
Abstract
Objective:
To explore how practitioner engagement and disengagement occurred, and how these may influence patient care and engagement.
Design:
A qualitative study using the Voice Centred Relational Methodology. Data included interviews, focus groups and observations.
Setting:
Inpatient and community stroke rehabilitation services.
Subjects:
Eleven people experiencing communication disability after stroke and 42 rehabilitation practitioners.
Interventions:
Not applicable.
Results:
The practitioner’s engagement was important in patient engagement and service delivery. When patients considered practitioners were engaged, this helped engagement. When they considered practitioners were not engaged, their engagement was negatively affected. Practitioners considered their engagement was important but complex. It influenced how they worked and how they perceived the patient. Disengagement was taboo. It arose when not feeling confident, when not positively impacting outcomes, or when having an emotional response to a patient or interaction. Each party’s engagement influenced the other, suggesting it was co-constructed.
Conclusions:
Practitioner engagement influenced patient engagement in stroke rehabilitation. Practitioner disengagement was reported by most practitioners but was often a source of shame.
Keywords
Introduction
Rehabilitation involves an interaction between at least two parties, a practitioner and a patient. Some have argued patient engagement is necessary to obtain maximum benefits from rehabilitation.1,2 ‘Engagement’ is a complex concept with multiple meanings.3,4 These can include it being an interactive interpersonal process or an observable patient behaviour akin to compliance. A recent review argued engagement is often co-constructed within patient-practitioner relationships. 3 Patients in several studies have suggested their perceptions of practitioner engagement influenced their own engagement in services.5–7 Within our study, we consider engagement a co-constructed relational process between the practitioner and patient which involves a process of gradual connection between the two parties.3,8 Our research focuses specifically on people experiencing communication disability after stroke. Patient-practitioner interaction can be significantly affected in the presence of a communication disorder which can result in a lack of involvement and difficulty participating,9–11 key components of engagement. 3
While there has been reasonable attention to patient engagement in rehabilitation, there has been little consideration of practitioner engagement. This is perhaps not surprising as rehabilitation practitioners themselves have not historically been the subject of research. A review of papers published in three leading rehabilitation journals in 2012 demonstrated only 2.1% of studies addressed practitioner behaviours or variables. 12 However, a small body of evidence indicates a practitioner’s attitudes and behaviours may influence patient engagement3,4,7,13 and how practitioners work with their patients. 14 Accordingly, there seems to be a reasonable case for attending to practitioner engagement if we are to develop comprehensive understandings of engagement in rehabilitation. This paper explores how practitioner engagement and disengagement occurred in stroke rehabilitation, and how these appeared to influence patient engagement.
Methods
This study used the Voice Centred Relational Approach, an interpretive qualitative methodology. This focuses on the multiple perspectives and understandings evident within a person’s talk and action.15–17 These perspectives and understandings are considered ‘voices’. This methodology uses a Listening Guide to help researchers attend to the different perspectives within people’s talk and action16,17 by attending to how people speak of themselves, of others, of the relationship between themselves and others, and the context surrounding them.
Patient participants were eligible if they: (a) experienced a stroke and communication disability; (b) had accessed or were accessing rehabilitation; (c) could provide informed consent; and (d) were able to participate in interviews with supported communication. Patient participants were purposefully selected. Criteria included type and severity of communication impairment, gender, and service used. They were recruited through rehabilitation services and non-governmental organisations. Practitioner participants were eligible if providing stroke rehabilitation in the city where the study occurred. They were purposefully sampled, seeking diversity in discipline, clinical experience and clinical setting. Research and ethics boards provided institutional and ethical approval. All participants received written and verbal information prior to providing written consent. Information was modified using principles of communication accessibility for people experiencing communication disability. 18
The study had two components. The first involved interviews and focus groups while the second was observational. Initially, interviews were completed with seven patient participants and four rehabilitation practitioners. The practitioners had not been involved in the care of any of the patient participants. Interviews explored experiences of engagement. Each lasted 45 to 60 minutes. Two focus groups were completed with ten additional practitioners, exploring experiences of engaging patients in rehabilitation. Focus groups lasted between 60 and 75 minutes. All interviews and focus groups were audio-recorded and transcribed while patient interviews were also videotaped to capture non-verbal data. 19 Each interview and focus group was considered a data-set.
