
Abstract
Background:
Internationally, policy calls for care homes to provide reliably good end-of-life care. We undertook a 20-month project to sustain palliative care improvements achieved by a previous intervention.
Aim:
To sustain a high standard of palliative care in seven UK nursing care homes using a lower level of support than employed during the original project and to evaluate the effectiveness of this intervention.
Design:
Two palliative care nurse specialists each spent one day per week providing support and training to seven care homes in Scotland, United Kingdom; after death audit data were collected each month and analysed.
Results:
During the sustainability project, 132 residents died. In comparison with the initial intervention, there were increases in (a) the proportion of deceased residents with an anticipatory care plan in place (b) the proportion of those with Do Not Attempt Cardiopulmonary Resuscitation documentation in place and (c) the proportion of those who were on the Liverpool Care Pathway when they died. Furthermore, there was a reduction in inappropriate hospital deaths of frail and elderly residents with dementia. However, overall hospital deaths increased.
Conclusions:
A lower level of nursing support managed to sustain and build on the initial outcomes. However, despite increased adoption of key end-of-life care tools, hospital deaths were higher during the sustainability project. While good support from palliative care nurse specialists and GPs can help ensure that key processes remain in place, stable management and key champions are vital to ensure that a palliative care approach becomes embedded within the culture of the care home.
Keywords
Background
More people now live longer; those living beyond 75 years will increase from around 5 million in 2010 to 8 million in 2030. 1 People will be older when they die, 2 and the number of care home residents will increase. 3 More care home residents will die there, increasing the importance of palliative care in these settings. 4,5
Good quality palliative care in care homes is reflected by a number of markers. These include a plan of action for end-of-life care, the establishment of mechanisms to discuss and record the preferences of residents approaching end of life, ongoing review of a resident’s need for end-of-life care, use of care pathways for dying residents, and access to staff training. 6 While some care homes already implement these processes to some extent, there is much variability. 7 Consequently, interventions that can be readily adopted and sustained by care home staff are required and would benefit many.
In 2007–2008, an intervention to improve palliative care in all seven nursing homes located in a geographically defined area of the United Kingdom was implemented. The intervention was based on the Gold Standards Framework for Care Homes (GSFCH) programme and ran for 18 months. 8 The GSFCH programme is an evidence-based approach that aims to improve the care provided to residents approaching end of life through better coordination and organization. As part of the GSFCH study, each care home appointed two ‘key champions’ to coordinate the project in their own nursing home and to help embed the new systems that were implemented. Key champions attended a four day training course ‘Foundations in Palliative Care for Care Homes’ 9 and were encouraged to cascade this training to the care home staff. An experienced nurse researcher working full-time on the project visited each care home every 10 to 14 days, providing ongoing advice, training, role modelling and support to the staff and management. This resulted in a significant increase in the use of advance care plans, completion of Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) status documentation, and use of the adapted Liverpool Care Pathway (LCP). 10 Hospital deaths and inappropriate hospital admissions decreased during the project, and bereaved relatives expressed greater satisfaction with care. 8,11
At a time of international economic uncertainty, cost-effective sustainability is vital if good palliative care is to become embedded in everyday practice. However, sustaining new interventions in service organizations is complex and multifaceted. 12,13 Many time-limited interventions such as the GSFCH project described above are taking place in care homes, but there is little consideration of the most appropriate levels of support needed to sustain them and incorporate new processes into routine practice. There is a need for projects that aim to sustain and evaluate the outcomes achieved during original time-limited interventions, even when the initial level of resources is not available or when the implementation of the project needs to be adjusted to fit with local constraints. We could find no previous studies evaluating the sustainability of such interventions.
The aim of the sustainability project reported here was to sustain the results achieved following the initial GSFCH project using a lower level of care home support. Specifically, compared with the original GSFCH project, this project aimed to sustain (a) the proportion of residents dying with a care plan in place, (b) the proportion of residents dying on a care pathway, (c) the proportion of residents with DNACPR documentation in place, and (d) the proportion of residents dying in the care home. A further aim was to guide wider roll-out of the intervention through the United Kingdom.
