
Abstract
Design
A qualitative study using uni-professional focus groups, forming the first stage of a multi-phase co-design project to develop a model of care for early sling removal after conservatively managed proximal humerus fracture.
Setting
Focus groups were conducted online via Microsoft Teams with participants from a wide geographical spread across multiple United Kingdom National Health Service Trusts.
Participants
Healthcare professionals (n = 23), including orthopaedic surgeons, therapists (physio and occupational), and nurses, recruited through purposive sampling.
Intervention
Three focus groups explored healthcare professionals’ perspectives on early sling removal in the non-operative management of proximal humerus fractures. Patient and public involvement and engagement work informed study design, identifying the need to first understand professionals’ viewpoints before engaging patients and progressing to consensus co-design.
Main measures
Data were collected through focus groups supported by pre-session forms and analysed thematically following Braun and Clarke's framework using NVivo software.
Results
Three overarching themes were identified: Navigating pain and fear, clinician confidence, and early engagement. Fear of patient harm and high pain levels in the early weeks were barriers to early sling removal. Confidence was influenced by experience, fracture severity and limited evidence, with hierarchical decision-making by surgeons. Participants considered enablers to be consistent messaging, early education, and reassurance to support both clinicians and patients.
Conclusions
Whilst healthcare professionals recognise benefits of earlier sling removal, implementation is limited by pain, uncertainty, and hierarchical decision-making. These findings highlight the need for multidisciplinary, co-designed pathways. There is a need next to explore patient perspectives to inform future co-designed pathways.
Keywords
Introduction
Proximal humerus fractures account for 5%–6% of all adult fractures, 1 with an estimated 706,000 occurring worldwide annually. 2 Traditionally, treatment has consisted of either surgery (fracture fixation or arthroplasty), 3 or conservative management formed of sling immobilisation and physiotherapy. Delivery of treatment for this patient group can be via multiple healthcare professionals, including orthopaedic surgeons, nurses, physiotherapists and occupational therapists, whose roles often overlap across accident and emergency and fracture clinic settings. Any change in practice, therefore, requires engagement from all groups.
A randomised controlled trial showed that surgery was no more effective than conservative management for proximal humerus fractures and is less cost-effective, thereby supporting conservative management as a favoured approach. 4 However, there is limited evidence to guide what conservative management should entail. A systematic review synthesising the evidence for conservative management found there was vast variation in how long patients were immobilised for, types of slings used and when and how exercises were introduced and progressed. No relationship was found between complications and these components. 5
About a week after a bone breaks, the haematoma (blood clot) which forms at the fracture site starts to organise. This leads to the formation of a soft callus, which helps stabilise the broken bone, 6 a stage often associated with reduced pain and the opportunity to introduce gentle rehabilitation, whereas rigid immobilisation may inhibit callus formation. 7 Prolonged sling use can be associated with increased pain, stiffness, delayed return to function and also represent a burden on health care systems including hospital length of stay and social care needs. 8 Despite this, sling use is still often recommended for up to six weeks. 5 The term early sling removal lacks a standardised definition within current evidence or practice, necessitating investigation of clinicians’ perspectives on its timing and implementation. Protocols for managing this patient group are often historical, and the reasons why emerging evidence has not translated into practice remain unclear.
Despite growing interest in reducing immobilisation after proximal humerus fracture, implementation of earlier sling removal in routine practice remains inconsistent. Existing literature has predominantly focused on clinical and functional outcomes, with limited attention to how professional roles, responsibilities, and decision-making structures shape immobilisation advice and rehabilitation timing. Clarifying how clinicians conceptualise and operationalise this early phase is necessary for optimisation of intervention fidelity, thereby enabling more rigorous evaluation.
Given that early sling removal is potentially appropriate and could provide benefits to patients, this study aims to explore the views of healthcare professionals involved in the conservative management of proximal humerus fractures and to identify barriers and enablers to routinely offering early sling removal.
Methodology
Ethical approval was granted by the University of Leicester Health, Biological and Psychological Sciences Research Ethics Committee on 3 February 2025 (project ID 1918). Informed consent was obtained electronically from all participants prior to study commencement.
