patients with advanced disease (e.g. if they also included a family member or carer). Interventions directed to children were also excluded.
Information sources
A pilot search in Medline and CINAHL enabled identification of possible terminology. Initially, a pilot search in Medline and CINAHL was undertaken to identify key terms with the guidance from a library expert. We also examined the search strategy employed in related systematic reviews 2 and contacted key authors for their full lists of search terms. In addition, we compared our search terms with the Mesh terms taxonomy in PubMed (and their equivalents in other databases). A second-stage search applied the identified key words and index terms across the following databases:
Medline via OVID (1946 to October 2015);
Embase via OVID (1980 to October 2015);
CINAHL via EBSCO (1986 to October 5 2015);
The Cochrane Library via Wiley (October 2015).
Search
Three groups of words and their equivalents were combined using OR within each group: (1) advanced disease (including palliative/terminal care/medicine or catastrophic/critical illness or hospice or neoplasm or aged or disease progression or terminally ill), (2) cost-effectiveness (including costs or economics or cost analysis or cost effective or cost benefit analysis or health care costs or patient readmission or LOS); and (3) Clinical Nurse Specialist (including advanced practice nursing or nurse practitioners or critical care nursing or nurse clinicians). Each group was combined again using the operator AND. All search strategies are presented in Supplementary Material Appendix 1.
Study selection
Study selection was conducted in two stages. First, all titles and abstracts were screened for relevance by at least two reviewers (N.S.-B. and J.S. or G.C.). Disagreement was resolved by consensus. Second, studies that met the inclusion criteria were obtained and read. Reasons for exclusion were documented. EndNote was used to manage references.
Data collection process and data items
Information was recorded in an Excel chart developed for this review. Data were extracted by a research assistant (N.S.-B.) and included the following: publication details (author, year), country, study design, disease, interventions and nurse activities, nurse training, outcomes, results and conclusions.
Synthesis of results
A narrative approach to synthesis was selected because of the great variety of study designs and outcome measures. It was not possible to conduct a meta-analysis of cost and resource utilization findings; instead, we focused on understanding and displaying patterns across the body of research. 2
Quality assessment
There is no universally validated scale to assess quality in quantitative studies, and there is little evidence that such scales improve the validity of conclusions drawn from systematic reviews. Most tools are scales or checklists. 14 We carried out quality assessment using software from the Joanna Briggs Institute for evidence-based health care 15 (Supplementary Material Appendix 2). Two reviewers independently answered each question; any disagreement was resolved by consensus. While we did not exclude studies on the basis of our quality assessment, we provide detailed information about study quality within the paper and its appendices.
Results
Study selection
A total of 7731 papers were obtained from the initial database search (Figure 1). After adjusting for duplicates, 5984 citations remained. Of these, 5749 studies were discarded after reading the title and/or abstract because they clearly did not meet the inclusion criteria. The full text of the remaining 235 articles was read and assessed for eligibility. Of which, 156 studies did not meet the inclusion criteria; the reasons for their exclusion were documented. A total of 79 studies were included in this review.
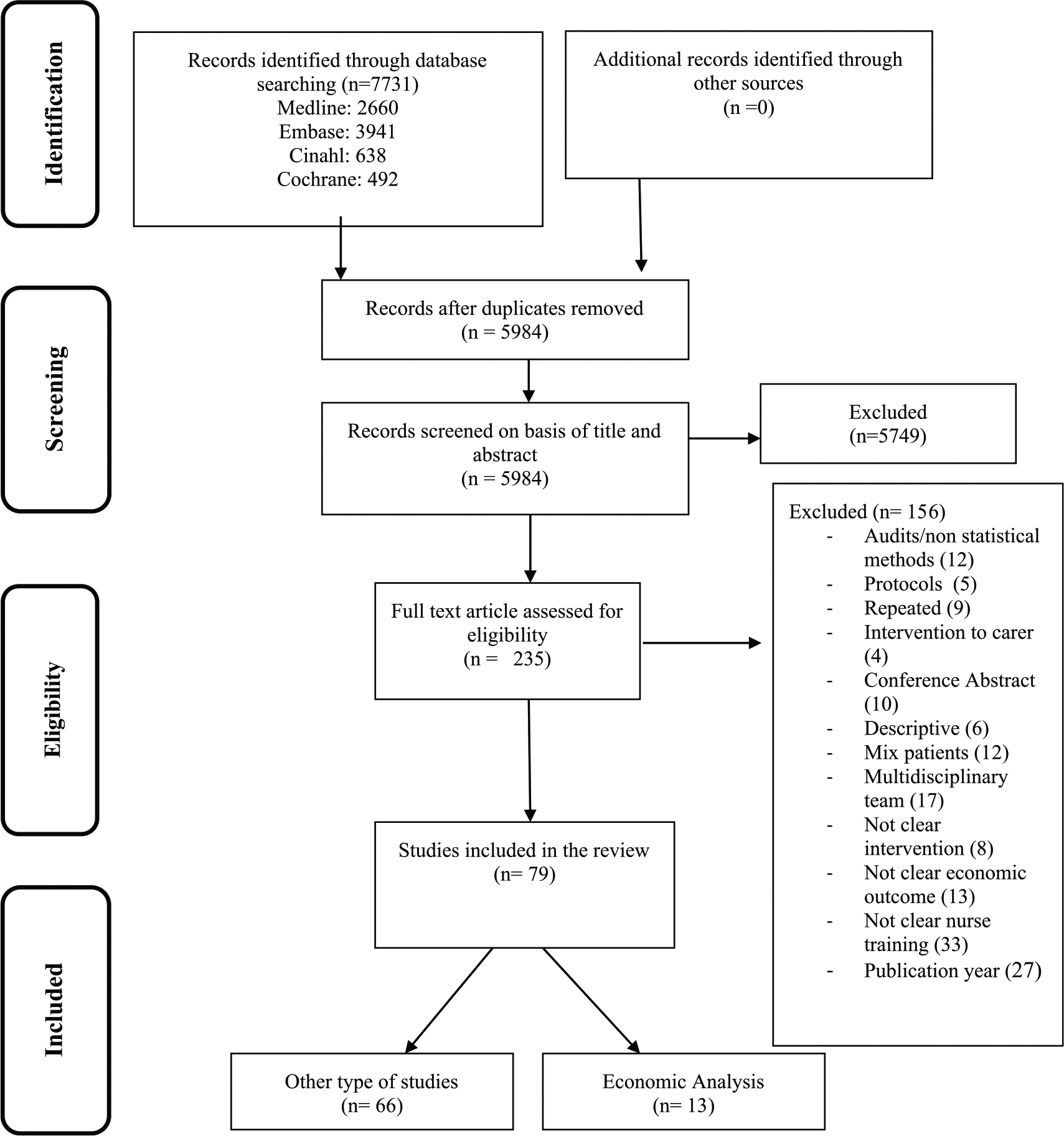
PRISMA flow diagram.
