
Abstract
Background:
Achieving home care and home death is increasingly used as an outcome measure of palliative care services.
Aim:
To appraise the state of the science on dying at home.
Methods:
Appraisal and narrative review developed from a plenary presentation at the European Association for Palliative Care (EAPC) 2012 meeting examining the research on variations and trends in place of death, factors associated with dying in the preferred place, presenting evidence on outcomes for those dying at home and suggesting future research questions.
Results:
Meeting patients’ preferences and creating home-like environments has been a major concern for hospice and palliative care since its inception. During the 20th century, in many countries, hospital deaths increased and home deaths reduced. Despite the fact that this trend has been halted or reversed in some countries (notably the United States, Canada and, more recently, the United Kingdom) in the last 5–20 years, a home death is still a distant reality for the majority, even though evidence shows it is the most commonly preferred place to die. Epidemiological studies identified factors associated with home death, including affluence, patients’ preferences, provision of home care and extended family support. Evidence about the benefits of home care is conflicting, but recent data suggest that holistic well-being may be greater at home.
Implications:
We call for further analyses of variations in place of care and place of death and robust studies on how patients and families formulate and change preferences over time. Regular monitoring of outcomes, quality and costs of palliative home care is urged.
Introduction
The place where we spend the most important moments of our lives is a relevant issue to all of us. For instance, the debate about home versus hospital birth has been fuelled by observational studies, which suggest that planned home birth in many places can be as safe as planned hospital birth, and with fewer interventions and complications. 1 Equally, place of death has been of growing interest in palliative and end-of-life care. There are several reasons for this. There is an international move to reduce hospital stays, to increase community support on the grounds of reducing iatrogenic disease, hospital-acquired infection, health-care costs and inappropriate lengthy hospital admissions and to more closely meet patient and family choice. In turn, meeting patients’ and families’ preferences has been gaining relevance in the last years due to the increased recognition for the need to empower patients and families (with advanced care planning for instance) and to support patients with chronic non-malignant diseases. 2
Alongside these general trends, striving for a home or ‘home like’ environment has always been an important part of palliative care. In the United Kingdom, Dr Cicely Saunders 3 developed inpatient hospices as an alternative to hospitals, where the hospice staff are the ‘hosts’ to patients and their families and provide a more home-like environment. Soon after, she and her colleague Dr Mary Baines recognised the need to feed the principles back to the patients’ own homes.4,5 There was a drive in the United Kingdom and Italy to find ways to offer treatments for complex problems, which had usually required hospitalisation, such as intestinal obstruction, and studies showed that obstruction could be managed out of hospitals and in an inpatient hospice or at home with good patient quality of life.6,7 In the United States, from the outset, hospices had a strong emphasis on home care and on patients spending the majority of their time at home and/or dying at home.8–10
Nowadays, this debate is increasingly relevant for all palliative care stakeholders and constitutes a public health issue due to the rising numbers of deaths and increasing health expenditure. Evidence from systematic reviews suggests home palliative care results in higher caregivers’ and patients’ satisfaction,11,12 reduced length of stay in hospitals 11 and greater odds of dying at home.13,14 However, work is still needed to understand which components of the intervention provide the highest benefit.11,15
Variations and trends in place of death: international, national and local
Many outcomes (e.g. morbidity and mortality) vary by socio-economic status, and therefore, early research in this field examined whether home death could be similarly influenced. Clinicians working in community palliative care teams witness the value that patients and families place on being at home. It is a familiar environment where they maintain control and greater freedom than in hospital or even inpatient hospice.
This led to a preliminary investigation of the variation in home deaths for people who died from cancer. Higginson et al. 16 studied the 5-year average proportion of home deaths in 44 electoral wards (voting districts with a population of 3819–11,350) in one London district. The most striking finding was the degree of variation. In one electoral ward, 5% of cancer deaths were at home, and in another, 46% were at home. There was an inverse correlation between home death and social deprivation, as assessed by underprivileged area score – an index of 8 aspects of affluence or not (Spearman Rho = −0.63 (95% confidence interval (CI): −0.44 to −0.79)), so that in poorer areas, fewer cancer patients died at home, but this did not explain all the variation.
The degree of social variation in the part of London where the study was conducted was large – ranging from the so called ‘boulevard of billionaires’ in Kensington to the highly socially deprived areas in northwest London. However, subsequent whole population research confirmed the high level of variation (from <10% to >65% in England) and the inverse relationship between social deprivation and home cancer death.17,18 The project disseminated to each district in the United Kingdom their individual data on place of death to raise awareness of the issues. The degree of inequity was supported internationally by the research of Pritchard et al., 19 Weitzen et al. 20 and Mitchell et al.,19–21 which was simultaneously studying variation in the United States using the Brown Atlas and empirical studies, and by the study of Costantini et al. 22 in Genoa, Italy.