Method
Characteristics of participating care homes
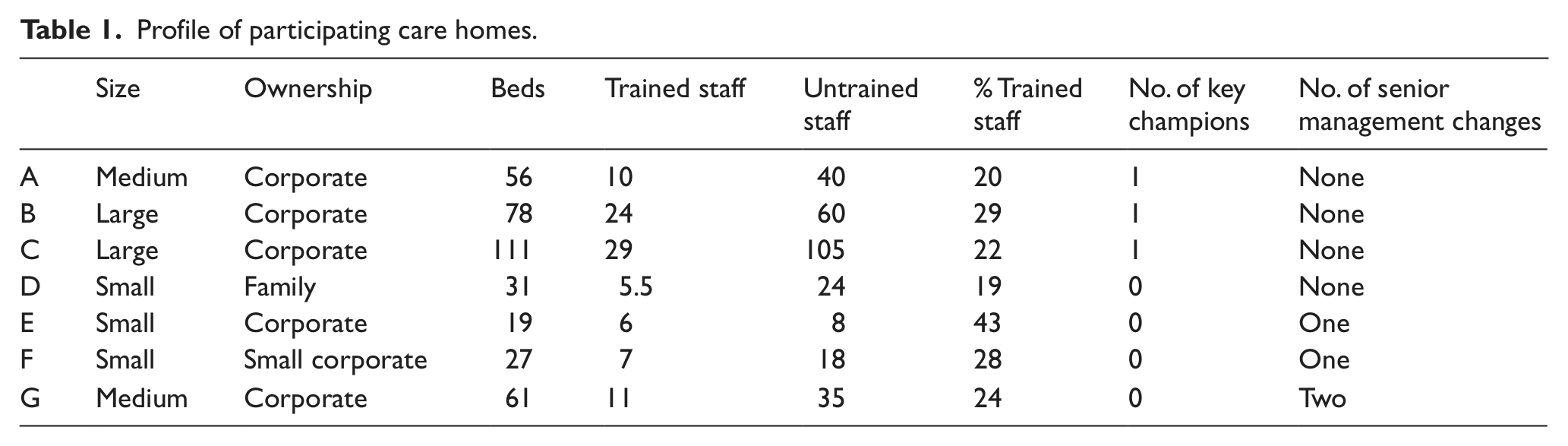
All seven care homes in the initial project 14 took part in the sustainability project. Three care homes experienced changes of senior management during the project (Table 1). One care home was unable to participate initially due to temporary closure and management changes (care home G)but later became involved. Only three of the original 16 key champions remained between the completion of the original project and the start of the sustainability project. Most had left the care homes in the interim.
Profile of participating care homes.
Sustainability project intervention
From November 2009 to June 2011, six of the seven care homes received dedicated support from two community palliative care clinical nurse specialists (CNSs) (B.S. and R.M.) who each spent one day per week working with care home managers, staff and GPs. This equated to approximately 7.5 h of support per care home per month. The CNSs provided a rolling education programme based on the Macmillan Foundations in Palliative Care for Care Homes. 9 This programme has four modules: (a) first principles, (b) communication, (c) pain and symptom management and (d) bereavement. Communication skills development was also offered to staff, who were given the opportunity to shadow community CNSs and hospice staff for a day.
The nurse specialists helped care home staff consider if residents might benefit from a palliative approach. Central to this was the use of a ‘supportive/palliative care register’. This register involves classifying each resident according to prognosis. A prognostic indicator of ‘A’ reflects a resident who is expected to live for more than a year, ‘B’ reflects a prognosis of ‘months’, ‘C’ reflects ‘weeks’ and ‘D’ reflects ‘days’. The nurse specialists attended care home monthly meetings where the palliative care register was discussed. These meetings were also attended by the GP responsible for the majority of care home residents. At these meetings, the nurse specialists supported care home staff in assessing the prognosis of a resident. They also offered support by phone and in person outside of these meetings as required. Care home staff were encouraged to implement anticipatory care plans (ACP) from admission. They were also informed of the benefits of using pain assessment tools and were trained to use the adapted LCP when residents were identified as approaching death.