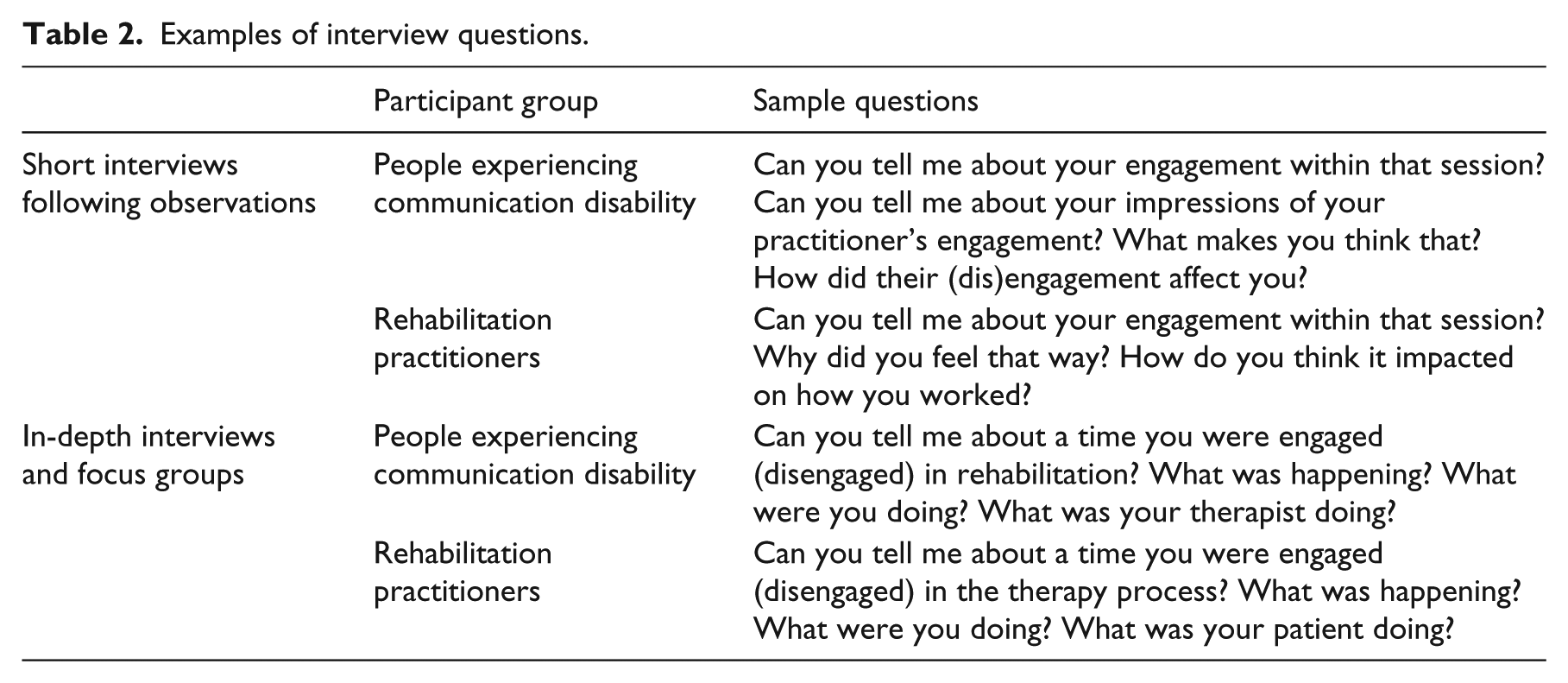
The observational component focused on interactions between 28 rehabilitation practitioners and four patients, through each patient’s course of rehabilitation (n=28 patient-practitioner dyads). The details of data gathering are summarised in Table 1. Interactions were observed and recorded using video and field-notes, capturing 187 hours of interactions, including scheduled treatment sessions, incidental interactions on the ward, personal cares, ward rounds and meetings. Observations were supported by ninety-three short interviews with patients and practitioners after observed interactions, each lasting 5-15 minutes. Five stimulated recall sessions 20 were conducted with practitioner participants who watched a recording of an interaction between themselves and their patient and participated in an interview which explored their reasoning and interpretations within that interaction. After rehabilitation ended, 15 in-depth interviews were completed with practitioners, exploring their experiences of engagement, primarily focusing on their experiences with the patients in the study. These lasted between 45 and 60 minutes. Examples of questions asked in interviews are provided in Table 2. The OHW Scales, 21 published scales of speech, language, and cognitive-communication impairment developed by O’Halloran, Hickson and Worrall, were completed to determine severity of communication impairment. All material pertaining to each patient-practitioner dyad was collated into one document. Each of these 28 documents was considered a data-set.