Finding information on real-time variation in place of death by local authority (which includes several electoral wards) in England is now made possible by the work of Dr Julia Verne and colleagues at the South West Public Health Observatory (SWPHO). English areas can immediately and freely find information on the proportion of home, hospital or hospice deaths, how they compare with other areas in England or within their region, plus much other demographic information, via the new UK End of Life Care Intelligence Network (http://www.endoflifecare-intelligence.org.uk), a national collaboration created and supported by the UK End of Life Care Strategy.
During the 1990s and 2000s, home death proportions increased in Canada and the United States, while they fell in much of Europe. Between 1994 and 2004, the proportion of hospital deaths in Canada fell from 77.7% to 60.6%, while home death proportions increased from 19.3% to 29.5%. 23 In the United States, the percentage of Americans dying as hospital inpatients decreased from 54% to 41% between 1980 and 1998. 24 The US Hospice Care Benefit was introduced in 1982 and may have influenced this shift. 25 Disappointingly, for the United Kingdom, during the period 1984–1999, despite the growth in palliative care and hospice services, there was no change in the proportion of home cancer deaths, and the gap between poor and rich areas remained unchanged. 18 A subsequent analysis from 1974 to 2003 also showed an overall slow steady fall in home deaths, with home death proportions falling fastest in the oldest age groups and among non-cancer patients. 26 However, because of encouragement to the UK End of Life Care Strategy introduced in 2004, since 2005, there has been a small increase in home cancer deaths (from 22.1% to 27.3%) and home non-cancer deaths (from 16.7% to 18.2%). Population-based data also found home death increases in some regions of Europe – for example, in Genoa (Italy), a home palliative care team appeared to have increased home deaths.22,27
National policies introduced in other European countries may now help to improve palliative care for patients and families and allow care and dying in the place of choice. These include the following: the German 2007 Law for provision of specialist outpatient palliative care; 28 the Belgian 1998 Law of one home care team with two nurses and one doctor for 100 patients or per 300,000 inhabitants; 29 the French 2002 national palliative care programme to establish palliative home care, palliative care units and campaign to raise awareness among population; 29 and the Italian 2010 Law of continuity between hospice and home care. 30 Considerable international variations exist in place of death from cancer, but this is harder to interpret than within country variations because of many differences in national policies, coding systems and cultural expectations.31,32
What do people actually want?
Many studies have researched preferences for both place of care and place of death in cancer in different populations and contexts and with different questions. Place of care and place of death are not the same, but preferences are associated. Asking the question in different ways (where do you think you would be best cared for or where would you ideally like to be) gives different responses. Therefore, research in this field needs to develop consistent methods. For place of death, there is consistent evidence across many studies that home is the main preference (25%–87% favouring home deaths, depending on whether the question was asked to patients, caregivers or general population), 33 and in many studies, this is followed by a preference for inpatient hospice (9%–30%). Hospital and nursing homes have lower preferences. 34 Robust international population-based evidence now comes from the PRISMA (Reflecting the Positive diveRsities of European prIorities for reSearch and Measurement in end of life cAre) survey of 9344 citizens across seven European countries, where home preference ranged from 51% (Portugal) to 84% (Netherlands) and hospice preference from 9% (Flanders) to 29% (England). 35 Longitudinal studies of place of death preferences in patients approaching the end of life have shown that some patients shift their preference, away from home and towards inpatient hospice or other inpatient setting. Nonetheless, even in these studies, home remained the preference for the majority,36,37 with some variation probably due to how the question was asked. Recent work has suggested that for many, preferences are stable. 38 There are differences in preferences among different groups – for example, among older people or those with different cultures. However, this should not be assumed, as preferences among UK cancer patients from the Black Caribbean culture were found to be similar to those from White patients. 39
It is also worth considering what a preference means and how it is formed. A preference will be affected by prior experiences (good and bad), those of friends and recent experiences of how services have worked, as well as the patient’s condition and the views of family and friends. A shift in preference may be influenced by, for example, care at home breaking down or failing, particularly good (or poor) experiences in hospital or inpatient hospice, physical symptoms or perception of family burden. The reasons for change in preferences are currently poorly studied and need further research.33,34
Furthermore, there are different forms of preference. In a longitudinal study, Townsend et al. 37 distinguished between a preference in ‘ideal’ circumstances and one in ‘existing circumstances’. Over time, these two forms of preferences diverged, the proportion of patients who stated a preference for home death given ‘existing circumstances’ fell from 59% to 48%, and the preference in ideal circumstances for home death increased from 67% to 70%. If preferences in ‘ideal’ and ‘existing’ circumstances are different, then it would be valuable to understand the gap and the reasons for this. Moreover, preferences may exist along a continuum 40 rather than being one choice versus a diametrically opposed choice. It may be helpful to understand more about the interplay of different factors influencing preferences and how they change over time. Figure 1 illustrates three possible preference trajectories assuming that the preference in ideal circumstances remains stable and there is always a gap between ideal and existing circumstances.
