
Abstract
Background:
The provision of high-quality palliative care in nursing homes (NHs) is a major challenge and places demands on the knowledge and skills of the staff.
Aim:
This study assesses the palliative care knowledge of staff in NHs in Europe.
Design:
Cross-sectional study using structured survey
Setting/participants:
Nurses and care assistants working in 322 representative samples of NHs in Belgium, the Netherlands, England, Finland, Poland and Italy. Palliative care knowledge is measured with the Palliative Care Survey. Scores on the scales range between 0 and 1; higher scores indicate more knowledge.
Results:
A total of 3392 NH-staff were given a questionnaire, and 2275 responded (67%). Knowledge of basic palliative care issues ranged between 0.20 in Poland (95% confidence interval (CI) 0.19; 0.24) and 0.61 in Belgium (95% CI 0.59; 0.63), knowledge of physical aspects that can contribute to pain ranged between 0.81 in Poland (95% CI 0.79; 0.84) and 0.91 in the Netherlands (95% CI 0.89; 0.93), and knowledge of psychological reasons that can contribute to pain ranged between 0.56 in England (95% CI 0.50; 0.62) and 0.87 in Finland (95% CI 0.83; 0.90). Factors associated with knowledge were country, professional role and having undertaken formal training in palliative care.
Conclusions:
Knowledge of nurses and care assistants concerning basic palliative care issues appears to be suboptimal in all participating countries, although there is substantial heterogeneity. Education of nursing staff needs to be improved across, but each country may require its own strategy to address the unique and specific knowledge gaps.
What is already known about the topic?
Qualitative and small-scale studies suggest that nursing home staff may have poor knowledge of palliative care.
Educational gaps in the training of nursing home staff have been addressed as an important barrier to high-quality palliative care.
To develop effective training strategies to improve the quality of palliative care in nursing homes, empirical evidence regarding the current palliative care knowledge of the nursing home staff and of the factors that are associated with the level of knowledge are required, but not available.
What this paper adds?
A cross sectional study of 2275 nurses and care assistants working in representative samples of nursing homes in Belgium, the Netherlands, England, Poland and Italy shows that staff knowledge concerning common palliative care issues is generally poor.
Implications for practice, theory or policy
The large variation in the level of knowledge between the countries suggests that each country may require its own training strategy to address the unique knowledge gaps of all levels of its nursing home staff.
Introduction
The provision of high-quality palliative care to the growing number of older people living and dying in nursing homes is a challenge in European countries and requires that staff possess adequate knowledge and skills. The world’s population is ageing. 1 In Europe, the largest percentage increase is predicted to be among those aged 85 years and older.1–4 A growing number of people will die of old age after a long period of living with multiple chronic life-limiting conditions. 5 Most older people will experience complex needs and will, at some point, require long-term care in a nursing home.6,7 In Europe, between 12% and 38% of older people die in a nursing home and this number is expected to increase in the future. 8 In addition, the median survival after admission to a nursing home is decreasing, 9 implying that almost all residents of nursing homes can be considered to be at the end of life, making palliative care the most appropriate care approach for this population.
Nursing homes, instead struggle to meet the palliative care needs of their residents. Many residents suffer from distressing symptoms such as pain, dyspnea and depression and have unmet needs regarding physician communication, emotional support and respectful care.10–14 Educational gaps in staff training have been identified as an important barrier to high-quality care.15–18 Qualitative and small-scale studies performed in Denmark, Ireland and England indicate that nursing home staff may have poor knowledge of palliative care and of pain and other symptoms control.19–23 Although nursing home staff have a lot of experience in caring for dying residents, they often lack formal training in palliative care. Clear evidence regarding the current palliative care knowledge of nursing home staff and the factors associated with such knowledge is required in order to develop effective training strategies.
To date, no international comparative study has been conducted in this field. PACE (Palliative Care for Older People) is a multi-country, EU-funded project that has set out, among other goals, comparative research on nursing home staff knowledge regarding palliative care, and on the factors associated with the level of such knowledge. There is a large diversity in the degree in which palliative care is developed and implemented in the six countries in the PACE project (Belgium, the Netherlands, England, Finland, Poland and Italy). The work by Froggatt et al. 24 demonstrates that in Belgium, the Netherlands and England, a wide range of initiatives exist on macro, meso and micro levels to develop palliative care in nursing homes and that there is evidence of large proportions of nursing homes providing palliative care for residents in those countries. In Poland, and especially in Italy and Finland, hardly any initiatives exist to develop palliative care in nursing homes and there is no evidence of engagement by and within nursing homes with palliative care initiatives or care provision. 24 The six countries in the PACE project thus reflect a variety of palliative care structures, organizational models and policies, and different stages of development and implementation of palliative care in nursing homes, 24 which makes an international comparison of particular interest.
The aim of this study is to (1) document and compare the palliative care knowledge of nursing home staff (nurses and care assistants) in Belgium, the Netherlands, England, Finland, Poland and Italy and (2) identify which country, facility and staff factors are associated with such knowledge.
Methods
Study design
In 2015, we conducted a cross-sectional study in nursing homes in Belgium (Flanders), the Netherlands, England, Finland, Italy and Poland. In the nursing home setting, registered nurses and care assistants usually deliver most of the direct care. For each participating nursing home, the administrator was asked to fill out a questionnaire on facility characteristics. A questionnaire on staff knowledge of palliative care was distributed among all nurses and care assistants who were present or on duty in the nursing home at the time a study researcher visited the facility.
Sampling of nursing homes
Nursing homes were selected using proportional stratified random sampling, taking into account region, facility type and bed capacity, using publicly available lists of nursing homes in all countries except Italy, where no public list of nursing homes is available; a convenience sample was used there, based on a previously constructed cluster of nursing homes, covering the three macro regional areas of Italy and taking into account different size and type of facilities existing in the country. In England, nursing home recruitment was enhanced using the nationwide ENRICH research network to increase participation.
