
Abstract
Objective
To synthesize research about clinical reasoning and decision-making among therapists in inpatient rehabilitation facilities about how they organize care and use their treatment time.
Data sources
PubMed, CINAHL, and PsycINFO were searched for relevant empirical studies published prior to January 13, 2026.
Review methods
Scoping review. The review process was organized using Covidence. Included studies featured descriptions of clinical decisions explained by occupational therapists, physical therapists, and speech therapists in inpatient rehabilitation facilities. Two reviewers coded the extracted themes through inductive analysis using Dedoose.
Results
Of 1239 articles identified through the search process, 51 met inclusion criteria. We identified six factors across studies that contributed to therapists’ clinical decision-making including: (1) consideration of non-medical circumstances (with sub-themes of understanding the patient's perspective, presence of families and caregivers, and assessment of patient resources); (2) collaboration and roles within care teams; (3) within-session communication techniques; (4) knowledge-base and the influence of experience; (5) medical and safety considerations; and (6) balancing institutional priorities within treatment. We created a concept map showing connections across these six factors.
Conclusion
The process of making decisions about therapy time and organization of care within inpatient rehabilitation settings is complex and requires integration of multiple factors. Therapists usually prefer familiar approaches to complex or time-intensive ones, and local culture shapes decision-making norms. Future research may examine how these factors relate to patient outcomes and implementation of practice changes such as introduction of new evidence-based treatments or assessment tools.
Keywords
Introduction
A primary goal of inpatient rehabilitation is to help patients regain enough functional independence to safely discharge to the community1,2 while reducing the risk of hospital readmissions.3,4 Patients admitted to inpatient rehabilitation facilities in the United States are supposed to receive three hours of therapy per day,1,5 divided among occupational therapy, physical therapy, and speech-language pathology. How this therapy time is divided among disciplines—and how therapists decide what to focus on in treatment—varies depending on the facility, the treatment team, and the needs of each patient.1,5,6
In addition to providing timely and effective rehabilitation care, facilities must also manage costs and adhere to government and institutional policies. Government policies shape what diagnoses can be treated in inpatient rehabilitation, the types of therapy services offered, and length of stay recommendations. 7 Clearly understanding the competing priorities therapists must consider on a day-to-day basis can help researchers identify different factors impacting patient outcomes and opportunities to alleviate routine challenges in practice.
Previous literature examining therapist decision-making in inpatient rehabilitation have primarily focused on decisions about admission, referrals, 8 assessment tool selection, goal-setting procedures, 9 and discharge planning.10,11 However, there has been less emphasis on exploring therapists’ real-time decision-making and clinical reasoning about treatment planning and service delivery. A longtime concern in the broader field of rehabilitation has been how to determine the components of effective treatment to strengthen the evidence-base. 12 To address this gap, this scoping review aims to synthesize existing literature on clinical decision-making by therapists in inpatient rehabilitation facilities about how to plan care and use treatment time.
Materials and methods
We conducted a scoping review of the literature following Arksey and O’Malley's methodological framework.13–16 This five-step approach includes: (a) identifying research questions; (b) identifying relevant studies; (c) selecting studies; (d) data extraction and charting; and (e) collation, summarization, and reporting of results. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews. 17 As this is a scoping review and not a systematic review, the protocol was not registered.
Stage 1: Identifying the research question
We used an iterative, team-based approach to develop and refine the research question.14,16 Our research question is: “What factors influence clinical decision-making for therapists in inpatient rehabilitation facilities?”.
Stage 2: Identifying relevant studies: sources and search strategy
We consulted a health research librarian to develop our search strategy. We searched PubMed, CINAHL, PsycINFO, and manually searched relevant review articles’ reference lists to identify eligible articles. Search terms are summarized in Table 1 (see also Supplemental Table 1). The search was updated through January 13, 2026.
Search strategy for PubMed database.
