
Abstract
Objective
This study aimed to explore the acceptability and factors that influenced implementation of a multidomain, home-based fall prevention programme (Integrate) for people with Parkinson's disease who fall recurrently, and their care-partners.
Design
Qualitative, inductive thematic analysis of semi-structured interviews.
Setting
Homes of Integrate participants in Sydney, Australia.
Participants
Eighteen interviews with people with Parkinson's disease and/or their care-partner who were purposively sampled after completing Integrate.
Intervention
Integrate was delivered by occupational therapists and physiotherapists and included personally tailored home fall-hazard reduction, exercise (leg muscle strength, balance and freezing of gait) and safer mobility strategies delivered over 6 months.
Results
Five themes were identified: (a) the importance of personalisation, (b) a collaborative effort, (c) capacity building, (d) navigating fall risk with Parkinson's is complex and (e) the ease (or not) of making changes. Participants and their care-partners appreciated the personalised, home-based programme that involved shared decision-making and was delivered by expert therapists. They developed increased safety awareness and problem-solving skills. Making improvements, receiving ongoing support from therapists and care-partners and making change easier promoted sustained engagement. However, some participants faced emotional and psychological barriers to engagement including fatalistic beliefs about disease progression and a desire to avoid appearing ‘disabled’. The reality of Parkinson's disease motivated participants to make changes but Parkinson's-related impairments such as apathy and motor fluctuations hindered this.
Conclusions
People with Parkinson's disease who are recurrent fallers, and their care-partners, found the Integrate programme acceptable and were able to engage with it with guidance and support from therapists.
Introduction
Parkinson's disease is the fastest growing neurodegenerative disease, with the number of people with Parkinson's disease globally expected to double between 2020 and 2040, exceeding 12 million people. 1 Falls increase as the disease advances, and around two-thirds of those who fall do so recurrently. 2 These falls are personally and financially costly.3,4 Fall prevention strategies that are effective across the disease spectrum are therefore urgently needed to reduce the fall-related healthcare needs of this growing population.
Fall prevention exercise programmes reduce falls in people with mild to moderate Parkinson's disease by around 26%, 5 leaving an unacceptably high fall rate. The World Guidelines for Falls Prevention 6 recommends personalised multidomain interventions be delivered by multidisciplinary teams including occupational therapists and physiotherapists. This includes a conditional recommendation that people with Parkinson's disease specifically be offered multidomain interventions, with further research required. 6
Our research team recently designed and tested the Integrate programme: a personalised, multidomain, home-based intervention designed for recurrent fallers with Parkinson's disease, including those with cognitive impairment. 7 Delivered by occupational therapists and physiotherapists, the 6-month programme included home fall-hazard reduction, exercise, and training in safer mobility behaviours. Among 29 participants, the intervention was feasible and appeared to improve safe mobility and reduce falls. 7 To enhance the programme's effectiveness in future trials and large-scale implementation, it is important to understand the perspectives of participants and their care-partners. This qualitative study aimed to evaluate the Integrate programme's acceptability by exploring the experiences of people with Parkinson's disease and their care-partners and factors influencing programme implementation.
Methods
Semi-structured interviews conducted between July 2021 and February 2024 were used to explore participants’ views in depth. Interviews were analysed with reflexive, inductive thematic analysis, using an interpretivist paradigm8,9 that enabled subjective interpretations of experiences without preconceived hypotheses. Ethical approval was granted by the University's Human Research Ethics Committee (2019/034) prior to commencing recruitment. All participants with Parkinson's disease and any participating care-partners provided written informed consent. This study is reported using the Standards for Reporting Qualitative Research. 10
Eighteen interviews were analysed: ten dyads (people with Parkinson's disease and their care-partner), two interviews with only the care-partner and six with only the person with Parkinson's disease. Eligibility for the Integrate study included neurologist-diagnosed idiopathic Parkinson's disease, experienced at least two falls in the previous six months, and ability to walk independently for at least 10 metres (with or without a walking aid). Participants with significant cognitive impairment (Montreal Cognitive Assessment <19, 11 or a level of functional cognition the researcher deemed required assistance to safely participate) were included if a willing and able care-partner also consented. People with severe cognitive impairment (Montreal Cognitive Assessment < 5) 11 or medical conditions which would interfere with the safety of the study or interpretability of the results (e.g. unstable or severe chronic health conditions, a neurological condition other than Parkinson's disease) were excluded. Participants for this qualitative study were purposively sampled from the broader participant pool to ensure diversity in sex, disease severity, fall rates and adherence to the Integrate programme. Sampling continued until data saturation was reached with no new ideas emerging from the data. No participants who completed Integrate declined to be interviewed.