Data collection for observational component.

Examples of interview questions.
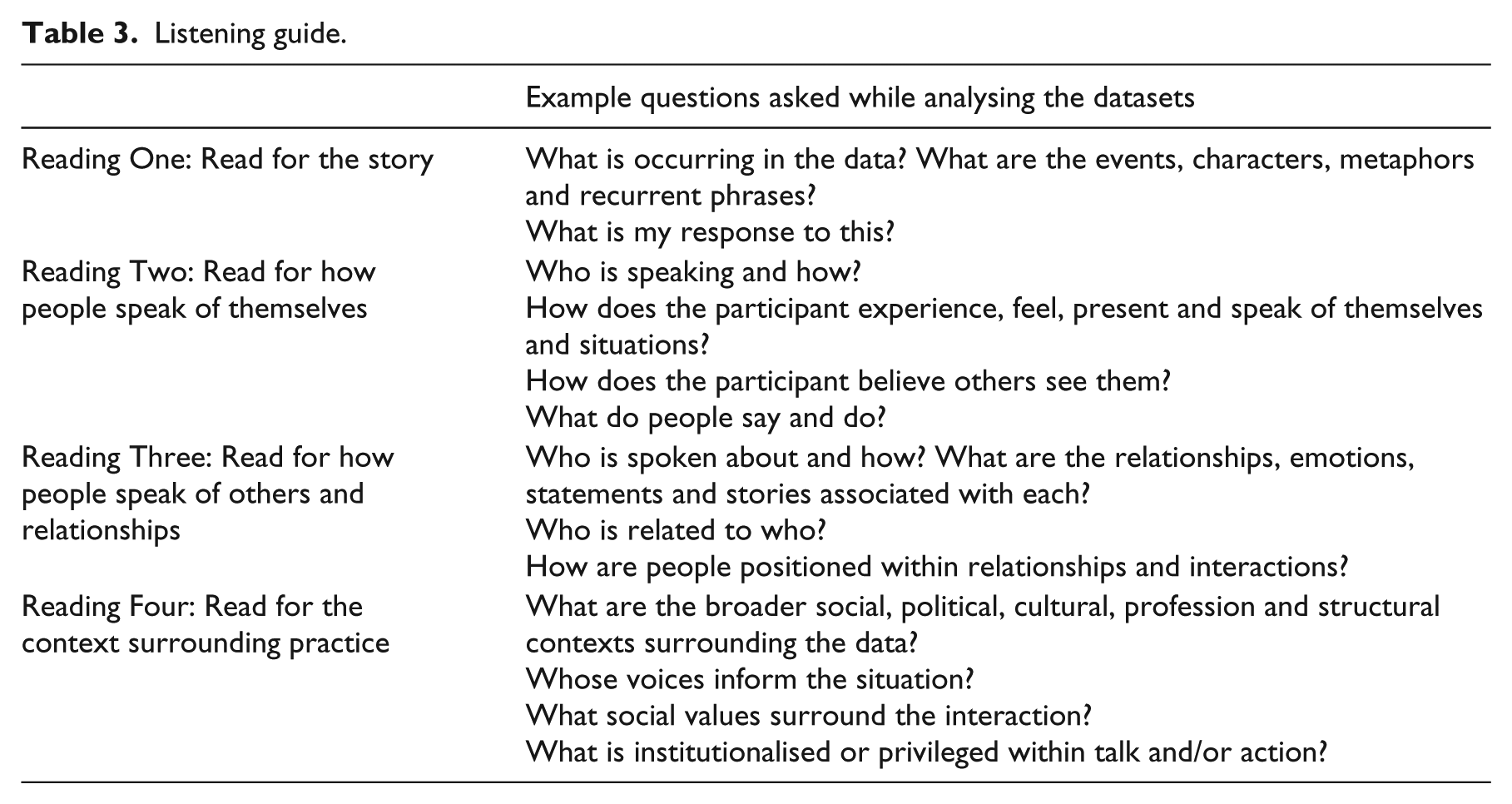
Data analysis was sequential, occurring first at the level of individual data-sets (individual interviews, focus groups, and patient-practitioner dyads) and then across data-sets. First, a Listening Guide was used to analyse within each data-set. This involved multiple readings of the data, guided by a series of methodologically and theoretically-informed questions16,17 (see Table 3 for examples of questions). Analysis considered what people said within interactions with participants and the researcher, as well as paralinguistic features and body positioning. The analysis was compiled into a memo. 22 Each memo incorporated raw data and analysis of how people spoke of themselves and others, the relationships between them and the context surrounding the interaction. Memos captured similarities and differences across the dataset as well as recurring themes and voices, surprising findings and areas for further consideration.