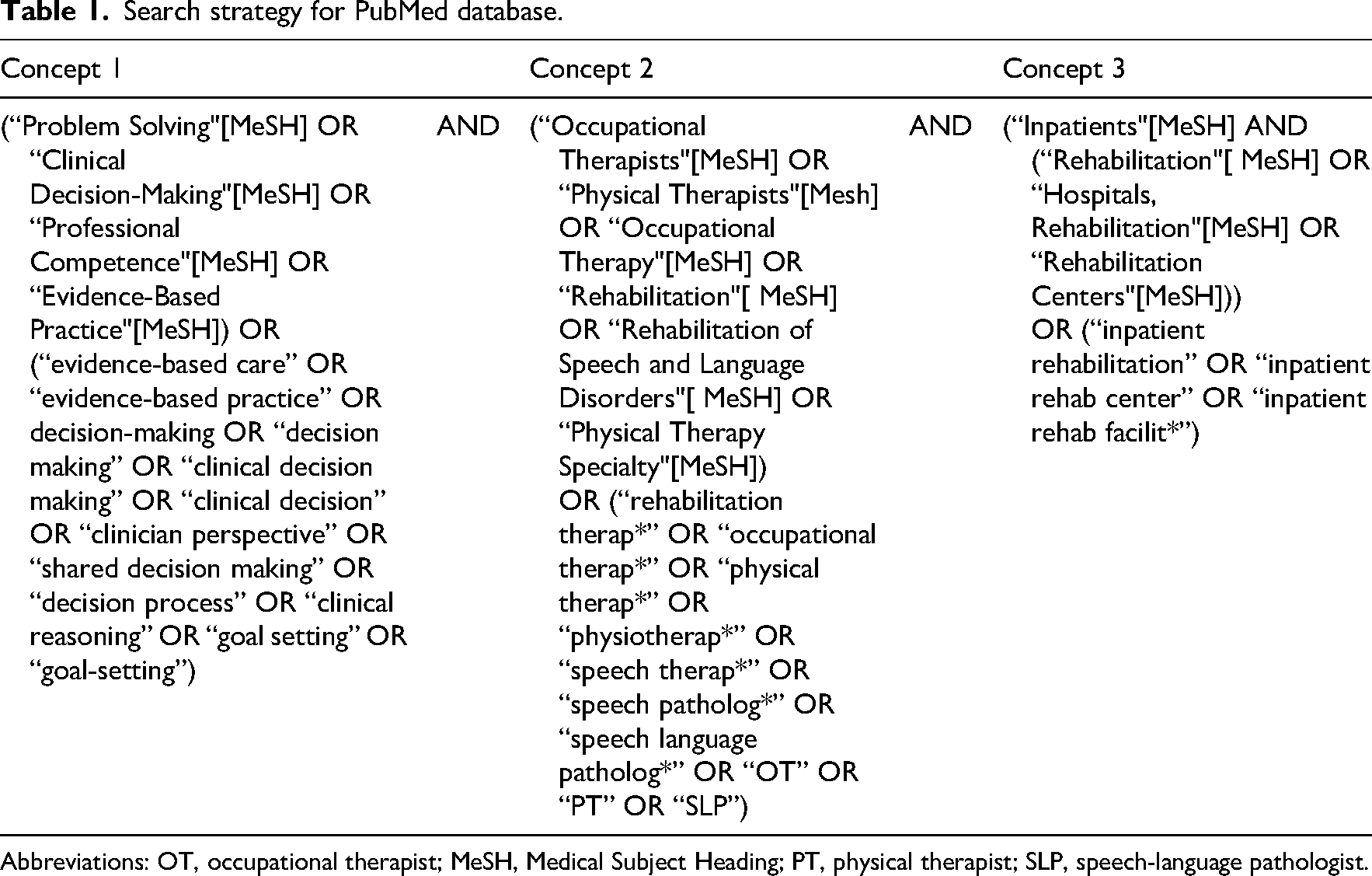
Abbreviations: OT, occupational therapist; MeSH, Medical Subject Heading; PT, physical therapist; SLP, speech-language pathologist.
Stage 3: Study selection
Studies were eligible if they described reasons behind clinical decisions for adult patients in an inpatient rehabilitation facility, and involved occupational therapists, physical therapists, or speech-language pathologists. Studies were excluded if they (a) did not pertain to the therapy process, (b) were review articles, (c) were not published in English, or (d) were not peer-reviewed. There were no restrictions on country or publication year. We used the United States Centers for Medicare and Medicaid Services’ definition of inpatient rehabilitation facilities: rehabilitation hospitals and units that provide intensive post-acute rehabilitation programs and require admitted patients to tolerate three hours of therapy per day. 18 We reviewed the content of articles published outside of the United States to determine whether inpatient setting requirements were comparable. We included articles with multidisciplinary teams when therapists’ perspectives could be distinguished from those of other team members.
We imported search results into Covidence 19 and removed duplicates. Two reviewers independently screened titles and abstracts for inclusion. In instances of disagreement, a third reviewer cast the deciding vote. The same process was followed for full-text reviews of articles that passed the initial screening. The first author re-reviewed articles throughout the study and involved the team in decisions, in line with recommended scoping review procedures.14,16
Step 4: Charting the data
We developed a data extraction template in Covidence that included: study title, publication year, authors, country, objective, study design, funding sources, therapist participants’ characteristics (sample size, profession, gender, years of experience), patients’ diagnoses, and data about clinical decisions. Clinical decision data included text describing therapists’ choices and the reasoning underlying those choices. Decisions included but were not limited to selections of treatment goals, practice settings, therapeutic activities or exercises, and communication strategies. Two reviewers extracted decision-related passages from each included article. The first and second authors conducted the final review and synthesized extracted data, which were then uploaded to Dedoose for thematic analysis. 20
Stage 5: Collating the data
We used a codebook approach21,22 to develop themes through inductive coding using Dedoose. 20 We chose inductive coding to represent the original sources’ meanings. 22 Each researcher independently assigned codes to segments of extracted data excerpts. Excerpts could contain multiple codes. A codebook approach provided a systematic way of refining codes and ensuring consistent interpretation of the data. 23 The first and second authors grouped codes describing similar phenomena into categories, which were iteratively revised in relation to the data as a whole. Throughout coding and theme development, we sought to preserve the context of the data, represent pragmatic choices and nuances within the decision-making process, and avoid assumptions about the intent behind therapists’ decisions. Our team reached consensus on themes and sub-themes by discussing discrepancies in interpretation.