Setting and participants
The term nursing home in this study refers to a long-term care facility for older people defined as ‘a collective institutional setting, where care is provided for older people who live there, 24 hours a day, seven days a week, for an undefined period of time’. 24 Indeed, these facilities have different names in different countries, for example, nursing homes, care homes, homes for the elderly or residential homes. Within the countries participating, three types of nursing homes can be defined: type 1 with on-site physicians and nurses/care assistants, type 2 with on-site nurses/care assistants and off-site physicians and type 3 with on-site care assistants and off-site nurses and physicians. 24
The staff members surveyed in this study are nurses and care assistants. Nurses are registered nurses in all countries. For Finland, the category also includes licenced practical nurses. Care assistants provide personal care and support the registered nurses, working under supervision in a team.
Data collection
Managers of the sampled nursing homes in each country received a letter introducing the project and asking for participation in the study; additional contact was made by phone or e-mail whenever deemed necessary. In each participating nursing home, a contact person was identified and appointed. This person listed all nurses and care assistants employed in the nursing home and on duty at the time of the visit by a study researcher. The contact person distributed questionnaires to all nurses and care assistants on such list with indications to returning them back within a month. Reminders were sent out by the contact person to ensure that respondents remained anonymous to the study researchers. Up to two reminders were sent to non-responders. All participants took part on a voluntary basis; hence, their written responses were taken as valid informed consent. Data collection procedure has been previously described in more detail. 25 In all participating countries, ethical approval was obtained from the respective committees. The Netherlands and Italy were exceptions, as the consulted committees judged that no formal ethics approval was necessary.
Measurements
Staff characteristics evaluated were age, gender, professional role, that is, care assistant or nurse, receipt of formal training in palliative care and number of years working in residential care.
Palliative care knowledge was measured using the subscale of the Palliative Care survey instrument 26 reflecting basic knowledge of palliative care that underpins care planning and decision making. It comprises three subscales: (1) end-of-life factors, reflecting knowledge of common end-of-life issues such as the management of weight loss and pain and the use of feeding tubes, (2) physical factors, reflecting knowledge of physical factors that can contribute to physical pain and (3) psychological factors, reflecting knowledge of psychological factors that can contribute to physical pain. The items of the Palliative Care survey are presented in Table 2. Mean scores on the subscales range between 0 and 1 with higher scores indicating better knowledge.
Analyses
All analyses were performed with SPSS 23. To take into account clustering of nursing home data, multilevel models were created for all analyses. Depending on the dependent variable – continuous, binary or categorical – generalized linear mixed models were designed with, respectively, normal, binomial or multinomial distribution, respectively. Country was included as a fixed effect in each model to test for differences between countries. Nursing home was included as a random effect in each model.
Multiple linear mixed model analyses were conducted to study the effect of the factors associated with staff knowledge. Factors entered in the models were country, facility type, professional role (i.e. care assistant or nurse), age, gender, years of experience in direct resident care and receipt of formal training in palliative care. Results are presented as estimated differences and 95% confidence intervals (CIs).
An alpha level of <0.05 defines the statistical significance.
Results
In the 322 participating nursing homes, 3392 staff were given a questionnaire. Of these, 2275 were returned (response rate 67.1%), 53% of the respondents were nurses and 47% were care assistants. Response rate in each of the six countries is reported in Supplementary Figure 1.
Characteristics of the study population
In all six countries, the majority of the respondents were older than 35 years, except in Italy where nursing staff appeared significantly younger (p < 0.001) and had fewer years of experience in direct patient care (p < 0.001; Table 1). In most countries, care assistants were more prevalent: 85.8% in the Netherlands, 77.2% in England, 58.9% in Poland and 53.1% in Belgium. In Italy, the questionnaire was answered almost entirely by registered nurses alone (99.4%, p < 0.001), while in Finland, the majority of the respondents were licenced practical nurses (68.9%). In all countries, the majority reported having had some education in palliative care, but there were significant differences between the countries. Staff in Belgium had participated in training in palliative care (74.3%) significantly more often than staff in any other country.
Characteristics of the participating nurses and care assistants.