Focus groups were used to explore healthcare professionals’ perspectives, facilitate interaction, and identify areas of convergence and divergence. These were undertaken uni-professionally to allow participants to speak openly among peers without the influence of hierarchical or inter-professional dynamics that may occur in mixed groups. 9 This approach also enables the identification of within-profession nuances to build a richer understanding of emerging barriers and enablers. The study was theoretically underpinned by interactionism, which emphasises how social interactions and shared experiences contribute to the construction of group understanding. 9
A diverse patient and public involvement and engagement group consisting of seven members who have experienced the injury or spent time in a sling was formed and utilised throughout this study. This group includes patients from a variety of ethnic and cultural backgrounds, from a diverse social background and includes members requiring care and assistance. An expert advisory panel of surgeons, physiotherapists, and patients was also convened to guide study progress and co-design. Early patient and public involvement and engagement work indicated that understanding healthcare professionals’ perspectives was a necessary first step, as their acceptance and confidence would be central to the successful implementation of any model of early sling removal. Healthcare professionals were identified as key stakeholders whose views needed to be explored independently from patients to avoid cross-influence and to ensure both perspectives could later be compared and integrated meaningfully in the co-design process.
The lead researcher, a female specialist physiotherapist undertaking a PhD with a strong interest in early mobilisation, acknowledged the potential for bias due to prior beliefs and professional background. Some participants were known to the researcher through previous networks; however, this familiarity did not influence the sampling process or the nature and openness of the discussions within the focus groups. Reflexivity was maintained through ongoing reflection and awareness of influence on data collection and interpretation. 10
A realist ontology and interpretivist epistemology guided the study. Realists believe there is an underlying reality, whilst acknowledging an external reality influenced by social and contextual factors. 11 The study aimed to uncover underlying rationales behind current practices. An inductive, interpretivist approach was used to understand participants’ experiences and meaning-making. 12
Eligible participants were National Health Service professionals involved in managing proximal humerus fractures. Purposive sampling aimed to capture diverse views across professions, grades, and regions. Recruitment ran from 4 to 22 February 2025 via social media (X) and professional networks, with participants completing an expression of interest form. Up to eight participants per group (total target = 24) were invited to uni-professional focus groups (surgeons, therapists, nurses). A recruitment target of up to eight participants per focus group was set, in line with recommended guidelines for ensuring adequate and manageable group sizes, 13 yielding a total potential sample of 24 participants.
The principles for deciding saturation in theory-based qualitative studies are outlined by Francis et al. 14 However, given the study's aim to explore the perspectives of three distinct professional groups, an a priori decision was made to conduct a minimum of three focus groups, regardless of whether data saturation was reached prior to this point. Saturation was concurrently monitored during analysis. This approach combined a priori sampling based on professional representation with ongoing assessment of thematic saturation.
Participants completed a pre-focus group form detailing their current management practices (sling type, duration, exercise timing, and influencing patient factors). This ensured insights into baseline practice and supported discussion. A topic guide (Supplemental File 1), refined and piloted with input from expert stakeholders and Patient and Public Involvement and Engagement group, was used to guide but not dictate discussion.
Focus groups were conducted via Microsoft Teams, lasting 60 min, and facilitated by the lead researcher (HT), with another researcher and a Patient and Public Involvement and Engagement member present as moderators. Sessions were audio recorded, transcribed verbatim, and pseudonymised (identifiers such as names and location of work were replaced with codes P1-23). Participants were aware of the facilitator's professional background.
Pre-focus group responses were analysed using deductive content analysis 15 to assess current practices. Focus group data was analysed using thematic analysis using Braun and Clarke's six-step framework. 16 NVivo software (2020, R1) was used to code, organise, and visualise data. A reflexive diary was maintained, and transcripts were member-checked by the Patient and Public Involvement and Engagement representative and peer debriefing amongst the research team. Initial coding was inductive, followed by iterative refinement incorporating deductive elements aligned to study objectives. 17 Themes were developed collaboratively with researchers and the Patient and Public Involvement and Engagement members.