Details of the Integrate programme are reported elsewhere. 7 Briefly, participants completed a six-month, home-based and personally tailored multidomain programme to improve mobility safety and reduce falls, delivered collaboratively by occupational therapists and physiotherapists. Participants received 8 to 12 therapy sessions based on personal need. The first six participants received an average of 4 sessions via telehealth using videoconferencing software due to the COVID-19 pandemic; the remainder was home visits conducted in person. The programme included home fall-hazard reduction (e.g. decluttering, bathroom rails), exercise (for leg muscle strength, balance and freezing of gait) and training in safer mobility behaviour strategies (e.g. slowing down and concentrating in risky situations). Tailoring was based on each participant's functional cognition, 12 physical ability, home environment and care-partner support, with a focus on collaborative goal setting and problem solving between therapist, person with Parkinson's disease and care-partner.
Semi-structured interviews lasting up to 60 minutes were conducted with the participant at home, over the phone or via video call based on participant preference. Interviews were conducted 1 to 2 weeks after the post-intervention assessment. Participating care-partners were interviewed alongside the person with Parkinson's disease. The female interviewer (RS) was an experienced research physiotherapist; she had previously conducted research interviews and received training and guidance from researchers with qualitative experience (NEA and CGC). Participants were aware that the interviewer was a physiotherapist as she completed the post-intervention assessments, but participants had no other relationship with her. The interviewer was not involved in delivering the intervention, thereby minimising potential bias in her approach or in participant responses. An interview guide with prompts was used to ensure consistency while allowing flexibility to probe responses as needed (see Online Supplementary Material 1). The interviewer recorded field notes at the end of each interview. Interview audio was digitally recorded and transcribed verbatim by a transcription service. Member checking was not used to avoid overburdening participants. 13 Instead, the interviewer summarised and checked the key points with the participants at the end of each section of the interview.
Data was analysed thematically 8 by a team of physiotherapy researchers with qualitative research experience (NEA, LG, SSP), physiotherapy honours students (AD, ST) and a medical student who was also an occupational therapist (CK). Analysis was facilitated by NVivo 14 (Lumivero, Denver, CO). All transcripts and field notes were read multiple times and coded line by line by one researcher (NEA) and by at least one other researcher to achieve researcher triangulation. Codes reflecting similar ideas were grouped into themes and subthemes through an iterative process of discussions amongst the team until consensus was reached. Final themes were agreed upon by all authors. To protect participant privacy quotes have been anonymised.
Results
Participant characteristics are presented in Table 1. Overall, participants were a mean (SD) of 14 (7) years since diagnosis, had moderate to advanced Parkinson's disease and fell recurrently, with a median of 22 falls per person in the year prior to commencing the Integrate programme. Eleven (61%) were male and 17 (94%) were living with a care-partner, typically their spouse/partner. Exercise adherence data was available for 15 participants (83%) with overall high but individually variable adherence (median of 95% of prescribed exercise sessions completed, range 12–221%). Adherence to the home hazard reduction was available for all participants, with a median of 100% (range 67–100%) of recommendations partially or fully completed. Adherence to the safer mobility behaviour strategy intervention was available for 11 participants (61%) who reported using the strategies a median of 75% (range 50–87%) of the time.
Characteristics of the participants with Parkinson's disease.
