
Abstract
Background:
Although communicating effectively with patients receiving palliative care can be difficult, it may contribute to maintaining or enhancing patients’ quality of life. Little is known about the effect of training general practitioners in palliative care–specific communication. We hypothesized that palliative care patients of general practitioners exposed to the ‘Availability, Current issues and Anticipation’ communication training programme would report better outcomes than patients of control general practitioners.
Aim:
To evaluate the effectiveness of the Availability, Current issues and Anticipation training programme for general practitioners on patient-reported outcomes.
Design:
In a controlled trial, general practitioners followed the Availability, Current issues and Anticipation programme or were part of the control group. Patients receiving palliative care of participating general practitioners completed the Palliative Care Outcome Scale, the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 15 Palliative, the Rest & Peace Scale, the Patient Satisfaction Questionnaire–III and the Availability, Current issues and Anticipation Scale, at baseline and 12 months follow-up. We analysed differences between groups using linear mixed models. Trial registration: ISRCTN56722368.
Setting/participants:
General practitioners who attended a 2-year Palliative Care Training Course in the Netherlands.
Results:
Questionnaire data were available for 145 patients (89 in intervention and 56 in control group). We found no significant differences over time between the intervention and control groups in any of the five outcome measures. Ceiling effects were observed for the Rest & Peace Scale, Patient Satisfaction Questionnaire–III and Availability, Current issues and Anticipation Scale.
Conclusion:
General practitioner participation in the Availability, Current issues and Anticipation training programme did not have a measurable effect on any of the outcomes investigated. Patients reported high levels of satisfaction with general practitioner care, regardless of group assignment. Future research might focus on general practitioners without special interest in palliative care.
Keywords
Effective doctor–patient communication is widely accepted as an essential requirement for providing high-quality care.
Little is known about the effect of training general practitioners (GPs) in palliative care–specific communication.
In our controlled trial, we found no effects of the Availability, Current issues and Anticipation (ACA) training programme for GPs on any of our patient-reported outcomes (the Palliative Care Outcome Scale, the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 15 Palliative (EORTC QLQ-C15-PAL), the Rest & Peace Scale, the Patient Satisfaction Questionnaire–III (PSQ-III) and the ACA scale).
While most items showed near-ceiling scores in all groups, lower scores were observed for the following end-of-life issues in the ACA list: unfinished business, prognosis and possible complications, the actual process of dying, and end-of-life decisions.
Future training programmes such as the ACA programme should focus particularly on the issues that scored low in our trial.
Future research on GP communication skills training programmes in the palliative care setting should include a broad variety of GPs, including GPs who have less specific interest in palliative care issues.
Future efforts should be devoted to developing appropriate and effective training programmes in other countries than the Netherlands as well.
Introduction
While effective communication between health care professionals and patients is considered to be an essential requirement for providing high-quality care,1–6 communicating with patients receiving palliative care has been acknowledged to be more difficult than communicating with patients with less serious conditions. 7 Communication in palliative care involves addressing a complex mix of physical, psychosocial and spiritual/existential issues within the context of impending death. If a health care professional does not communicate skilfully, some, if not many, of the problems that patients are facing may not be identified and addressed, and the patient’s quality of life may be unnecessarily impaired. The results of our previous qualitative study suggest that the quality of general practitioner (GP)–patient communication in palliative care could be improved. 8
Earlier studies on communication skills training in cancer care among medical specialists and oncology nurses demonstrated moderate effects of training on communication behaviour, but little if any effects on patient-reported outcomes.9–20 To our knowledge, no such studies among GPs have been published. 21 To fill this gap, we designed a palliative care communication training programme for GPs, based on the results of recent studies on educational interventions in palliative care and on essential elements of GP–patient communication in palliative care.8,17,21–23 This training programme focuses on availability of the GP to the patient, current issues the GP should discuss with the patient and anticipation of various scenarios by the GP (Availability, Current issues and Anticipation (ACA)). In an earlier article, we reported on the effects of this programme on GPs’ competence. 24 The quantitative analysis of videotaped consultations of GPs with simulated patients did not show an effect of the ACA training programme on the number of issues discussed or the quality of GPs’ communicative behaviour. Using simulated patients to establish an effect is not optimal because it focuses on a single consultation, while in daily practice, communication between doctors and patients evolves during several serial consultations. Also, as communication skills training is ultimately geared toward enhancing health outcomes, it is important to assess patient-reported outcomes as well.
In this article, we report on outcomes reported by patients who received palliative care of GPs who participated in the ACA trial. We hypothesized that palliative care patients of GPs who had participated in the ACA training programme would score better on (1) palliative care outcome measures, (2) satisfaction with the communication with their GP, and (3) ratings of their GP’s availability, and discussion of current and anticipated issues.