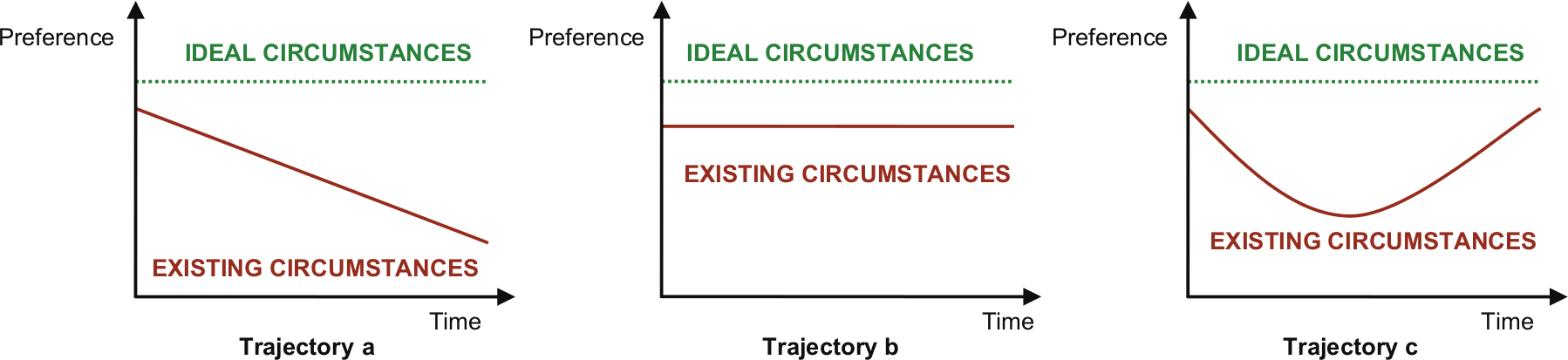
Three possible preference trajectories for place of care or death: preference of desired place of care or death; preference in ideal circumstances, for example, ‘Where would you like to be cared for or to die if it was possible?’ and preference in existing circumstances, for example, ‘Given your current circumstances and arrangements, where would you like to be cared for or die?’
In trajectory a in Figure 1, the gap increases because the preference decreases with time ‘given existing circumstances’. In trajectory b, a small gap is maintained at a constant level because existing circumstances remained stable. In trajectory c, the gap fluctuates due to changes in existing circumstances. These models do not comprehensively represent all possible preference trajectories, but they highlight the importance of understanding the dynamics of the processes that determine preferences. The gap between ideal and existing circumstances might help explain why patients change their minds and sometimes express different preferences for place of care and place of death. Understanding reasons for the gap would allow health-care providers to identify potentially changeable factors that could approximate ideal and existing circumstances. In a longitudinal study, Thomas et al. 40 identified four thematic domains of factors influencing preferences for place of death: the informal care resource, management of the body, experience of services and existential perspectives. These findings need to be appraised in larger samples and other settings.
What factors are associated with home care and home death?