Listening guide.
Analysis then occurred across data-sets, exploring the different voices or perspectives and understandings within and across the participants. For this paper, we focused specifically on the voices evident when people spoke of practitioner engagement and disengagement. We used analytic questions8,23,24 to explore how these voices arose, in what circumstances, how these were evident in the practitioner’s interactions and reflections, how they were perceived by the patient, and what effects these had for both the patient and practitioner. Memos recorded this emergent analysis. Constant comparison, comparing data across participants and contexts to explore similarities and differences, 22 was used to develop increasingly complex, nuanced understandings of practitioner engagement and disengagement.
Quality was guided by Tracy’s 25 criteria. Rigour was aided by gathering multiple forms of data from multiple participants over a prolonged period. There was regular discussion of the emergent analysis within the research team. Memos recorded emergent analysis and provided an audit trail through the research. Detailed description of practitioner engagement and disengagement, and integrating raw data alongside analysis also add rigour.
Results
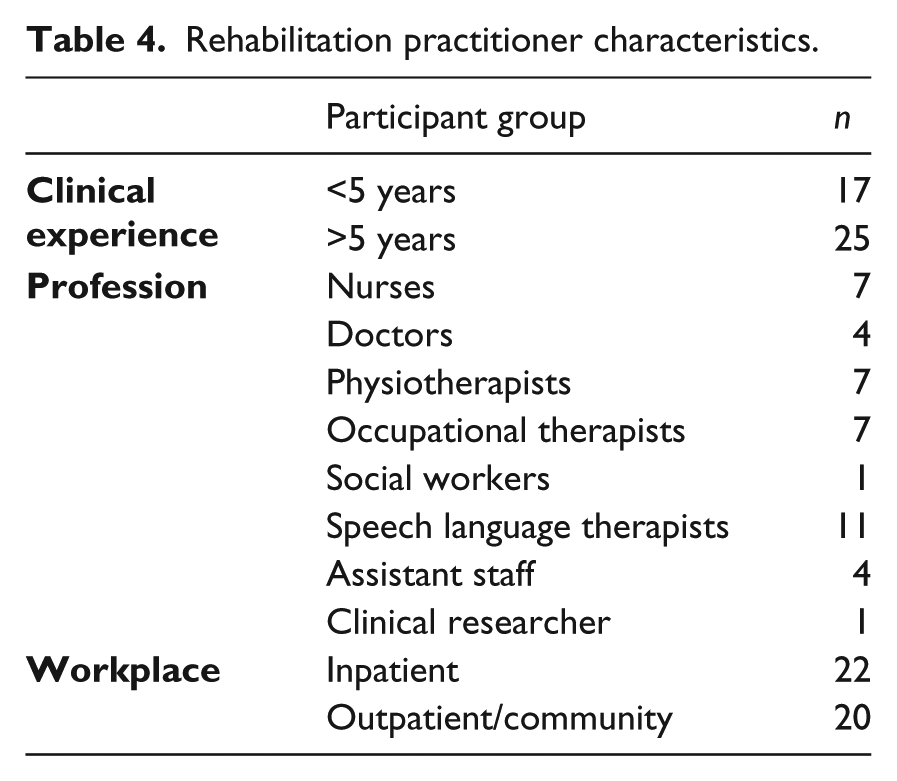
In total, 42 rehabilitation practitioners and 11 people experiencing communication disability after stroke participated in this study. Most rehabilitation disciplines were represented. Practitioners had a range of clinical experience from 1-30 years. Demographic information is summarised in Table 4.
