
Abstract
Background:
Clinical uncertainty is emotionally challenging for patients and carers and creates additional pressures for those clinicians in acute hospitals. The AMBER care bundle was designed to improve care for patients identified as clinically unstable, deteriorating, with limited reversibility and at risk of dying in the next 1–2 months.
Aim:
To examine the experience of care supported by the AMBER care bundle compared to standard care in the context of clinical uncertainty, deterioration and limited reversibility.
Design:
A comparative observational mixed-methods study using semi-structured qualitative interviews and a followback survey.
Setting/participants:
Three large London acute tertiary National Health Service hospitals. Nineteen interviews with 23 patients and carers (10 supported by AMBER care bundle and 9 standard care). Surveys completed by next of kin of 95 deceased patients (59 AMBER care bundle and 36 standard care).
Results:
The AMBER care bundle was associated with increased frequency of discussions about prognosis between clinicians and patients (χ2 = 4.09, p = 0.04), higher awareness of their prognosis by patients (χ2 = 4.29, p = 0.04) and lower clarity in the information received about their condition (χ2 = 6.26, p = 0.04). Although the consistency and quality of communication were not different between the two groups, those supported by the AMBER care bundle described more unresolved concerns about caring for someone at home.
Conclusion:
Awareness of prognosis appears to be higher among patients supported by the AMBER care bundle, but in this small study this was not translated into higher quality communication, and information was judged less easy to understand. Adequately powered comparative evaluation is urgently needed.
Keywords
Clinical uncertainty towards the end of life is emotionally challenging for patients and carers and professionally challenging for clinicians.
Poor communication is a common problem in health care, especially in the more advanced stages of disease.
The AMBER care bundle may improve awareness of prognosis and frequency of discussions between clinicians and patients and carers in the presence of clinical uncertainty. The AMBER care bundle did not appear to improve patient or family reported views of communication, and those who were cared for supported by AMBER had more concerns regarding home care.
Poor communication in the acute hospital setting continues to be an issue. Robust evaluation of the AMBER care bundle is urgently needed.
Introduction
Clinical uncertainty towards the end of life is distressing for patients and families.1–3 However, sharing the clinical situation, including uncertainty, is central to establishing preferences and priorities, enabling collaborative decision making 4 and empowering patients and carers.5–7 While clinicians’ disclosure of clinical uncertainty with patients can be associated with increased satisfaction,8,9 without explanation it is associated with poor satisfaction, mistrust and loss of confidence in the clinicians.10–13
Recent reports have highlighted failings in open and honest communication with patients and carers.14,15 Care in acute hospitals often focuses on immediate clinical problems with little recognition of transitions between clinical phases 16 and inadequate communication with patients and families. 17 Throughout their last year of life, people spend up to 1 month in hospital; currently, 53% of all deaths in England occur in hospital, 18 despite most people expressing a preference to be cared for, and die, at home. 19 This has led to calls for preferences and priorities to be discussed earlier in patients’ disease trajectories. 20
The AMBER care bundle was developed to improve care for patients in the acute hospital setting who are deteriorating, clinically unstable, with limited reversibility and at risk of dying in the next 1–2 months. 21 This intervention has an algorithmic approach and is intended to encourage the clinical team to develop and document a clear medical plan and consider anticipated outcomes and resuscita-tion and escalation status; this is revisited daily (see Supplementary Appendix 1). The bundle also aims to increase frequency of communication with patients and family regarding treatment plans, preferred place of care and other concerns. While it prompts advance care planning, the AMBER care bundle differs from advance care planning tools because it shapes current management as well as plans for future care. The AMBER care bundle has been identified as a key enabler in the transforming end-of-life care in acute hospital programme 22 and is now being piloted or used across 38 hospitals in England. Moreover, it is also being piloted in nine hospitals in New South Wales, Australia. Importantly, it has not yet been evaluated in a comparative study. 23 This study, therefore, aimed to examine the experience of care supported by the AMBER care bundle compared to standard care in the context of clinical uncertainty, deterioration and limited reversibility.
Methods
Design
In this mixed-methods 24 observational study, we compared the experiences of care for people supported by the AMBER care bundle with those receiving standard care, using contemporary qualitative interviews with patients and carers and followback surveys of bereaved caregivers.
Setting
There were three large London acute tertiary National Health Service (NHS) hospitals: two where the AMBER care bundle was fully implemented (comparison wards not possible) and hospital 3 with implementation on five wards (permitting comparison). The AMBER care bundle wards in hospital 3 were as follows: one respiratory, two endocrinology, one neurology and one health and ageing. The comparison (standard care) wards were as follows: two acute medical, two health and ageing and one stroke.