Inequities continue to exist in place of death. Those from lower socio-economic groups or living in poorer areas are less likely to die at home.13,41,42 Culture and ethnicity affect place of death. Analysis of data from 68,804 patients resident in South East England, who died of cancer, found that following adjustment for confounders, death in a hospice was significantly less likely for Pakistani patients (odds ratio (OR) = 0.47, 95% CI = 0.30–0.74), Indian patients (OR = 0.68, 95% CI = 0.55–0.84) and Bangladeshi patients (OR = 0.33, 95% CI = 0.19–0.56). Furthermore, death at home was significantly less likely in Black African patients (OR = 0.48, 95% CI = 0.36–0.65), Black Caribbean patients (OR = 0.78, 95% CI = 0.67–0.90) and Chinese patients (OR = 0.46, 95% CI = 0.28–0.76). Pakistani, Indian, Bangladeshi, Black African, Black Caribbean and Chinese patients were all significantly more likely than White patients to die in hospital. 43 People living in metropolitan areas are less likely to die at home.44,45 The relationship between age and place of death is more complex. In the United Kingdom and many countries, older people with cancer are less likely to die at home and in inpatient hospices. 46 Indeed, in the United Kingdom, hospital is the most common place of death up to the age of 90 years when nursing home takes over. 46 Diversely, in New York and in Singapore, home deaths increase with age.41,47
In order to enable more cancer patients to die at home and to tackle inequities, an understanding of the factors associated with death at home is required. Despite the predominance of a preference to die at home and increases in cancer home deaths in Canada, the United Kingdom and the United States, a home death is still far from being a reality for the majority of people dying of cancer in these and other countries.23,24,32,35,48 A conceptual model developed in 2006 continues to find empirical support from many different studies. 13 The model grouped risk factors into those related to the illness, the individual and the environment, the latter being the most important group in influencing death at home. Through systematic review, the authors found high-strength evidence for the effect of 17 factors, of which six were strongly associated with home death: patient’s low functional status (adjusted OR (AOR) = 2.29–11.1), their preferences (AOR = 2.19–5.47), home care (AOR = 1.37–5.1) and its intensity (AOR = 1.06–8.65), living with relatives (AOR = 1.78–7.85) and extended family support (AOR = 2.28–5.47). New evidence from recent systematic reviews suggests that home palliative care services also increase the odds of home death, compared to usual care.14,49 The model now requires greater testing, ideally comparing the relative contribution of factors in single studies. Social conditions, preferences and home care are factors that must also be better understood.
Is home care or home death better than other places – for example, the hospital?
Understanding whether people’s experiences of the dying process and its outcomes differ by place of death is vital. We still do not know whether dying at home is better than dying in hospital for patients and families. There is some evidence suggesting that psychological, social and holistic measures of the patient’s well-being in the last weeks or days of life may be better for patients dying at home.50–53 However, the findings regarding symptoms and family outcomes are not consistent enough to support that dying at home is better, worse or similar to dying in institutional settings.
The evidence is particularly disparate for the two most researched outcomes: pain and grief. Since Parkes’ 54 study in 1967–1971 in London, studies have been showing conflicting findings. Seven more recent studies showed inconsistencies in what was considered a ‘home death’, in the measurement of pain and in the groups compared.50,54–60 This highlights the need for greater clarity and consistency in measurement and patient selection.
There is divergence also regarding the experience of death at home on the family. Using UK data from the Regional Study of Care of the Dying (RSCD) in 1990 on four grief-related binary questions, Addington-Hall and Karlsen 61 reported greater grief when death took place at home. Quite the opposite, the US longitudinal study Coping with Cancer (2002–2008) found that relatives of patients who died in hospital were more likely to develop a prolonged grief disorder 6 months after (assessed using the validated Prolonged Grief Disorder Scale), than those who experienced a death at home with hospice care (AOR = 8.83, 95% CI = 1.512–51.77, adjusted for baseline pre-loss grief). 51 Differences between home deaths with and without hospice care and intensive care unit deaths did not reach statistical significance. None of five other studies (all but one conducted with relatives of patients who received palliative care) found associations between grief and place of death, four of which used the Texas Revised Inventory of Grief (TRIG).51,61–66 There remains a lack of population-based studies, which adjust for prior relationship, and a need for new evidence to clarify this.
Implications for the future of research in this field
Data on place of death are easily accessed in many countries, making this a useful and practical outcome that can be compared cross-nationally and across regions within the same country. Epidemiological analyses have shown that information on place of death is valuable for planning service provision, detecting regional or other inequities and changing trends. Therefore, the continued monitoring of place of death can support evidence-based decisions about health-care development and organisation, by uncovering emergent population needs and facilitating the comparison between different regions.