Methods
Setting and participating GPs
This controlled trial was conducted during the first year of an existing postgraduate, 2-year Palliative Care Peer Group Training Course (PCPTC) for GPs in the Netherlands, where care to most patients in the palliative phase is provided in the patient’s home by generalists such as GPs and primary care nurses, with advice from end-of-life consultants when needed. The PCPTC consists of four 2-day residential courses, followed by 2-h peer group sessions with five GPs in each group, facilitated by a palliative care consultant, every 6–8 weeks. The residential courses focus on symptom control, ethical and spiritual/existential issues, management of care and communication skills. The peer group sessions provide inter-GP consultation. In an evaluation of the PCPTC, GPs reported an increase in their end-of-life care knowledge and skills. 25
All GPs enrolled in the four PCPTCs which started in 2006 and 2007 were invited to take part in the study. Without randomization, we assigned two PCPTCs (Eindhoven, 2006, and Rotterdam, 2007) to the intervention condition in which the ACA training programme was integrated into the existing course, and two PCPTCs (both in Amsterdam, 2007) to the control condition. For the latter group, all communication skills training was moved to the second year of the programme, that is, after the follow-up assessment.
Patients
After enrolment in the study, we asked the GPs (by a letter, with one or two phone calls as reminders) to select all patients who met the following criteria during the 3 months preceding the first (baseline) and third (12-month follow-up) residential course: (1) advanced illness with a life expectancy of less than 6 months (estimated by the GP), (2) at least 18 years of age, (3) adequate command of the Dutch language, (4) no serious psychopathology or cognitive disorder and (5) receiving care primarily from the participating GP. Given the short life expectancy of this population of patients, the patients included at 12-month follow-up were other patients than those at baseline.
The GP briefly described the study to eligible patients and asked them to participate. Patients interested in participating were sent an information sheet about the study, an informed consent form, a questionnaire and a postage-paid return envelope. If we did not receive a completed informed consent form and questionnaire within 2 weeks, the patient was phoned once or twice as a reminder.
Intervention
The ACA training programme consisted of eight steps (see Box 1), supported by the ACA checklist (see Box 2). 23 Steps 1 and 2 took place on the first day. Within 2 months, GPs received individual feedback on their videotaped consultation (step 3). During the following months, they completed step 4 in order to formulate their personal learning goals (step 5). Six months after the start of the programme, the GPs participated in role-play exercises (step 6). Finally, a second simulated consultation was videotaped (step 7) to allow participants to assess their communication skills against the ACA checklist (step 8).
The eight steps of the Availability, Current issues, Anticipation (ACA) training programme
Step 1 – Videotaped general practitioner (GP)–patient interview with a trained actor simulating a patient in an advanced stage of lung (role A) or colon (role B) cancer, according to detailed scripts; immediately after the interview, the participant receives general feedback on communication style from the actor.
Step 2 – Instructions on the ACA checklist, using oral presentations and written information (ACA booklet).
Step 3 – Feedback according to the ACA checklist on GP performance during the videotaped GP–patient interview in step 1.
Step 4 – Studying the ACA checklist, discussing this material with peers in small groups and trying out newly acquired skills in their own general practice to identify problem areas from their own experience.
Step 5 – Formulating learning goals based on the previous steps.
Step 6 – Role-play exercises tailored to the GP’s individual learning goals.
Step 7 – A second videotaped interview with an actor simulating a patient.
Step 8 – Using the second videotaped interview and the ACA checklist as tools for self-assessment of their communication skills.
The Availability, Current issues, Anticipation (ACA) checklist
Availability (of the general practitioner (GP) for the patient)
Taking time
Allowing any subject to be discussed
Active listening
Facilitating behaviour (e.g. empathic, respectful, attentive, occasionally also phoning or visiting the patient spontaneously)
Shared decision-making with regard to diagnosis and treatment plan
Accessibility (e.g. phone numbers)
Current issues (that should be raised by the GP)
Diagnosis
Prognosis
Physical complaints and worries
Psychosocial complaints and worries
Spiritual/existential complaints and worries
Wishes for the present and the coming days
Unfinished business, bringing life to a close
Treatment and care options (concerning 1–7)
Anticipating (various scenarios)
Offering follow-up appointments
Possible complications
Wishes for the coming weeks/months (personal wishes as well as preferences with regard to medical decisions)
The actual process of dying (final hours/days)
End-of-life decisions
Outcome measures
We asked the participating patients to complete the following questionnaires:
1. Palliative care outcome measures.
1.1. The Palliative Care Outcome Scale (POS), a validated 10-item questionnaire, covers the main components of palliative care. Eight questions have a 5-point Likert-scale response from 0 (‘not at all’) to 4 (‘overwhelming’), and two questions have 3-point Likert-scale responses (0–2–4). Patients were asked to answer the questions according to their experiences during the previous 3 days. Higher scores indicate more severe problems.26–28 1.2. The European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 15 Palliative (EORTC QLQ-C15-PAL) measures the health-related quality of life of cancer patients in palliative care as experienced during the previous week. It consists of 15 questions organized into two function scales (physical and emotional), seven symptom scales (e.g. fatigue, nausea/vomiting and pain) and an overall quality-of-life scale. Responses to 14 questions are given on a 4-point Likert scale ranging from 1 (‘not at all’) to 4 (‘very much’), and to the ‘overall quality of life’ question on a scale from 1 (‘very poor’) to 7 (‘excellent’). The scores are linearly converted to 0–100 scales, with higher values representing better functioning and quality of life, and greater symptom burden.29–31 1.3. The Rest & Peace Scale (RPS). In our qualitative study, we obtained information from patients, GPs and end-of-life consultants about what they considered to be desired outcomes of palliative care.
8
We used the six most frequently reported indicators of successful palliative care as items for the RPS: My GP helped me to (1) feel comfortable; (2) feel at peace; (3) accept my advanced illness; (4) value the last period of my life; (5) experience that the GP respects me; and (6) find out my preferred place to die.
All questions have 5-point Likert-scale responses from 1 (‘strongly agree’) to 5 (‘strongly disagree’). Scores are transposed so that higher scores always indicate better palliative care outcome.
2. From the validated Dutch version of the Patient Satisfaction Questionnaire–III (PSQ-III), we used the subscales interpersonal manner (7 items), communication (5 items) and time spent with GP (2 items). All questions have 5-point scale responses from 1 (‘strongly agree’) to 5 (‘strongly disagree’). Scores were transposed so that higher scores always indicate greater patient satisfaction.32,33
3. The ACA scale measures the extent to which the GP was available for and discussed important issues with the patient. The ACA checklist consists of 19 items divided into three categories: Availability (6 items), Current issues (8 issues) and Anticipation (5 issues) (see Box 2). All questions have 5-point Likert-scale responses from 1 (‘strongly agree’) to 5 (‘strongly disagree’), with higher scores indicating that the GP was more available and discussed more issues.
Additionally, the patient and GP questionnaires contained items assessing their socio-demographic and other characteristics.
Statistical analysis
We assessed the comparability of GPs in the intervention and the control condition on socio-demographic and professional characteristics using chi-square for categorical variables and the Mann–Whitney test for interval level variables. Variables on which the two GP groups were not comparable at baseline were entered as covariates in subsequent analyses.
We calculated the sample size on the primary outcome measure at GP level ‘number of 13 current and anticipated issues discussed’ (see Box 2) and considered a 0.5 standard deviation (SD) difference (which corresponded with one issue more or less) between groups as clinically relevant. Such a difference can be detected with 64 GPs in each group (power = 0.80, two-sided alpha = 0.05). 24
Due to poor prognosis, patients assessed at follow-up were different from those at baseline. Therefore, we present patient characteristics for all four groups. Missing data were minimal (0%–4% missing items), and values for these missing data were estimated using single response function imputation. 34
As the GP was the experimental unit of analysis and patients were nested within GP by time combinations, we used linear mixed models and accompanying effects to evaluate between-group differences over time for all outcome variables. In all analyses, we used the GP’s sex, age, practice location and percentage of full-time equivalent (FTE) working as covariates. Outcomes were presented as means, SDs and intervention effects. Between-group differences were first tested at the sum score/scale level. Where appropriate, analyses were conducted at the individual item level, but only when the results at the higher (scale) level were statistically significant. To adjust for multiple testing, the level of significance was set at 0.01. For all scales, we calculated internal consistency reliability using Cronbach’s coefficient alpha. All analyses were conducted in SPSS 20.0 (SPSS, Inc., Chicago, IL, USA).
Results
GP and patient characteristics
All 126 GPs eligible for the study agreed to participate. In all, 62 GPs (‘Eindhoven’ and ‘Rotterdam’) were assigned to the intervention group and 64 (‘Amsterdam’) to the control group. Of the 62 intervention GPs, 43 included one or more patients (30 GPs at baseline and 27 at follow-up). Of the 64 control GPs, 34 included patients (31 GPs at baseline and only 10 at follow-up) (see Figure 1). The primary reasons for not including patients were no patient needing palliative care in practice during inclusion periods, reluctance to ask a seriously ill patient to participate and the rapidly deteriorating condition of patients. Intervention GPs were more likely to practise in a rural location than control GPs. No further between-group differences were observed in the background characteristics of the GPs (Table 1). Also, the characteristics of those GPs who provided patients to the study were similar to those who did not.