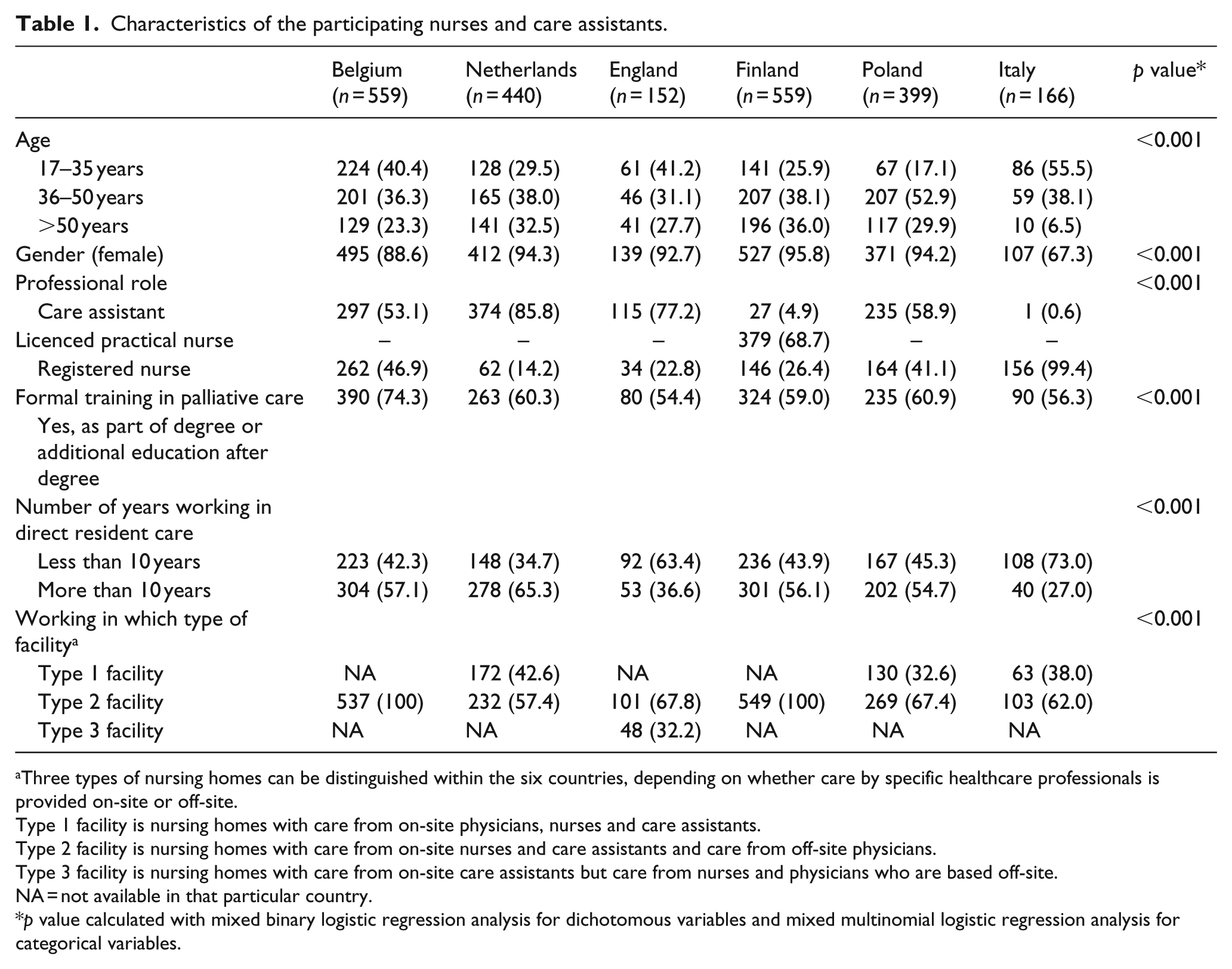
Three types of nursing homes can be distinguished within the six countries, depending on whether care by specific healthcare professionals is provided on-site or off-site.
Type 1 facility is nursing homes with care from on-site physicians, nurses and care assistants.
Type 2 facility is nursing homes with care from on-site nurses and care assistants and care from off-site physicians.
Type 3 facility is nursing homes with care from on-site care assistants but care from nurses and physicians who are based off-site.
NA = not available in that particular country.
p value calculated with mixed binary logistic regression analysis for dichotomous variables and mixed multinomial logistic regression analysis for categorical variables.
Nursing home staff knowledge of palliative care in the six countries
Knowledge about common palliative care issues such as pain, breathing and nutrition, measured with the subscale of ‘end-of-life factors’ ranged between 0.20 in Poland (95% CI 0.19; 0.24) and 0.61 in Belgium (95% CI 0.59; 0.63; Figure 1). Knowledge of physical aspects of disease or care that can contribute to pain measured with the subscale of ‘physical factors’ ranged between 0.81 (95% CI 0.79; 0.84) in Poland and 0.91 (95% CI 0.89; 0.93) in the Netherlands (Figure 2). Knowledge of psychological factors that can contribute to pain measured with the subscale of ‘psychological factors’ ranged between 0.56 in England (95% CI 0.50; 0.62) and 0.87 in Finland (95% CI 0.83; 0.90; Figure 3). Staff knowledge scores did not differ by facility type in any country (data not shown). However, there were significant differences between nurses and care assistants in all six countries, with nurses having higher knowledge scores than care assistants on all three subscales (Figures 1 to 3).
