
Abstract
Objective
Moderate to severe persistent pain can affect up to 25% of people after a knee replacement for osteoarthritis. The aim of the trial was to test the feasibility of implementing Kneed, a novel digital pain rehabilitation self-management programme.
Design
Prospective, two group parallel randomised pilot study.
Setting
Online in Australia.
Participants
Adults with persistent pain rated as ≥4/10 in the operated knee more than 3 months post-knee replacement for osteoarthritis.
Intervention
The Kneed group were provided with 8 weeks of access to a digital pain rehabilitation self-management programme and compared to usual care.
Main measures
Recruitment, acceptability, usability and limited efficacy with descriptive statistics.
Results
Sixty participants, mean age 68.7 years, 75% female, 66.7% retired and 43% living outside metropolitan areas, were recruited between 15 October and 19 December, 2024 via social media advertising with 418 online eligibility surveys performed. There were 190 (45.5%) deemed potentially eligible; 82 (19.6%) left contact details and 60 (14.4%) consented. At 8 weeks, there were 48 (80%) participants remaining in the trial (20 Kneed (64.5%), 28 usual care (96.6%)). A majority of the Kneed group found the Kneed programme acceptable, would use it again and found that it helped them effectively manage pain and function.
Conclusion
It is feasible to recruit and retain older Australians with moderate to severe knee pain post-knee replacement for a trial testing a digital pain rehabilitation self-management programme. A larger trial is indicated to further test the clinical effectiveness of Kneed to reduce pain and improve function.
Keywords
Introduction
Australian data indicate that at 6 months post-knee replacement, 17% of people report moderate pain and 8% severe pain. 1 Further Australian observations indicate that 4.7% and 6.6% continue to have severe knee pain at 12 and 36 months, respectively. 2 Combining these results, with approximately 80,000 knee replacements performed annually in Australia, 3 4000 to 20,000 new recipients each year may be expected to experience moderate to severe persisting knee pain during their first 12 months post-surgery.
Pain persisting post-knee replacement is associated with considerable personal burden including poorer general and physical health, higher pain catastrophising and reduced satisfaction, 4 reduced function and a lower quality of life, 2 sleep dysfunction and fatigue. 5
Once surgical complications have been excluded, persistent pain post-knee replacement can be understood in a biopsychosocial context 6 with multiple risk factors and potential contributors. 7 There is often a continuum of persistent pain that commences with pain associated with osteoarthritis, is exacerbated by surgery and extends through the recovery period.
A biopsychosocial pain rehabilitation programme to address the complexities of persistent pain post-knee replacement, as well as the impact of this pain, offers a potential solution. 8 However, a recent systematic review 9 established that there was not enough evidence of effectiveness of rehabilitation therapy or programmes in this cohort.
Digital solutions, as adjuncts to traditional rehabilitation therapy, provided in the acute and subacute phases post-knee replacement, have demonstrated small clinically insignificant differences 10 and have not been researched in the chronic phase. 9 Unsupervised digital programmes have demonstrated short-term benefit in chronic musculoskeletal pain conditions 11 and have the potential to improve access to pain management.
To address the gap in available rehabilitation therapy for persistent pain following knee replacement, Kneed, a digital pain rehabilitation self-management programme that uses a biopsychosocial framework, has been developed. Self-management, common to community rehabilitation programmes, 12 is based on a model that includes education and skill-training that is beneficial in managing chronic disease, 13 a category that can include persistent pain. 14 Behavioural change techniques have been included in Kneed to improve engagement and participation and promote change. 15
The aim of this pilot study was to test the feasibility of implementing Kneed. The primary pre-specified measures included recruitment, acceptability and usability with secondary measures providing limited efficacy testing of clinical outcomes. 16 Additionally, we documented what constitutes ‘usual care’ in people with persistent pain post-knee replacement.
Methods
A prospective, two group parallel assessor-blinded randomised pilot trial was conducted online in Australia. The intervention group was provided with 8 weeks of access to Kneed, an online pain rehabilitation self-management programme and compared to a ‘usual care’ waitlist-controlled group, with allocation on a one-to-one ratio. The trial design and reporting have been written in accordance with the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement extension to randomised pilot and feasibility trials. 17
The trial was delivered virtually and participants randomised to the intervention arm could engage with Kneed by accessing an online website from anywhere in Australia. The data were collected by secure electronic surveys hosted by Qualtrics™ (Seattle, Washington and Provo, Utah) with individual links to the surveys sent to participants via email.
Participants who were 18 years and over, who had undergone a total knee replacement for osteoarthritis at least 3 months prior to enrolment in the trial were eligible. Participants were required to have an average daily pain score of greater or equal to 4 out of 10 (assessed on a numerical rating scale of 0 to 10) over the preceding week and self-report that they are able to walk safely in their home, safely exercise, read English and have reliable access to a computer, internet and an active email account. Exclusions included people with a plan to undergo further surgery (knee or other) in the next 3 months and those who did not have osteoarthritis as the primary diagnosis (including people who had a revision knee replacement, those with inflammatory arthritis or knee joint infection based on self-report).
Participants were recruited via an online social media advertising campaign with Meta advertisements. The advertisement contained a link to a landing page on Qualtrics™ containing the explanatory statement followed by a survey that assessed eligibility criteria. If potential participants were eligible and they left their details, the participant was contacted by phone by the research assistant KR to perform a secondary check of eligibility and discuss the trial. All eligible participants were then sent the explanatory statement and an electronic consent form to sign prior to enrolment. Once consented, KR sequentially allocated the participant to the next study identification number and notified the participant of their allocated group. All other trialists remained blinded to group allocation. Outcomes were all collected electronically. An AUD$100 gift voucher was sent to each recipient once they completed the 8 week surveys to reimburse them for their time. The initial aim was to recruit 50 participants (25 in each group) as a sample to obtain estimates to detect a medium standardised effect size in a larger trial. 18 Recruitment was extended to 60 participants on 10 December 2025 due to early attrition when seven out 23 participants (30.4%) did not return 4 week surveys.