Study characteristics
General characteristics
Around 60% of the studies were conducted in the United States and the United Kingdom (27 and 20 studies, respectively) (Figure 2(a)). The majority of studies were conducted in patients with heart failure (HF)16–36 (26.6%) or cancer (25%)37–53 (Figure 2(b)). We found 13 papers reporting formal economic analyses (such as cost-effectiveness ratios),16,30,31,33,35,39,44,47,54–58 9 of which were based on RCTs16,30,31,35,39,47,54,57,58 and 4 of which were other type of studies.33,44,55,56 We describe this group of studies separately, given the objectives of this review. A further 37 papers reported RCTs where economic outcomes, such as costs or resource use, were included as part of a wider set of outcomes.18,19,23,24,26,27,29,34,37,38,41–43,45,49–52,59–77 In all, 22 papers reported quasi-experimental studies20–22,25,28,32,36,40,46,53,78–89 and 7 reported service evaluations or other types of studies17,48,90–94 (Figure 2(c)). A wide variety of terms were used to describe nurses’ titles (Figure 2(d)), with the most common term being ‘nurse specialist’, employed by one-third of the studies.16–18,27,30,31,33–35,39,42,43,46,47,50,52,54,64–66,72,73,75,76,78,87
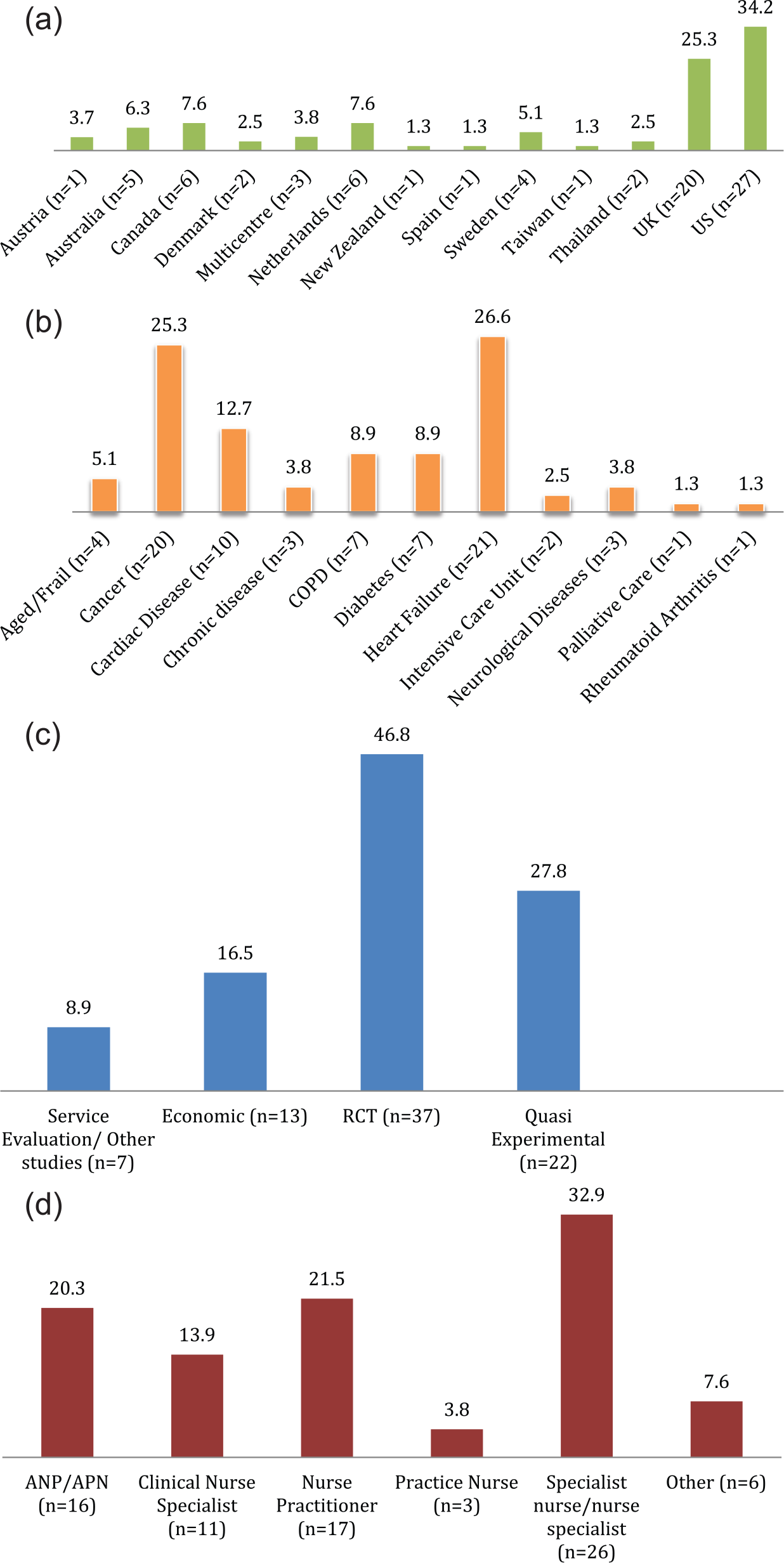
Characteristics of included studies: (a) studies by country (%), (b) studies by disease (%), (c) study designs (%) and (d) nurse title (%).
Interventions: type and setting
A wide variety of interventions were described. In general, interventions were complex and involved multiple interacting components (Figure 3).