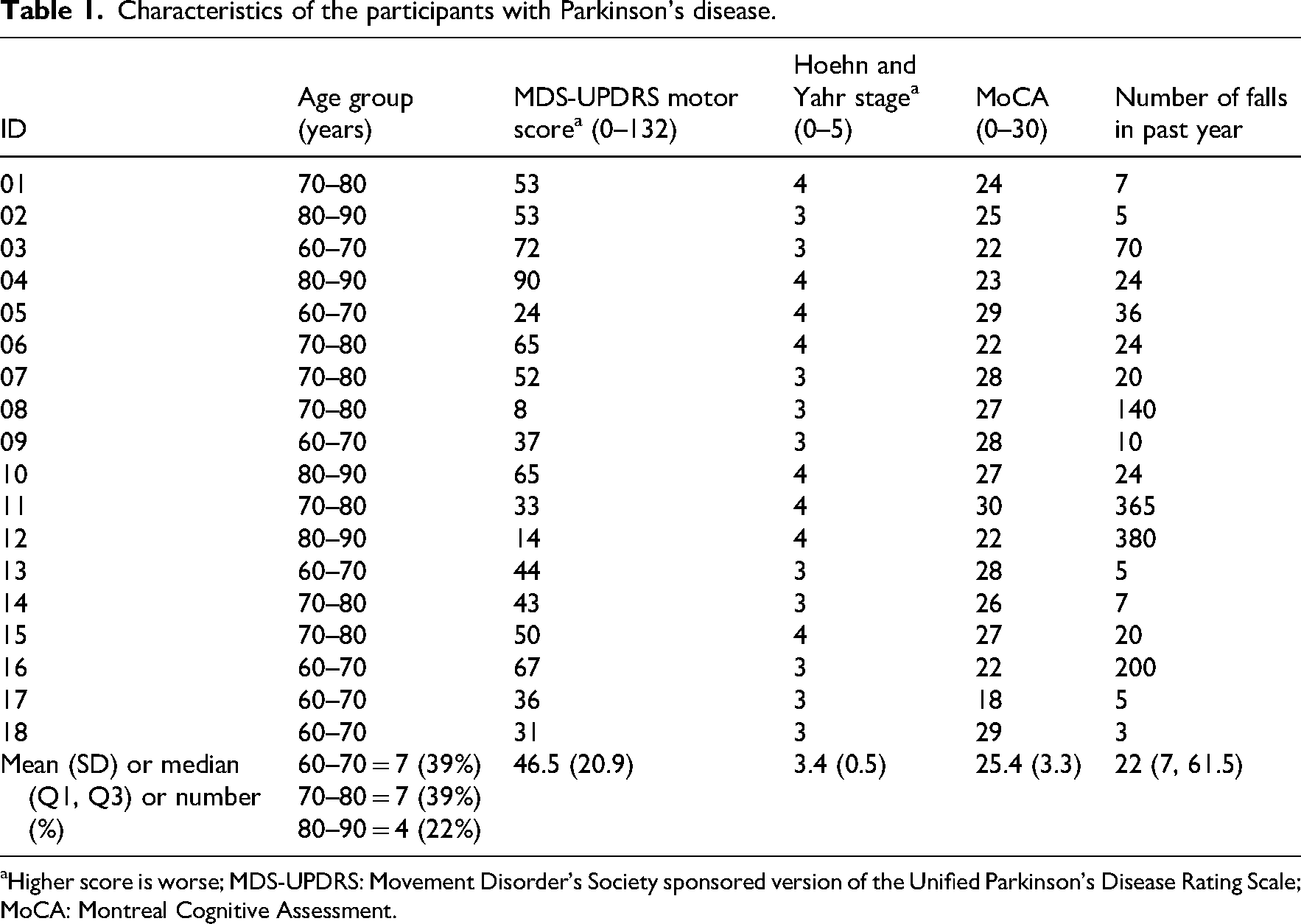
Higher score is worse; MDS-UPDRS: Movement Disorder's Society sponsored version of the Unified Parkinson's Disease Rating Scale; MoCA: Montreal Cognitive Assessment.
Five main themes with associated subthemes were elucidated from the experiences of people with Parkinson's disease and care-partners regarding the Integrate programme and factors that influenced its implementation (see Online Supplementary Material 2).