Contemporary interviews
Purposive sampling
We purposively sampled for heterogeneity across the two groups in order to understand how care was perceived and understood among different people with different characteristics. Potential patient participants under the care of a palliative care team were selected according to the following criteria:
AMBER care bundle status
AMBER – supported by the AMBER care bundle (hospitals 1–3) Comparison – would be appropriate for care supported by the AMBER care bundle if they were on an AMBER care bundle ward (hospital 3 only)
Disease
Cancer Non-cancer.
A family member was approached where the patient was too unwell to participate. Potential participants were not approached for the study if they lacked capacity to provide informed consent, were considered too distressed or were too unwell to participate.
Recruitment
Identification and first approach for the study was by the palliative care team (February–June 2013). Participants provided informed consent before commencing the interview with the researcher (K.B.), a sociolinguist with extensive experience of interviewing in palliative care research.
Data collection
The topic guide, shaped by a literature review, explored participants’ experiences of care and involvement in treatment decisions while in hospital, including the following:
Illness history
Reason for admission and recent illness
Patient’s main problems, symptoms and concerns
Whether and how the health-care team have been able to help with these concerns
Information and communication
Clarity of information
Consistency of information
Opportunities to ask questions
How patient or carer concerns were managed
Whether they felt that their concerns were listened to
Involvement in decision making
Involvement in decision about the patient’s care
Opportunities to talk about the future and future care
Unresolved concerns
Experience of care provided
Confidence in the care and treatment provided
Experiences of how different care providers had worked together.
All interviews were audio-recorded and transcribed verbatim. Recruitment continued until data saturation was achieved, and no new themes were emerging from the interviews.
Analysis
All interviews were analysed by K.B. using thematic analysis in five stages: familiarisation, coding, theme development, defining themes and reporting. 25 To address issues of analytical rigour and trustworthiness, a subset of transcripts were double-coded by J.K. A re-iterant process of discussing areas of agreement and disagreement took place between K.B. and J.K. to achieve consensus. Alternative interpretations were incorporated in the analysis. The analysis was further tested during discussions with colleagues and meetings of the project advisory steering group. Attention was also paid to non-confirmatory cases where emerging themes contradicted more common ideas. 26 Comparison was made between the AMBER care bundle and comparison groups for each emergent theme. To preserve anonymity, participants were pseudo-anonymised. Analysis was managed using NVivo qualitative analysis software (Version 10).
Followback survey
Identification
Next of kin (NOK) were identified from electronic patient records (EPRs) for patients who had died within 100 days of discharge following an admission between December 2011 and December 2012. One group had received care supported by the AMBER care bundle; the other was a comparison group. Comparison patients were identified by a hospital consultant and clinical nurse specialist independently examining content of EPR data to identify patients who, all things being equal, would have been appropriate for care supported by the AMBER care bundle if they were on an AMBER care bundle ward. Criteria for selection were deterioration, clinical instability, limited reversibility and being at risk of dying within 1–2 months as available in clinical records.
Recruitment
All identified NOK were sent a letter from the palliative care team 4–10 months following bereavement, with the survey and a Royal College of Psychiatrists bereavement support leaflet. If no response, a second pack was sent 1 month later.
Date collection
We used a modified QUALYCARE postal survey, 27 highly acceptable to participants in bereavement research. 28 This examines the last 1–2 months of the decedent’s life, including quality and consistency of information and communication with clinicians.
Analysis
Analysis compared the groups, in particular questions about communication, information sharing, awareness of illness and length of stay, using independent t-tests and χ2 tests. Statistical significance (two-sided) was set at p < 0.05. For the followback survey, we calculated sample size estimates in relation to variables that were central to understanding to what extent the AMBER care bundle achieved its goals. Therefore, we wanted to detect potential differences in the percentage of respondents unable to gain sufficient information regarding a patient’s condition; distributions from followback surveys varied between 39% and 64%.29,30 With power set at 80% and alpha at 0.05, similarly 69 cases would be required from each group to detect this difference. In order to detect differences in the percentage of patients who knew they were going to die, previous studies have ranged between 51% and 69%.31,32 With power set at 80% and alpha at 0.05, we estimated a minimum of 113 cases would be required from each group to detect a similar difference.
Integration of data
The interview and survey data were integrated at the point of analysis, in a convergent design, interrogating the data around common key themes and questions, 33 as demonstrated through the integrated results presented below.