The intervention group was provided with usernames and passwords to access the Kneed programme website for 8 weeks. Kneed is an unsupervised, self-management pain rehabilitation programme developed as part of a translational research Doctor of Philosophy degree at Monash University. Kneed provides choice to self-select learning opportunities from a menu 19 of modules that includes pain neuroscience education, exercises, motor imagery, desensitisation techniques, relaxation, sleep and cognitive strategies such as goal setting and managing flare-ups of pain (Supplemental File 1). Participants allocated to usual care were instructed to continue with their current self-directed or clinician-directed treatment and were offered access to Kneed at the conclusion of their 8 week assessments.
Recruitment was assessed by recruitment video views (impressions), the click through rate to the Qualtrics™ explanatory statement, eligible surveys undertaken, per cent eligible consenting and retention in the trial. We intended to record use of the Kneed programme including time spent on the programme per user, and per cent completing 1 h but these could not be assessed due to technical and privacy limitations and were changed post-hoc to completion of the introductory module and starting the main modules). ReCAPTCHA (Google Inc.) scores (range zero to one) were used in Qualtrics™ to screen for bots (internet automated programmes) with a score of <0.5 considered likely to be a bot. Demographic details collected included self-reported age (years), self-described gender (‘male/female/non-binary/third/prefer to self-describe/prefer to not say’), culture (‘which culture do you most identify with’), highest level of education, work status and postcode which was converted into a Modified Monash Model location. 20
Acceptability (satisfaction, intent to continue to use the programme and perceived usefulness) and website usability were measured using the mHealth App Usability Questionnaire, a reliable and valid tool that measures three domains: ease of use, design and satisfaction and usefulness 21 at 8 weeks in the Kneed group. The tool was adapted with permission to use the word ‘website’ rather than ‘app’. Other word substitutions were made such as ‘pain and function’ for ‘health’, ‘pages’ for ‘screens’ and ‘design’ for ‘interface’. It had one question removed (‘I feel comfortable using this app in social settings’) as this was not applicable to the Kneed website. Participants rated Kneed using a seven-point scale from one (strongly disagree) to seven (strongly agree).
Pain outcome assessments were based on recommendations made in the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials statement. 22 Average knee pain in the operated limb was assessed using a numerical rating scale at baseline, 4 weeks and 8 weeks. The Oxford Knee Score was used as a validated condition-specific categorical measure of pain and function at baseline, 4 weeks and 8 weeks, with scores from zero (worst) to 48 (best). 23 The Oxford Knee pain subscale score, zero is worst, 28 is best (dichotomised to assess for high pain = scores ≤14) 24 and the Oxford Knee functional subscale score, zero is worst, 20 is best, were both derived from the Oxford Knee Score. 25 Health-related quality of life was measured using the EuroQol EQ-5D visual analogue scale at baseline and 8 weeks, zero is worst and 100 is best. 26 Depression, anxiety and stress were assessed using the Depression, Anxiety and Stress Scale 21 at baseline and 8 weeks. 27 Scores for each domain range from zero (no symptoms) to 42 (maximum number of symptoms). The Pain Catastrophising Scale (zero is lowest, 52 is highest) assessed catastrophising at baseline and 8 weeks. 28 The Pain-Self-Efficacy Questionnaire (zero is lowest, 60 is highest) assessed confidence to self-manage pain at baseline and 8 weeks. 29 A seven-item Global Patient Impression of Change question was assessed at week 8 with participants asked ‘since the start of this study, my persistent knee pain is’. 30 Participants with pain that was ‘much’ or ‘very much improved’ were considered clinically important responders. 22 Participants were asked to report which health practitioners they had seen and which medications they had taken with regards to their knee pain over the previous month at baseline, at 4 weeks and at 8 weeks, providing a continuous 12 week assessment period. Doses and frequency of medication use were not monitored.
Participants were randomised to either Kneed or the usual care group. Allocation was single-blinded and a randomisation schedule for 74 possible participant allocations was prepared by a biostatistician blind to group while both the participants and the research assistant KR were aware of treatment assignment after randomisation. NJ, the Kneed platform manager, was blinded to group and participant allocation. Randomisation was undertaken by a professional biostatistician DM using Stata 18 statistical software (Stata Corporation, College Station, TX, 2023). Random permuted blocks of varying length, as recommended by CONSORT, were employed. 31 The resulting randomisation schedule, in the form of a spreadsheet, had each study identification number randomly allocated a letter of A or B. This was then supplied to the research assistant 2 weeks prior to commencement of the trial and KR created sealed, opaque, numbered envelopes containing the group A or B to match the spreadsheet. At commencement of the trial, KR randomly allocated each group (i.e. treatment or control) to either A or B using a coin toss and remained the only person aware of allocation until after statistical evaluation was completed. Each participant was then sequentially assigned to either A or B based upon the randomisation schedule following consent.
As this was a small feasibility trial, no external data monitoring was required. Data were stored securely on Monash University servers. For the primary outcome, descriptive statistics were calculated for recruitment measures, acceptability and usability. For the secondary clinical outcomes, primary analysis was not pre-specified and a per protocol analysis was conducted. Descriptive statistics were provided to measure the differences in means between baseline and 8 weeks, along with 95% confidence intervals. As recommended for feasibility studies, no tests of statistical significance were performed. 17 A responder analysis was conducted evaluating participants with ≥30% and ≥50% reductions in average pain from baseline to 8 weeks and those who reported that they were ‘much’ or ‘very much improved’ from baseline. Descriptive statistics were provided for healthcare utilisation. Outcomes of usual care participants who crossed over to Kneed after trial completion were not monitored. Ethics was obtained from Monash University Human Research Ethics Committee, Project ID 41207.