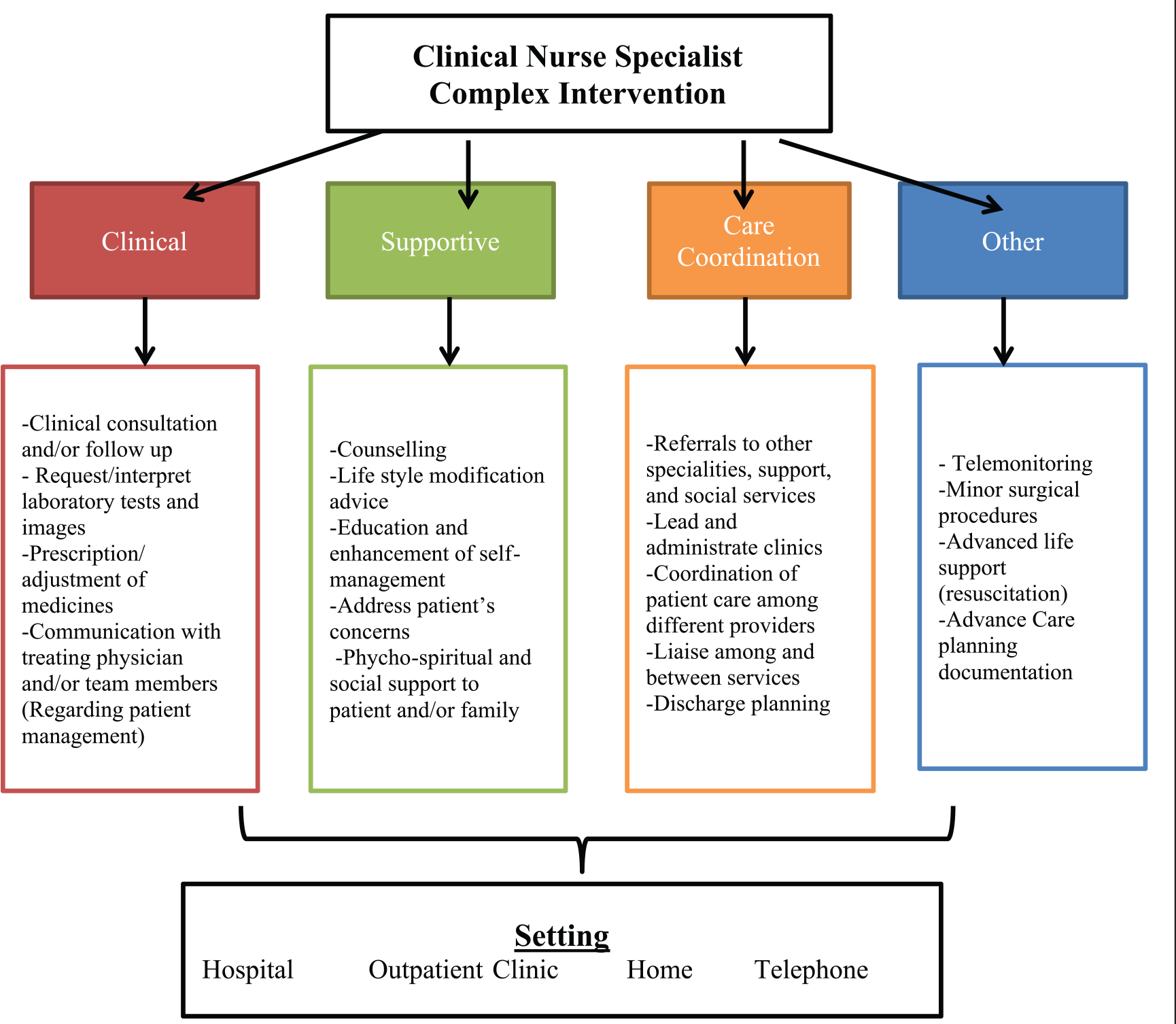
Components of Clinical Nurse Specialist interventions.
Interventions in which the clinical component was predominant included activities directed to the diagnosis, treatment and control of the disease and were performed in hospitals, outpatient clinics or patients’ homes.
Some papers described interventions that were supportive. They sought to increase patients’ knowledge about their disease and its management, and at the same time aimed to give psychological/spiritual support.
The roles adopted by the CNSs were usually reported to be multiple, and in many cases included care coordination activities.
Table 1 shows the components of the interventions (e.g. nurses’ specific activities) in each of the included papers. It was not always clear what the specific activity involved. For example, use in the papers of general terms such as ‘in-hospital care and self-care’, 80 or ‘monitoring patient’s condition’, 62 made it difficult to identify nurses’ specific activities. We found a wide range of activities reported, including clinical consultations (in hospitals, at home, specialist clinics or via the telephone), the request of follow-up investigations, prescription or adjustment of medications, referrals to other agencies or staff, provision of support directed at overall well-being, and education to enhance self-management, as well as administrative work and liaison and communication with other professionals.
Components of CNSs interventions.
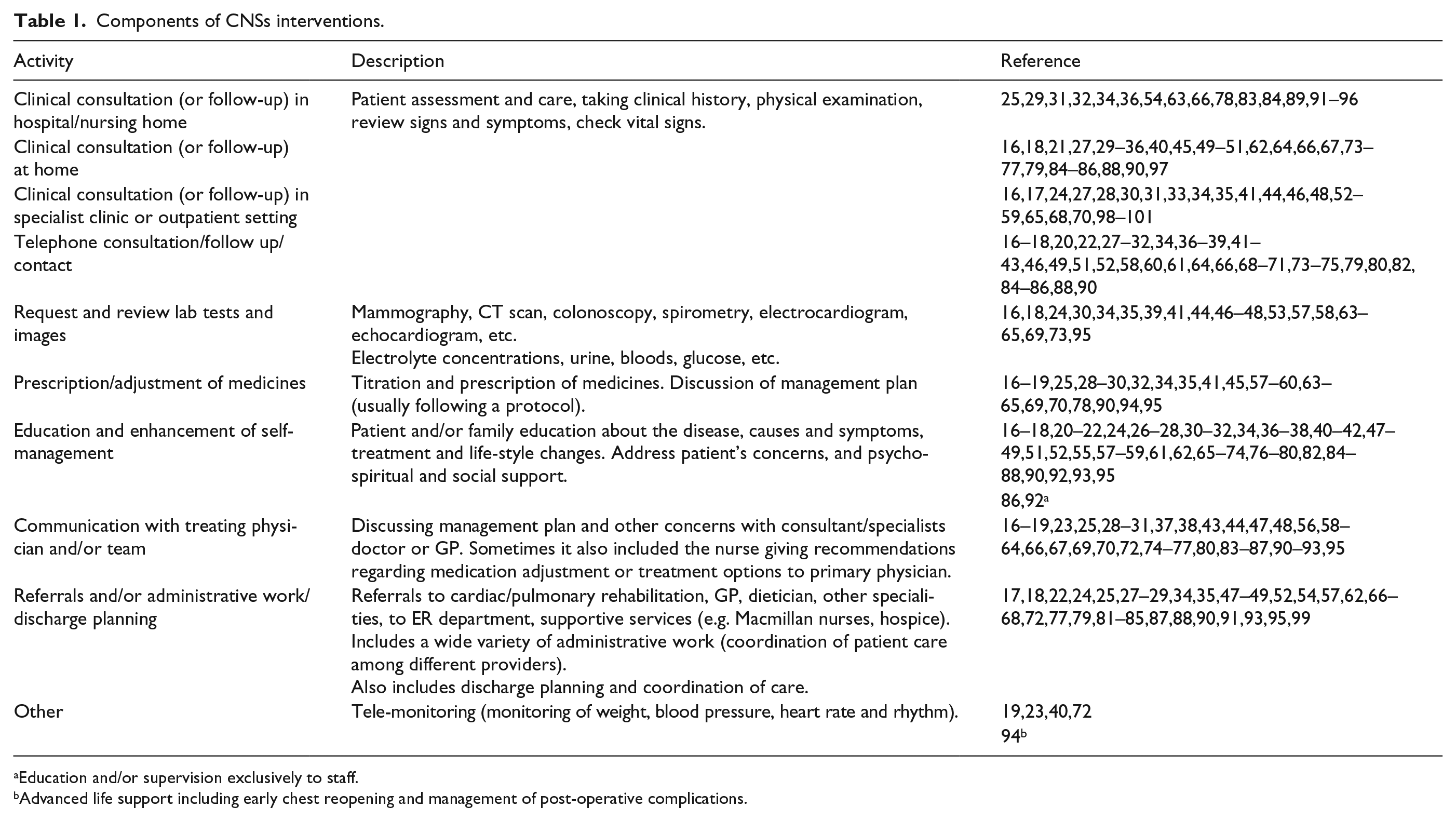
Education and/or supervision exclusively to staff.