The importance of personalisation
Tailor-made for one
Participants appreciated the programme was individualised to address their personal Parkinson's disease impairments (e.g. freezing of gait) and activity limitations. They described previous experiences in ‘one size fits all’ group programmes as not entirely meeting their complex needs. The delivery of the programme in the home environment was a key part of the tailoring process, as therapists could contextualise the individual's mobility problems. Being at home allowed ‘a complexity and variety’ (care-partner ID 02) along with a level of safety in the exercise set up that people had not experienced when translating interventions from the clinic to the home. …having someone come in to look at the home is useful because it mirrors the same activities and environment that I have to deal with every day. (ID 11)
The programme was flexible to meet needs
In addition to the programme being personally tailored, participants appreciated that it could be adapted to accommodate unexpected or additional constraints, such as busyness, fatigue or pain. There was also the ability to modify that exercise or to say that the exercise is not suitable for me at the time because I have the additional back surgery. (ID 11)
A collaborative effort
Involvement in decision making
Participants reported they were able to have a ‘personal exchange of ideas’ (ID 02) and conversations with the therapists that were ‘guiding’ (care-partner ID 10). This fostered a sense of ownership over their intervention and empowered them to raise concerns when things weren’t working optimally, leading to trialling different strategies to find the most effective solution. …it wasn’t like a doctor–patient thing, it was very much a ‘we’re in this together’ sort of thing… (ID 07)
The value of expert knowledge
Participants valued therapists’ extensive knowledge about Parkinson's disease and intervention that specifically accounted for their problems. Some explained that they had not made home safety changes earlier as they did not know what changes to make. Several noted that they now had strategies that helped them to manage their freezing of gait and therefore walk more safely. But it is rather marvellous having people who are specifically working with Parkinson's people. (care-partner ID 02)
However, one participant felt the programme did not add to their knowledge about safer mobility due to previous health professional input. I’ve been along that sort of track several times now with the specialist… there's not much I could add. (ID 04)
Support and accountability
Regular discussions with the therapists provided support and positive reinforcement that helped participants to adhere to the programme and continually adapt it to their needs. One participant described the therapist as ‘a voice on my shoulders’ (ID 07) encouraging her to use her safer mobility strategies. One care-partner whose spouse did not enjoy exercise described how the therapist's affirmation of his struggles and thoughtful advice helped him to exercise and ‘sort of gave him a pick me up for the day…’ (care-partner ID 06). Care-partners highlighted the importance of consistent, one-on-one care, particularly for participants with cognitive impairment. Collaborative goal setting and problem solving promoted a sense of personal responsibility in directing their own care and fostered self-management skills. …we have to own these problems, you know, they’re not somebody else's’ problems, they’re my problems, and the only person that can do it is me. (ID 07)
For most participants, care-partners played an important supportive role, providing encouragement and prompts to exercise and use safer mobility strategies. Active care-partner involvement also ensured participants completed the intervention optimally and remained committed to the programme. I find it hard to get up but if I’ve got somebody pushing me or motivating me, I find it easier. (ID 09)
Care-partners also expressed that they felt reassured and supported by the therapists. This support was enhanced when participant dyads shared mutual beliefs about the benefit of the intervention. However, when beliefs were conflicting, the care-partner was less able to encourage positive change and at times tension arose in the relationship. Person with Parkinson's disease: My brain's going to get worse. Doing exercise or whatever, it's still going to get worse. I can’t see the point. (ID 12) Care-partner: I can see the benefit. He can’t. As to improve his situation. I think if he did the exercises, it would make him stronger, in his legs, but he doesn’t think it will. (care-partner ID 12)
Capacity building
Planning to be safe
Participants described how the programme taught them to identify risky situations and be more mindful of safety when moving. They described how they planned ahead, adjusted the environment, sought help from others or took extra care, including using their safer movement strategies. This led to greater willingness and confidence in engaging in daily activities. I’m conscious of maintaining balance. I’m more conscious of the way I’m walking. I tend to think more about what I’m doing before I do it. So, it's increased my awareness of not getting into situations where I used to before and put myself in danger. (ID 09)
Some participants chose to avoid activities they felt they were unable to complete safely. In contrast, one spoke of increased confidence in his abilities after completing the programme but reflected that at times this led to carelessness. Because I think I feel more confident going and doing things. It's given me more confidence, I guess, and maybe the more I fall. (ID 10)
Despite the ability to identify risky activities, a few participants noted that the desire or need to undertake the activity superseded any concern about falling. One described needing to leave his walker behind when working in his garage as the space was not conducive to using a mobility aid. Another felt compelled to climb a stepladder to reach an item as there was no-one else to do it. Participants described how they were careful when doing these activities. While participants noted that increased safety awareness helped to reduce falls, some found the extra vigilance difficult to maintain. …I have been known recently to climb on a little two step because I needed to get something in a top cupboard… but should I lose the balance I’ve got something to hold onto. (ID 11) I have to be aware 24 hours of the day. (ID 07)
Adapting and equipping for the future
Participants were able to extrapolate from their prescribed home hazard reduction recommendations and safer movement strategies and develop their own strategies in different and novel situations. One participant described how she implemented her own movement strategy to make golfing safer. … when I’m hitting a ball, instead of going back to […] my buggy or whatever, I have to now – and I’ve only just worked this out […] push it forward quite a few steps before I hit it so that I’m going forward, not backwards. So, there are sort of things like that I’m trying to initiate if I can. (ID 07)
Participants also described how their new awareness, knowledge and skills in planning to be safe would equip them to solve mobility safety issues into the future. They described improved awareness of when to seek help and would likely seek expert advice before making any significant changes in relation to home hazard reduction. When we’re about to do that I’d more than likely contact an OT, to go through the process of getting their opinion on what we want to do and whether it's feasible or a waste of time. (ID 09)
Navigating fall risk with Parkinson’s is complex
The reality of Parkinson's as motivation
Having a progressive condition motivated participants to complete the Integrate programme as they wanted to remain physically mobile, minimise falls and get up from the floor independently.