Results
Recruitment commenced on 15 October 2024, with the first participant enrolled on 23 October 2024, and the final participant enrolled on 19 December 2024. There was no recruitment in the first week using static picture advertisements only. After 1 week, the strategy was changed to a recruitment video. The video received 662,110 impressions in Australia over the following 58 days with 85% of impressions (65% women and 20% men) from those over the age of 55. Meta reported that there were 21,547 clicks (a 3.3% click through rate) on the video link through to the Qualtrics™ landing page containing the explanatory statement and eligibility survey.
The explanatory statement was viewed, at least partially, 2187 times (10.1%), with 409 (18.7%) of these views estimated by Qualtrics™ to represent bots. There were 418 eligibility check starts with 93 (22.2%) likely to be bots (Figure 1). There were 190 (45.5% of attempts) deemed potentially eligible, with 35 (17.3%) likely to be bots. In total, 82 left contact details (19.6%) and the research assistant attempted to contact each one (unable to contact four) and re-performed the eligibility check (11 ineligible) and consented (seven didn’t consent) 60 eligible people (14.4%). One person was recruited for every 11,035 video views, 359 click-throughs, 36 views of the landing page, seven eligibility checks and three of those potentially eligible. The linear relationship between these recruitment events is shown in Figure 2 in Supplemental File 2.
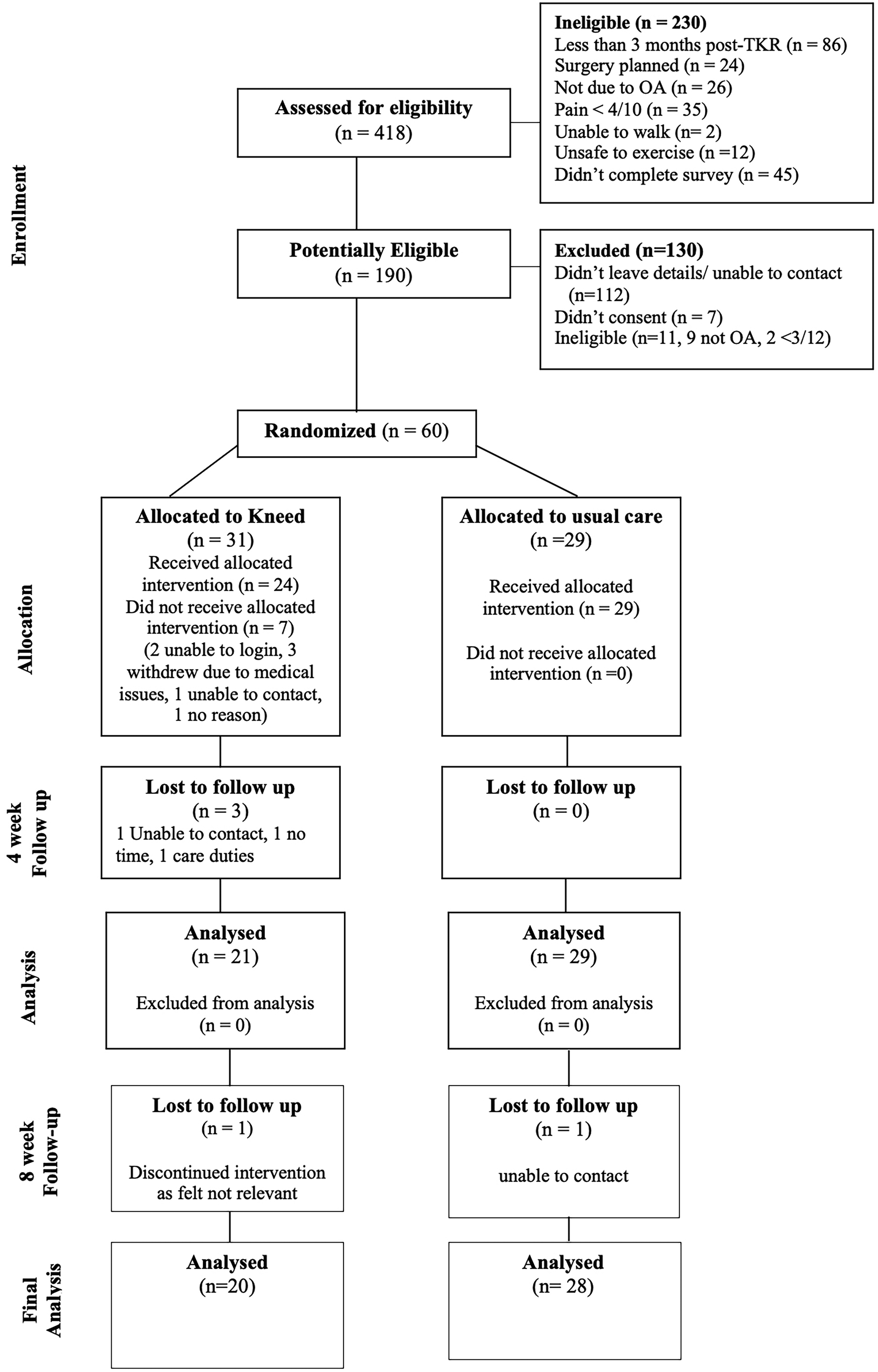
Consort diagram of participant flow.
Of the 60 enrolled participants, 31 were randomly allocated to Kneed and 29 to usual care. There were 50 (83.3%) participants remaining in the trial at 4 weeks and 48 (80%) at 8 weeks (Figure 1). The 10 participant withdrawals in the first 4 weeks occurred exclusively in the Kneed group. Seven of the 10 did not start the Kneed programme at all, and the three who did start did not finish the introduction. Reasons for withdrawals included unrelated medical issues, an inability to login and use the technology, not enough time and two were uncontactable. There were two additional participant withdrawals between the 4 and 8 week surveys, one from each group. The Kneed participant reported that the survey questions were not applicable to them. They did however access the programme and reported a 40% improvement in average pain scores from baseline to 4 weeks. The participant who withdrew from the usual care group was uncontactable, they had high pain at baseline and had no change in average pain score between baseline and 4 weeks.