Results
Of the 1239 articles identified through our search process, we included 51 in our analysis (Figure 1). Thirty-two were qualitative studies, nine used mixed methods, five were quantitative, and five were case reports (Table 2). Included studies were conducted in the United States (n = 16), Australia (n = 11), the United Kingdom (n = 7), Canada (n = 5), New Zealand (n = 4), the Netherlands (n = 1), Portugal (n = 1), Finland (n = 1), Iceland (n = 1), Japan (n = 1), Norway (n = 1), Switzerland, Austria, and Germany (n = 1), and Belgium and the Netherlands (n = 1). Thirty-four studies included only therapists, whereas 17 studies included therapists plus other rehabilitation team members. Therapist sample size varied widely (range: n = 1–174).
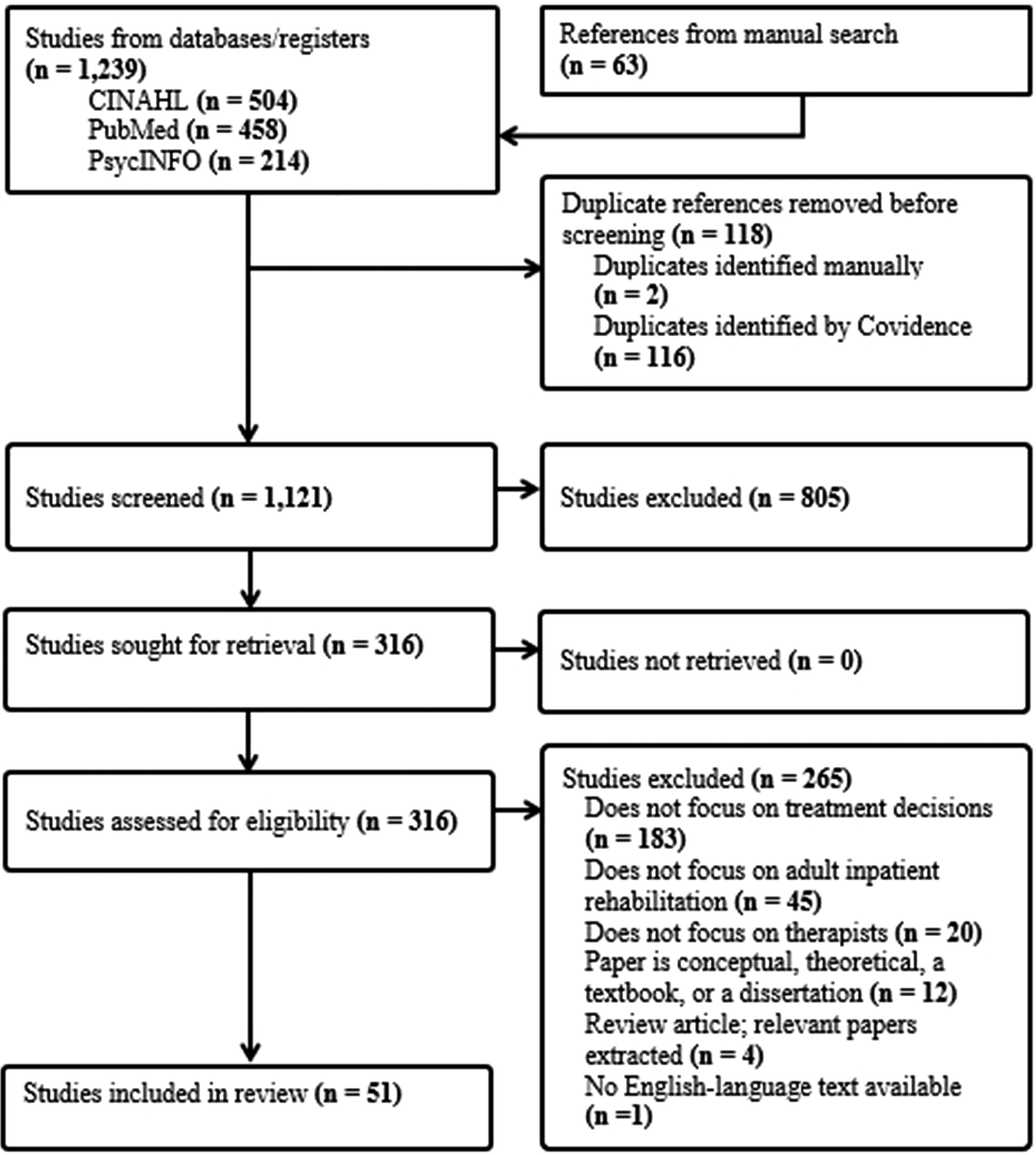
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart. 17
Study characteristics and corresponding themes.