Advanced life support including early chest reopening and management of post-operative complications.
General characteristics by study type
Economic studies (n = 13)
A total of 13 economic papers were included. Three reported a modelling of economic data (observational studies).33,55,56 A further nine reported RCTs.16,30,31,35,39,47,54,57,58 The final paper reported a prospective study. 44 In general, studies compared usual care (e.g. care provided by doctor or care provided in hospitals), with nurse specialist care (e.g. specialist clinic, home visit or telephone follow up). Two studies compared interventions with different amount of nurse involvement (e.g. high- vs low-level support).31,55 Table 2 shows the main characteristics of the economic studies, which are described in the following paragraphs.
Characteristics of economic studies.
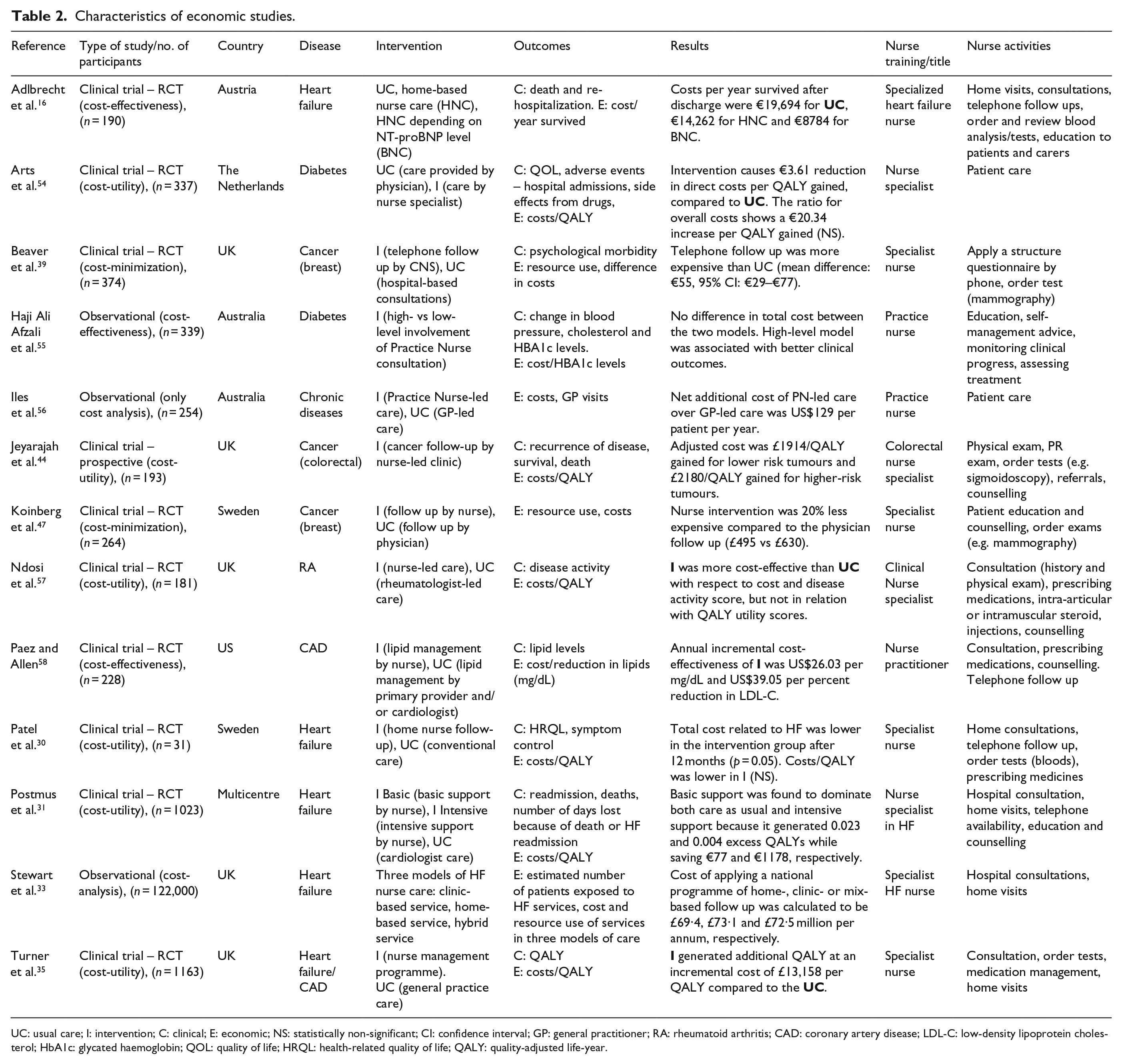
UC: usual care; I: intervention; C: clinical; E: economic; NS: statistically non-significant; CI: confidence interval; GP: general practitioner; RA: rheumatoid arthritis; CAD: coronary artery disease; LDL-C: low-density lipoprotein cholesterol; HbA1c: glycated haemoglobin; QOL: quality of life; HRQL: health-related quality of life; QALY: quality-adjusted life-year.
Six cost-utility analyses analysing the cost per QALY gained were found.30,31,35,44,54,57 Three cost-effectiveness studies were included comparing the cost per gained health outcome (e.g. year survived, 16 HBA1c levels 55 and lipid-level reduction 58 ). Beaver et al. 39 and Koinberg et al. 47 performed cost-minimization studies measuring and comparing input costs, and assuming outcomes to be equivalent. Finally, Stewart et al. 33 and Iles et al. 56 reported cost analyses.
Totally, 11 out of 13 studies reported costs from one-third party/health care system perspective (e.g. only direct costs were considered). Two studies included additional costs. Beaver et al. 39 included indirect costs such as number of missing days at work and patient transportation costs. Ndosi et al. 57 calculated costs from the perspectives of the NHS (clinic and NHS resources), health care (NHS plus out-of-pocket) and ‘societal perspective’ (including loss trough time off work). The way costs were calculated varied across studies.
RCTs (n = 37)
A total of 37 RCTs were included. Most compared a specialist nurse intervention with standard care (e.g. physician-led care or usual care).18,27,29,34,41,43,49–52,59,61–71,73–77 Four interventions described tele-monitoring or telephone follow up in patients with HF,19,23 colorectal cancer 42 and chronic obstructive pulmonary disease (COPD). 72 Bakitas et al.37,38 described a multicomponent educational intervention for patients with advanced cancer, Berkhof et al. 60 evaluated the effects of an outpatient on-demand interventions for patients with COPD, while Cockayane et al. 24 and Heisler et al. 26 described novel interventions for patients with HF. Finally, King et al. 45 evaluated the effects of home-based chemotherapy given by CNSs to cancer patients.