From November 2009 to June 2011, the care home managers or charge nurses recorded information about each death that had occurred during the month. All information was anonymized before being communicated to the nurse specialists and analysed by the hospice-employed research facilitator (A.F.). Anonymized data collected for each deceased resident included the following: prognosis in the weeks prior to death (as indicated by the supportive/palliative care register), DNACPR documentation status, whether the resident was on the LCP or had an anticipatory care plan in place before they died and preferred and actual place of death.
The sustainability project reported here was a continuation of the original project that was deemed a service evaluation by the South East Scotland Research Ethics Committee. 8 Thus, formal approval by the local research ethics committee was not required. The management team in each care home gave permission for the sustainability project and data analysis.
Outcomes/measures
To determine whether the sustainability project managed to sustain the outcomes achieved during the original GSFCH project, the following outcome measures were compared between the original GSFCH project and the sustainability project:
DNACPR documentation in place. Proportion of deceased residents where DNACPR documentation had been completed.
ACP. Proportion of residents with any form of anticipatory care plan in place.
LCP (adapted). The proportion of residents known to have died on the adapted LCP.
Inappropriate hospital deaths of frail elderly patients. ‘Inappropriate hospital deaths’ were defined as ‘frail elderly patients with dementia who had been gradually deteriorating, admitted to hospital with suspected pneumonia/dehydration, who then died within 3 days of admission’. 8,14
Hospital deaths. The proportion of deceased residents who died in hospital.
Results
Education activity
Thirty-five workshops were carried out during the course of the project. Staff across all care homes were invited to attend each workshop, and the number of workshops was based on staff need and CNS time. Each workshop lasted 2.5 h and was facilitated by both nurse specialists. On average, approximately four staff members attended each session, and staff from all care homes participated. Workshop attendees were primarily care assistants (75%) and trained staff nurses (21%), reflecting the overall staff composition. A further nine care home staff shadowed a nurse specialist and hospice staff for a day.
Palliative care outcomes