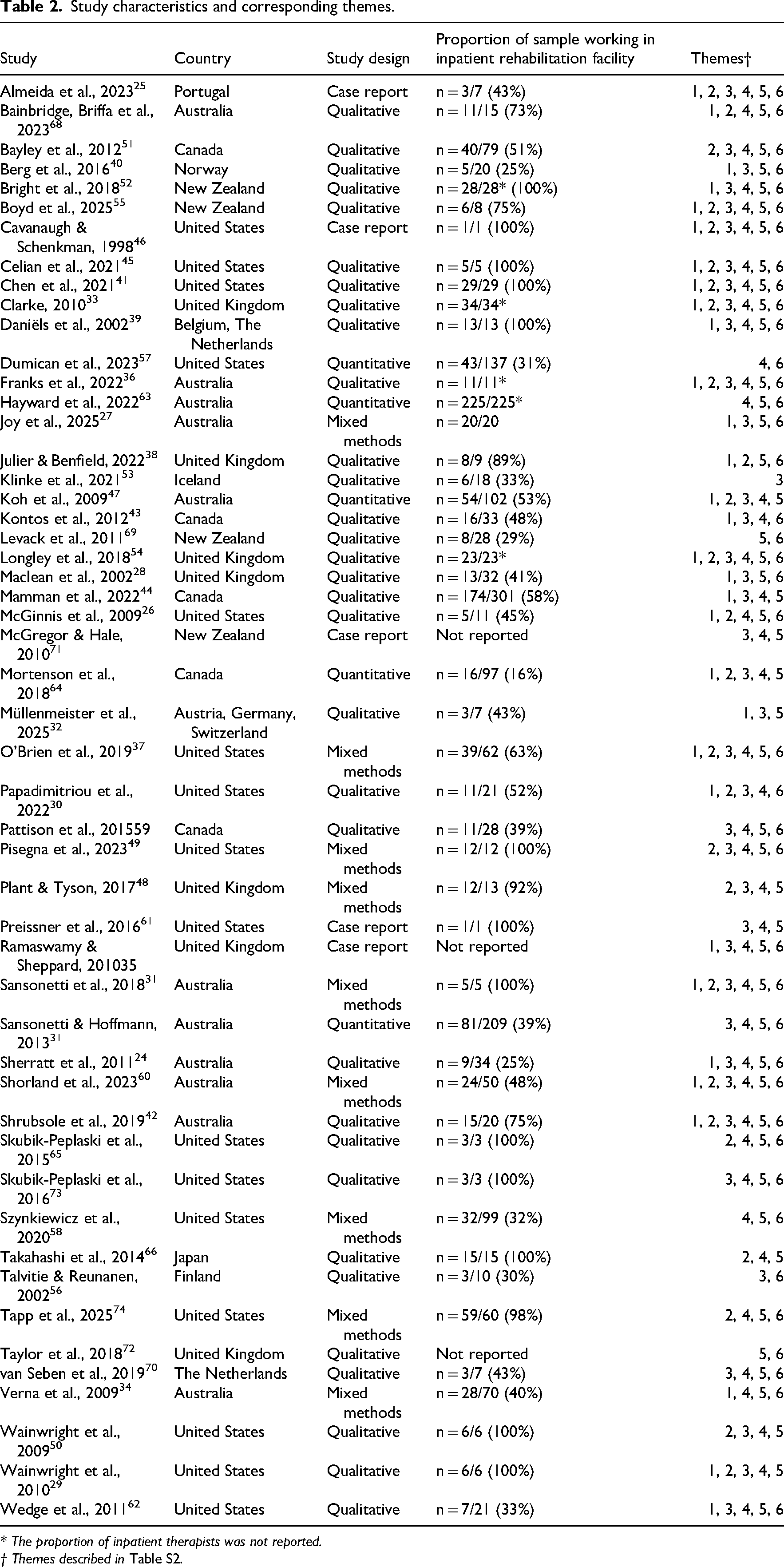
* The proportion of inpatient therapists was not reported.
† Themes described in Table S2.
Overview of thematic analysis results
Factors influencing therapists’ clinical decision-making processes in inpatient rehabilitation facilities were categorized into six key themes: Consideration of Non-Medical Circumstances, Collaboration and Roles within Care Teams, Within-Session Communication Techniques, Knowledge-Base and the Influence of Experience, Medical and Safety Considerations, and Balancing Institutional Priorities within Treatment.
Theme 1: Consideration of non-medical circumstances
Consideration of Non-Medical Circumstances describes how therapists integrate factors about a patient's context, such as their at-home support network and care preferences, in decision-making. This theme incorporated sub-themes of Understanding the Patient's Perspective, Presence of Families and Caregivers, and Assessment of Patient Resources. Findings from 31 articles contributed to this theme and its sub-themes.