Possibly due to the small sample size, there were apparent differences in baseline characteristics shown in Table 1 and Table 7 in Supplemental File 3, but differences in baseline patient-reported scores were minimal. Mean age for the usual care and Kneed groups was 70 and 67 years respectively with ages ranging from 37 to 85 years. The proportion of females was higher in the usual care group (86% vs. 65%). Median time post-knee replacement was 19 and 14 months for the usual care and Kneed groups respectively with wide variation as demonstrated in the boxplot (Figure 3, Supplemental File 4). Over 80% of participants reported a comorbidity, the commonest being hypertension (48%) (Figure 4, Supplemental File 5). The population lived in six Australian states and territories, with 43% of the total sample from outside metropolitan areas (48% usual care and 42% Kneed).
Baseline characteristics.
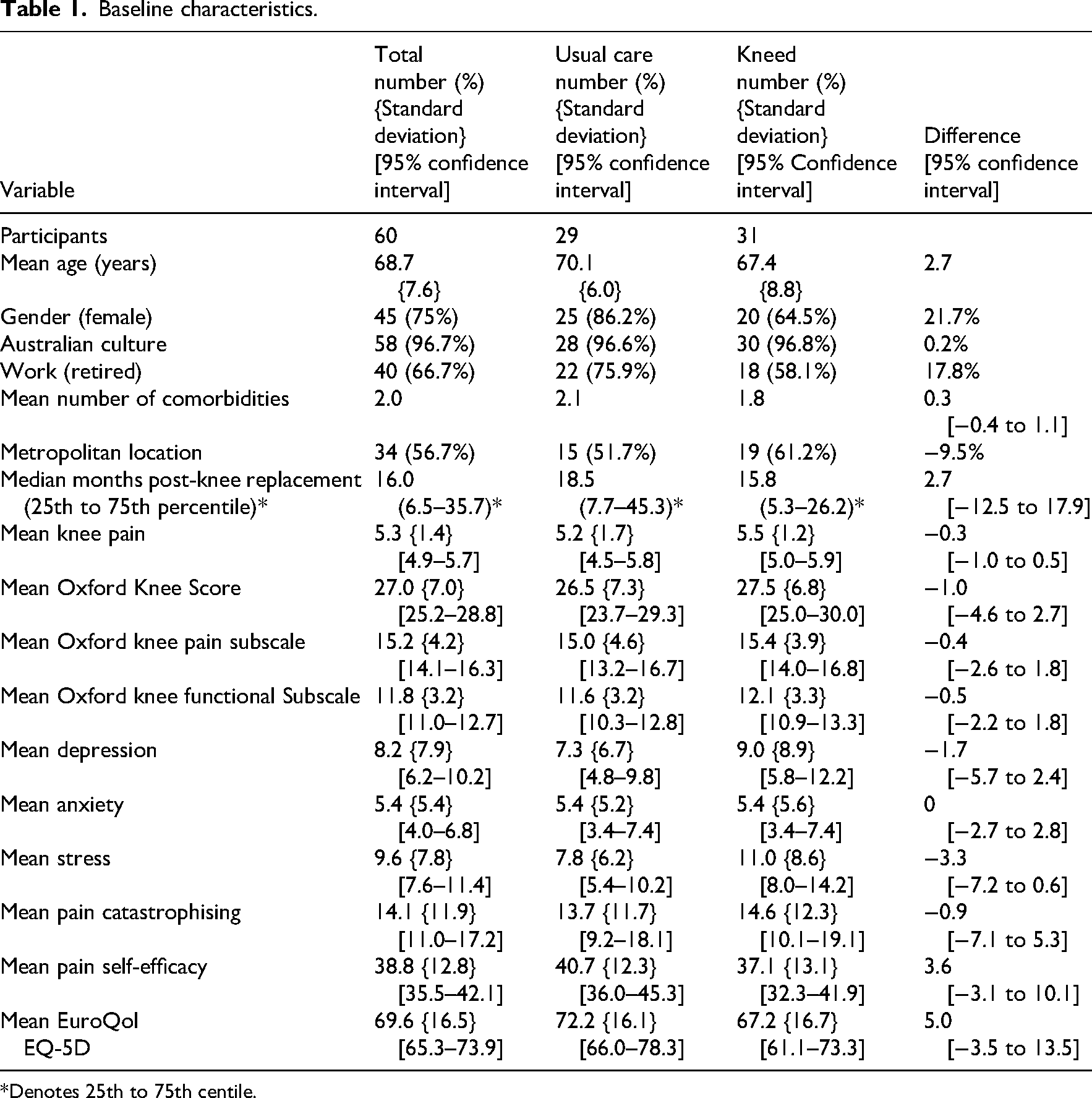
*Denotes 25th to 75th centile.
The mean knee pain was moderate (5.3, 95% confidence interval 4.9 to 5.7) and 24 participants (40%) had high pain scores, 13 (45%) in the usual care group and 11 (36%) in the Kneed group. Feedback was provided by 19 of the 20 Kneed participants with individual question results shown in Table 8, Supplemental File 6. Overall, the mean score was 5.8 (standard deviation 1.1, 95% confidence interval 5.2 to 6.3), where 5 = somewhat agree and 6 = agree. For the ease of use domain, the mean score was 6.0 (standard deviation 1.1, 95% confidence interval 5.5 to 6.5), for the design and satisfaction domain, the mean score was 5.9 (standard deviation 1.2, 95% confidence interval 5.3 to 6.5) and for the usefulness domain, the mean score was 5.6 (standard deviation 1.1, 95% confidence interval 5.0 to 6.1). A majority of participants agreed or strongly agreed that they were satisfied with the website, that they would use the website again and that the website helped them manage their pain and function effectively (Figure 5, Supplemental File 6). There were 11 Kneed participants who provided additional comments about their experience with Kneed, included verbatim in Table 9, Supplemental File 6.