Quasi-experimental studies (n = 22)
In total, 2 out of 22 papers described telephone/monitoring follow-up interventions for patients with cancer and HF, respectively.20,40 One describes the impact of the Evercare managed care intervention led by CNSs on hospital use in a nursing home population. 83 There was a broadly equivalent focus in terms of setting with regard to the studies: eight reported CNS-led interventions targeted at hospital patients25,28,78,80,81,87–89 and nine reported CNS-led interventions in the community or care home, which included the following: transitional care, care management and self-care/disease management interventions.21,22,32,36,79,82,84–86 Two studies focused on CNS-led follow-up clinics as part of a multidisciplinary management programme for patients with rectal cancer.46,53
Service evaluation and other type of studies (n = 7)
Five studies reported outcomes of ‘before and after’ evaluations of specialist nurse-led services, including home-based PC, 91 monitoring and taking care of intensive care unit (ICU) 94 and tracheostomy patients, 92 and outpatient clinics for patients with HF 17 or head and neck cancer. 48 Comparison was characteristically made with patients acting as their own controls or with a different cohort of patients prior to the initiation of the intervention. The remaining two studies comprised a natural experiment using a pre–post design to evaluate the effect of a transitional care clinic for individuals discharged from a skilled nursing facility 93 and a retrospective observational cohort study of the effects of a home-based cardiac surgery nurse practitioner intervention on readmissions. 90
Synthesis of results
Results by study type
RCT
A total of 17 RCTs did not report any significant difference between groups in terms of LOS, emergency department (ED) visits, number of days in the ICU, medication use or readmissions.19,24,26,37,38,42,43,49,52,60,63,67–69,71,72,75 They examined a model of CNS-led disease management or self-management in HF,19,24,26 cardiac care,63,67,68,71 COPD,60,72 cancer care37,38,42,43,49,52,75 or chronic diabetes. 69 Six studies examined a formal PC or supportive care model,26,37,38,42,43,52 and two examined the use of CNS-led tele-care or tele-monitoring.19,72
Nevertheless, 13 RCTs reported that CNS-led interventions were effective in reducing specific economic outcomes. Four RCTs reported reduction in doctors’ visits (GP or specialist visits),49,60,61,63 two reported reductions in ED visits,64,77 five reported reductions in hospital readmissions18,29,34,62,64 and seven reported reductions in LOS.18,23,27,34,61,64,77 Two RCTs found that CNS-led interventions were effective at increasing the use or prescription of medications.34,59
CNS-led interventions were found to be less expensive than usual care in 4 out of 20 studies reporting costs.29,41,64,65 A further 2 of the 20 studies reporting costs found that CNS interventions were more expensive,70,74 although in each case, the potential for cost-effectiveness was noted due to other positive outcomes. For example, Strong et al., 74 in a trial of a nurse-led clinic for management of people with depression due to cancer, reported that it was potentially cost-effective due in terms of the increase in quality-adjusted life-years achieved, as well as achieving good feasibility and acceptability. In all, 14 studies found non-significant or inconclusive results regarding costs.19,43,45,50,51,59–62,66,69,73,75,76
Quasi-experimental studies
Readmissions were reduced in the intervention group in 10 out of 17 studies reporting this outcome:20,22,25,28,32,79,80,83,84,86 5 evaluated a disease management CNS-led intervention for patients with HF or cardiac disease,20,22,25,28,80 3 evaluated a transitional care model led by CNSs32,84,86 and 1 each evaluated a case management model – Evercare led by a CNS for long-term care residents 83 and a CNS-led psychosocial support intervention for patients with heart disease. 79
LOS was also reduced in 8 out of 13 studies22,25,28,81,83,84,86,88 employing a similar range of care models, that is, disease management,25,28,81 case management83,88 and transitional84,86 or home-based care. 22 Three of these latter studies also reported that CNS-led interventions reduce costs of care.22,81,84 The CNS-led case management intervention in a long-term care population (Evercare) increased doctors’ visits (GP) to the long-term care facilities at the same time as reducing transfers to hospital, 83 while two of the disease-management-directed CNS-led interventions for patients with HF similarly increased prescription and use of medications among recipients.25,28 Reynolds et al. 89 found, in a study comparing hospital follow-up care led by consultants with care led by Parkinson’s disease nurse specialists, that the intervention was significantly more expensive compared to the control group.
Service evaluation and other type of studies
Of the seven studies included in this category, four showed statistically significant reductions in re-hospitalizations;48,90,91,93 Lukas et al. 91 and Park et al. 93 also found that the CNS services reduced LOS. Regarding medication use, one study reported an increase in the prescription of medicines on the intervention group after the introduction of a CNS clinic for HF patients, 17 and one of the palliative and supportive care interventions enhanced chemotherapy treatment completion and reduced on treatment dose deviations. 48 Two interventions reported a reduction in hospital 91 and direct readmission costs.
Results of cost-effectiveness (economic evaluation studies)
In total, 13 studies were identified that may be classed as formal health economic studies and in which there was a variety of evidence about cost-effectiveness. Most evidence was from studies of HF nurse specialists or CNSs working with high-risk coronary heart disease patients,16,30,31,33,35,58 although there were also some studies of CNS-led cancer care39,44,47 and of other conditions.54–57
In seven studies, there was clear evidence of cost-effectiveness or improvement on health economic outcomes,16,31,33,35,44,47,58 five of which considered interventions in heart disease or cardiac care patients: Adlbrecht et al. 16 showed in Austria that the supporting home-based nursing care with specialist nurses was both cost-effective and cheaper than standard care for HF patients. The costs per year survived after discharge were significantly lower for the intervention group compared to usual care. In the United States, incorporating nurse case management of cardiovascular disease risk factors into primary care settings was shown to be similarly cost-effective. 58 The annual incremental cost-effectiveness of NP case management was US$26.03 per mg/dL and US$39.05 per percent reduction in low-density lipoprotein cholesterol (LDL-C). 58 It is important to consider that this conclusion should be interpreted with caution since the results are given in terms of costs/lipid reduction, which is a risk factor and nor at disease per se. A cost-utility analysis in the United Kingdom showed that a nurse-led disease management programme for patients with heart disease was cost-effective, generating an additional QALY at an incremental cost of £13,158 per QALY, compared to the control group. 35 In England, an observational study showed that a specialist nurse home service improves quality of life and reduces readmissions in patients with congestive HF, while also reducing costs. 33 In a large-scale multicentre trial in the Netherlands among patients with HF, offering basic support to patients with mild to moderate HF and intensive CNS support to patients with severe HF improved health outcomes at slightly higher costs. 31
Finally, two studies of cancer care by CNSs also demonstrated cost-effectiveness. These included a trial of a UK nurse-led follow-up clinic for patients with colorectal cancer 44 and a 5-year follow-up study in Sweden of patients with breast cancer showing that CNS-led care was cheaper and led to similar outcomes compared to physician-led care (€495 vs € 630 per person, respectively). 47
In four studies, cost-effectiveness was not demonstrated mainly because of methodological challenges. In the first of these, a study of nurse-led care compared to physician-led care of patients with rheumatoid arthritis, 57 CNS care was shown to be equivalent in terms of quality and in some cases cheaper. In the second study, home-based CNS follow up of patients with HF in Sweden was shown to be significantly cheaper at 12 months than standard care, at equivalent clinical outcomes, although small number of patients made conclusions difficult to draw. In addition, costs per QALY were lower in the home care group but the difference did not reach statistical significance. 30 In the third study of CNS-led care for patients with diabetes, CNS-led care generated a modest reduction in costs per quality-adjusted life-year gained compared to usual care, although statistical significance was not reached. 54 Similar conclusions were reached in Australian study of CNS-led care for people with diabetes. 55
The remaining two studies classified as economic analysers included a short-term cost-minimization study examining a telephone follow-up CNS-led intervention for patients with breast cancer in the United Kingdom 39 and a cost analysis of effects of practice nurse-led care for chronic diseases. 56 In both cases, the interventions were associated with higher costs compared to usual care although some patients preferred these care models.