Sub-Theme: Understanding the patient's perspective
As reported in 15 articles, therapists’ understanding of patients’ social contexts,24–27 personal values, 28 and emotional states24,29 informed clinical decisions. In one study of therapists working with patients with disorders of consciousness, therapists described “looking for a person” by “observ[ing] signs that can point to patients’ intention, motivation, or volition that could not be classified as mere bodily reflexes or responses” 30 (p6) to infer patient intent and guide treatment. Decisions were informed by understanding the patient's life before injury31,32 and getting to know the patient on a personal level rather than solely through treating their illness or impairment.29,33 Therapists’ perceptions of a patient's satisfaction with treatment also affected whether to continue the treatment. 34 Conflict between the patient's and the therapist's values could pose challenges, as in one study which reported an ethical dilemma for therapists when a patient wanted to explore end-of-life care options. 35
Sub-Theme: Presence of family and caregivers
Twenty-two studies reported family and caregiver influence on treatment decisions, including when to set goals, 31 whether to train a patient to use an assistive device,36,37 whether to prescribe therapeutic activity to be performed outside of treatment sessions, 27 and collaborating with family members to obtain preferred foods from outside the hospital for use in oral trials to train swallowing. 38 Family reports helped therapists understand whether an intervention was beneficial beyond standard measurable outcomes like improved function or reduced impairment. 34 Therapists relied on families and caregivers to guide decision-making if the patient was unaware of impairments 39 or experienced communication difficulties. 40 Family members and caregivers most frequently influenced decisions about whether the family could support the patient in a selected intervention throughout recovery and after discharge.36,38,41,42 Therapists considered family members’ physical capacity to safely assist patients and “willingness to perform intimate care tasks.” 41 (p8) Conversely, therapists sometimes excluded family from treatment decisions because they viewed input as irrelevant or perceived that it made treatment more difficult 43 or due to the patient's preference. 24
Sub-Theme: Assessment of patient resources
Six articles described therapists’ Assessment of Patient Resources to influence treatment decisions. Resources included equipment available for independent practice, 27 home characteristics,24,37,44 ability to obtain an assistive device through personal finances or insurance, 36 and prior experience with using an assistive device for mobility. 37 For example, a therapist may not use an assistive device in treatment if they perceive the patient will experience barriers (i.e., cost, insurance) to acquiring the device after discharged. Thus, therapists’ assessments of patient resources influenced post-discharge treatment objectives.36,44,45
Theme 2: Collaboration and roles within care teams
Collaboration and Roles within Care Teams describes how therapists’ roles and interactions with other health professionals impact their decisions. Twenty-six articles contributed to this theme. Perceptions of professional scope of practice influenced decisions, such as believing that occupational therapists must address self-care activities regardless of the patient's priorities, 31 or that intensive aphasia treatment was integral to what it means to practice as a speech-language pathologist. 42 Therapists frequently described teamwork as helpful for developing complementary treatment goals 46 and using an multidisciplinary approach to interventions.33,36,47,48 Multidisciplinary communication and collaboration enhanced therapists’ confidence in their treatment plans. 49
Varied skill levels 41 or areas of expertise 38 among team members were positive factors in decision-making. Newer clinicians valued co-treating and discussing plans with experienced colleagues.29,50 Collaboration was beneficial for implementing complex interventions or using specialty equipment37,38,45 Therapists viewed conducting interventions in a therapy gym as positive because they could ask other staff for help if needed. 47 Poor staff support impeded collaborative interventions and utilizing complex equipment. 51
Some studies highlighted barriers to collaboration.33,42,51 Insufficient leadership 42 and unclear role delineation among professional disciplines33,51 caused friction among therapists and nursing staff. Decreases in staffing posed barriers to teamwork, with one therapist stating, “As staffing decreased all of us went into crisis mode so everyone was pushed just to [focus on] their own tasks.” 51 (p1636)