Results
Participants
Contemporary interviews
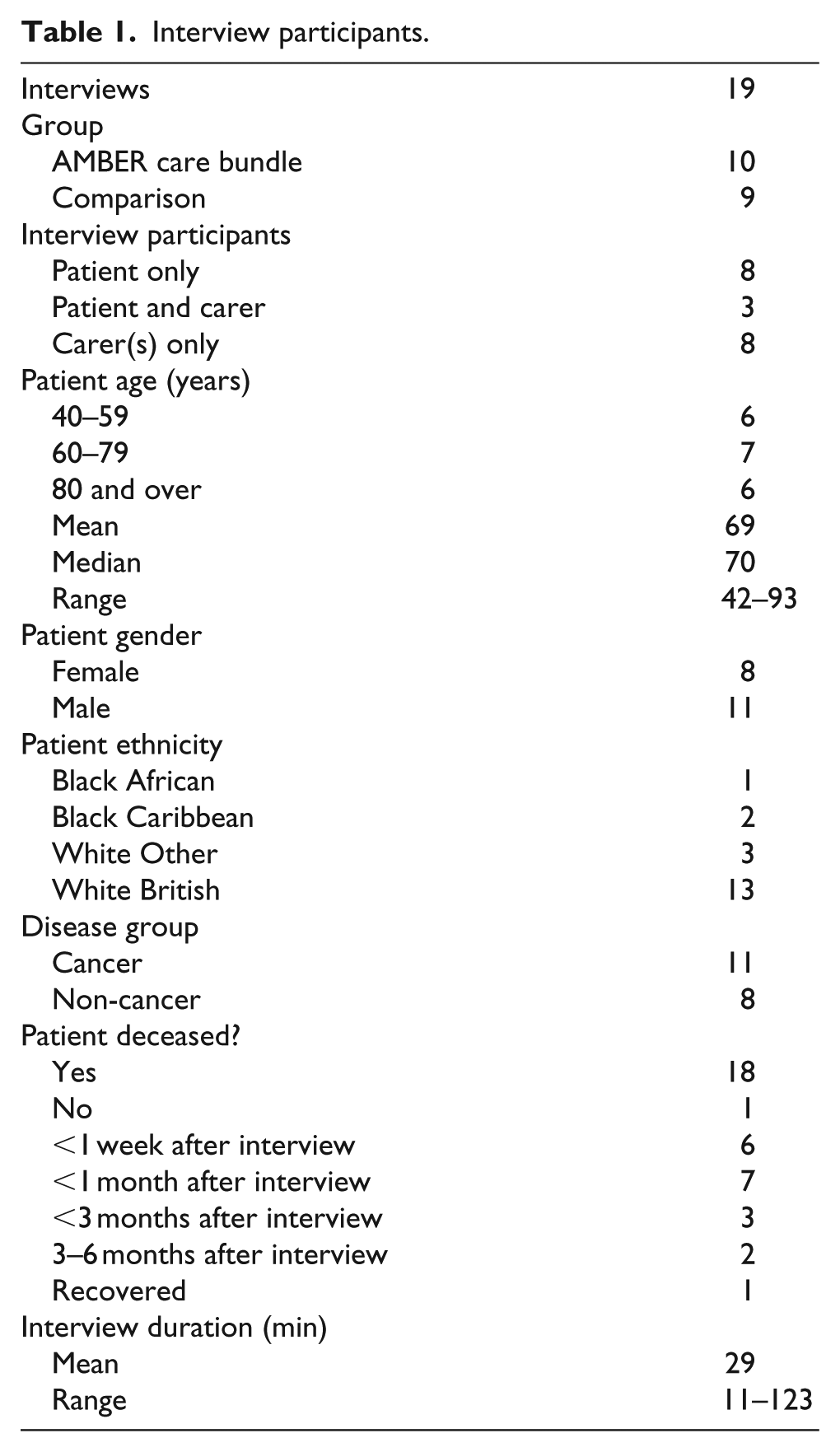
A total of 23 patients and informal carers participated in 19 interviews (Table 1) – 8 interviews with patients only, 3 interviews with patient and carer dyads (patient and partner or spouse), and 8 interviews with carers only (including spouse, mother, brother, son, daughter, daughter in law, and niece), one of which was with two carers together. 10 AMBER care bundle and 9 comparison, where 11 had cancer and 8 non-cancer diagnoses (brain tumour, spinal tumour, dementia, stroke, hip fracture, heart failure, liver failure and kidney failure). Mean interview duration was 29 min (range: 11–123 min).
Interview participants.
Followback survey
A total of 482 surveys were sent to the NOK: 261 deceased patients supported by the AMBER care bundle and 221 who received standard care (Table 2). Overall response rate was 20% (n = 95). Although the response rate differed between the two groups (AMBER care bundle 23% and comparison 16%), this was not statistically significant (χ2 = 3.01, df = 1, p = 0.08).