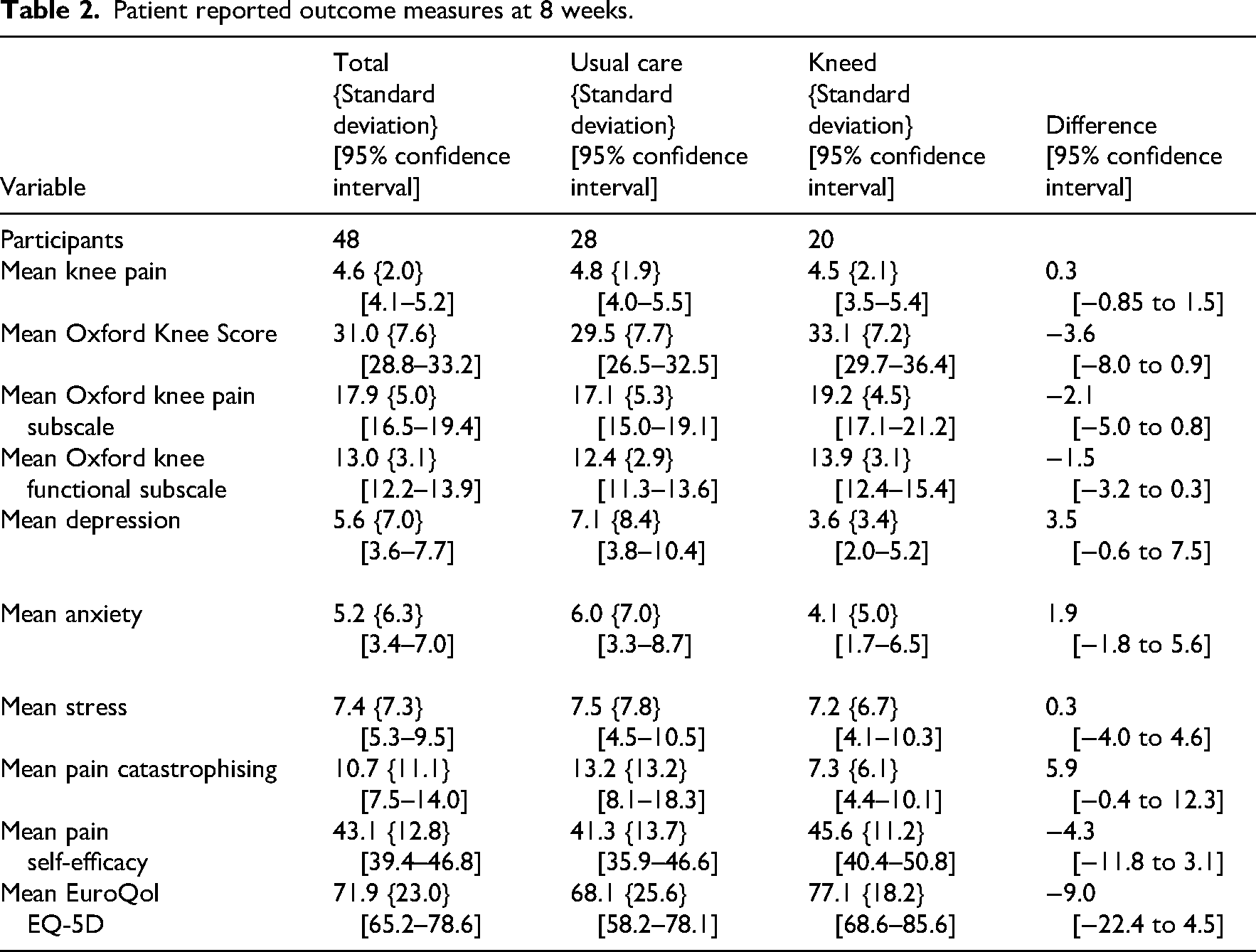
Patient reported outcome measures for pain and function were assessed at 4 weeks and means and confidence intervals are provided in Table 10, Supplemental File 7. All of the patient reported outcome measures were collected at 8 weeks (Table 2). For both groups, there were mean group trends towards improvements in pain and function between baseline and 8 weeks. Improvements for mental health status, catastrophising and self-efficacy were more notable during this time in the Kneed group. Health-related quality of life declined by four points in the usual care group over 8 weeks, whereas it improved by 10 points in the Kneed group.
Patient reported outcome measures at 8 weeks.