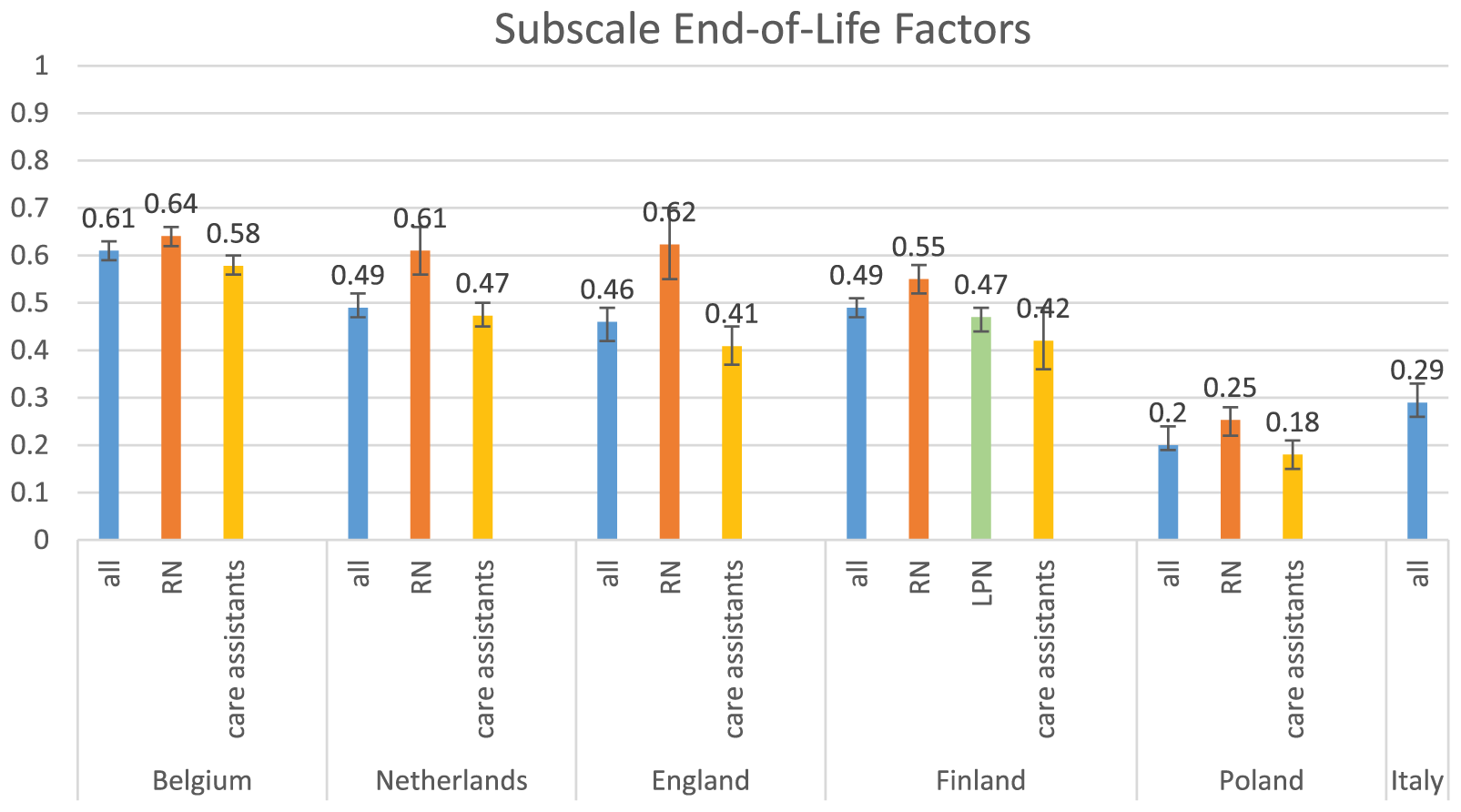
Knowledge of nursing home staff about end-of-life factors.
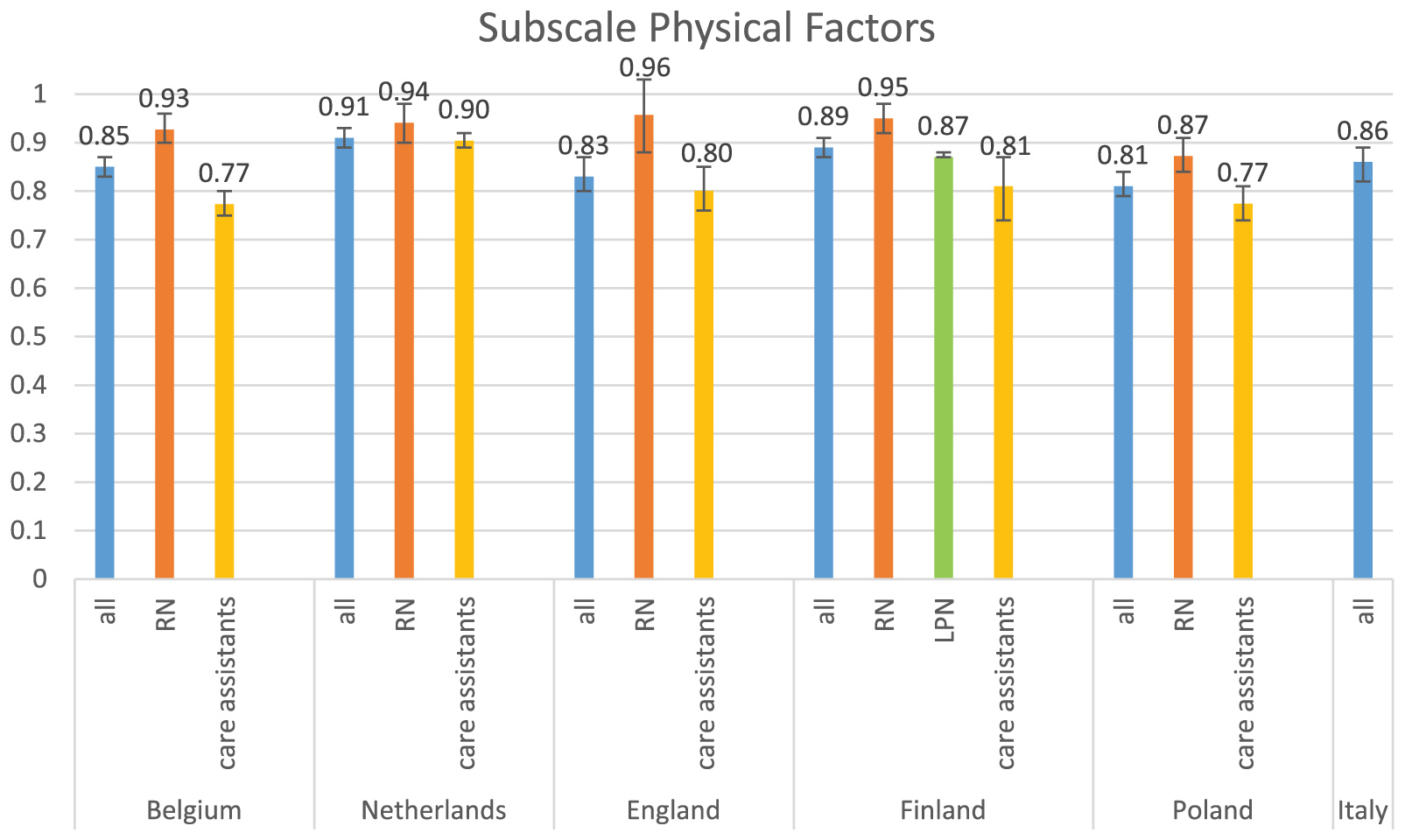
Knowledge of nursing home staff about physical factors that can contribute to pain.