The study is reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist. 18
Results
A total of 129 individuals completed the expression of interest form. Twenty-four were purposively sampled and consented; 23 attended focus groups comprising of seven therapists (four physiotherapists, three occupational therapists), eight orthopaedic surgeons, and eight nurses. One participant was unable to attend due to work commitments. Participants represented diverse regions across the United Kingdom, including Scotland, North West and South West England, Yorkshire and Humber, East of England, and London (Figure 1), and came from healthcare organisations of varying sizes and service capacities. All reported managing at least 10–50 proximal humerus fractures annually, with most treating 50–100, and two treating over 100 cases per year.
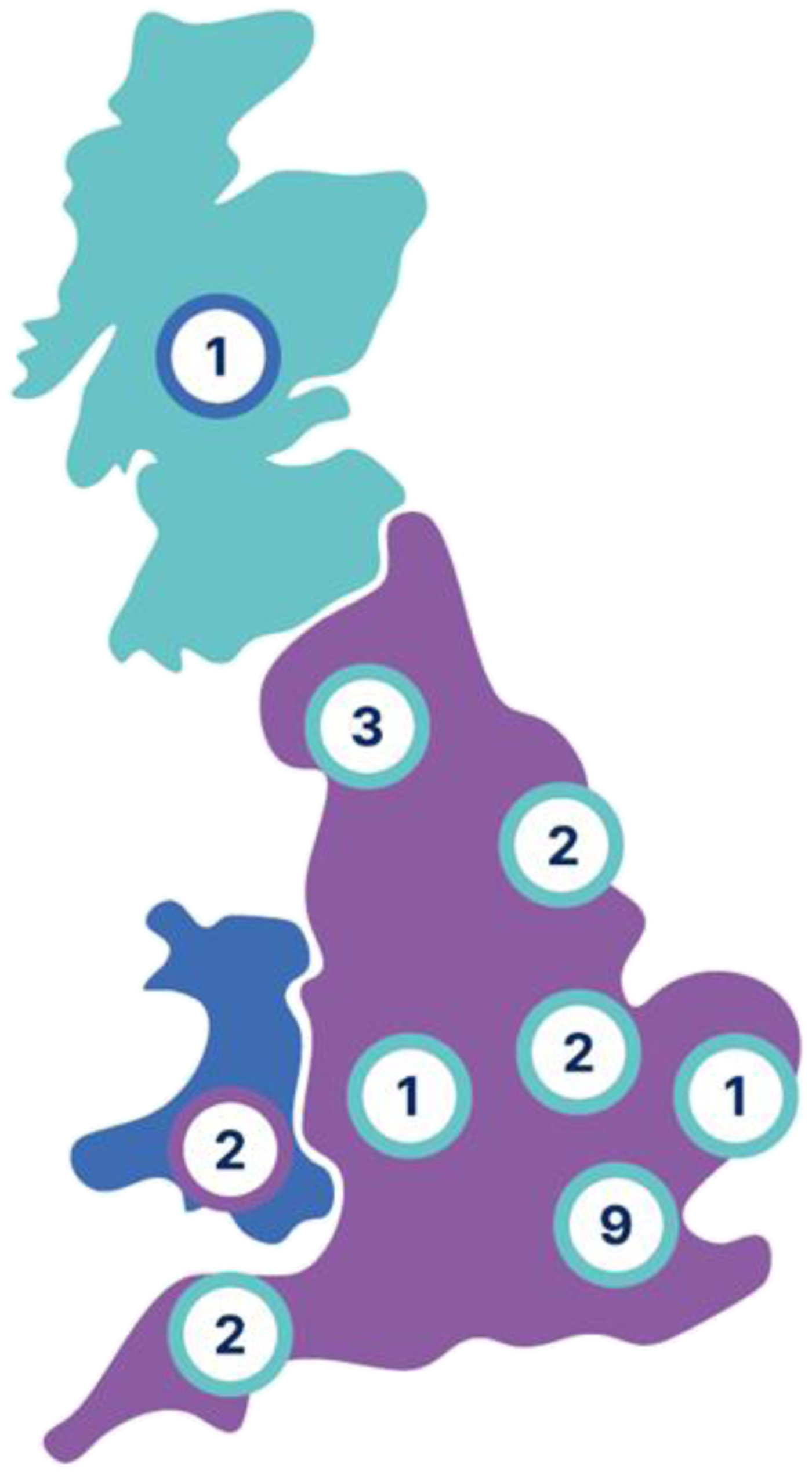
Sampling regional representation.