Rehabilitation practitioner characteristics.
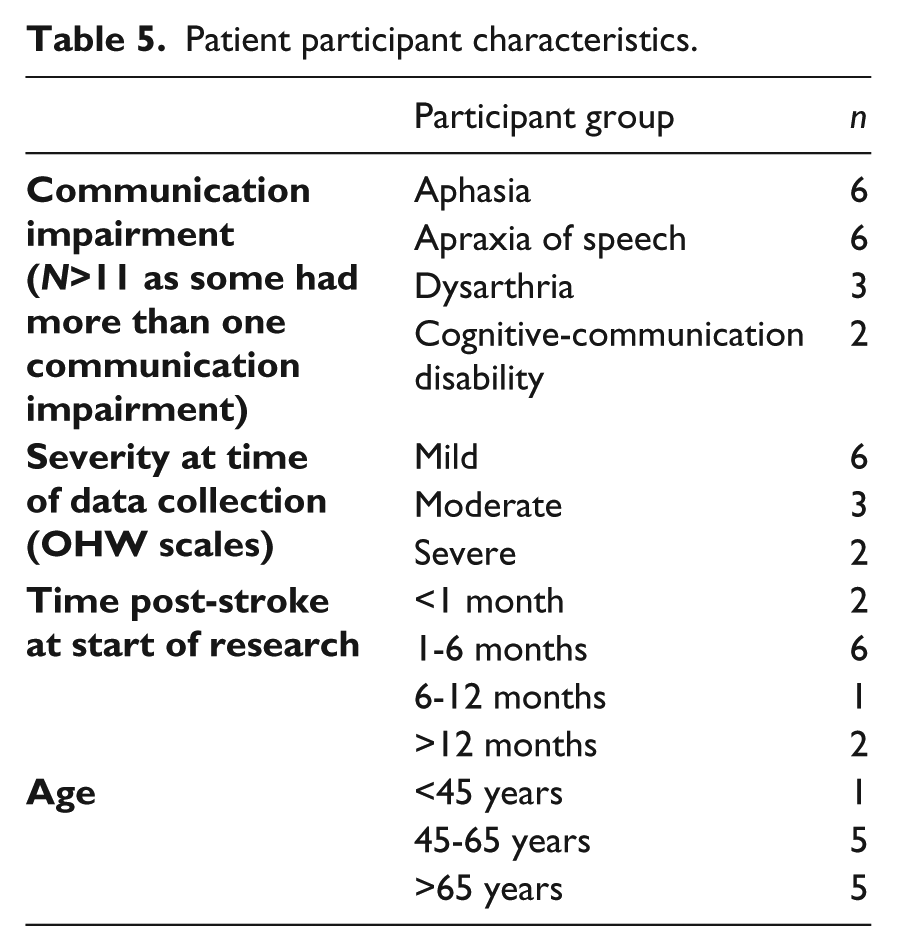
Patient participants experienced a range of communication impairments. Most were accessing rehabilitation services at the time of data collection and had their stroke within the last six months. Their age ranged from 42-75 years of age. Patient characteristics are summarised in Table 5.
Patient participant characteristics.
The engaged and disengaged practitioners
Patients and practitioners both considered the practitioner’s engagement influenced patient engagement. Practitioner engagement was complex, influenced by their knowledge, confidence and perceptions of the patient’s engagement. All practitioners discussed times of engagement and disengagement, though stigma was associated with disengagement.
The engaged practitioner
Engaged practitioners talked positively and mindfully about their engagement. Both patients and practitioners emphasised the importance of practitioner engagement. One patient talked of struggling in therapy, not seeing the purpose but tolerating it in the hope she might see improvement and become engaged. She considered her speech language therapist’s engagement helped her engage:
Being persistent and their attitude that ‘we can do it’ … [her] eye contact that made me feel like they really are caring, they care about me. Not just in it for the job but they’re in it for me, going the extra mile (Patient A, mild aphasia).