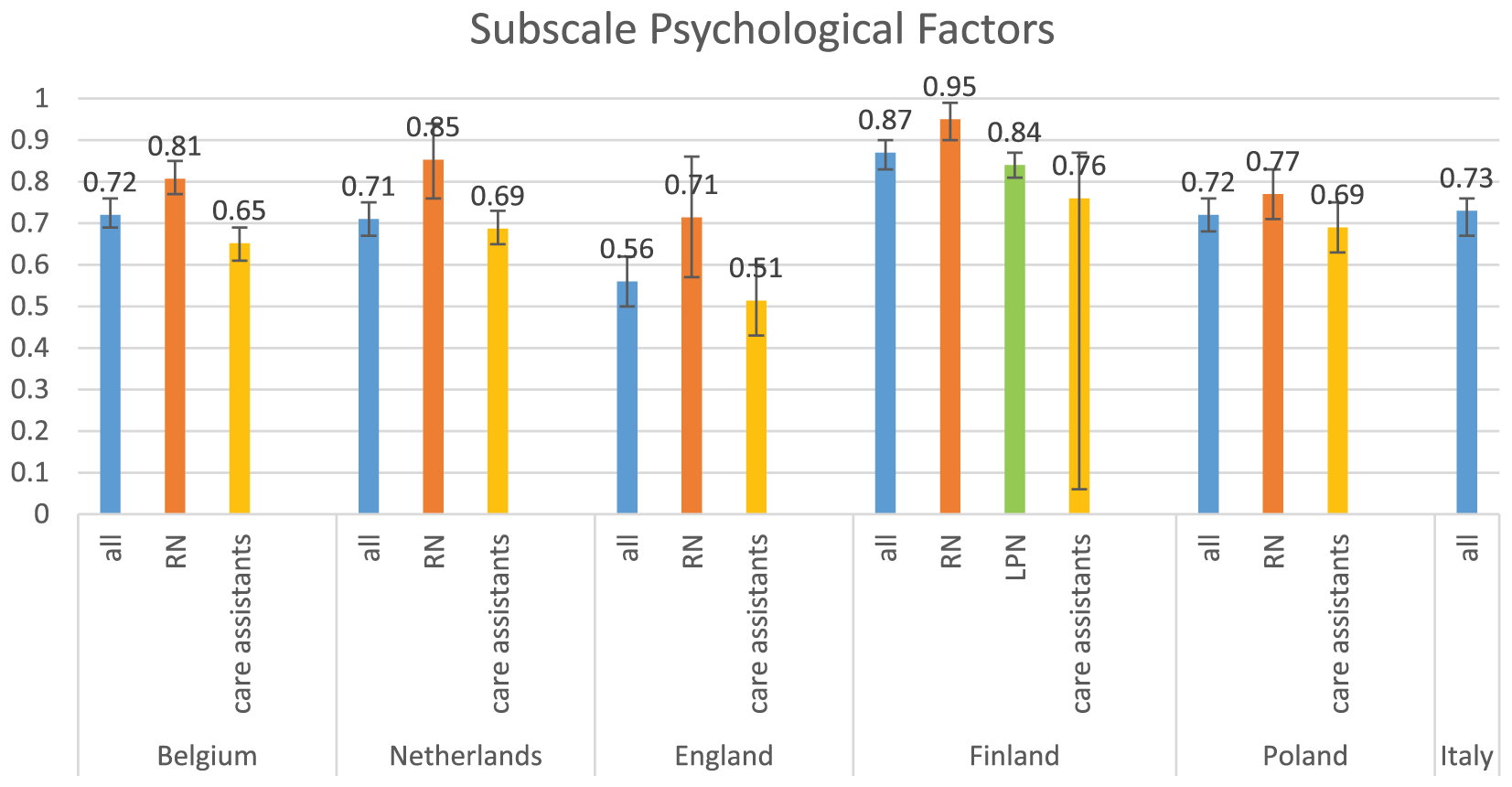
Knowledge of nursing home staff about psychological factors that can contribute to pain.
Substantial differences emerged when analysing responses to the different items of the Palliative Care Survey (Table 2). The proportion of nursing staff correctly disagreeing on feeding tubes prolonging life ranged between 15.1% in Poland to 69.9% in Belgium (Table 2). With the exception of Finland where 72.4% of the staff knew that addiction is not a problem with pain medications in palliative patients, less than half of the nursing staff in the other countries appeared to know it (Table 2).
Percentage of correct answers of nursing home staff on knowledge items of the Palliative Care Survey in the six countries.