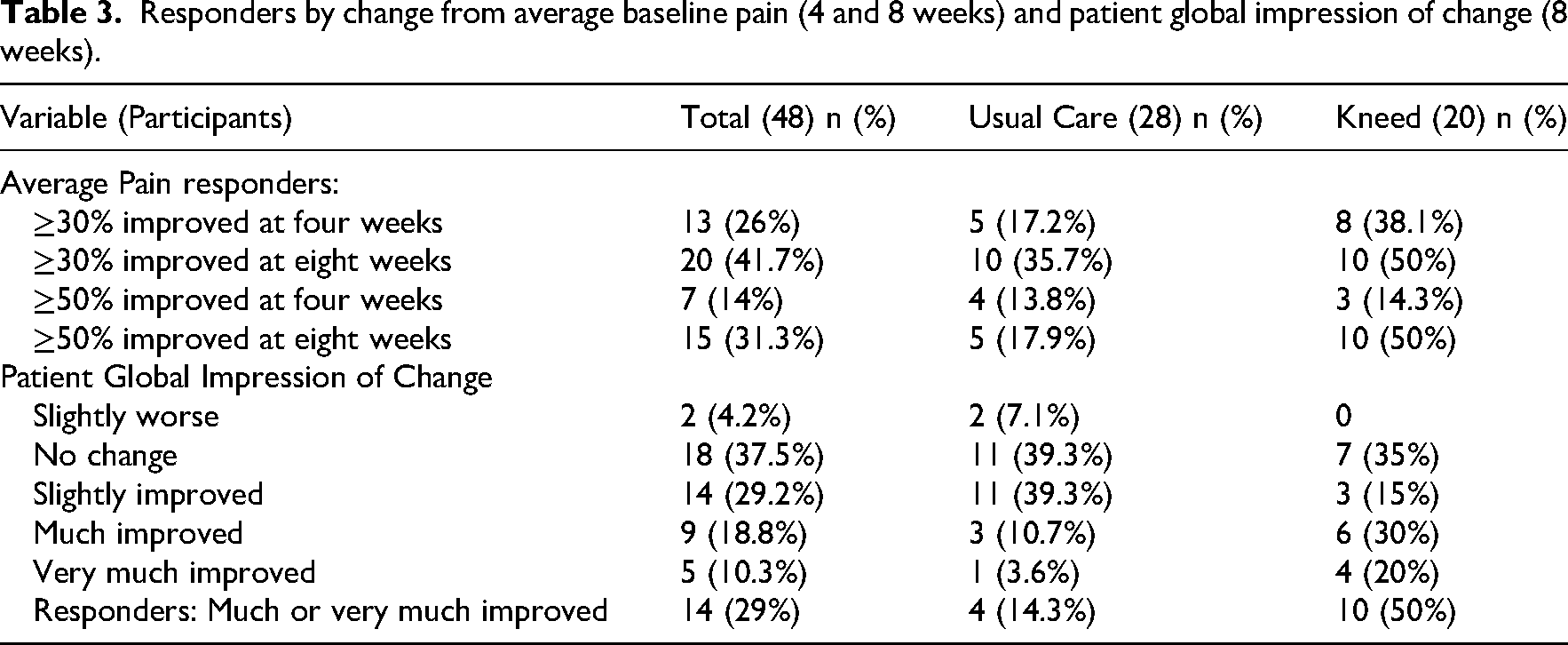
Individual responders sorted by improvements in mean pain ≥30% and ≥50% from baseline to 4 weeks and 8 weeks are shown in Table 3. At 8 weeks, 18% of the usual care group and 50% of the Kneed group experienced a ≥50% improvement in average pain. Assessed using the Patient Global Impression of Change, 14.3% of the usual care group and 50% of the Kneed group were individual responders (Table 3).
Responders by change from average baseline pain (4 and 8 weeks) and patient global impression of change (8 weeks).
Further analysis demonstrated the improvements made in all outcome measures by patient global impression of change responders (from both groups) compared to non-responders (Table 11, Supplemental File 8).
Health practitioner attendance is summarised in Table 4. Attendances with general practitioners, physiotherapists and orthopaedic surgeons were the commonest at baseline although 32% of trial participants had not consulted a health practitioner in the 4 weeks prior. This appeared to relate to time post-knee replacement (Figure 6, Supplemental File 9).
Health practitioners consulted specifically for knee pain in the 4 weeks prior to baseline, 4 week and 8 week assessments.
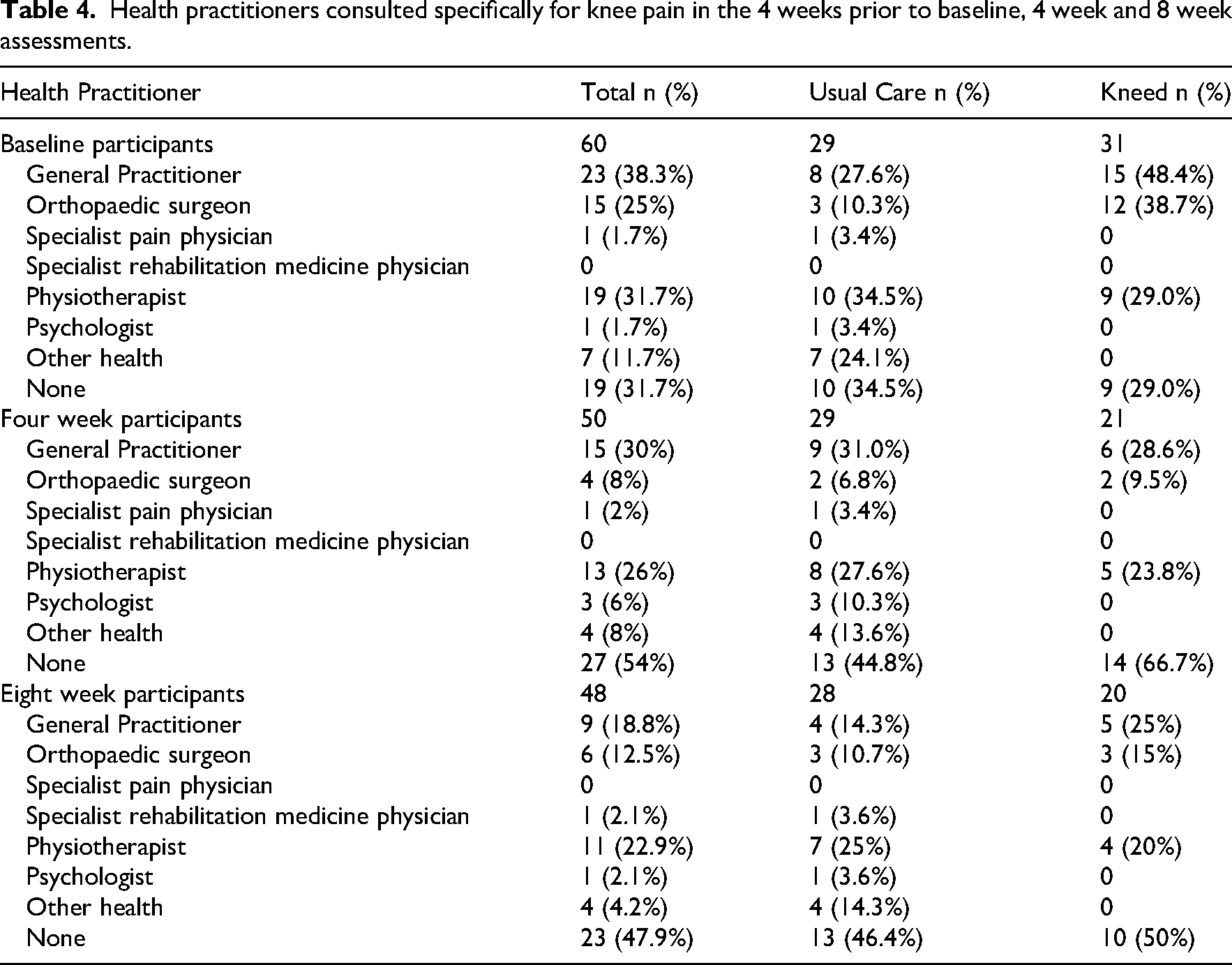
For both groups, attending health practitioners declined over the 12 week trial period (visualised in Figure 7, Supplemental File 9) and there was a corresponding increase in the percentage of participants who were not seeing a health practitioner for their persistent knee pain from 34.5% to 46.4% in the usual care group and 29% to 50% in the Kneed group.