Results of costs and resource use
The most common economic outcomes reported were costs and readmission rates (Table 3). We found that CNS interventions may be effective in reducing health care costs (13 out of 46 studies reported statistical significant reduction16,22,29,30,41,47,57,64,65,81,84,90,91). Another 22 out of 46 studies reported that the intervention increases costs, although the results were statistically significant in only six of them.35,39,56,70,74,89
Regarding resource use (Table 3), there is evidence that CNS interventions may be effective in reducing hospitalizations and/or readmissions (20 out of 46 papers showed statically significant reductions in this outcome, while the remaining 26 did not report significant levels or reported non-significant results). LOS was significantly reduced in 17 out of 33 studies, and only 1 study showed that the intervention significantly increases LOS. 36 The rest of the papers (15 out of 33) reported no significant levels or it was not clear.
Summary of outcomes: resource use, costs, and cost-effectiveness.
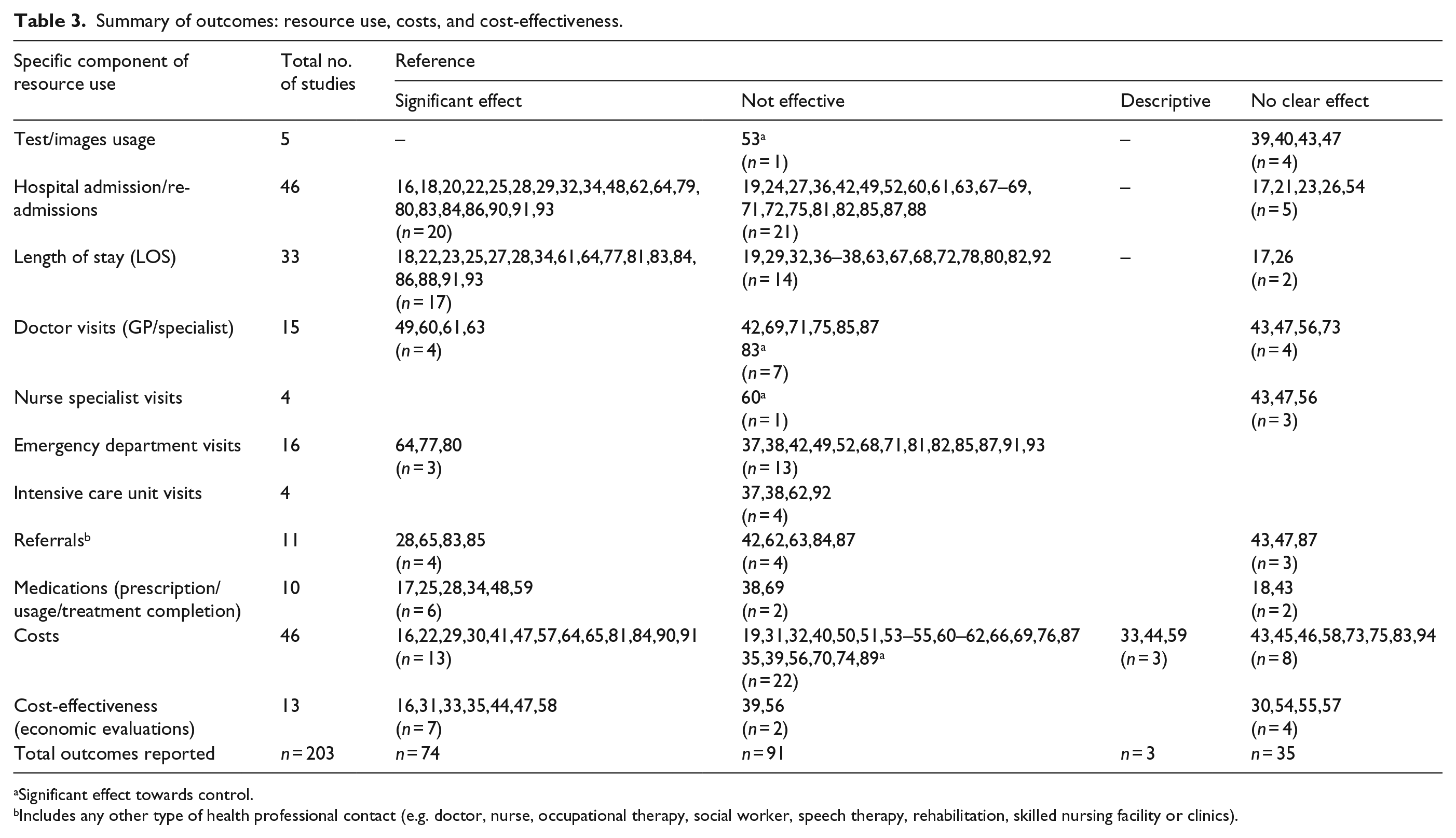
Significant effect towards control.
Includes any other type of health professional contact (e.g. doctor, nurse, occupational therapy, social worker, speech therapy, rehabilitation, skilled nursing facility or clinics).
There is insufficient evidence to demonstrate that CNS interventions lower days in the UCI or ED visits. Four studies reported UCI days, all of which showed non-significant changes between groups.37,38,62,92 Regarding ED visits, only 3 out of 16 studies found that intervention group significantly reduced this outcome,64,77,80 while the remaining 13 showed no significant changes.37,38,42,49,52,68,71,81,82,85,87,91,93
There is also insufficient information to make conclusions on the effect of doctors (general practitioners or specialist/consultant) and CNS visits in any setting (Table 3). Of 15 studies describing the utilization of doctors/physicians as an outcome, only 4 reported a statistically significant decrease in doctors’ visits in the intervention group: Berkhof et al. 60 concluded that COPD patients in the intervention group visited GPs significantly less (but CNSs more) than those in the control group. McCorkle et al., 49 Davies et al. 61 and Goldie et al. 63 found that women in the control group visited their primary care providers less often compared to those in the intervention group. However, another study found opposing results, 83 and others were inconclusive43,47,56,73 or reported non-significant results.42,69,71,75,85,87 There was a lack of evidence regarding CNS visits. Of 4 studies examining the latter, one concluded that intervention group had significantly more visits to the specialist nurse 60 and the other three were inconclusive.43,47,56
There was some evidence with regard to referrals (e.g. to other health care professionals, health services or clinics). Of 11 studies, 7 were inconclusive (showing non-significant differences or not reporting significant levels.42,43,47,62,63,84,87 In contrast, four studies reported significant differences regarding referrals. In the first, Naylor et al. 85 concluded that the intervention reduced home health aides (p = 0.008) and physical therapy referrals (p = 0.001), although no significant changes were found for occupational therapy, social worker, vocational training, speech therapy and rehabilitation. In the second, an evaluation of a CNS disease management model for HF, Lowery et al. 28 concluded that the intervention significantly increased referrals to primary care and cardiology clinics. Kane et al. 83 found significant changes in referrals for physical, occupational and speech therapy, and podiatry, while Houweling et al. 65 found that the percentage of patient referred back to the GP on the last months was significantly higher in the CNS intervention group.