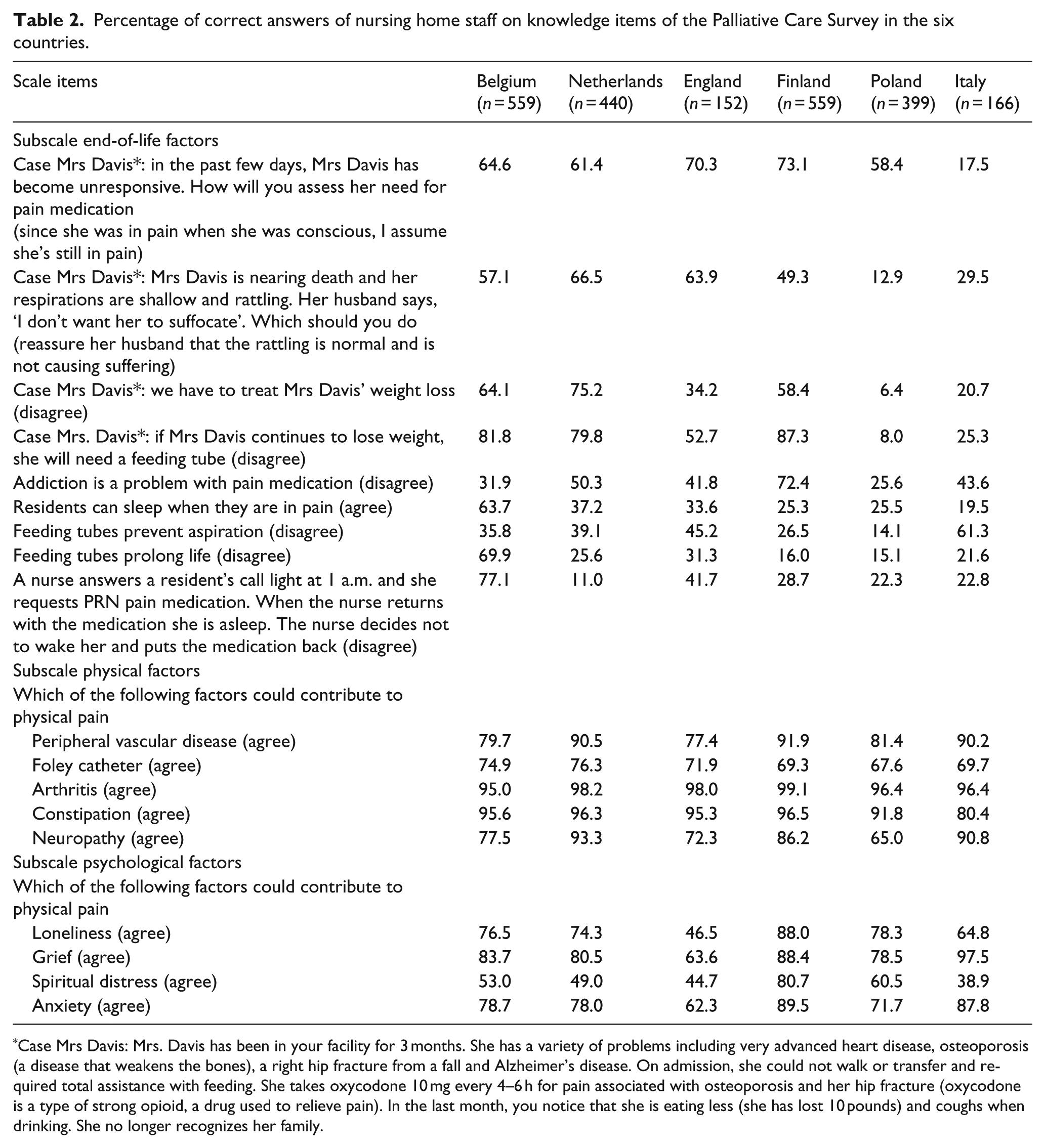
Case Mrs Davis: Mrs. Davis has been in your facility for 3 months. She has a variety of problems including very advanced heart disease, osteoporosis (a disease that weakens the bones), a right hip fracture from a fall and Alzheimer’s disease. On admission, she could not walk or transfer and required total assistance with feeding. She takes oxycodone 10 mg every 4–6 h for pain associated with osteoporosis and her hip fracture (oxycodone is a type of strong opioid, a drug used to relieve pain). In the last month, you notice that she is eating less (she has lost 10 pounds) and coughs when drinking. She no longer recognizes her family.
Factors associated with palliative care knowledge
Factors significantly associated with palliative care knowledge of nursing staff (in all three subscales) were country, professional role of the staff – with nurses having more knowledge than care assistants – and receipt of formal training in palliative care as part of their basic qualification or as additional training (Table 3).
Mixed linear regression analyses of factors associated with staff knowledge of palliative care.