In total, 132 residents died during the course of the sustainability project. Key outcomes were compared to the initial, more intensive, GSFCH intervention, where significant improvements had occurred. 8 During the sustainability project, there was a further increase in the proportion of residents who experienced some form of anticipatory care planning and had DNACPR documentation in place. Furthermore, a greater proportion of residents were on the LCP when they died; and inappropriate hospital deaths fell to 4% of all deaths. Thus, these outcomes continued to show significant improvements compared with baseline levels reported before the initial GSFCH intervention. However, hospital deaths increased to 23% during the sustainability period (Table 2).
Primary outcomes of the sustainability project compared to the original GSFCH project (%).
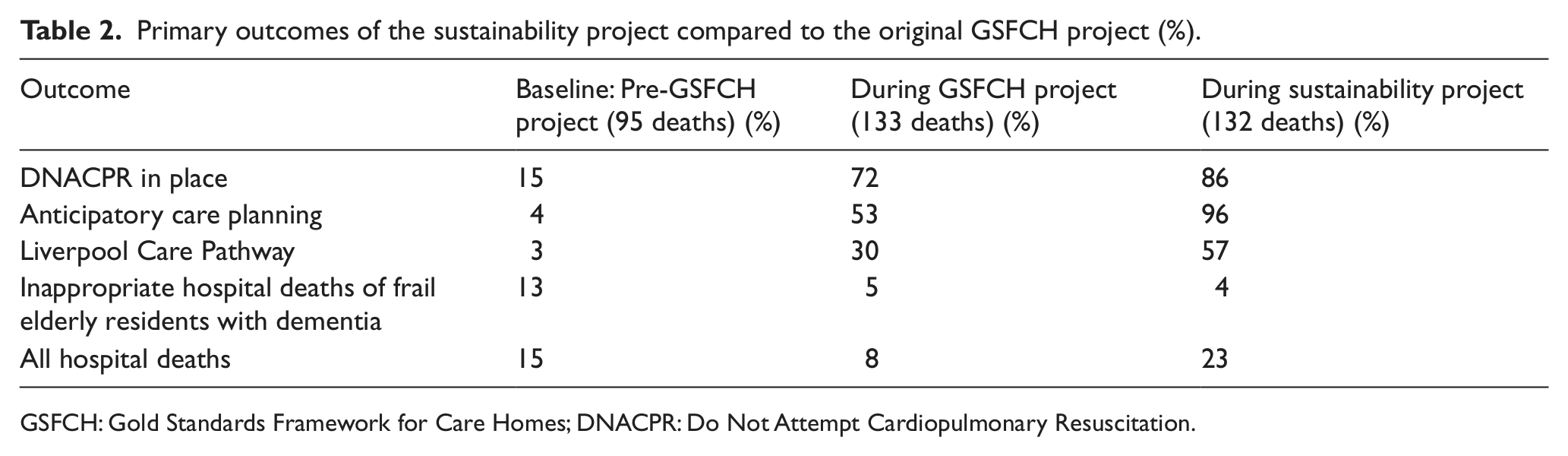
GSFCH: Gold Standards Framework for Care Homes; DNACPR: Do Not Attempt Cardiopulmonary Resuscitation.
Hospital versus care home deaths
During the sustainability project, 30 of 132 residents (23%) died in hospital. None of these residents had been expected to die in the coming days (i.e. none had been classified as ‘D’ on the supportive/palliative care register); and 63% had been expected to live for a number of months or years (i.e. had a prognostic indicator of A or B). Reasons for hospital admissions included sudden collapse, sudden deterioration or a fall.
Just over half of those who died in hospital did not have a DNACPR in place, though 80% had experienced some form of anticipatory care planning. Place of death preference was unknown for half of the residents who died in hospital. In all cases, care home staff did not know whether the resident had been on an integrated care pathway prior to death. In contrast, residents who died in a care home tended to have a DNACPR in place (97%), had an ACP in place (99%) and were more likely to have been on the LCP prior to death (57%). All residents who died in the care home had had their preferences for place of death recorded.
Stable versus unstable care homes
The outcomes for care homes that had not experienced management changes during the sustainability project (stable care homes) were compared with those that had experienced changes (unstable care homes). Overall, the outcomes for the three care homes that experienced management changes were inferior to the four stable care homes. Of particular note, hospital deaths in the care homes that had management changes were notably high at 50%; and staff in these care homes were less able to identify frail elderly patients with dementia who were close to death (Table 3).
Key outcomes for stable and unstable care homes.
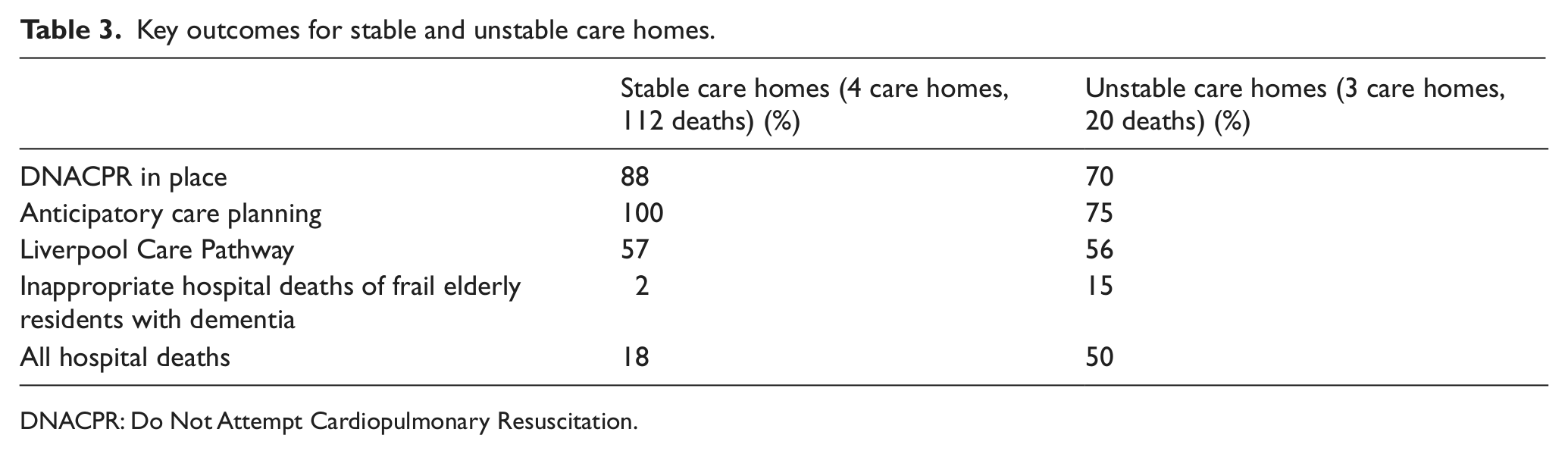
DNACPR: Do Not Attempt Cardiopulmonary Resuscitation.