Five studies reported the use of laboratory test or images as an outcome, of which four did not find or report statistical significant changes.39,40,43,47 In an exception to this pattern, the fifth study 53 found that CNS requested significant more blood samples compared to surgeons when following up colorectal cancer patients.
Medication prescriptions were significantly increased in the intervention group in two studies,17,59 and medication uptake/use by patients was raised in another three studies.25,28,34 A study of a CNS-led supportive care intervention for patients with head and neck cancer found that in the intervention group, there was a statistically significant chemotherapy treatment completion and dose reduction compared to the control group. 48 Four studies either did not find or did not report significant levels on this outcome.18,38,43,69
Table 3 summarizes the components of resource use: studies that reported a statistically significant effect towards the intervention group (or after the intervention in ‘before and after’ studies) on specific outcomes were classified as effective (a total of 74 outcomes were reported as effective in the included studies). However, studies that reported a significant effect favouring the control group, or those reported non-significant outcomes, were classified as non-effective interventions (91 outcomes). Some of the studies did not report any significant level (or it was not clear after reading the article). In this case, papers were classified as not clear for that specific outcome (35 outcomes). A small number of papers (5 out of 92) did not compare outcomes between groups, and reported a specific value in specific outcomes (e.g. cost of intervention); these were classified as descriptive.
Study quality
A summary of the quality of the included studies is presented in Figure 4(a)–(c). The RCTs scored well on most quality indicators including randomization procedures, statistical analysis, clear description of interventions and measurement of outcomes using reliable instruments. The quasi-experimental studies had greater variability in quality. Although, in general, statistical methods used were clearly described and outcomes were measured in a reliable way for both groups, randomization procedures were not always described and it was not always clear whether an intention to treat analysis was performed or whether the groups were treated similarly other than the intervention. There was variation in RCTs and quasi- experimental studies on whether participants or allocators were blinded to treatment group allocation and whether control and intervention groups were comparable at entry to the trial. Economic evaluation studies were of good quality as well, having clear research questions and descriptions of the way costs were calculated. Weaknesses were lack of reporting of adjustments of cost for differential timing and variability in whether sensitivity analysis was performed.
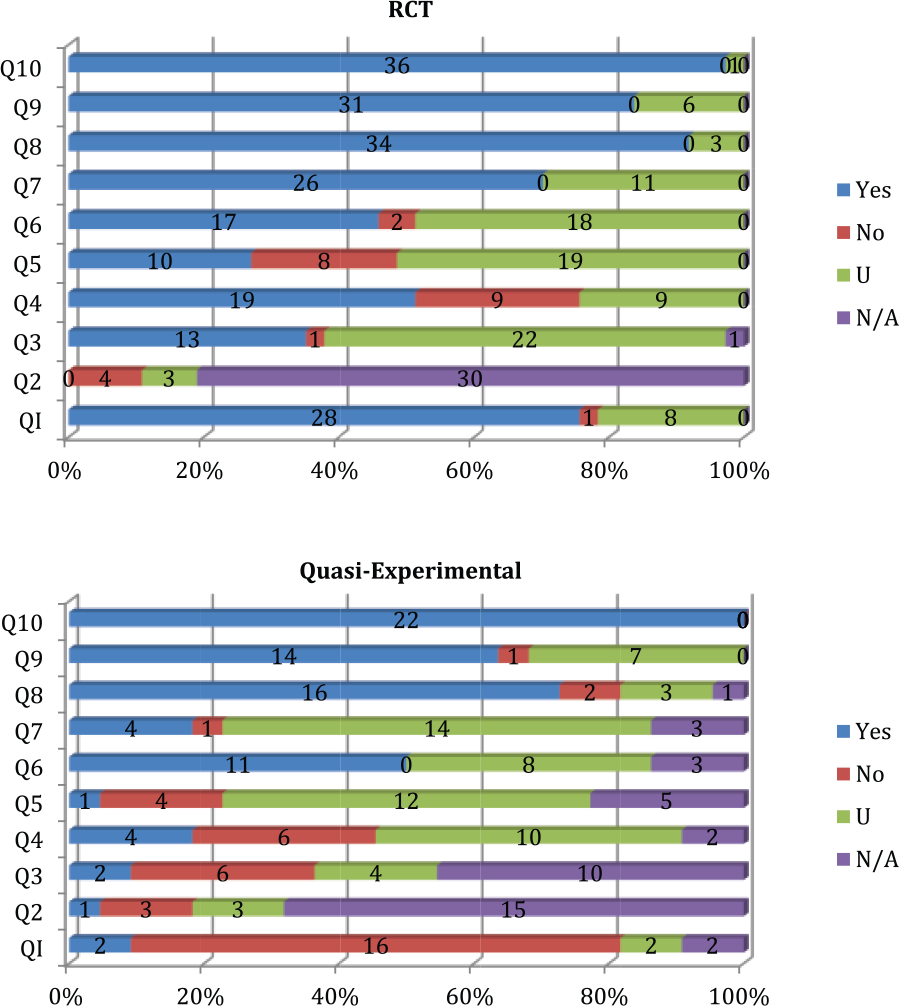
Quality assessment of randomized controlled trials and quasi-experimental studies.
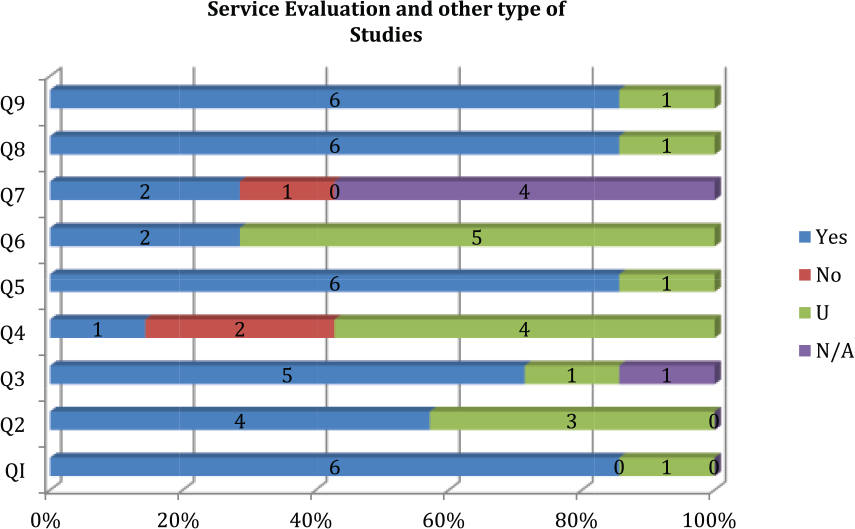
Quality assessment of service evaluation and other type of studies.