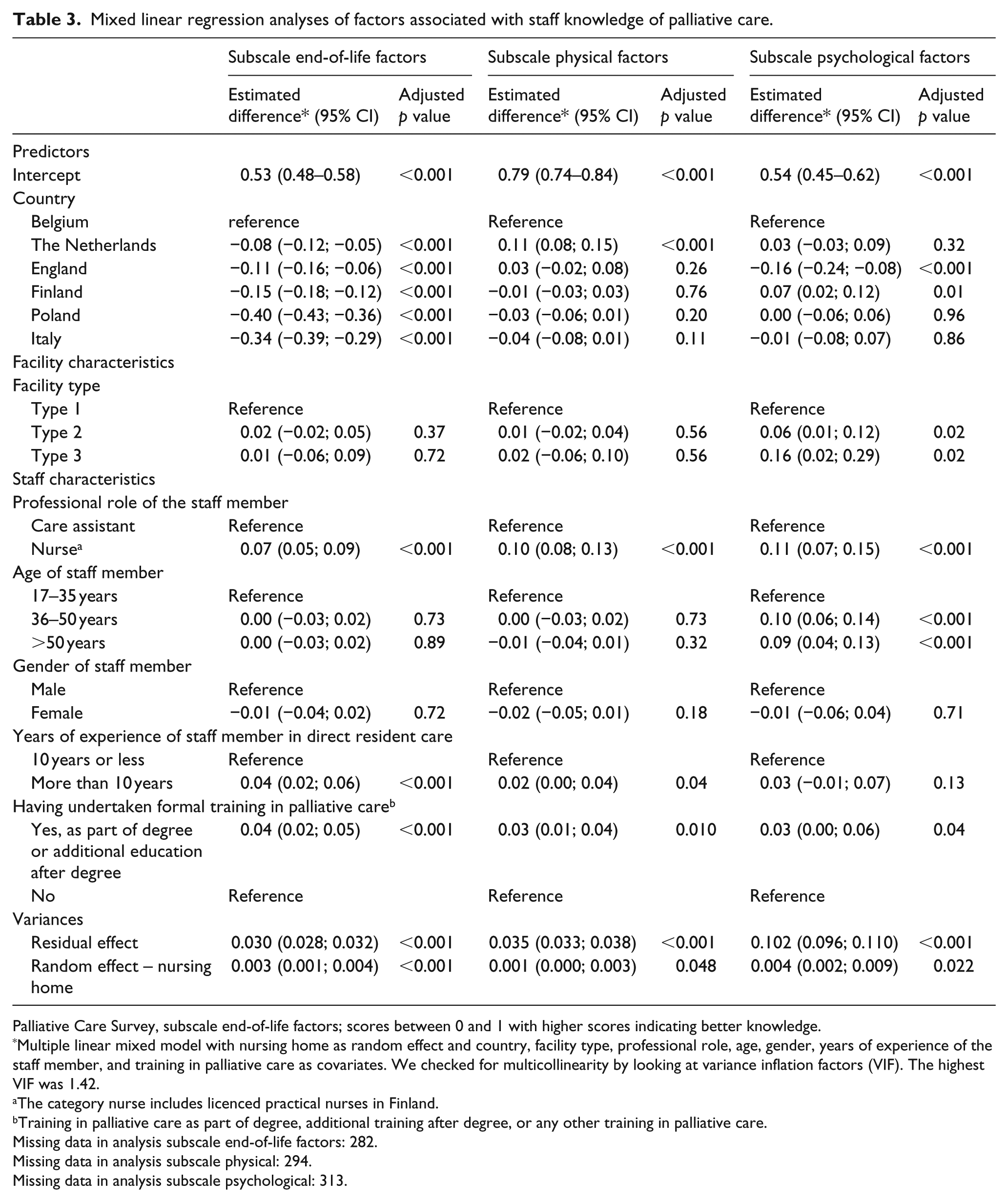
Palliative Care Survey, subscale end-of-life factors; scores between 0 and 1 with higher scores indicating better knowledge.
Multiple linear mixed model with nursing home as random effect and country, facility type, professional role, age, gender, years of experience of the staff member, and training in palliative care as covariates. We checked for multicollinearity by looking at variance inflation factors (VIF). The highest VIF was 1.42.
The category nurse includes licenced practical nurses in Finland.
Training in palliative care as part of degree, additional training after degree, or any other training in palliative care.
Missing data in analysis subscale end-of-life factors: 282.
Missing data in analysis subscale physical: 294.
Missing data in analysis subscale psychological: 313.
Adjusting for differences in facility type, professional role of the staff, age, gender, years of experience and receipt of training in palliative care, country remained significantly associated with palliative care knowledge. Nursing home staff in Belgium appeared to have more knowledge about common issues concerning palliative care than staff in any other country (p < 0.001). Staff in the Netherlands appeared to have more knowledge about physical aspects that can contribute to pain than staff in any other country, while staff in Finland had significantly more knowledge about psychological reasons that can contribute to pain than staff in Belgium (estimated difference 0.07; 95% CI 0.02; 0.12, p = 0.01).
As expected, nurses appeared to have better knowledge than care assistants (p < 0.001 on the three subscales), as did those who had undertaken training in palliative care (p < 0.001 on subscale end-of-life factors, p = 0.010 on subscale physical factors and p = 0.04 on subscale psychological factors).
Better palliative care knowledge was associated with the number of years of experience in direct residential care. Staff who had more than 10 years of experience had more knowledge than those with fewer years of experience (estimated difference 0.04; 95% CI 0.02–0.06; p < 0.001).
Furthermore, better knowledge about psychological factors contributing to pain was associated with facility type and with nursing staff age. Staff members working in type 2 or 3 facilities and those older than 35 years appeared to have better knowledge than those working in a type 1 facility (p = 0.2) and those younger than 35 years (p < 0.001; Table 3).
Discussion
Main findings
The results of this study document that knowledge of important palliative care issues such as management of pain or weight loss or the use of feeding tubes is generally poor among nurses and care assistants in all six participating EU countries. However, substantial variations are evident across countries. Palliative care knowledge appears to be particularly deficient among staff in Poland and in Italy. In all countries, knowledge about psychological and especially about physical factors contributing to pain is better than the knowledge on other common palliative care issues. Nurses have better knowledge than care assistants, and that applies to those having undertaken formal training in palliative care.
Strengths and limitations of the study
This study is the first large-scale study assessing palliative care knowledge of nurses and care assistants across six European countries. We were able to compare data from 2275 individual nursing staff members from 322 nationally representative nursing homes in six EU countries.
However, the study has also some limitations. First, even though we conducted a rigorous sampling, it is possible that facilities with a special interest in palliative care were more prone to participate in the study. Although we cannot dismiss it completely, this limitation is always present in large-scale representative surveys. Second, despite high response rates achieved in most countries, this was not the case for the Netherlands (51.7%) and especially for England (31%). Third, the Palliative Care Survey covers basic aspects of palliative care related to pain and symptom management, but not other important elements such as knowledge of psychosocial or existential aspects, communication, grief and bereavement or advance care planning. Finally, the use of a questionnaire to assess knowledge may induce bias as the respondents have the opportunity to look up the correct answers or to discuss the questions among each other.