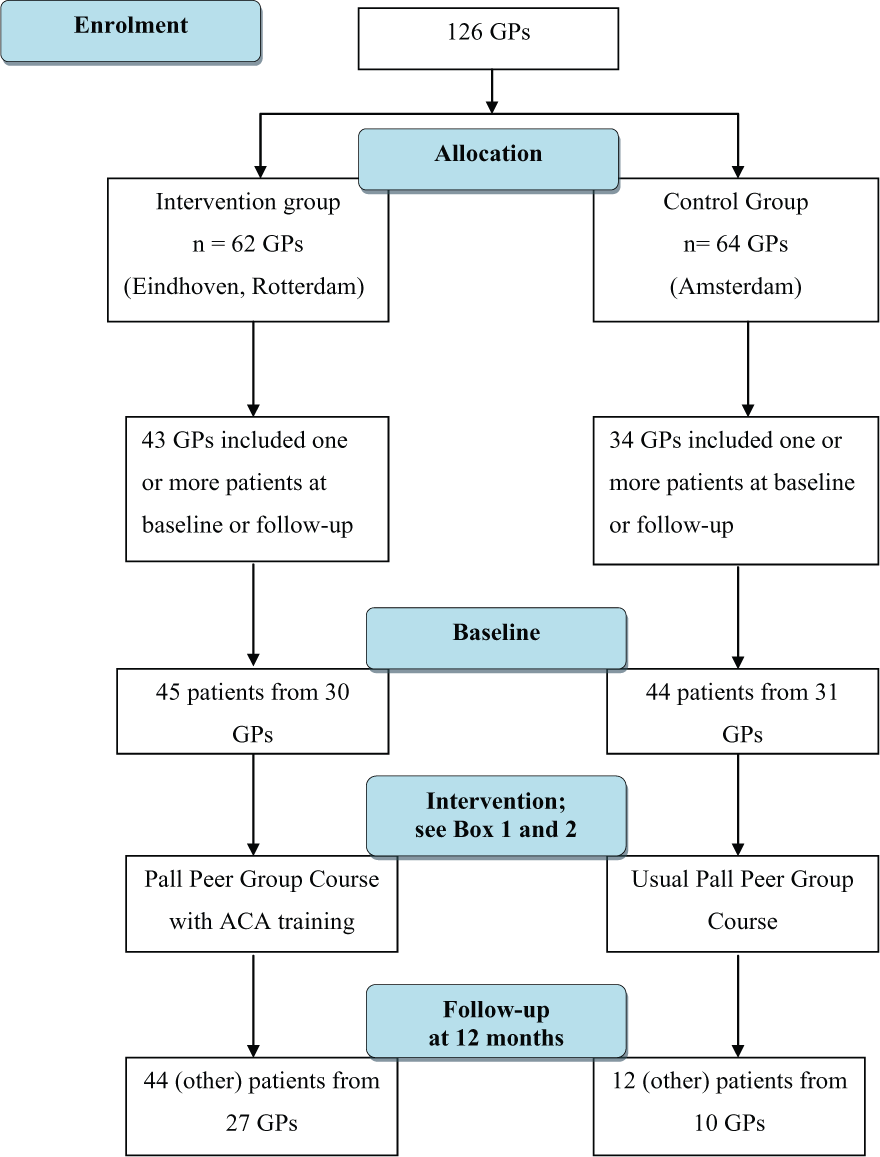
ACA trial flow diagram.
Socio-demographic and professional characteristics of participating general practitioners (GPs).