Followback survey participants.
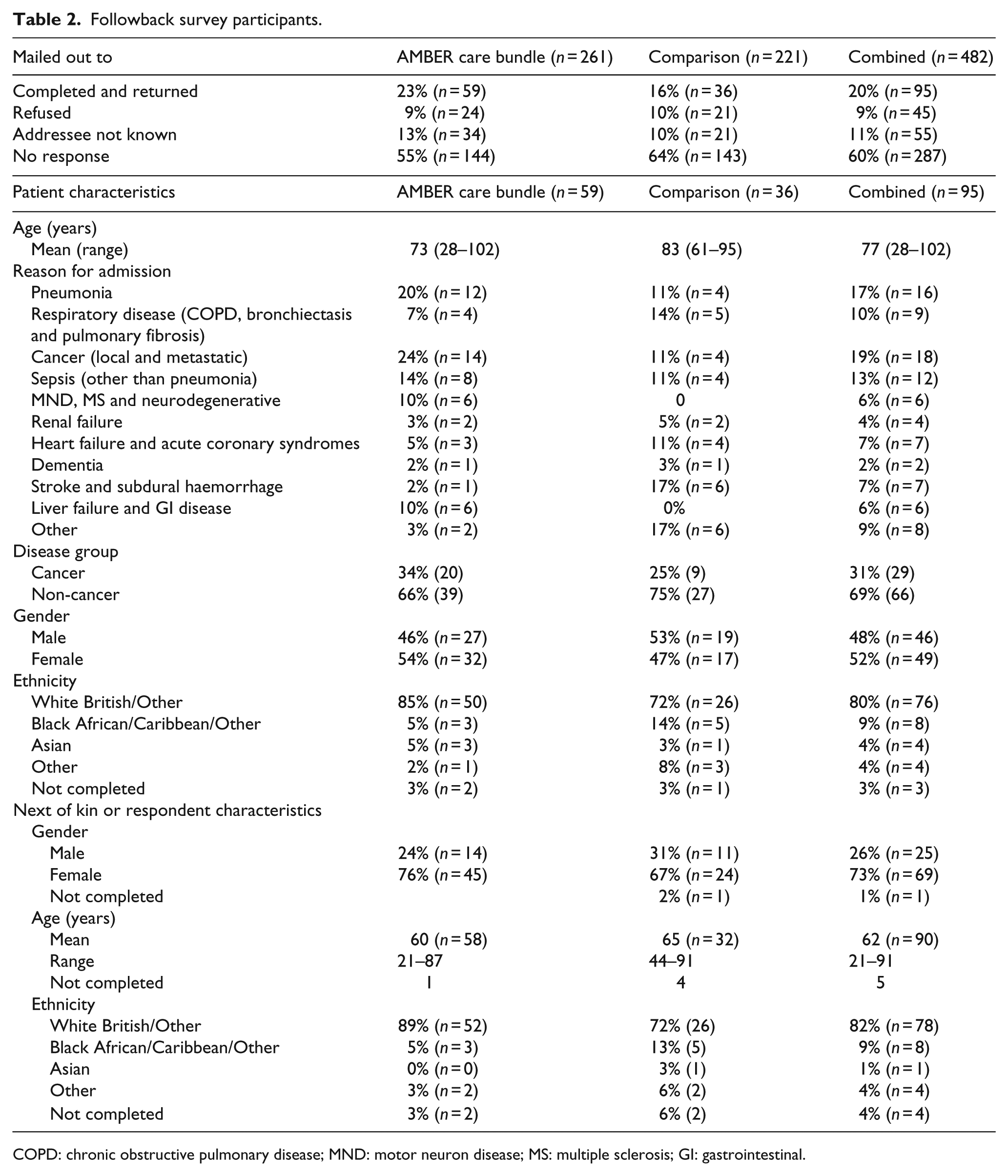
COPD: chronic obstructive pulmonary disease; MND: motor neuron disease; MS: multiple sclerosis; GI: gastrointestinal.
The first section of the results will present the differences between the AMBER care bundle and standard care experiences for patients and carers, and the second section will present the similarities.
1. Exploring the AMBER care bundle and comparison group experiences (survey and interviews) – differences
In both the interviews and survey, differences emerged in the experiences of those in the AMBER care bundle and comparison groups. Specifically, these were related to awareness of the clinical situation and discussion and realisation of preferences for place of care. For each of these, the experiences shared in the followback survey and contemporary interviews are described below.