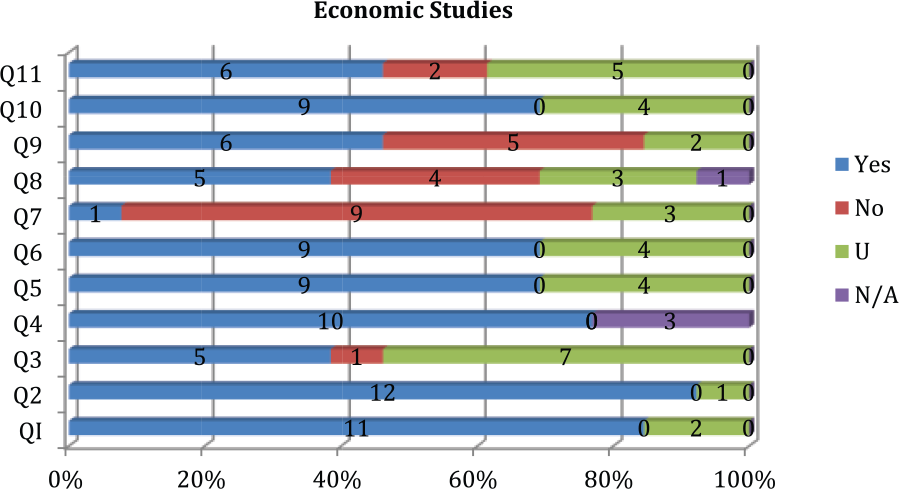
Quality assessment of economic evaluation studies.
The service evaluation and other studies had variable quality. They had some limitations regarding the description and inclusion in analysis of outcomes of people who withdrew from the study, strategies to identify and deal with confounding factors and sufficient length of follow up. Please refer to Supplementary Material Appendix 3 for more information about each specific study.
In general, because of the nature of the studies was reviewed, some criteria, such as concealing treatment groups and blinding participants, were not applicable to all the studies. In many cases, the CNS interventions were not well described, so it was difficult to evaluate whether the groups treated identically other than for the named intervention.
Discussion
Summary of evidence
This systematic review suggests that CNS interventions for patients with PC needs may be effective in reducing health care costs. In total, 13 out of 46 studies reported statistically significant reductions in costs, and 6 concluded that the intervention significantly increased costs. However, many of the studies were limited in terms of the length of follow-up. We therefore know little about the long-term cost implications: even if costs are increased short term by a CNS intervention, CNS-led care may lead to health care costs being off-set over time. This may be due to a decrease in preventable events and better satisfaction/quality of care experience; greater access to treatment/care. Moreover, the methodology used to calculate costs in each study was different and often not clearly described, which might affect the final conclusion.
The evidence regarding resource use shows that CNS interventions may also be effective in reducing specific outcomes, specifically hospitalizations and re-hospitalizations/admissions, as well as LOS. Very few studies concluded that the intervention significantly increased these outcomes, while an important proportion of them reported positive effects in reducing them. Similarly, 6 out of 10 studies showed significant increase in prescription and usage of medications, suggesting that CNS interventions may enhance this outcome.
However, there is insufficient evidence to make conclusions regarding ED and ICU visits, as well as doctor and nurse specialist visits, referrals and labs/exams/images.
Overall, the evidence regarding the cost-effectiveness of CNS interventions is inconclusive. Although 7 out of 13 economic analyses reported some grade of cost-effectiveness, 4 more were inconclusive and 2 more concluded that the intervention was more expensive.
Limitations
Although an attempt was made to include research relating to interventions exclusively performed by CNS for patients with PC needs, or in which CNS had a clear defined role, the boundaries between what the CNSs did and the input of other contributors were often hard to assess when deciding about study inclusion. All the interventions described in the studies included in the review were complex: they had various interacting components, and frequently involved flexible activities on the part of the CNSs delivering care to patients. 11
A variety of different interventions were reported in the included studies. Nevertheless, it was not always clear what the nurses’ roles (specific activities) were. For example, when using words such as ‘patient assessment or care’, or when a CNS was introduced into an existing in-hospital service and specific tasks were not clearly described. In those papers in which the role was described in more detail, we found that the nurses’ activities could be mainly clinical, supportive or administrative/care coordination.
Although some authors developed their own inclusion criteria and definitions, we found an extensive variety of terms to describe a ‘CNS’ and a frequent lack of specification of their experience and training. This has made it challenging to consolidate evidence related to cost-effectiveness.
Moreover, we used a broad definition of patients with PC needs to reflect the reality of the range and complexity of patients with different diseases and different phases of illness who can benefit from PC. This gave rise to challenges in comparing and contrasting the studies. The applicability of this evidence is further limited by the preponderance of research from resource rich countries (especially the United States and the United Kingdom), with diverse health care systems and funding.
The quality of included studies is variable. Many were not randomized and did not use a control group, affecting the validity and reliability of the results. In total, 46 (9 of which were economic analyses) out of the 92 included studies were RCTs, and they included multiple outcomes, patients and interventions. In some, the study population was small and approaches to statistical analysis were not clear; some did not report statistical significance.
Conclusion
This review provides an insight into the wide range and complexity of engagement of CNSs with patients with PC needs, in many different settings of care. However, it highlights important limitations in the evidence base that should be considered when developing further research, and when considering from a strategic planning perspective whether CNSs may be able to contribute to the provision of PC at scale, given the range and complexity of patients in need in contemporary health care systems 102 and the unlikelihood of being able to ensure that every person in need access a dedicated specialist PC service.103,104
Our review suggests that CNSs may have an important role in PC provision, but this is a role that is currently poorly recognized and rarely clearly articulated. In terms of cost and cost-effectiveness, it is clear that CNSs may have the potential to enhance quality at neutral or lower costs to health care system while enhancing or delivering similar clinical or patient-reported outcomes but that new studies are necessary that address characteristic methodological shortcomings. Future research of the CNS contribution to PC should ensure that the CNSs’ expertise, training and specific intervention(s) are clearly described, focus on patient-perceived benefits and include longitudinal study of economic impact. In the meanwhile, consideration should be given to the inclusion of CNS-led care in national and international policies aimed at integrating PC into wider health care and thus enabling more people to benefit from a PC approach at all stages of illness. 105
Footnotes
Acknowledgements
Registration: Protocol registration Prospero CRD42016033689.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Marie Curie Research Grants Scheme (grant no. C306277/A18867).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.