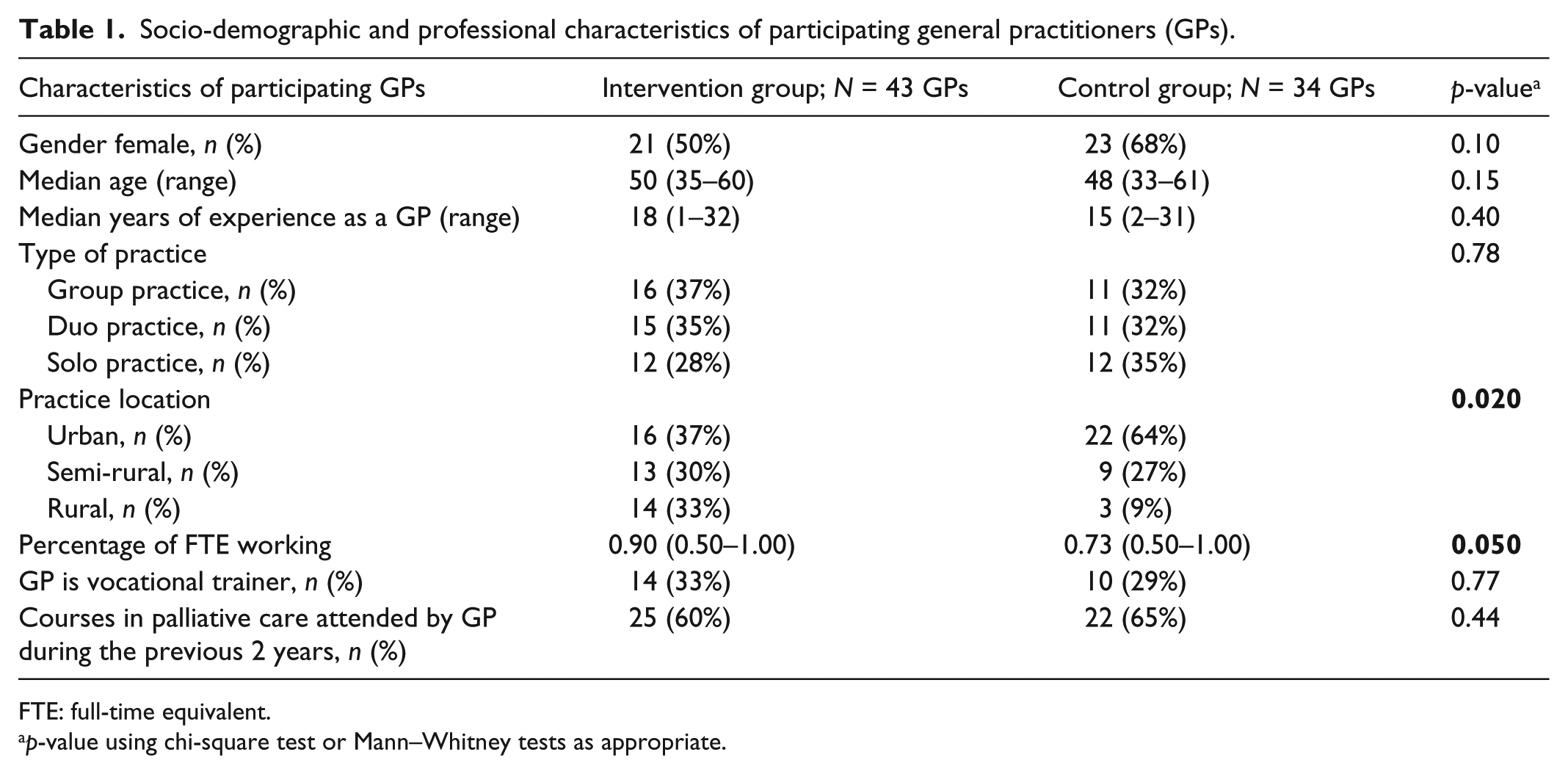
FTE: full-time equivalent.
p-value using chi-square test or Mann–Whitney tests as appropriate.
In total, the participating GPs included 169 palliative care patients, of whom 157 (93%) completed the questionnaire. Reasons for non-response were too weak to complete the questionnaire (8x), transfer to another setting (2x) and unknown (2x). We excluded 12 of 157 questionnaires because they were completed by a relative. The remaining 145 questionnaires (89 at baseline and 56 at follow-up) were included in the analysis.