Identifying patients approaching end of life
The prognostic indicator associated with all residents who died was examined Occasionally, care home staff were unable to determine whether a resident was expected to have years (A) or months (B) to live, so chose A/B instead of a discrete category. This also occurred at times when deciding between B and C or C and D prognostic indicators. Approximately one-third of deceased residents were identified as approaching death prior to actual death, that is, had a prognostic indicator ‘D’, suggesting only days to live (Figure 1(a)). All these residents died in the care home. However, 30% of residents who died had a prognostic indicator of ‘A’ or ‘A/B’ indicating that they had not been expected to die in the short term. Sixty-three per cent of these residents died in the care home, while 37% died in hospital (Figure 1(b)).
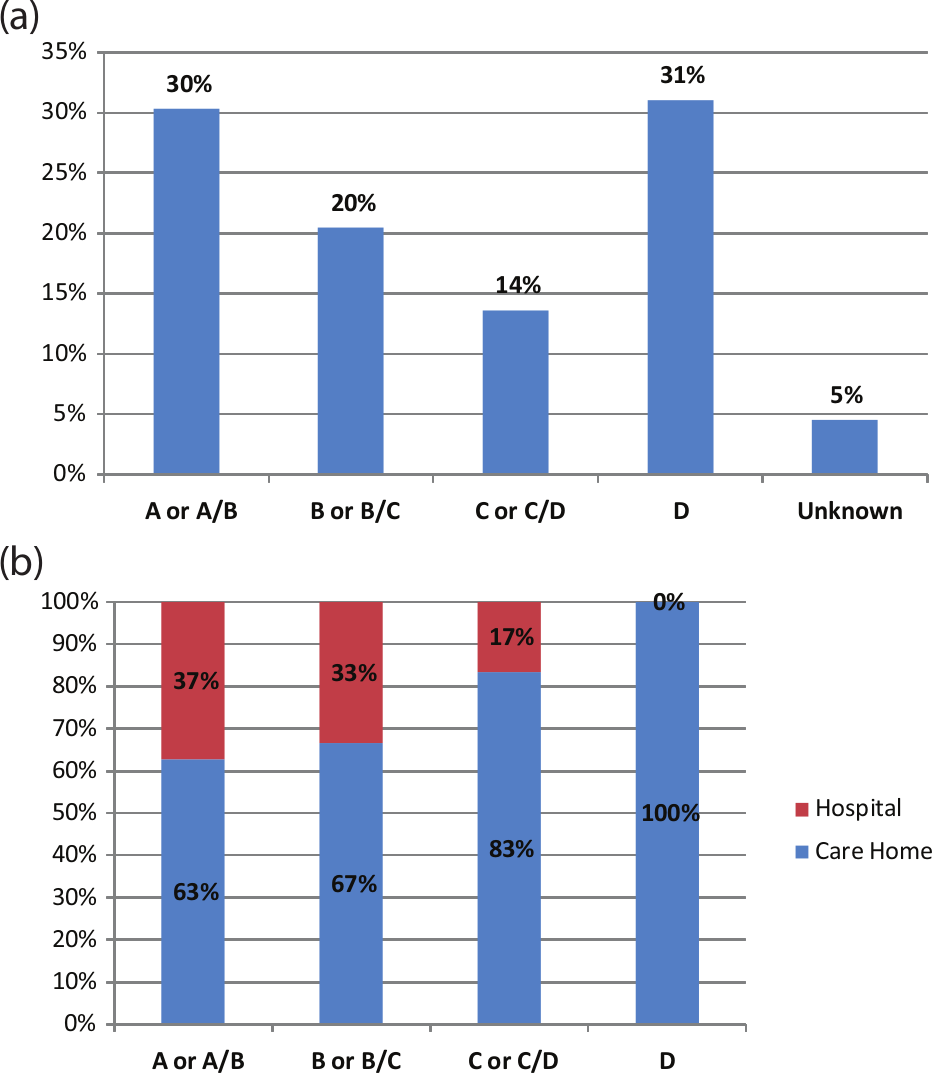
(a) Prognostic indicator associated with deceased residents (N = 132) and (b) prognostic indicator of residents and actual place of death (N = 126).