At baseline, 90% of participants in both groups reported that they were taking medication to treat their knee pain (Table 5). Paracetamol (75.9% usual care and 71% Kneed) and non-steroidal anti-inflammatory drugs (51.7% usual care and 41.9% Kneed) predominated. Twenty-five per cent of participants had taken an opioid (oxycodone, tramadol, tapentadol or other) in the 4 weeks prior to the baseline assessment (19.4% usual care, 29% Kneed). Opioid use had declined at 8 weeks (14.3% usual care and 10% Kneed).
Medication taken in the 4 weeks preceding baseline, 4 week and 8 week assessments.
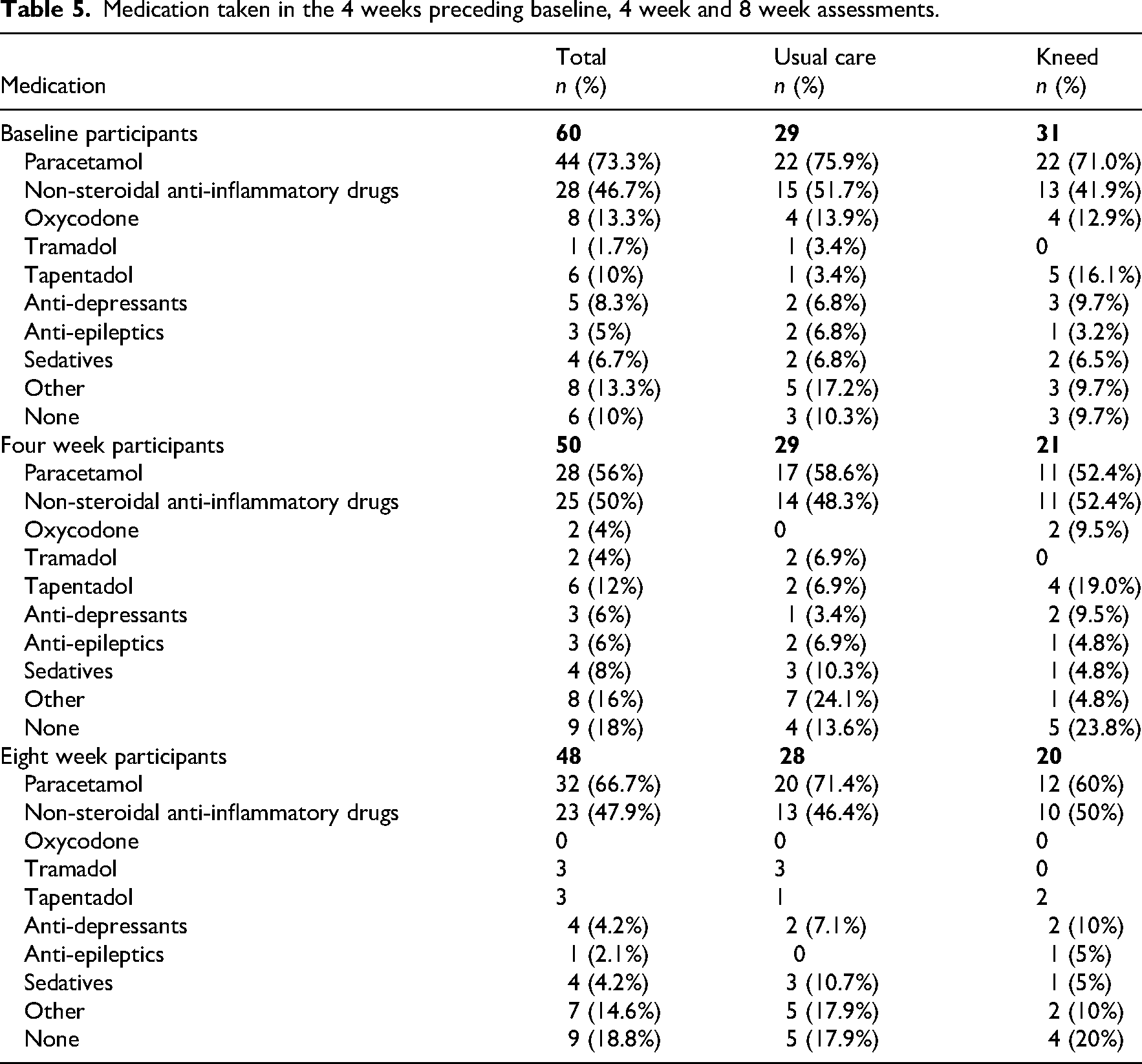
Over the trial period, medication use generally declined (visualised in Figure 8, Supplemental File 9) with an almost doubling of the number of total participants taking no medication for their knee pain from 10% to 19% of participants (usual care 10.3% to 17.9% and Kneed 9.7% to 20%).
One participant in the usual care group reported a surgical procedure on their knee between the 4 and 8 week surveys and there was an improvement in their average pain score of 25% from baseline (and 4 weeks) to 8 weeks. No adverse events were reported.