Pre-focus group responses revealed interprofessional variations in the management of proximal humerus fractures in terms of how long patients should remain in a sling and the terminology around rationale for sling use.
Focus group themes
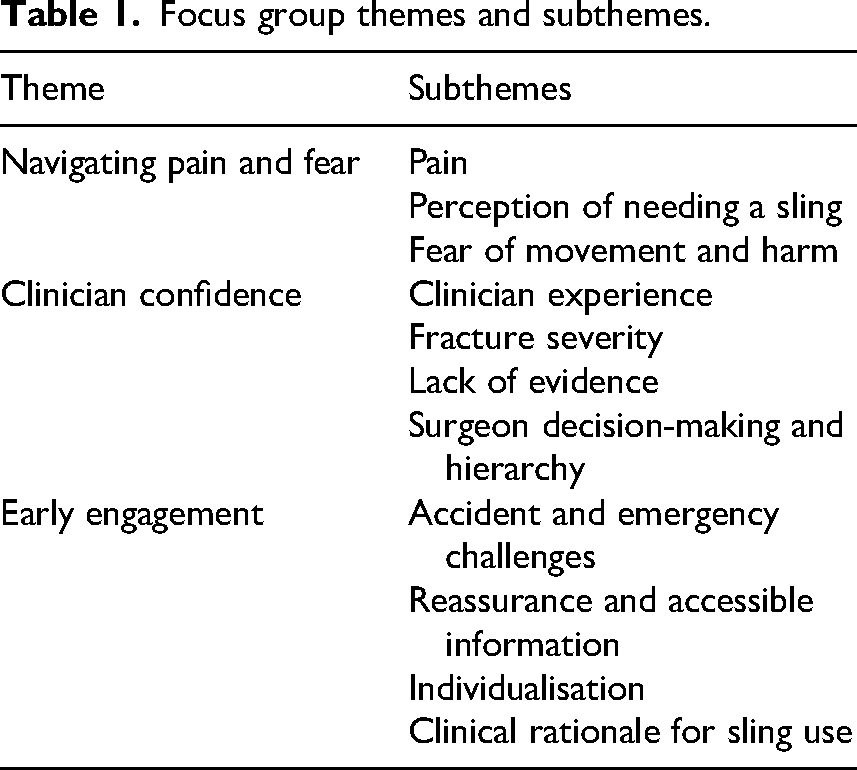
Initial analysis generated 36 codes across the three focus groups. Data saturation was achieved when no new themes or subthemes were generated beyond the second focus group. The third focus group confirmed thematic sufficiency across the three professional groups. Three overarching themes were developed regarding early sling removal across all profession groups, summarised in Table 1 (See Supplemental file 2 for visualisation of the themes).
Focus group themes and subthemes.