Patients perceived the practitioner was engaged when they detected a “passion for the job … not just going through the motions” (Patient B, dysarthria), or when they appeared to personalise their work to meet the needs of the individual patient, evident in “how much the therapist puts their mind into the patient” (Patient C, moderate aphasia).
Practitioners acknowledged that their engagement mattered. They considered it helped their patients engage. Some argued “at the beginning, our engagement is almost more important than [the patient’s engagement]” (community physiotherapist). It was considered essential to “gain their engagement” (community occupational therapist). At times, it appeared that the ‘engaged practitioner’ was a performance for facilitating and maintaining patient engagement, akin to a sales strategy, “selling yourself and the package of care” (community occupational therapist). Practitioners presented as being engaged to maximise engagement with them and the rehabilitation process:
You know when you front up at the door, you’ve got to be able all smiles and enthusiastic in order to maximise that engagement. I would literally take a deep breath before going in to gather all my enthusiasm and encouragement and my wisdom and sometimes you’re literally can’t just knock on the door and sometimes you’ve actually got to switch on your therapeutic self (community physiotherapist).
When engaged, some practitioners described themselves as excited and motivated, invested at an emotional level, as evidenced in their word selection, non-verbal communication such as laughter, and facial expression. Their engagement was enhanced by patient achievement and professional satisfaction:
I work with swallowing as well, that’s awesome … It’s so great when you can tell someone that they’re allowed to eat again (laugh) … Ah the swallowing thing is awesome … I think I’m also excited cos he’s such a young guy and he’s lost so much (inpatient speech language therapist).
Some practitioners discussed and demonstrated a more deep-seated internal state of engagement. This functioned as a lens through which they viewed rehabilitation, their way of working and their patient’s actions and engagement. They reflected on and explicitly prioritised their own, and their patient’s engagement, as evident in a description of practice:
I felt I was very engaged and he was involved – a partnership thing. My engagement is quite important. You have to be in the moment, constantly monitoring change, seeing if I do x, what does he do, how does he react? The first couple of sessions are really about getting them on your boat, getting them on board (inpatient physiotherapist)
This practitioner described “weighing up the best way to work”, balancing service and patient needs to engage the patient. Other practitioners talked of working “outside the box” (community social worker), sometimes putting service requirements to one side such as completing assessments within a specified time period if they considered this would negatively impact on engagement. When engaged in this way, practitioners valued engagement and saw patient engagement and disengagement as their responsibility, something they could and should influence. Their engagement and their concern for the patient’s engagement was sustained, attended to, and enacted over a period of time, rather than being a finite performance at the start of rehabilitation.
The disengaged practitioner
Practitioner disengagement was intermittently present in the narratives of most practitioners. However, it appeared somewhat taboo. One community speech language therapist said “we don’t really talk about it, do we?” while her colleague said “you don’t think it should happen so you don’t talk about it”. Disengagement was sometimes seen as a personal failing, contrary to unspoken expectations of what a ‘good rehabilitation practitioner’ should be.
When asked about disengaged practitioners, patients commonly described those who focused on service requirements, seeming disconnected or disengaged with them as an individual. Such practitioners might “come in and do a job but they don’t know me” (Patient D, mild dysarthria) or “just go through the motions” (Patient E, moderate aphasia). While patients tolerated this, some reported anger toward such staff. In the context of communication disability, practitioners who did not initiate or facilitate communication were perceived as disengaged and distant:
They scurry over and turn me. They walk away, not even putting the bed rail up … They don’t want to talk. I think they feel awkward because I couldn’t talk back then. They’ve not even tried. (Patient F, initially severe aphasia and apraxia).
Such disengagement could exacerbate feelings of isolation, dependency and disability.