Theme 3: Within-session communication techniques
Within-Session Communication Techniques, appearing in 39 studies, described how therapists selected communication techniques to match patient needs and functioning.32,39,46,50 Some studies reported therapists using communication to increase collaborative decision-making during treatment, facilitating patient participation in goal setting, evaluations, and intervention selection.24,44,47 Therapists generally chose communication strategies to enhance patients’ understanding in therapy sessions, such as creating video recordings to provide visual feedback, using gestures and other physical cues, and repeating information based on patient cognitive and communication needs.46,50,52–54 Therapists also adapted communication strategies to address patients’ lives and values.28,55
However, communication decisions could also be exclusionary. One study reported that clinicians used medical terminology to communicate with their colleagues in the presence of patients while limiting patients’ participation in the conversation. 43 In another study, therapists relied on one-way communication, describing their expectations and reasoning for their treatment approaches to the patient without providing opportunities for feedback. 56 Exclusion could happen unintentionally, as seen in a study in which researchers observed therapists making unilateral decisions despite believing they were involving the patient. 48 (p270)
Theme 4: Knowledge-base and the influence of experience
Forty-two studies reported that therapists used specific categories of knowledge, such as clinical experience, scientific evidence, and practice guidelines, to inform decisions. Research evidence and clinical training (including continuing education) influenced intervention choices,29,57,58 assessment selection,25,59,60 use of assistive technology, 36 and goal setting practices. 61 Access to 36 and knowledge of 62 evidence-based practice techniques impacted whether therapists chose to use them. When selecting assessments, therapists considered the psychometric properties of the assessment (i.e., reliability, sensitivity) 46 and whether the assessment was objective. 37 Additionally, therapists relied on treatment guidelines, including facility protocols 63 and insurance reimbursement regulations. 45
Therapists relied on prior clinical experience to inform all aspects of treatment decisions.29,37,45,62,64,65 Therapists sometimes prioritized their experience over evidence-based techniques or novel interventions. 51 Therapists reported reluctance to change habits in response to new evidence,51,59 or adapted newer evidence-based interventions based on their experience.26,59,66 Similarly, unclear evidence surrounding the best course of treatment for patients with disorders of consciousness led one rehabilitation team to rely on experimentation and observation. 30 Due to external time pressure and logistical factors, therapists also selected tools, assessments, and interventions they considered simple based on their experience. 46 They favored outcome measures which were quick to administer, involved little equipment, and were easily accessible in the facility, 62 and avoided those difficult to access. 67 One paper reported that speech-language pathologists chose oral trials for patients with dysphagia due to being easy to deliver and effective, despite safety concerns. 38
Therapists across disciplines also disclosed individualized beliefs guiding clinical decisions. Some therapists prioritized listening to one's “gut.”54,68 Subjective assumptions about treatment efficacy and judgments of patient characteristics were also identified as knowledge sources. 55 For example, therapists reported believing too many new things will overwhelm a patient, 50 feeling like they “should be doing” occupation-based interventions, 65 (p255) presuming they might “take away somebody's hope” 39 (p170) in discussing prognosis, or making less effort to motivate elderly patients who they assume “have less to live for.” 28 (p447)
Theme 5: Medical and safety considerations
Forty-six studies described Medical and Safety Considerations, such as the patient's physical, medical, and cognitive attributes, as impacts upon clinical reasoning. Mobility and risk were often reported together,37,46,68,69 therapists considered risk as a major factor in whether to prescribe assistive devices for mobility.37,46,68 Pain, 41 visual neglect,39,41,68 cognitive impairments (including safety or risk assessment),29,31,34,38–41,44–46,48,54,68 and age24,28,45,70 were depicted as safety concerns. Therapists focused on promoting independence with functional tasks using assistive technology37,71 and compensatory strategies to address medical and safety needs. 36