Discussion
This pilot study aimed to test the feasibility of Kneed, a novel pain rehabilitation self-management programme for people with persistent pain post-knee replacement. We have demonstrated satisfactory recruitment/uptake, acceptability and usability of Kneed. Clinical outcomes for Kneed and usual care have been documented. What constitutes usual care for this cohort in terms of health practitioner consultations and medication use has also been documented.
We were successfully able to recruit almost one participant per day once the advertisement changed to video from a static picture. The large number of views of the video and eligibility checks supports an argument for the interest and demand for treatment of persistent pain post-knee replacement. Importantly, our study determined that recruitment of older participants to an online programme via social media advertising was possible. With the mean age of our cohort at 68.7 years, our study is reflective of the mean age of 68.4 years of the Australian population undergoing knee replacement 3 supporting feasibility for this mode of recruitment.
An important consideration for the feasibility of the recruitment strategy is the large volume of eligibility screening questionnaire responses. In such a context, the use of manual screening by a research team member was necessary to ensure exclusion of non-people (bots) from the process, estimated to be 18.6% of eligibility survey attempts in our study, a lower rate than previous research. 32 An additional benefit of this secondary screening was ensuring participants truly fit the eligibility criteria, which can be an issue in online recruitment. 32 Although not required to bolster recruitment, future trials could consider inclusion of subgroups of those considered ineligible for this study (n = 203; 47.7%) such as those with inflammatory arthritis, people with pain less than 4 out of 10 and people who have had revision knee surgery as there has been little research in these subgroups.
One of the potential benefits of digital programmes is their vast reach. We observed this in our trial with recruitment of participants living in six different states and territories of Australia and 43% of participants living outside metropolitan areas.
Consistent with previous research investigating digital interventions for persistent pain, 33 we observed a considerable loss of participants in the intervention arm (withdrawal n = 11, 35.5%). For example, in a supervised Australian digital pain programme, only 69% of those randomised to the intervention group completed 50% or more of the programme and follow-up questionnaires. 34 Significant withdrawal and low adherence to complete digital programmes has also been seen in real-world trials in persistent pain. 35 In our study (n = 10, 83.3%) of withdrawals occurred before the participant had completed the introductory programme module to unlock the rest of the programme, suggesting that the programme may not have met expectations or appeared too burdensome for some participants, especially if they were unwell or had other challenges. Exploring this further will be important in future research studies.
The majority of the Kneed group was satisfied with the programme, would use it again and endorsed that the website helped them manage their pain and function effectively. Clinical outcome analysis is limited by the small numbers, retention and the nature of a pilot study. The positive outcomes for 50% of the individuals in the Kneed group who completed the 8 week follow-up (responders with ≥50% reduction in pain and/or ‘much or very much improved’ and ≥50% reduction in average pain scores) are sufficiently promising to consider further evaluation. Addressing the biopsychosocial nature of pain also appeared to result in improvements in depression, anxiety and stress scores, catastrophising and health-related quality of life.
Without evidence-based alternatives, the Kneed programme, which is safe, low cost and easily accessible, offers enormous potential. A reduction in healthcare resource use (health practitioner attendances and opioid use) may be another potential benefit to participation in the programme.
We have been the first to document 12 weeks of what constitutes usual care for people with persistent pain after knee replacement with a high proportion of participants continuing to attend health practitioners and take medication for pain. Although participants were a median of 16 months post-knee replacement, almost a third of participants were consulting a physiotherapist for their knee pain at baseline, a quarter were consulting an orthopaedic surgeon and almost 40% were consulting a general practitioner.
Over 8 weeks, 14% in the usual care group were responders (‘much’ or ‘very much improved’) and only 18% experienced a ≥50% reduction in average pain despite medication use, medical consultations and physiotherapy. This may indicate the limitations of current approaches and a need for a change of the usual care model. Medication use, while highly prevalent in this group, may have limited efficacy and lacks an evidence base. 36 Non-steroidal anti-inflammatory drugs use particularly should be reviewed considering the potential harms in a population with a high prevalence of hypertension (48%), diabetes (17%) and digestive problems (24%).
Study limitations include potential selection bias introduced by the social media recruitment method (e.g. more females than males) and differences in baseline characteristics (despite randomisation), attrition bias with uneven dropout rates and performance bias due to single blinding. Generalisability of the study to other countries and different patient cohorts will require further investigation.
In conclusion, we have been able to demonstrate satisfactory recruitment of older people with moderate to severe pain and disability following knee replacement to participate in a novel digital pain rehabilitation self-management programme in Australia. A larger trial is required to be more confident that Kneed provides a clinical benefit.
Clinical messages
This is the first trial to test a digital self-management rehabilitation programme to treat moderate to severe persistent pain post-knee replacement.
Recruitment of older people via social media advertising to participate in an unsupervised digital programme is feasible with potential to help them effectively manage their pain and function.
Supplemental Material
sj-docx-1-cre-10.1177_02692155251375382 - Supplemental material for A pilot randomised controlled trial of an online self-management programme for people with persistent pain post-knee replacement (Kneed)
Supplemental material, sj-docx-1-cre-10.1177_02692155251375382 for A pilot randomised controlled trial of an online self-management programme for people with persistent pain post-knee replacement (Kneed) by Nathan Johns, Dean McKenzie, Bernadette Brady, Justine Naylor and John Olver in Clinical Rehabilitation
Footnotes
Acknowledgements
We acknowledge the work of our research assistant Kalinda Randazzo who was instrumental in conducting this trial.
Ethical approval
Ethics approval was obtained from the Monash University Human Research Ethics Committee, Project ID 41207.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: A grant was received from the Epworth Monash Rehabilitation Research Unit (EMREM) to fund the research assistant and Peninsula Health Department of Rehabilitation Special Purpose Fund for recruitment advertising costs.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Dr Nathan Johns developed Kneed as part of a Doctor of Philosophy (PhD) thesis at Monash University and is the sole owner of copyright. The remaining authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability
Data are available on request due to ethical/privacy restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.