Awareness of the clinical situation
Followback survey
The AMBER care bundle family meeting is an opportunity to discuss prognosis, preferences, priorities and concerns. Significantly more of the AMBER care bundle group than the comparison group reported that the patient was aware they were going to die from their illness (72% compared to 48%, χ2 = 4.29, p = 0.04; Table 3). Also, significantly more of the AMBER care bundle group recalled a clinician discussing with the patient that they were likely to die from their illness (59% compared to 32%, χ2 = 4.09, p = 0.04; Table 3).
Followback survey results.
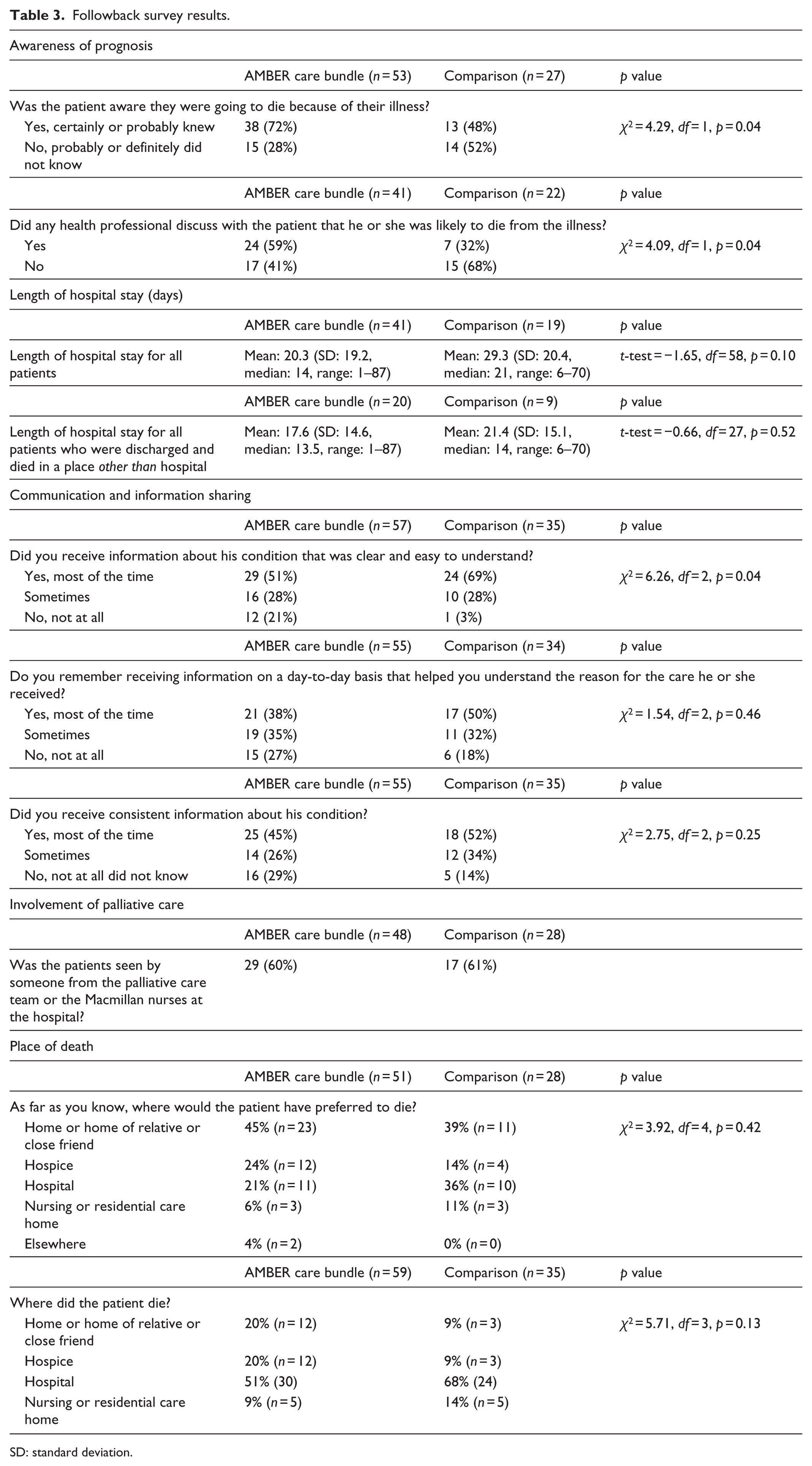
SD: standard deviation.