Theme 1: Navigating pain and fear
That first couple of weeks. My experiences, these patients struggle with pain…. They're really painful. I don't think I'd want to move it – P1 (therapist) Some patients believe more is better when it comes to immobilisation … and they feel safer in the sling. They've heard stories, or they just instinctively feel safer with the sling. Even when we explain the risks of stiffness, they sometimes cling to the perceived protection – P7 (therapist) … especially in some of the X-ray, the images are quite frightening to patients if they see them…. you've got an X-ray that can look pretty horrendous’ – P5 (therapist)
Theme 2: Clinician confidence
Nurses overall lacked confidence to encourage earlier sling removal, and felt that slings should not be removed before the four weeks stage. I think, doing it anything less than the four weeks it could actually prolong injury to the fractures. So I just stay based on the four weeks so that the fracture could heal fully – P18 (nurse) The most difficult thing is on the configuration of the fracture and the likelihood of displacement. Now I know we all like to think, oh, we can say this is stable from like day dot, but I think they do have the capacity to move and I think that's often why we bring them back at two weeks or even three or four weeks to check on an X-ray they haven't displaced – P15 (surgeon) I think if you were running a trial about early mobilisation versus not, I think you'd get really good buy in. And I think there'll be loads of surgeons who would want to have a good piece of evidence – P9 (surgeon) It's kind of stipulated by our consultants…. once they've had … an orthopaedic appointment and been given the green light from them – P5 (therapist)
Theme 3: Early engagement
I just think that is a common patient complaint, a patient is not given the proper education about the exercises or activity modifications – P10 (surgeon)
So trying to re-educate around, I'd rather you took your pain relief and started to get some gentle movement because actually you've been in pain, and holding your arm against your side isn't going to necessarily help us get better – P1 (therapist) By implementing early intervention strategies in A&E, streamlining follow-up care, and addressing patient anxiety, we can improve the outcomes for patients with proximal humerus fractures – P7 (therapist) what's acceptable to the patient in terms of removing the sling, maybe that's something you know an individual approach and as their pain allows might be a consideration – P5 (therapist)
Discussion
This study explores healthcare professionals’ views on early sling removal after proximal humerus fracture and highlights the multiple patient, clinician and system-level factors shaping practice. Pain and fear dominated decision-making. Healthcare professionals perceived the early post-injury period as highly painful, reinforcing patient expectations of prolonged sling use and heightening anxiety about movement and harm. These concerns led many to doubt that patients would accept earlier removal, particularly when X-rays appeared severe. This may represent a form of unconscious gatekeeping by healthcare professionals, thereby acting as an unintended barrier to practice change.
Clinician confidence also influenced practice. Less experienced staff (< five years qualified) and nurses tended to default to longer immobilisation, whilst more experienced healthcare professionals recognised uncertainty, particularly in the absence of clear protocols or robust evidence. Fracture severity and surgeon hierarchy further shaped practice. Increasing confidence may require clear guidance in the form of adaptable protocols or decision-making tools and education. The dominant role of surgeons in decision-making was apparent, confirming the hierarchical nature of orthopaedic care, suggesting that change efforts must target surgeon behaviour.
Early engagement was viewed as critical. Inadequate or conflicting information at the point of first contact was seen to heighten patient anxiety and immobilisation. Clear, consistent messages and timely reassurance were seen as key enablers of early sling removal, particularly when tailored to pain and function rather than rigid timelines. These findings underscore the importance of addressing both patient-level fears and system-level barriers through evidence-based guidance, clinician education, and early, consistent communication to support implementation of early sling removal. Future research should therefore focus on designing and testing early educational interventions, particularly in the acute care setting, that are capable of reducing fear, promoting consistent messaging across professional groups, and supporting patients to mobilise safely from the outset.
Current practice remains variable, with beliefs of healthcare professionals underpinning prolonged sling use. Despite research showing no increased complication rates with early mobilisation5,19,20 concerns about harm persist. A recent randomised controlled trial (including displaced fractures) demonstrated no complications when early mobilisation was introduced, 21 supporting the safety of this approach.
Although pain was recognised as a barrier to early sling removal by all healthcare professionals, discussion of pain management was limited, suggesting a potential oversight. Current literature largely overlooks pain control, focusing instead on physiotherapy timing. A Cochrane review by Handoll and Brorson 3 reported pain reduction with acetaminophen and NSAIDs, and Lefèvre-Colau et al. 22 found improved outcomes with unspecified oral analgesics. Many studies fail to detail pain medication use, including type, dosage, or duration. Effective pain relief strategies may be required to support early sling removal and should be examined in future research.