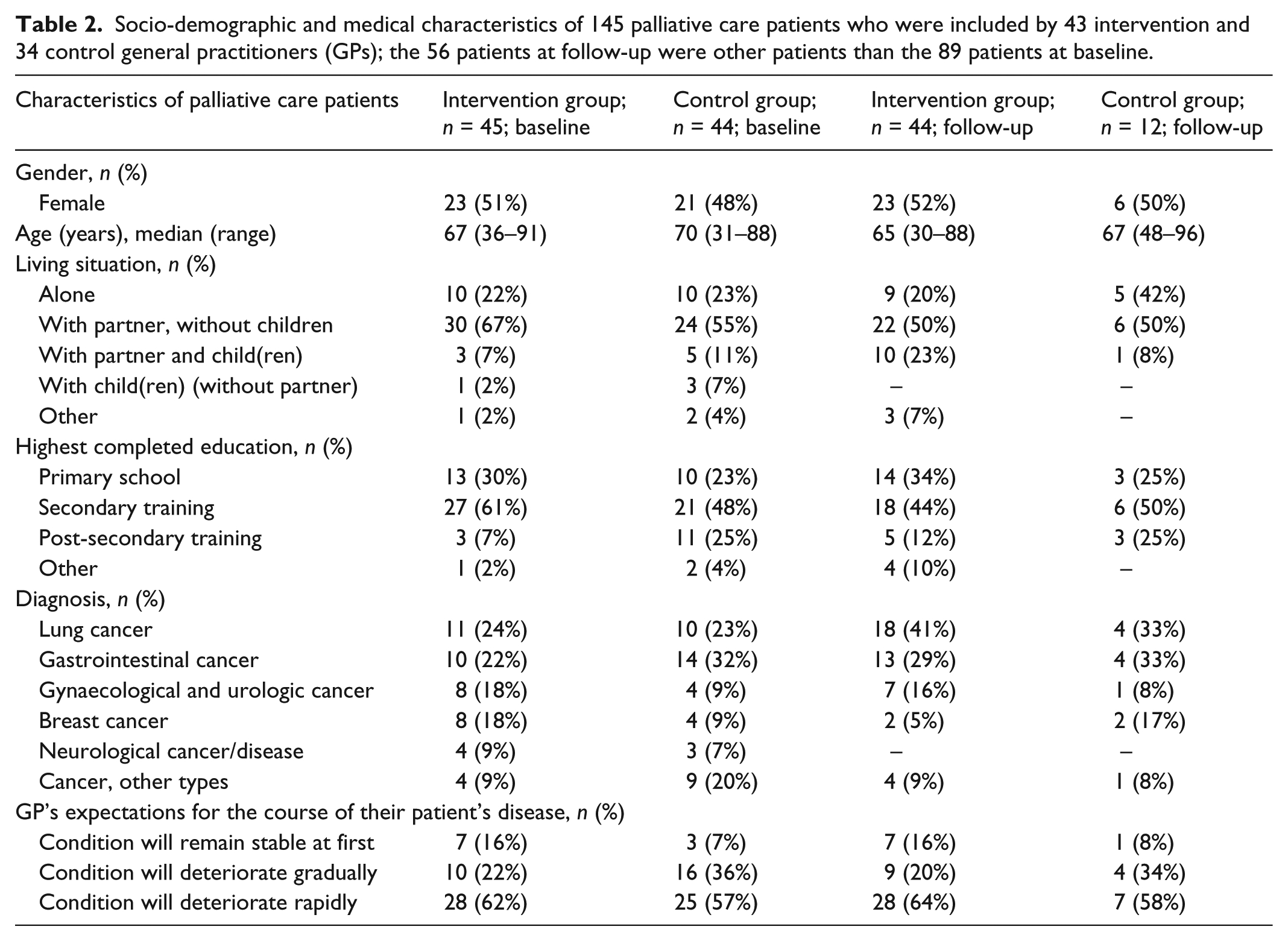
Patient characteristics were comparable for all four groups. Almost all patients had cancer, but three patients had a neurological disease (see Table 2). At follow-up, we collected only 12 questionnaires in the control group. As was to be expected, all patients at follow-up were other patients than those at baseline.
Socio-demographic and medical characteristics of 145 palliative care patients who were included by 43 intervention and 34 control general practitioners (GPs); the 56 patients at follow-up were other patients than the 89 patients at baseline.
Outcomes
Primary outcomes
We found no significant effects of the ACA training programme on patients’ ratings of palliative care outcomes (POS, QLQ-C15-PAL and RPS), satisfaction with the communication with their GP (PSQ-III) or GP’s availability and discussed current and anticipated issues (ACA scale) (see Table 3).
Sum scores and effect of ACA communication training programme for the Palliative Care Outcome Scale (POS), the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 15 Palliative (QLQ-C15-PAL), the Rest & Peace Scale (RPS), the Patient Satisfaction Questionnaire–III (PSQ-III) and the ACA scale, based on ratings by 145 palliative care patients of intervention GPs (n = 43) and control GPs (n = 34), at baseline and at follow-up (the 56 patients at follow-up were other patients than the 89 patients at baseline).