Contemporary interviews
Carers supported by the AMBER care bundle described clinicians deliberately seeking them out to update them and address concerns, which represented a source of enormous support: one of the doctors actually rung me from home at nine o clock at night once because she realised she’d forgotten or hadn’t had a chance to come and see me so that was … was really nice and that was much appreciated. (Cheryl, daughter of a man with lung cancer – AMBER)
Further differences were evident in the contemporary interviews. Although both groups reported difficulties with inconsistent information, for those supported by the AMBER care bundle, incomplete or inconsistent information was often described in the context of rapidly changing clinical situations, as a cause of clinical uncertainty, as illustrated below (emphasis added): As I say it’s just … not knowing exactly like, that’s the only thing that bothers me … they can’t predict … but I know he is getting weaker. (Mary, wife of man with heart failure – AMBER)
Contrastingly, participants in the comparison interviews tended to report uncertainty as a result of the clinicians’ ‘assumptions’, due to their inadequate or incomplete knowledge, suggesting that perhaps the clinical uncertainty had not been fully explained (emphasis added): They come in everyday … the only question I’ve got and they can’t answer is exactly how long have I got … they don’t know … it’s all assumption. (Martin, man with bladder cancer – Comparison)
These differences suggest those supported by the AMBER care bundle may have more of an understanding of the clinical uncertainty and its resultant impact upon clinicians’ ability to provide consistent and complete information.
Discussion and realisation of preferences for place of care
Followback survey
Length of hospital stay was not significantly different between the groups: AMBER care bundle group mean hospital stay 20.3 days (range: 1–87 days) and comparison group 29.3 days (range: 6–70 days; Table 3). Broadly, similar proportions of patients cared for on AMBER care bundle wards (45%, n = 23/51) and the comparison group (39%, n = 11/28) were known to have preferred a home death. However, the numbers of AMBER (20%, n = 12/59) and comparison group (8%, n = 3/35) patients who did so (or the home of a relative or friend) differed, although this difference was not statistically significant.
Contemporary interviews
Concerns of caring for a relative at home were more evident among those supported by the AMBER care bundle than the comparison group, including feeling unprepared practically and emotionally for the experience, questioning whether they would cope and facing the physical reality of death of a relative at home. Although preferred place of care was elicited and potentially expedited, concerns regarding discharge were not addressed drawing into question the quality of the discussions: Even now we’re still having conversations about … are you going to go home and … although he wants to I don’t think that it’s perhaps the best place and I don’t think that he really thinks that it’s the best place … from a practical point of view … so I guess maybe you know if someone had said … actually … have you really thought about the implications of this … might have been useful … um at the time when he was saying yes I want to go home. (Cheryl, daughter of a man with stomach cancer – AMBER)
These unresolved concerns were also found in the followback survey free-text entries (Table 4).
Followback survey free-text comments.
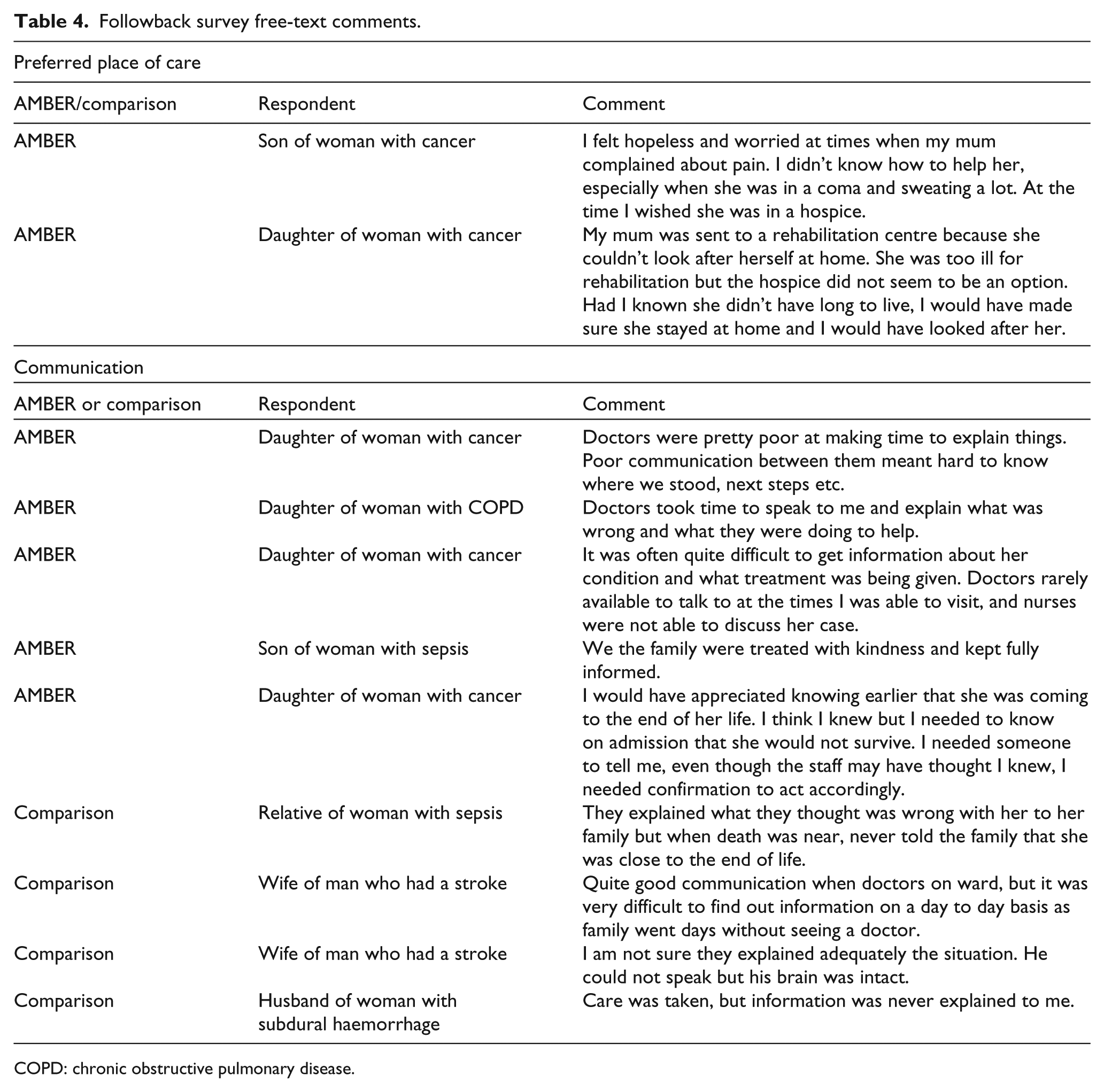
COPD: chronic obstructive pulmonary disease.
2. Communication concerns (survey and interviews) – similarities