Preferences for sling type varied, with surgeons favouring collar-and-cuff slings for theoretical alignment via gravity and therapists reporting better comfort with broad arm slings. Patient comfort and adherence were acknowledged, indicating that patient involvement in sling selection warrants further exploration.
Strengths of this study include a multi-professional sample and broad geographical representation. Limitations relate to self-selection, meaning participants may be more invested in the topic than typical practitioners. The use of social media as a recruitment method may have also caused a bias on sampling of those who are more active on such platforms. The separation of the professional groups enabled participants to openly express their views amongst peers, however a further limitation of this may have been the inability to directly observe interactions and potential differences of opinions between professional groups. Further research is required to explore patient perspectives and evaluate implementation strategies, and bring all stakeholder groups together to codesign an intervention.
This study provides insights into the potential barriers and enablers of early sling removal, but further work is needed to answer questions presented:
Addressing these uncertainties will be central to developing a model of care that is safe, acceptable, and meaningful for both patients and clinicians.
In summary, healthcare professionals recognise the benefits of earlier sling removal but have concerns, particularly regarding patient fear, pain, and fracture severity. Surgeons play a central role in decision-making, indicating that behaviour change interventions may need to focus on this group. Guided by early patient and public involvement and engagement input, this study forms the first stage of a multi-phase co-design project, recognising that healthcare professionals’ perspectives are critical to the feasibility of routinely introducing early sling removal. Given that anticipated patient acceptance was a major concern, exploring patients’ views is planned as the next stage, enabling comparison of perspectives before progressing to co-design of a model of care.
See Supplemental file 3 for infographic of summary of findings.
Clinical messages
Healthcare professionals supported earlier sling removal but had concerns about pain, patient fear, and harm. Given surgeons’ key decision-making role, behaviour change efforts should target this group to support adoption of early sling removal care models
Consistent, evidence-informed messaging and early patient education are seen as essential to build confidence in healthcare professionals to support delivering early sling removal.
Understanding professional perspectives is a crucial first step in developing co-designed, patient-centred care pathways that address barriers of uncertainty and hierarchical decision-making.
Supplemental Material
sj-docx-1-cre-10.1177_02692155261437345 - Supplemental material for Healthcare professionals’ perspectives on early sling removal following conservatively managed proximal humerus fractures: A qualitative study
Supplemental material, sj-docx-1-cre-10.1177_02692155261437345 for Healthcare professionals’ perspectives on early sling removal following conservatively managed proximal humerus fractures: A qualitative study by Helen Tunnicliffe, Seth O’Neill, Sion Scott, Harvinder Singh and David Wright in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155261437345 - Supplemental material for Healthcare professionals’ perspectives on early sling removal following conservatively managed proximal humerus fractures: A qualitative study
Supplemental material, sj-docx-2-cre-10.1177_02692155261437345 for Healthcare professionals’ perspectives on early sling removal following conservatively managed proximal humerus fractures: A qualitative study by Helen Tunnicliffe, Seth O’Neill, Sion Scott, Harvinder Singh and David Wright in Clinical Rehabilitation
Supplemental Material
sj-pdf-3-cre-10.1177_02692155261437345 - Supplemental material for Healthcare professionals’ perspectives on early sling removal following conservatively managed proximal humerus fractures: A qualitative study
Supplemental material, sj-pdf-3-cre-10.1177_02692155261437345 for Healthcare professionals’ perspectives on early sling removal following conservatively managed proximal humerus fractures: A qualitative study by Helen Tunnicliffe, Seth O’Neill, Sion Scott, Harvinder Singh and David Wright in Clinical Rehabilitation
Footnotes
Ethical approval
Ethical approval was granted by the University of Leicester Health, Biological and Psychological Sciences Research Ethics Committee on 3 February 2025 (project ID 1918).
All participants completed informed consent forms.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Helen Tunnicliffe is funded by the National Institute for Healthcare Research Doctoral Clinical Academic Fellowship (grant number NIHR304095).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
De-identified transcript excerpts and NVivo codebooks are available from the corresponding author on reasonable request, in accordance with ethical approval and participant consent.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.