Preferred place of death
A preferred place of death (PPD) was recorded for 86% of all residents. In all cases, the patient’s PPD was the care home. Eighty-six per cent of those with a recorded preference died in the care home. In contrast, only 26% of those with an unknown preference died in the care home. Residents with an unknown PPD were five times more likely to die in hospital compared to those with a known PPD - 14% of residents with a known PPD died in hospital compared with 74% of those with an unknown PPD.
Discussion
Principal findings and possible explanations
During the sustainability project, with less than half of the previous amount of nursing support and other resources, the improved outcomes were largely maintained. Indeed, there were further increases in the completion of DNACPR documentation, ACPs and the adoption of the adapted LCP. Inappropriate hospital deaths of frail elderly individuals with dementia remained at levels similar to those reported during the original GSFCH project. Despite this, an increase in total hospital deaths occurred. The sustainability project appeared to assist in the implementation of key processes that are indicative of good quality palliative care but did not sustain the exceptionally high level of care home deaths.
Hospital deaths were 23% during the sustainability project. This is in line with the national average across Scottish care homes, which was 23% in 2009 and 2010. 15 However, this was a considerable increase from 8% reported during the original GSFCH project. There are a number of factors that may account for this increase. First, three care homes experienced management changes during the sustainability project – hospital deaths in these care homes were higher than in the stable care homes, contributing to the overall increase. Second, of the 16 key champions deemed pivotal to embedding the principles of palliative care within the care homes in the original GSFCH project, only three remained in the sustainability project. Such high levels of staff turnover are not uncommon in care home settings. Third, a higher level of support was available to care home staff and managers during the GSFCH project. During the GSFCH project, one full-time palliative care nurse worked to support the care homes; however, during the sustainability project, support equating to only 0.4 full-time equivalent (FTE) was available. Fourth, factors such as the commitment and availability of the nurse researcher may have had a significant, albeit transient influence on hospital deaths during the original GSFCH project.
Feedback from care home managers and a GP involved in the initial project suggested that the high levels of care home deaths reported prior to the sustainability project were viewed with concern by the Care Commission (now the Care Inspectorate); that is, there was some discomfort that perhaps too many residents were dying in the care home. According to care home managers, this concern may have made staff more hesitant to care for dying residents in the care homes, thus resulting in a subsequent increase in hospital transfer. While concern at unusually high levels of care home deaths is understandable and may be appropriate, it is also important that commissioners and policy-makers understand that care home deaths can indicate good quality palliative care.
Hospital deaths may have increased as the type and needs of individuals being admitted to care homes are changing. Residents are older and have more complex symptoms. 16 Multi-morbidity is very common 17 and makes prognostication more challenging for care home staff. Care home nursing staff may need additional training and support to deal with these more complex situations where people deteriorate suddenly and unexpectedly; and to recognize dying, which is a considerable skill, and requires confidence and the ability to take responsibility. Until such training is available, they may feel more confident transferring the resident to hospital, rather than managing their symptoms in the care home.