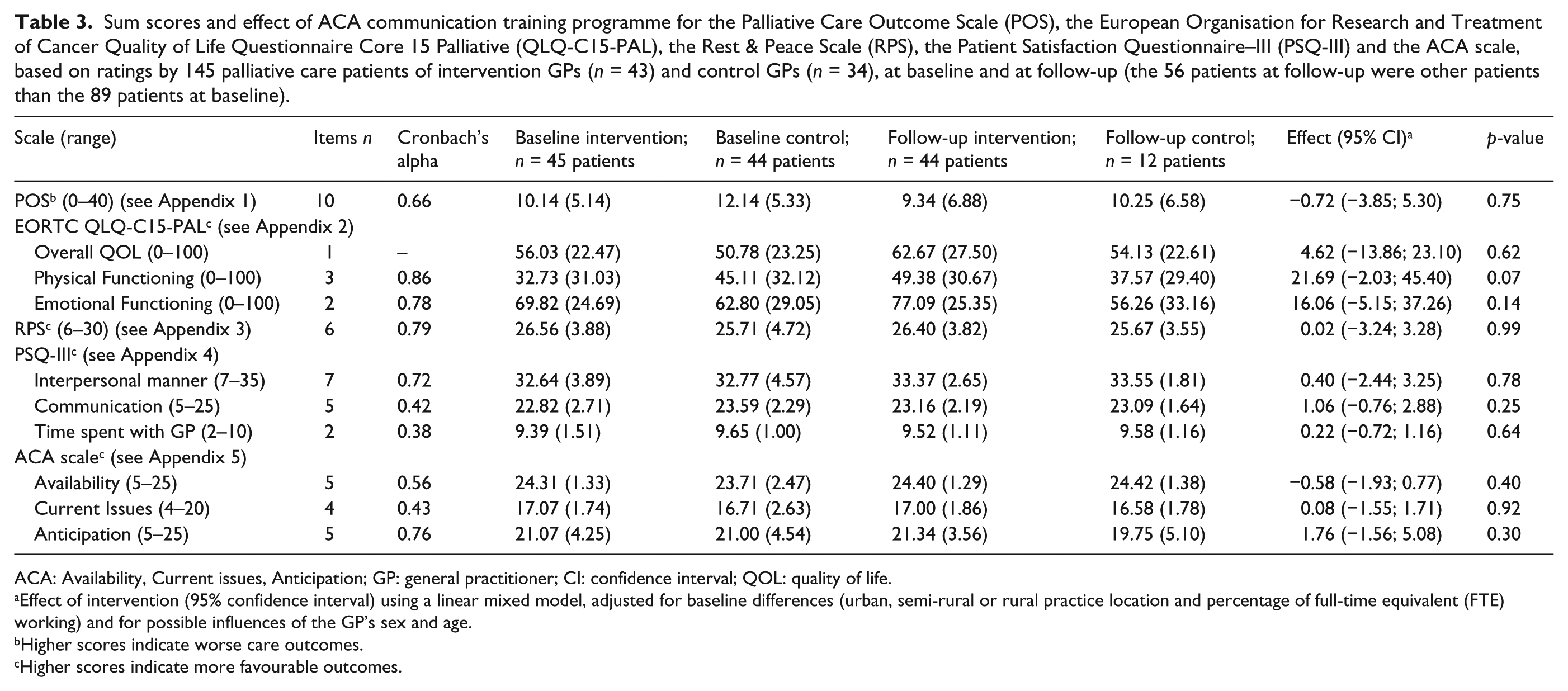
ACA: Availability, Current issues, Anticipation; GP: general practitioner; CI: confidence interval; QOL: quality of life.
Effect of intervention (95% confidence interval) using a linear mixed model, adjusted for baseline differences (urban, semi-rural or rural practice location and percentage of full-time equivalent (FTE) working) and for possible influences of the GP’s sex and age.
Higher scores indicate worse care outcomes.
Higher scores indicate more favourable outcomes.
Descriptive results
Most Rest & Peace items, all PSQ-III items and most ACA items showed near-ceiling scores in all groups. For the QLQ-C15-PAL, the most prevalent symptoms were fatigue, appetite loss and pain. For the RPS, lower scores were observed for ‘my GP helped me to find out my preferred place to die’. For the ACA scale, lower values were observed for ‘unfinished business’, and to a lesser extent for ‘prognosis and possible complications’, ‘the actual process of dying’ and ‘euthanasia’.
Discussion
In this controlled trial, we found no significant differences over time between the intervention and control GPs in the patients’ mean ratings on any of the five outcome measures. In general, patients greatly appreciated the palliative care provided by their GPs. They gave near maximum ratings for ‘comfortable’, ‘at peace’, ‘acceptance’, ‘valuable last period of life’ and ‘respect’ (RPS), for satisfaction with the communication with their GPs (PSQ-III), and for most items of the ACA scale. The lower scores we found in both groups for one RPS and a few ACA items suggest that GPs might take more initiative to discuss the following end-of-life issues: unfinished business, prognosis and possible complications, the actual process of dying, including the preferred place of death, and end-of-life decisions.