There were also some similarities to the experiences shared by the two groups. Both those supported by the AMBER care bundle and the comparison group described challenges when communicating with clinicians. Concerns were related to the actual information shared and the process of information sharing. For each of these, the experiences shared in the followback survey and contemporary interviews are described below.
Information shared
Followback survey
Respondents from the AMBER care bundle group were less likely than the comparison group to report that information was clear and easy to understand (69% vs 51%, χ = 6.26, p = 0.04). However, there were no differences in frequency or consistency of communication with clinicians between the groups (Table 3).
Contemporary interviews
The impact of inconsistent information was also described by interview participants, often in very emotive terms: We were told on a Sunday evening at seven … that … we need to make preparations to get John either to our local hospital … or indeed home because there’s nothing more that can be done for him … and then on the Monday morning to arrive and be told by his consultant that … John’s doing remarkably well … and there’s no reason that within a couple of months he shouldn’t be back up and on his feet … the emotional trauma for you … for all of us. (Tom, brother of man with spinal tumour – Comparison)
Process of information sharing
Concerns were also raised, regarding the process of information sharing with the clinicians.
Followback survey
Respondents shared positive experiences of communication with clinicians but also feelings of abandonment at evenings and weekends. Few doctors were present to talk to, as described in the survey free-text entries (Table 4).
Contemporary interviews
Participants described the need for a single point of contact to provide continuity and avoid unnecessary confusion. Participants also described insensitivity in the manner information was shared. Several evidently distressing experiences were described in both groups: The doctor told me we are in a situation of diminishing returns and ought to let nature take its course … this was so blunt … I couldn’t sleep for two days. (Devan, man with lung cancer – AMBER)
Discussion
This first comparative evaluation of the AMBER care bundle found that it may be associated with increased frequency of discussions about prognosis with patients and families and improved awareness of the clinical situation. However, there were no significant differences in length of hospital stay, satisfaction with communication, or frequency and clarity of information shared.
The AMBER care bundle appeared to enable more of an understanding of the reasons underlying clinical uncertainty, increased awareness of the clinical situation and increased frequency of discussions about prognosis. However, clarity of information sharing was worse among the AMBER care bundle group than the comparison group. The use of other approaches such as proactive elderly advance care planning tools on comparison wards may have affected this. It is possible that while discussions took place among the AMBER care bundle group, the information was not communicated effectively due to lack of skills in communicating the complexity of clinical uncertainty and prognostication or increased complexity of discussions among this group with more information being shared, resulting in possible confusion. Inadequate explanation of clinical uncertainty has been found to negatively affect patient and carer experiences, 13 and poor communication can be detrimental to patient experiences and understanding of prognosis, results and treatment plans. 34 The findings from this study suggest that without appropriate support and training, alongside the AMBER care bundle, communication of information may remain unsatisfactory.