… on the floor and being unable to get up and just sit there, I could not bear to have that happen again. (ID 02)
For some, the realisation that they had already experienced deterioration underscored the necessity of the intervention, prompting them to take action to reduce their fall risk. I knew I needed them [rails in the bathroom]…because I’d had a couple of falls in the bathrooms, and I did not want to have anymore. (ID 07)
Participants often described how education and support from the therapists helped them reframe Parkinson's disease as a manageable condition. Several reported how having goals to strive for motivated them to keep trying.
I think it's a motivation rather than a programme. You give me something to achieve – to aim for. I didn’t achieve the maximum – but I’m always trying to do better. (ID 08)
Emotional and psychological resistance to changes: Participants described affective barriers that made it difficult for them to engage with the programme. A few were fatalistic and had little motivation to complete the programme, believing that the progressive nature of Parkinson's disease made any long-term benefit unlikely.
…but it's [any benefits] all so subtle you don't notice it. (ID 13)
Some participants were reluctant to implement home hazard reduction measures due to concerns about aesthetics and the emotional impact of acknowledging functional decline, viewing it as ‘an admission of disability’ (ID 09). Safer mobility strategies were sometimes conspicuous, and one participant expressed this was a barrier to using her strategies in public, as a friend had commented that it looked ‘funny’ (ID 07). Nonetheless, therapists were often able to help people with Parkinson's disease accept and use equipment or strategies. …[Spouse] is a very proud man, and he thought it was, not degrading but…not something he’d want to use, but when [the therapist] suggested it, he went along with it, and he does use it. (care-partner ID 10)
A few wanted to continue undertaking certain high-risk activities, as they did not want to admit they were not able to do them safely anymore. I got into trouble once when I got [the handyman] to start the chainsaw and I used it. [Spouse] came straight out and said what is going on, why are you using that?… I was a lot more cautious than I used to be with it, but I should not be doing this at all. (ID 09)
Parkinson's takes control
Some people with Parkinson's disease expressed frustration with their impairments interfering with their ability to engage with the programme. They spoke of challenges due to poor memory, fatigue, apathy, anxiety and motor fluctuations. Unfortunately for [spouse] he can vary so much from day to day… the Parkinson's seems to just take hold on a particular day. No reason or rhyme particularly and no particular time of day… (care-partner ID 09)
The ease (or not) of making changes
System barriers
For larger home fall-hazard reduction changes such as installation of ramps and rails which required external service providers, participants often cited barriers and lengthy delays related to government means testing and approval processes. The occupational therapist was able to guide people through the process and expedite it when necessary. We were put on a waiting list for the ramp, and then [spouse] was having falls, and I let them know, but still waiting, and I think [the occupational therapist] approached them and it wasn’t long after that the builder came. (care-partner ID 03)
Competing priorities
Competing priorities affecting time, energy and money influenced programme adherence. Most participants reported they had plenty of time to undertake the program, as they were retired and the COVID-19 pandemic restricted their social life. Others described difficulty finding time to exercise or preferring to do exercises and physical activity different to ones prescribed. Additionally, participants spoke of having a finite amount of physical and cognitive energy with which to achieve their daily tasks and explained that completing the programme was not always their highest priority. Participants also spoke of competing financial priorities preventing them from making some of the home fall-hazard reduction changes. I’ve got a lot of little jobs going on around here that occupy my mind… I found that I just didn’t have the time. The speed I work at now is dead slow. (ID 06) I am planning to make that change [handheld shower], it's just unfortunately my hot water service went, the roof went with the floods. I've had to replace a few things that have cost a few thousand dollars, so even though it was only [approx. $260 AUD]… but I need a new fridge, and I need a hot water system. (ID 11)
Making new habits is hard (but possible)
Participants spoke of difficulties establishing new habits for exercise or using safer mobility strategies. They described that a regular exercise habit was made easier by therapists assisting them to determine how they could build the exercise into their daily routines. The provision of a simple instruction booklet with pictures also helped, with some using the booklet as a prompt to exercise. Therapists promoted the use of safer mobility strategies through repetition, mantras (e.g. stop, think, be safe), and signs and notes placed strategically in the environment as reminders. We had a ‘big’ mantra for a long time that works very well. (care-partner ID 02)