The study had a number of strengths and limitations worth noting. To our knowledge, this is the first study on effectiveness of a palliative care communication training programme for GPs using outcomes at patient level. 21 Both the educational approach and content of the intervention are evidence-based. Patient-reported outcomes were quantitatively measured with three validated instruments (POS, QLQ-C15-PAL and PSQ-III) and two study-specific instruments (RPS and ACA scale). This study focused on GPs’ performance, which is the (patient-reported) fourth level of Miller’s pyramid model (‘knows’, ‘knows how’, ‘shows’ and ‘does’). 35
Although we assigned participating GPs to either the intervention or the control condition without randomization, we carefully compared both groups and included significant between-group differences on background characteristics as covariates in subsequent analyses. However, the necessity of using different patients at baseline and follow-up complicated the design. The relatively modest sample size, particularly at follow-up, limited the power of the study. The recruiting of only 12 patients in the control group at follow-up compared to 44 in the intervention group may reflect a lower motivation to recruit patients by control GPs than by intervention GPs. Although only about half of the GPs included patients in the study, the response rate among patients was very high. Although the GPs were not blinded to the training condition, their patients were.
In our previous qualitative study, 8 we assumed that GP–patient communication in the palliative care setting was suboptimal. Yet, in the current trial, patients reported high levels of satisfaction with the communication and care provided by their GP. This discrepancy might reflect some level of selection bias (i.e. that GPs referred only certain patients to the study), some degree of reluctance on the part of patients to be critical of the care they received, limitations of the questionnaires used or a combination of these factors.
In a systematic review on communication training programmes for health care professionals (other than GPs) which focused on life-limiting conditions, a number of important features of a successful communication model were identified, including focused participant-led training and using effective communication to improve patient understanding and flexible patient-led ‘Advance Care Planning’. 36 This is in line with the educational methods and content of the ACA training programme.
In a German study of the impact of a basic training course in palliative care for GPs, no significant training effect was found on the patient-reported outcomes (the POS and the QLQ-C15-PAL). 37 Similarly, although a Cochrane review on the effectiveness of communication skills training for medical specialists and oncology nurses in cancer care demonstrated moderate effects on health care professional communication behaviour, few effects were observed on patient-reported outcomes. 38
We found no effect of the ACA training programme at either the GP or the patient level. 24 Although our findings indicate that the intervention is ineffective, there are other possible explanations that should be taken into consideration when interpreting the results. First, in comparison to medical specialists and oncology nurses, the GPs in our trial may have been so well trained in doctor–patient communication as part of their pre- and postgraduate education that additional training in specific elements of communication in palliative care may not have added much to their communication skills. Moreover, by using PCPTCs for our study, we realized that we would be recruiting GPs with specific interest in palliative care. While this might have had implications for the generalizability of the results, it increased the feasibility of the project substantially. This may explain, at least in part, the high level of patient satisfaction with communication and palliative care provided by their GPs at baseline, which allowed little room for improvement on these outcomes over time.
Second, a study comparing the prevalence of GP–patient discussion of end-of-life topics across four countries found that Dutch GPs discussed more topics than GPs in Italy, Spain or Belgium. 39 This also may explain the high scores at baseline in our Dutch study.
Implications for clinical practice and future research
The descriptive results from our study suggest that although palliative care patients were generally quite satisfied with the care received from their GPs, GPs should take the initiative to discuss certain end-of-life issues, including unfinished business, prognosis and possible complications; the actual process of dying; and end-of-life decisions more often and/or more thoroughly. Future training programmes of this nature should give particular attention to these issues.
Future research on GP communication and care skills training programmes in the palliative care setting should include a broader sample of GPs, focusing on those professionals who have less experience (and perhaps less a priori interest) in palliative care issues. Although this may present real challenges in recruitment to such a programme, it may enhance the added value of the training experience considerably. Given international differences that have been reported in the literature on GPs palliative care-related communication behaviour, future efforts should be devoted to developing appropriate and effective training programmes in other countries as well. Hopefully, the lessons learned from our training programme can contribute to such efforts in the future.
Footnotes
Acknowledgements
We wish to thank Bernardina Wanrooij for granting us permission to evaluate the Availability, Current issues and Anticipation (ACA) training programme within her Palliative Care Peer Group Training Courses, and all patients and GPs who participated in the study.
Declaration of conflicting interests
The funding bodies had no involvement in or influence on the study and the authors.
Ethics committee
The study protocol was approved by the Medical Ethics Committee of the VU University Medical Center (2004/077). The trial was registered in the ISRCTN Register (ISRCTN56722368).
Funding
The study was funded by the Comprehensive Cancer Centres of Amsterdam and Eindhoven, CZ Healthcare Insurances, Pfizer bv and the Janivo Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.