Theme 6: Balancing institutional priorities within treatment
We identified institutional influences on clinical decision-making in 40 studies. The facility's physical environment, official policies, and company values shaped which treatments occurred. Institutional expectations of patient length of stay based on recovery milestones and institution regulations,39,49,54 treatment priorities,49,69 discharge preparation,39,72 measures, 57 safety and risk aversion, 68 and assistive technology use 45 influenced therapists’ choices in treatment. Workplace standards of session documentation also affected how therapists chose to treat.37,45,49 For example, a speech-language pathologist reported that documentation expectations prevented client-centeredness in aspects of aphasia treatment: “…it is expected that we come up with measurable goals, and written descriptions … I make the goal, and at best I get a confirmation that the client agrees.” 40 (p875) Additionally, some therapists found that factors in the treatment environment including noise 73 or availability of equipment,65,74 and access to space, stairs, and equipment that could be used outdoors 74 affected treatment decisions. Therapists recommended that facilities support technology access, quiet treatment environments, clear team communication, and education on evidence-based practices which could improve patient outcomes. 41
Time was a prominent focus in studies across countries, with concerns about time needed to train the patient,33,34,37,39,42,45,62 dividing limited time among multiple duties,45,51,58–60,65,69,70,72 or patient length of stay.38,39,49,54,69 Therapists preferred shorter assessments due to time restrictions impacted which assessments were selected.26,62,68 Some therapists reported not addressing long-term goals, social outcomes, 69 or mental health 49 because there was only enough time to focus on physical function. Institutionally projected discharge timelines resulted in discharge earlier than therapists would recommend, with discharge paperwork being completed during a treatment session in place of therapeutic interventions. 72
Conceptual connections among themes in decision-making
Figure 2 illustrates relationships across themes. Medical and non-medical factors, such as cognitive impairment and patient circumstances, guided within-session selection of communication techniques. Therapists opted for concise, closed-ended wording when instructing patients with cognitive disorders, 46 and adjusted communication style and treatment based on the family's participation in treatment. 41 In decisions regarding walking assistive devices, therapists considered the patient's non-medical circumstances like their home, in addition to medical factors like ability to balance. 37
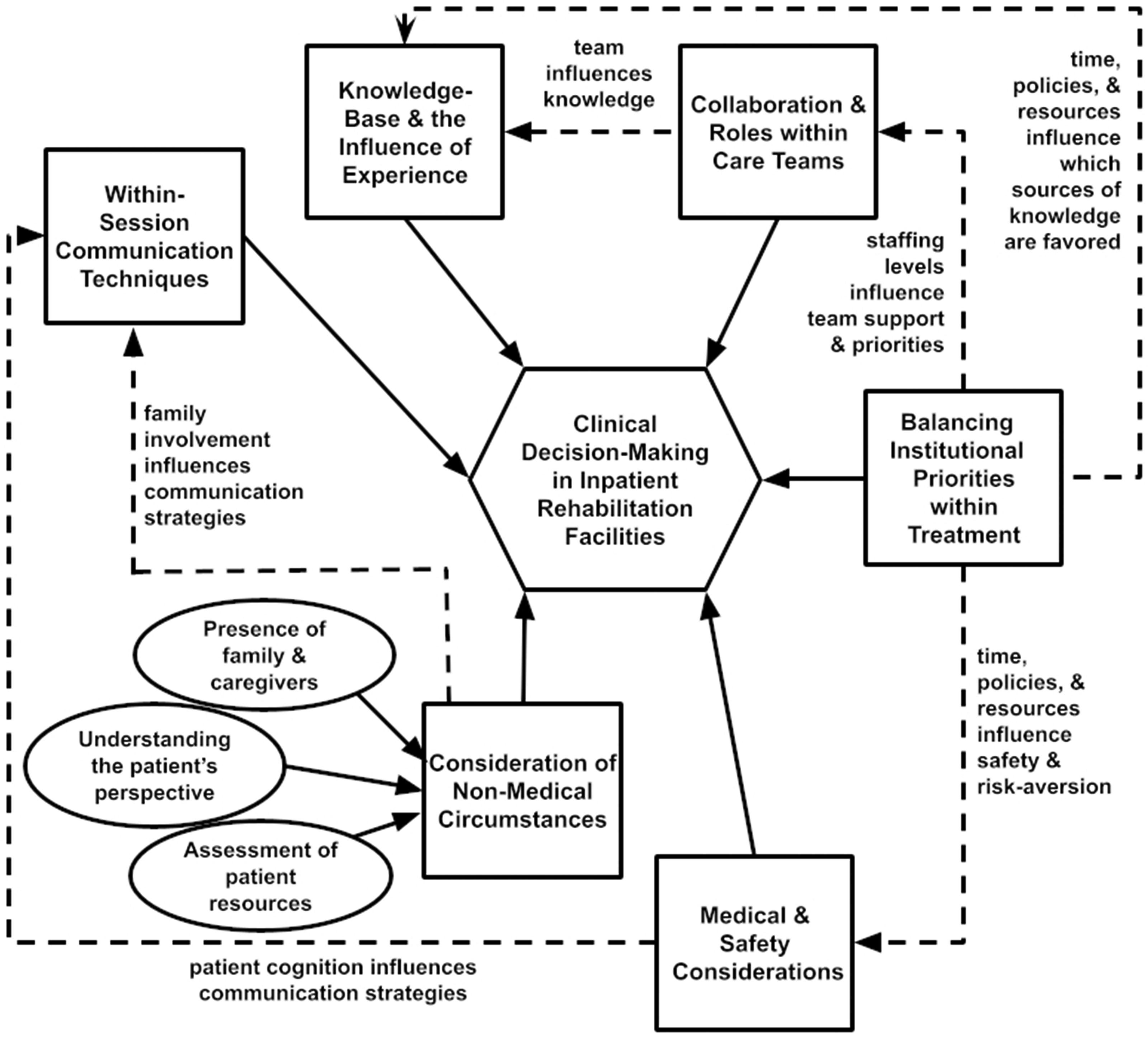
Concept map of thematic connections.
Time constraints and institutional priorities influenced the treatments therapists selected. Pressure to discharge patients to free up hospital beds led therapists to choose compensatory strategies instead of slower restorative treatments, while hospital culture surrounding risk influenced therapists’ perceptions of patient safety and decisions about walking independence. 68 Institutional factors also impacted the prioritization of knowledge sources, teamwork, and collaboration. Some therapists selected treatment according to their organization's protocol 63 or reimbursement requirements. 45 Others drew on prior clinical experience to choose familiar tools and approaches due to time pressure. 62 Teamwork was also influenced by the institution's staffing 38 and could be limited by understaffing. 51
Discussion
This scoping review synthesizes literature on clinical decision-making by therapists in inpatient rehabilitation facilities about how to plan care and use treatment time. The findings contribute a holistic view of the inpatient rehabilitation decision-making processes, illustrated by a concept map showing relationships among factors that may guide a single decision. Complementing findings of previous reviews on particular aspects of therapy decisions,8,75,76 our findings characterize a broad range of dynamically interacting and sometimes competing factors that clinicians must balance in real time. Any factor in the concept map may be a primary or partial driver of decisions, and may vary in influence based upon context. Our findings have implications for implementing new clinical tools, interventions, and processes in inpatient rehabilitation decision-making.