Residents with a known PPD were five times more likely to die in their preferred place compared with those for whom preferences were unknown. Nearly all residents who had no information on PPD had a prognostic indicator of A or A/B indicating that they had not been expected to die. However, good anticipatory care planning for residents could begin on first admission to the care home, so that staff are informed about the preferences of residents who deteriorate suddenly and can use this information as a guide to caring for the resident as they approach end of life.
A large UK study has shown that variability in GP support for care homes, in particular out-of-hours support, can be a challenge to the provision of good quality end-of-life care. 18 This is particularly relevant in care homes that work with a number of GP practices, as opposed to a single practice. 19 However, in the care homes described here, most residents are registered with the same general practice, and the GP from that practice was invited to attend the monthly meetings where changes in the health of residents were discussed. The level of support available to care homes from GPs appeared to be similar in both projects, and during both projects a directed enhanced service offering financial incentives to GPs to identify and support care home residents was available. This suggests that the good relationship established with GPs during the original GSFCH project was maintained during the sustainability project.
Strengths and limitations
This is the first study to specifically examine the sustainability of improvements in palliative care in care homes achieved following a more intensive initial implementation. It highlights some of the challenges associated with implementing a previously successful intervention with fewer resources. The nursing support offered to care homes during the sustainability project was integrated into the work of the local hospice community nursing team and thus had greater potential to be more cost-effective and sustained in the long run.
There is a wide variation in the way that end-of-life care tools and processes are implemented across care homes generally. 20 In the sustainability project, reported use of DNACPR documentation, anticipatory care planning and the LCP increased, suggesting growing familiarity with these systems. However, it is unclear the extent to which the use of such tools was embedded in practice – for instance, DNACPR status completion can be seen as a tick-box exercise or can be embedded within a comprehensive ACP. In future studies, more details in relation to how embedded these processes are within each care home and how well they are understood in context of offering good quality palliative care would be useful.
A distinction can be made between ascertaining the wishes of residents and implementing the wishes of residents. 20 For instance, if care home staff view anticipatory care planning as being predominantly about ascertaining the wishes of residents, this may downplay the importance of implementing these wishes. While evidence of anticipatory care planning is very useful, 21,22 outcomes that highlight the extent to which a resident’s choices were actually achieved are even more informative about the quality of care received by the resident. Such outcomes might include dying in the resident’s preferred place or a measure of family satisfaction with care following a resident’s death.
Implications for future research
Considerable research points to the benefits of implementing palliative care programmes in care homes. 8,18,23 More studies that examine the sustainability of improvements achieved during an initial programme are required. 24 Our study highlights the challenges in conducting such follow-up studies. For instance, the level of resources that was used for the initial implementation may no longer be available to provide the level of support initially received; management and staff changes mean that care homes come to the follow-up study with varying degrees of understanding and commitment to the project, and new policy developments, while helpful, can make it difficult to tease apart changes that are due to an intervention versus changes that would have occurred over time. Future sustainability studies that explore the impact of different components of these complex interventions (e.g. level of nurse specialist support available; existence of key champions, GP commitment; staff turnover; take-up of training; care home management style and staff confidence in delivering palliative and end-of-life care) are recommended.
Conclusion
A lower level of care home support managed to sustain, and in some cases improve, the use of supportive and palliative care tools in these care homes. However, despite increased adoption of these tools, reductions in hospital deaths were not maintained. While good support from specialist palliative care nurses and GPs can help ensure that key systems and processes remain in place, stable management and key champions are vital to ensure that a palliative care approach becomes embedded within the culture of the care home.
Footnotes
Acknowledgements
We would like to thank Dr Jo Hockley for very helpful comments on an earlier version of this manuscript. We would also like to thank the project steering group including Shirley Fife for their guidance in the early stages of this project and the staff and management of the care homes who took part in this study. Thank you also to two anonymous reviewers who provided very insightful and helpful comments.
Funding
This project was made possible by funding received from the Robertson Trust and the Midlothian Community Health Partnership.