Care-partners often provided prompts for completing the exercises and using the safer mobility strategies. Notably, some care-partners expressed that they would regularly prompt the safer mobility strategies, but preferred not to prompt the exercise too often as they felt it was bad for their relationship. And for me trying to tell him is no good either. It's just I’m a nagging wife. (care-partner ID 18)
Participants also described the environment itself became a cue to use a safer movement strategy, as they had repeatedly practiced the strategy in that area. They became better at recognising near falls or precursors to falls, such as gait festination, and used these as prompts to implement their safer mobility strategy. Many participants reported that at least some of their strategies were becoming a habit, though often they could not say how the habit formation had occurred. …it's subconscious, I do it all the time, I don’t even have to think about it. (ID 09)
Discussion
This study found the Integrate multidomain fall prevention programme for people with Parkinson's disease to be acceptable. People with Parkinson's disease and their care-partners valued the shared decision-making approach of expert therapists and skills learnt to improve the safety of their mobility. Participants were motivated to engage with the programme to optimise mobility and reduce falls, despite challenges in forming new habits. Barriers to engagement included fatalistic beliefs about Parkinson's disease, emotional and psychological difficulties accepting changes, interference from impairments and motor fluctuations, competing priorities and systemic barriers to modifications.
This study builds on previous fall prevention and exercise-based research, including the PDSAFE trial,14,15 which offered a personalised, home-based programme consisting of fall prevention exercise and strategies delivered by physiotherapists. Like Integrate, PDSAFE participants 15 valued the personalised programme and therapist and care-partner support, noting benefits in mobility, confidence and independence while barriers included time constraints, low motivation and Parkinson's-related impairments. 15 Other studies16–18 similarly identified that personalised approaches, participant empowerment and therapeutic partnerships facilitated engagement, while competing demands, non-motor impairments and psychological and emotional responses were barriers.
The acceptability of home fall-hazard reduction for people with Parkinson's disease has been underexplored. This study identified factors influencing adherence that align with findings in the general older population, including greater willingness to modify the home when the need and benefits were clearly understood.19,20 Shared decision making with expert therapists improved tailoring and acceptance of recommendations.20,21 Barriers mirrored those in previous research, including competing priorities (financial and time),22,23 stigma around aesthetics19,20 and system challenges20,23 such as navigating processes and delays in subsidised modifications. Support from healthcare providers (e.g. occupational therapists), particularly in coordinating with external agencies, can improve implementation. 24
Little is known about the acceptability of safer mobility strategies. Previous research with older adults 25 and people with Parkinson's disease26,27 described how people balanced the risk of falling with their desire to engage in enjoyable activities, maintain independence and live a ‘normal’ life. In this study, most participants were motivated to use safer mobility strategies to reduce their risk of falling, with greater movement awareness and planning for safety during risky activities. Reminders from care-partners, signs, notes, mantras and practice in the appropriate environment encouraged use of these strategies. However, making new safer mobility strategies a habitual part of daily routines was challenging. Habit formation involves cue-association mechanisms learned through repetition in specific contexts. 28 People with Parkinson's disease may struggle to establish new habits due to deficits in automaticity and motor learning. 29 Nonetheless, some participants in this study developed habits through intentional and context-driven practice over 6 months. Research is required to further explore strategies to optimally promote habit formation in people with Parkinson's disease, including those with cognitive decline.
Several clinical implications for fall prevention in people with moderate to advanced Parkinson's disease are highlighted by this study. Multidomain interventions are complex, therefore care-partners play an important role by supporting, encouraging and prompting participants. This was particularly important for those with impaired cognition. Care-partners therefore require appropriate training and support to fulfil their role safely and effectively without adding to their burden of care. Health professionals should also consider any potential psychological and emotional barriers to adopting fall prevention programmes, including difficulty accepting change, fear of appearing ‘disabled’ and fatalistic beliefs. Empathy and support from therapists can help people adjust to changes as their needs evolve over time.