The AMBER care bundle appeared to enable more of an understanding of the reasons underlying clinical uncertainty, increased awareness of the clinical situation and increased frequency of discussions about prognosis. However, clarity of information sharing was worse among the AMBER care bundle group than the comparison group. The use of other approaches such as proactive elderly advance care planning tools on comparison wards may have affected this. It is possible that while discussions took place among the AMBER care bundle group, the information was not communicated effectively due to lack of skills in communicating the complexity of clinical uncertainty and prognostication or increased complexity of discussions among this group with more information being shared, resulting in possible confusion. Inadequate explanation of clinical uncertainty has been found to negatively affect patient and carer experiences, 13 and poor communication can be detrimental to patient experiences and understanding of prognosis, results and treatment plans. 34 The findings from this study suggest that without appropriate support and training, alongside the AMBER care bundle, communication of information may remain unsatisfactory.
Those supported by the AMBER care bundle also volunteered more concerns about the reality of ‘going home’ than the comparison group. While discussions regarding preferred place of care had occurred, there were many unresolved concerns around leaving the security of the hospital, how they would cope at home and the support that would be available. One potential criticism of the AMBER care bundle is the lack of emphasis on exploring patient and family information preferences before initiating discussions. Clinicians are poor at estimating the information and decision making preferences of patients and carers.35–37 Also, patient and carer preferences often differ, and carers are poor at predicting the information preferences of patients. 38 Further communication training should accompany the AMBER care bundle, particularly in light of recent criticism of communication in the acute hospital setting,14,15 to ensure discussions are individually tailored accommodating patients’ and carers’ preferences for information and discussions.
Strengths and limitations
This study represents the first attempt to evaluate the AMBER care bundle in the acute hospital setting and has important strengths. The integration of the qualitative and quantitative data enabled the researchers to ask intersecting questions, facilitating a more complete exploration of care supported by the AMBER care bundle. Also, this study involved meaningful engagement with a hard-to-reach population who were clinically unstable, deteriorating, with limited reversibility and at risk of dying in the next 1–2 months. Over half of the patients interviewed died within 1 month of participating, and many within days, providing invaluable insights into experiences at such a challenging time.
However, the study has limitations. First, the design was observational. Although there was a comparative element, the comparison and AMBER care bundle groups were likely to be different in ways other than the intervention. Second, while this study was primarily exploratory, based on our sample size calculations, we failed to recruit sufficient numbers to detect other potential important differences – the response rate being considered as a marker of success. The EPR data from which we identified the participants for the followback survey were sometimes of poor quality; some addresses were redundant or the NOK was deceased making it impossible to identify an appropriate proxy. This was a particular problem for the comparison group, which had a very poor response rate. This not only raised general concerns for hospitals about the veracity of their data but also reduced the potential number of respondents and will also have biased the comparison group.
Third, the followback survey relies on ‘proxy’ experiences of bereaved caregivers rather than patient-centred accounts. While the validity of proxy accounts has been questioned,39,40 this approach is often employed27,32,41 to overcome difficulties of obtaining views of representative samples of patients. Many studies relying on patients’ accounts prior to death are potentially biased since they represent only a small proportion of patients with an identifiable terminal illness, who are relatively well and therefore able to participate, and are willing to take part. Fourth, the choice and matching of comparison wards were challenging, and it was not possible to control for other interventions which may have altered care. In particular, many patients were supported by a palliative care team, and this may have influenced the care provided.
Conclusion
This study found some potential benefits to care supported by the AMBER care bundle, in particular in terms of levels of knowledge of patients and caregivers. However, it also identified potential downsides, specifically concerning information and communication including about going home. This highlights the importance of ensuring adequate training when implementing the AMBER care bundle. Our study was small and may have been inadequately powered to detect other differences. Our data point to a need for robust sufficiently powered comparative evaluation of the AMBER care bundle and other similar tools and complex interventions utilised towards the end of life, including of potential benefits and harms. The findings also suggest that additional communication training is vital, as both groups in this study reported negative experiences.
Footnotes
Acknowledgements
We wish to thank the patients and informal carers who participated in this study. We also thank Jane Lewington, Natasha Lovell, Catherine Gwilt and Jennifer Karno for their support in this study.
Approvals
Ethical and research governance approvals were obtained (London Dulwich NRES Ref:12/LO/0043).
Declaration of conflicting interests
None declared.
Funding
This study was funded by the Guy’s and St Thomas’ Charity, UK. The funders had no role in the interpretation of the results.