When practitioners were disengaged, service provision was reportedly affected. One community physiotherapist described delaying telephone calls and intervention with patients. Another described focusing on to “doing only what I needed to do to meet my legal and ethical obligations … showing I had done the job” (community occupational therapist) before discharging the patient. In these situations, practitioners focused on disciplinary assessments and treatments; other aspects of rehabilitation such as therapeutic relationships were not spoken of. When practitioners were themselves disengaged, they appeared to position patient disengagement as a patient responsibility rather than being something they could or should influence. For example, one inpatient speech language therapist described herself as “powerless” in the face of patient disengagement. Others described reducing or avoiding interactions, for instance placing rehabilitation on hold or discharging the patient until they were “ready to engage”, placing responsibility on the patient. When practitioners were disengaged, it appeared to set up not only a cycle influencing patient disengagement, but also access to rehabilitation and service provision.
Practitioners appeared to be or become disengaged for a number of reasons. It often appeared a subconscious response when not feeling confident or knowledgeable, or when they perceived they were unable to make a difference. A community speech language therapist described entering an assessment feeling “irritated” as she felt other staff should have addressed the issue rather than referring to her. She commented “the whole way along, I couldn’t make, neither of us could understand why the other was there and what we were aiming at”. This practitioner described leaving the interactions “feeling quite disillusioned, I didn’t achieve anything”. She acknowledged “I didn’t feel engaged because it was such hard work”. Some practitioners may assume engagement should happen relatively automatically; when this did not occur as anticipated, it could trigger an emotional response and sense of uncertainty in the practitioner.
While the practitioner’s own disengagement often appeared subconscious, there were instances where it was an intentional strategy. An inpatient speech language therapist spoke of emotionally disengaging during interactions with a patient in severe pain. She described how the patient “was crying and I couldn’t help her … there’s a feeling of probably emotionally disengaging on purpose”. In these instances, disengagement reflected an attempt to maintain some control and to protect the practitioner from the emotional aspects of practice. Inherent within all narratives of disengagement was a sense of powerlessness, of not knowing how to facilitate patient engagement or their own engagement. Many practitioners appeared to have limited skills and strategies to change the situation which contributed to their disengagement.
Practitioner engagement and disengagement: A co-constructed phenomena
Within patient-practitioner dyads, each person’s engagement was influenced by their perception of the other person’s engagement, skills, attitudes and behaviours. When a patient was perceived as engaged, practitioners responded positively, with an out-patient occupational therapist saying “it’s easier for us to engage with them because you can see they’re keen and they want to be there, rather than ‘they’re ten minutes late and they’ve not shown up’”. Patients echoed this, with Patient A (mild aphasia) saying “It’s the therapists’ attitude and skills that helped me through”.
Engagement and disengagement often mirrored each other. Early in one episode of care, a patient talked of “hating therapy”, that it was “too hard” and he “didn’t want to go”. His inpatient therapist described therapy as “mediocre”. She questioned “why try?” and “what am I doing wrong?”. She was acutely aware of the patient’s engagement struggles and these impacted on how she viewed herself and her work, leading to her saying “I didn’t want to come back to work after the holidays. It’s just been too hard”. However, there was a turning point when the practitioner changed her approach and the patient started to see some progress. He commented “It’s magic, I’m finally feeling positive”, while his therapist said “He was so interested … My engagement is a lot easier. I can see the change. I feel that what we’re doing makes a difference so I feel more engaged”. Their words highlight how limited progress and perceived disengagement could impact on each party. The patient’s disengagement was mirrored in the practitioner’s struggle to engage. Their mutual increase in engagement illustrates how it can be dynamic and co-constructed, influenced by the other’s actions and their interpretation of the other person’s engagement.
Discussion
This study provides an in-depth understanding of how engagement can be co-constructed and how the practitioner’s engagement and disengagement influenced the patient’s engagement. Of note was the subtle, sometimes insidious impact of disengagement. It provides concrete examples of the ways in which their disengagement could impact on patient experience and care, by restricting access to, and delivery of, rehabilitation services. Accordingly, practitioner engagement is something that needs to be attended to if rehabilitation services are to truly meet the needs of patients and to offer evidence-based, person-centred care.