We observed that key patient dimensions drive decisions, including communication ability, medical conditions, and anticipated resources at home. Consistent with a prior review, 75 we identified experience as more influential than evidence. We found little consensus across studies regarding what treatments therapists chose, apart from those that are familiar,29,37,45,63–65 endorsed by the care team as a collaborative unit,29,33,36,38,41,46–48,50 or facilitated by the institutional environment.45,62,63,67 Hesitancy51,59 or selectivity26,59,66 toward incorporating new evidence-based treatments is consistent with the long-documented knowledge-to-practice gap. 77 Consistent with prior studies,8,75,76 institutions substantially influence therapists’ job duties,37,40,45,49,51,58–60,65,69,70,72 workplace procedures and policies,39,45,49,54,68 and resources62,63,65,67,74 that shape clinical decision-making. Thus, successful adoption of new evidence-based tools and practices in stroke inpatient rehabilitation will require substantial institutional support through focused, multi-pronged implementation strategies. 78
This review has limitations. Because we included studies from multiple countries, unique local regulations and institutional environments may not be captured in this review. Although familiarity with the inpatient rehabilitation facility setting and policies in the United States is an advantage for our team, our lack of experience in other countries may have biased our analysis toward US-based normative workplace communication, structures, policies, and practices.
Further research is needed to understand how clinical decision-making factors influence patient experience and health outcomes. Few studies thoroughly explored the underlying reasoning behind decisions or clinicians’ satisfaction with the decisions they could make. This study raises questions about how institutions can better support evidence-based treatments and innovative technologies into practices, and what decisions compromise patient care, particularly for vulnerable patients.
In conclusion, clinical decision-making in inpatient rehabilitation facilities requires balancing patient values and resources, tailoring communication strategies, and selecting the most appropriate treatment approach based on experience, knowledge, and the constraints of the institution and healthcare setting. As healthcare evolves, it is increasingly important to identify and improve upon components of clinical decision-making applied in rehabilitative care.
Therapy decision-making in inpatient rehabilitation facilities draws upon medical and safety considerations, non-medical factors (such as patient values and resources), within-session communication techniques, knowledge and experience to inform treatment, teamwork, and the priorities of the institution. Patient cognition and family involvement guide communication about clinical decisions. Time constraints, policies, available resources, institutional risk-aversion, and team collaboration influence therapists’ views of safety, employee role, and knowledge-sources in treatment. Understanding why decisions are made can help therapists analyze their reasoning, and help institutions support conditions for efficient, effective rehabilitation decisions.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155261435521 - Supplemental material for Factors influencing clinical decision-making in inpatient rehabilitation: A scoping review
Supplemental material, sj-docx-1-cre-10.1177_02692155261435521 for Factors influencing clinical decision-making in inpatient rehabilitation: A scoping review by Caitlin G. Dobson, Holly Carrington, Gloria M. Hernandez, Hannah C. Go, Sophia N. Hameed and Alison M. Cogan in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155261435521 - Supplemental material for Factors influencing clinical decision-making in inpatient rehabilitation: A scoping review
Supplemental material, sj-docx-2-cre-10.1177_02692155261435521 for Factors influencing clinical decision-making in inpatient rehabilitation: A scoping review by Caitlin G. Dobson, Holly Carrington, Gloria M. Hernandez, Hannah C. Go, Sophia N. Hameed and Alison M. Cogan in Clinical Rehabilitation
Supplemental Material
sj-docx-3-cre-10.1177_02692155261435521 - Supplemental material for Factors influencing clinical decision-making in inpatient rehabilitation: A scoping review
Supplemental material, sj-docx-3-cre-10.1177_02692155261435521 for Factors influencing clinical decision-making in inpatient rehabilitation: A scoping review by Caitlin G. Dobson, Holly Carrington, Gloria M. Hernandez, Hannah C. Go, Sophia N. Hameed and Alison M. Cogan in Clinical Rehabilitation
Footnotes
Acknowledgements
Authors C.G.D. and H.C. are supported through PhD student research assistantships in the Chan Division of Occupational Science and Occupational Therapy at the University of Southern California. A.M.C. is supported by a KL2 Mentored Career Scientist award from the Southern California Clinical Translational Science Institute & National Center for Advancing Translational Science. We gratefully acknowledge assistance from Karin Saric at the USC Norris Library, and former members of our lab: Eunhye Cho, Archie Patel, and Correon Potts.
Ethical approval and informed consent
There are no human participants in this article and informed consent is not required.
Author contributions
C.G.D. and A.M.C. co-conceived the study. C.G.D. designed the study and provided hands-on instruction to team members. All team members reviewed and extracted data from articles. H.C., G.M.H., and H.C.G. performed data cleaning on extracted data. C.G.D. and H.C. coded and analyzed data. C.G.D. performed data cleaning of codes and themes and developed the concept map with critical feedback from H.C and A.M.C. C.G.D. and H.C. wrote the manuscript with input from all authors, including conceptualization of the introduction by G.M.H., H.C.G, and S.N.H. A.M.C. provided critical feedback on the manuscript and mentorship throughout the project.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data sharing is not applicable to this article, as no new data were created or analyzed in this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.