Alongside these epidemiological analyses, we also need information about patient and caregiver outcomes, the extent to which individual preferences are met and the quality of care and death, which is the ultimate quality indicator. Such data will be vital in recording how place, outcomes, experience, quality and costs are related. One means to achieve this would be to put in place routine monitoring, in practice, of patients’ experiences and outcomes. Retrospective surveys are helpful but rely on the relatives’ views; these may be especially prone to recall bias regarding prior preferences for place of death. The Qualycare questionnaire and the Toolkit of Instruments to Measure End-of-life Care (TIME) are two examples of retrospective questionnaires that can be used to assess the quality of care and death. Prospective measurement of quality and outcomes are needed, using brief validated transferable measures such as the Palliative Care Outcome Scale or Edmonton Symptom Assessment System,67,68 perhaps incorporated into monitoring systems similar to the Australian Palliative Care Outcomes Initiative. 69
A better understanding of the factors influencing preferences for place of care and death, including age, culture, social conditions or previous care experiences, could inform the model of factors affecting place of death and contribute to the development of responsive palliative care services and clinical practice. Understanding the evolution of the gap between preferences in ‘ideal’ and ‘existing’ circumstances and also how previous experiences influence these would help build evidence on the importance and meaning of preferences. Questions to assess preferences should be carefully chosen and piloted whenever possible. Further studies assessing preferences in ideal and existing circumstances, building on those of Townsend and other, would be valuable.
Limitations of this narrative review
According to Mays et al., 70 narrative reviews ‘summarize, explain and interpret evidence on a particular topic/question’, dealing with studies’ findings and interpretations without attempting to synthesize them, with a less systematic and explicit approach, allowing for different types of evidence to be reviewed without generating completely new theories. This is the case here where we aimed to consider the state of the science and how the studies evolved over time to lead to current knowledge. It is possible that we have missed some aspects, which might have been detected in a systematic review. However, systematic reviews tend to ask specific questions and are not suited for providing an overview of a topic or field.
Conclusion
Since the early stages of the modern hospice movement, there has been an awareness of the great value patients and families place on being at home. Epidemiological studies show that trends of increasing hospital deaths are changing in some countries, but death at home is still not a reality for the majority and large variations remain. Preferences for place of care and death show that home is the main preference, followed by hospice, but there is a need for a greater understanding of factors underlying change of preferences and how often or why these change over time. Factors influencing home death suggest that inequities and unmet needs in this setting still exist. Ensuring the best palliative care in all settings is essential, but in order to meet people’s preferences, investment should focus on services that make a difference, such as home palliative care services. Measures to support family carers should be implemented, and more data are needed on cost-effectiveness of care, especially palliative home care. Measuring outcomes prospectively is important to capture experiences, alongside the more easily measurable place of death.
Footnotes
Acknowledgements
We thank Cicely Saunders International for hosting and funding much of the work presented.
Declaration of conflicting interests
No funder was involved in the article production or content, and the views are those of the authors and not any of the funding bodies. The authors declare that there is no conflict of interest.
Funding
The plenary that originated this article included data from studies and reports funded by the Department of Health, London Health Authority, Cicely Saunders International, the UK National Institute for Health Research (NIHR), the European Commission’s 7th Framework Programme and the Calouste Gulbenkian Foundation, to whom we are most grateful. The PRISMA project was funded by the European Commission’s Seventh Framework Programme [contract number: Health-F2-2008-201655] with the overall aim to co-ordinate high-quality international research into EoLC in cancer. PRISMA aimed to provide evidence and guidance on best practice to ensure that research can measure and improve outcomes for patients and families. PRISMA activities aimed to reflect the preferences and cultural diversities of citizens, the clinical priorities of clinicians, and appropriately measure multidimensional outcomes across settings where EoLC is delivered. Principal Investigator: Richard Harding. Scientific Director: Irene J Higginson. Other PRISMA members: Gwenda Albers, Barbara Antunes, Ana Barros Pinto, Claudia Bausewein, Dorothee Bechinger-English, Hamid Benalia, Emma Bennett, Lucy Bradley, Lucas Ceulemans, Barbara A Daveson, Luc Deliens, Noël Derycke, Martine de Vlieger, Let Dillen, Julia Downing, Michael Echteld, Natalie Evans, Dagny Faksvåg Haugen, Nancy Gikaara, Barbara Gomes, Marjolein Gysels, Sue Hall, Stein Kaasa, Jonathan Koffman, Pedro Lopes Ferreira, Arantza Menaca, Johan Menten, Natalia Monteiro Calanzani, Fliss Murtagh, Bregje Onwuteaka-Philipsen, Roeline Pasman, Francesca Pettenati, Robert Pool, Richard A. Powell, Miel Ribbe, Katrin Sigurdardottir, Steffen Simon, Franco Toscani, Bart Van den Eynden, Paul Vanden Berghe, Trudie van Iersel. The project DINAMO is funded by the Calouste Gulbenkian Foundation with the aim of enhancing advanced training and research to optimize home palliative care in Portugal. Principal Investigator: Barbara Gomes. Scientific Director: Irene J Higginson. Other members of DINAMO: Pedro L. Ferreira, Vera P. Sarmento, Helder Aguiar, Ana Lacerda.