What this study adds
All in all, this study highlights specific knowledge gaps. Although we found that many problematic issues are the same across countries, huge heterogeneity persists even after adjusting for confounders. Knowledge about basic palliative care issues is generally poor among nurses and care assistants in all countries, but particularly so in Poland and in Italy. A study of palliative care development in European care homes and nursing homes shows that there is a large variation in the degree to which palliative care is developed and implemented. 24 In Poland, and particularly in Italy, hardly any initiatives exist to develop palliative care in these settings and there is no evidence of engagement with palliative care initiatives by and within the care and nursing homes. 24 This may suggest that the degree of palliative care knowledge of nursing home staff is influenced by the availability of palliative care services and initiatives in the nursing home and by the extent of national policy and investment in palliative care development in the nursing home setting.
As expected, we found that in all countries nurses have better palliative care knowledge than care assistants. These results are in agreement with previous research by Unroe 27 in the United States and Ronaldson 28 in Australia. This reflects differences in palliative care education, and differences in roles and levels of care responsibilities.29,30 Care assistants often work under the supervision of a nurse and their direct care responsibilities are limited. However, as most direct care in nursing homes is provided by care assistants, they are in an ideal position to note clinical changes and to assess and address a resident’s needs, making knowledge of palliative care extremely relevant to them. A White Paper of the European Association for Palliative Care on palliative care education identifies nursing homes as a setting in which the staff, irrespective of their discipline, need to know the basic principles of palliative care. 31 This implies that all levels of staff need to be able to provide high-quality care to residents at the end of life. In this respect, this study shows very clearly that there is a strong need to further invest in basic palliative care knowledge and skills, especially for care assistants.
The results of this study provide insights into the specific knowledge gaps of the nursing staff in the six participating countries and also serve as a starting point for developing the most appropriate training. This should at least focus on basic palliative and end-of-life care issues such as the assessment and management of weight loss, death rattle, pain and the use of feeding tubes, but may need to be further extended to include other elements not considered in this study. Given the high staff turnover rate in the nursing home setting, continuous in-house education should also be implemented alongside the integration of palliative and end-of-life care in all curricula for future nurses and care assistants. To be effective, training initiatives should be embedded in a broad organizational approach.32–36 Envisioned management is essential to create a work environment that is supportive of staff members developing a leading role around palliative care.32–36 This means that there needs to be attention to staff motivation, adequate planning and that resources are made available to implement new improvement initiatives.37–39 Other factors impacting on the effectiveness of training strategies are in-person training, certification of implementation champions, providing opportunities for bedside learning, easier access to continuing education, cover to allow staff to attend training sessions and opportunities to assimilate new knowledge and to practice new working methods.36,39,40
Conclusion
While many factors have been identified as barriers to providing palliative care in nursing homes, this study focused on palliative care knowledge of nurses and care assistants being the most important professionals in these settings. We found that knowledge of basic palliative care issues such as the management of pain or weight loss or the use of feeding tubes is generally poor in all six studied countries although there are large variations across. Given the expected increase in the number of older people in nursing homes with palliative care needs, the provision of adequate training and education in palliative care to nursing home staff should be a high public health priority.
Footnotes
Acknowledgements
We thank all nursing homes and their staff for participating in this project. For Poland, we also acknowledge the Ministry of Science and Higher Education of Poland (decision NR3202/7.PR/2014/2 dated 25 November 2014). We also thank the ENRICH network for their support of the UK research team. Finally, we thank Roos Colman for her advice on data analysis and Jane Ruthven for her language editing. All authors were involved in either the study design, data acquisition or data analysis; all authors were involved in interpretation of data and writing of the manuscript, and take responsibility for the integrity of the data and the accuracy of the data analysis. *Other PACE collaborators not in the author list: Zeger De Groote, Federica. Mammarella, Martina Mercuri, Mariska Oosterveld-Vlug, Ilona Barańska, Paola Rossi, Ivan Segat, Eleanor Sowerby, Agata Stodolska, Hein van Hout, Anne Wichmann, Eddy Adang, Paula Andreasen, Danni Collingridge Moore, Harriet Finne-Soveri, Katherine Froggatt, Agnieszka Pac, Violetta Kijowska, Bregje Onwuteaka-Philipsen, Maud ten Koppel, Nele Van Den Noortgate, Jenny T. van der Steen, Myrra Vernooij-Dassen, and the European Association for Palliative Care Onlus, European Forum For Primary Care, Age Platform Europe and Alzheimer Europe.
Data sharing
No additional data available.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the European Union’s Seventh Framework Programme (FP7/ 2007e2013) under Grant agreement 603111 (PACE project Palliative Care for Older People). The project was co-funded by Polish Ministry of Science and Higher Education in the years 2014-2019 based on the decision no 3202/7PR/2014/2 dated on Nov. 25th, 2014. The funders had no role in study design, collection, analysis or interpretation of the data, nor in writing and the decision to submit this article for publication.
Research ethics
The research teams in all participating countries obtained ethical approval from their respective ethics committees. The Netherlands and Italy were exceptions, as the consulted ethics committees in these countries judged that no formal ethics approval was needed and provided waivers. Belgium: Commissie Medische Ethiek UZBrussel (B.U.N. 14321422845), 17/12/2014. England: NHS – NRES Committee North West-Haydock (15/NW/0205), 10/03/2015. Finland: Terveyden jahyvinvoinnin laitos, Institutet för hälsa och välfärd (1/2015) 2/2/2015. Italy: Universita Cattolica del Sacro Cuore. Netherlands: Medisch Ethische Toetsingscommissie VUMedisch Centrum, 29/1/2015. Poland: Komisja Bioetycza, Uniwersytetu Jagiellonskiego (122.6120.11.2015), 29/1/2015.