It appeared that engagement could beget engagement; disengagement could beget disengagement. It was dynamic and reciprocal, with each influencing the other. Engagement and disengagement arose within, and sometimes because of, the interpersonal relationship, as described by Ells and colleagues, 26 consistent with earlier calls that engagement is a relational process, not simply a patient state and/or behaviour. 3 Engagement, and relational aspects of care, are commonly neglected or backgrounded in stroke rehabilitation practice guidelines and within service requirements. 27 They may also be backgrounded, hidden or absent within health professional education which commonly focuses on technical skills and knowledge.28,29 This suggests they are perhaps not considered valuable or legitimate components of care and certainly implies a lower level of importance than seems warranted. The findings of this research justify the need for further attention to the practitioner, their thoughts, feelings and values, and strategies to modify engagement within clinical practice and stroke rehabilitation research.
Practitioner disengagement was complex and often went unspoken, suggesting it might be accompanied by stigma. This may also reflect a tension between real and ideal practice. 30 Unspoken ideals of ‘good practitioners’ may include an expectation they ‘should’ be able to engage and ‘should’ be engaged; yet in many situations, this appears not to occur in real practice between individual practitioners and individual patients. If practitioners consider they ‘should’ be able to engage, it may be more difficult for them to seek help or to expand their repertoire of skills in engaging patients, and in facilitating their own engagement. Arguably, practitioners need to be able to reflect on engagement, how rehabilitation occurs, and the emotional work involved in providing rehabilitation in a safe, supportive environment.
Emotions and professional uncertainty were often evident when practitioners discussed their disengagement, suggesting engagement-related work might be considered emotional work. While uncertainty is inherent within clinical practice, 31 when uncertainty provoked an emotional response and negative feelings about one’s own knowledge, skills and competence, it could result in disengagement. There has been little research into the emotional work of rehabilitation practice.12,32 If emotional work is not acknowledged in research and practice, it becomes another unspoken, potentially stigmatised aspect of practice with notable implications for patient care as staff experiences has been associated with patient experiences.33,34 Its impact on staff and patients provides support for our call to closely attend to practitioner engagement and disengagement.
Study limitations
There are some limitations which must be acknowledged. The research was completed within one city in New Zealand, limiting generalisability of findings which are influenced by sociocultural and socio-political factors inherent within the health care system. The sampling strategy sought diversity amongst participants; focusing on narrower groups of participants may have provided more in-depth understandings of engagement and disengagement. This study did not seek to explore the relationship between patient or practitioner variables and practitioner engagement or disengagement. The research focused on broad patterns of engagement across the rehabilitation episode rather than engagement and disengagement within individual treatment sessions. Different participants may have had different understandings of engagement, which may have influenced how they discussed it. The very presence of communication impairments may have impacted on how patients were able to discuss their perceptions of practitioner engagement, despite the presence of supported communication techniques. 18 Despite these limitations, by elucidating how engagement and disengagement may be enacted, perceived, and responded to, and by discussing what the consequences may be for patient care, this study significantly advances knowledge of how engagement can be co-constructed in rehabilitation. While this study focused on patients experiencing communication disability, we suggest the central thesis of this paper, that there is a need to attend to the practitioner’s engagement and disengagement, is relevant across rehabilitation settings and client groups.
Practitioner engagement and disengagement are important factors in rehabilitation. Contrary to dominant literature, engagement is not simply a patient state, but is co-constructed in part, through the practitioner’s own engagement. Practitioner engagement and disengagement can impact on patients and on the services they receive. While future work is required to explore the relationships between practitioner engagement and outcomes, this research clearly demonstrates that increasing practitioners’ awareness of their potential impact on patients is vital.
Practitioner and patient engagement in rehabilitation is influenced by their perceptions of the other’s engagement.
Practitioner engagement (and disengagement) can impact on how the patient experiences rehabilitation.
Practitioner disengagement appeared to influence patient care and clinical decision-making.
Footnotes
Acknowledgements
We wish to thank the participants in the study for sharing their experiences of stroke rehabilitation. We also thank the editor and the two reviewers for their thoughtful comments on early versions of this article.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by an AUT Vice Chancellor’s Doctoral Scholarship and a Laura Fergusson Rehabilitation Doctoral Scholarship (FB), and an AUT Contestable Grant (NK, FB and KM). At the time of the study, KM was the Laura Fergusson Professor of Rehabilitation at AUT.