Health professionals should also uphold the principle of dignity of risk, 30 allowing people with Parkinson's disease autonomy to choose which recommendations to follow. Some participants chose to undertake certain high-risk activities as the desire or need to undertake the activity outweighed the risk of falls. Further research is required to explore optimal implementation of this principle in clinical practice and the role of behaviour change techniques to address barriers to fall prevention, 31 such as social support and reframing perspectives on change. Such research may provide additional insights into increasing acceptance and adherence to fall prevention strategies.
This study also underscores the importance of involving people with Parkinson's disease and their care-partners in shared problem solving and collaborative goal setting. Participants valued being involved in individualising their fall prevention programme, which increased engagement. Equipping people with Parkinson's disease and their care-partners with fall-prevention knowledge and skills will help build their capacity to manage falls now and into the future when circumstances change.
This study had several limitations. The sample consisted of volunteers, who were possibly more motivated than the general Parkinson's population. Insights from less interested individuals may be lacking. Furthermore, although the study included participants with impaired cognition, those with severe cognitive impairments were excluded, meaning their perspectives and those of their care-partners were not represented. Despite encouragement for honest feedback, participants may have given positive responses to please the interviewer or avoid seeming critical.
In conclusion, this study provides new insights into how people with Parkinson's disease and their care-partners engage with a multidomain fall prevention intervention. Engagement was enhanced by the personalised and collaborative approach between participants and therapists. Participants felt empowered and better equipped to identify and address mobility safety-related problems and were motivated by their own improvements and their desire to remain independent. Conversely, engagement was hindered by fatalistic beliefs, emotional and psychological readiness for change, Parkinson's disease impairments, competing priorities and system-related barriers. Future research should address these barriers and further investigate the benefits of tailored, multidomain interventions on reducing falls in people with Parkinson's disease.
People with Parkinson's disease who have recurrent falls plus care-partners found a home-based multidomain fall prevention programme acceptable. Participants valued individualised programmes, shared decision-making, therapist expertise and increased their safety awareness during movement. Emotional and psychological barriers, such as fear of appearing disabled, need to be addressed.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155251365151 - Supplemental material for Acceptability of a programme for safer mobility (INTEGRATE): Perspectives of people with Parkinson’s disease and their care-partners
Supplemental material, sj-docx-1-cre-10.1177_02692155251365151 for Acceptability of a programme for safer mobility (INTEGRATE): Perspectives of people with Parkinson’s disease and their care-partners by Natalie E Allen, Annabel Darmali, Cecelia Koch, Sammi Tran, Serene S Paul, Colleen G Canning, Simone Edwards, Susan Harkness, Roslyn Savage, Lyndell Webster, Genevieve Zelma and Lina Goh in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155251365151 - Supplemental material for Acceptability of a programme for safer mobility (INTEGRATE): Perspectives of people with Parkinson’s disease and their care-partners
Supplemental material, sj-docx-2-cre-10.1177_02692155251365151 for Acceptability of a programme for safer mobility (INTEGRATE): Perspectives of people with Parkinson’s disease and their care-partners by Natalie E Allen, Annabel Darmali, Cecelia Koch, Sammi Tran, Serene S Paul, Colleen G Canning, Simone Edwards, Susan Harkness, Roslyn Savage, Lyndell Webster, Genevieve Zelma and Lina Goh in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors would like to thank the participants in this study.
Author contributions
NEA, SSP, CGC, contributed to the concept and design of the study, NEA, SSP, SH, RS, LG organised the study, NEA, SE, SH, RS, LW, GZ, LG provided the intervention and collected the data, NEA, AD, CK, ST, SSP, LG completed the analysis and interpretation of the results, NEA, AD, CK, ST, SSP, CGC, SE, SH, RS, LW, GZ, LG contributed to the writing of the manuscript.
Ethical considerations
This project received ethical approval from The University of Sydney's Human Research Ethics Committee (ref: 2019/034).
Consent to participate
All participants provided written informed consent prior to enrolment.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by a Parkinson's NSW Research Grant, a University of Sydney Laffan Equity Prize and The University of Sydney DVCR Support Fund for COVID-19 impacted research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability
The data supporting the findings of this study are available within the article. Individual transcripts cannot be provided as participants did not provide consent for that.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.