
Abstract
Objective
To determine the effect of education programs on fatigue outcomes in people with neurological conditions.
Data sources
MEDLINE, CINAHL, EMBASE, PEDRO until May 2025, according to PRISMA guidelines.
Review methods
Systematic review with meta-analysis of randomised controlled trials comparing education versus no education/other intervention on the outcome of fatigue for people with neurological conditions. Methodological quality and risk of bias were assessed using the Cochrane Risk of Bias Tool. Pooled effects were calculated using standard mean difference (SMD).
Results
We included 19 clinical trials of education for fatigue (n = 1970 participants) in five different neurological conditions. Education duration ranged from 4 to 12 weeks, 79% (n = 15) of trials included people with multiple sclerosis and 18% (n = 3) included people with stroke. Most education (11 trials, 58%) was delivered in a group setting. Education reduced fatigue compared with usual care by a SMD −0.28, 95% CI [−0.45 to −0.11]. Greater benefits for fatigue were observed when education was delivered one-to-one (SMD −0.44, 95% CI [−0.77 to −0.12]) than in group sessions (SMD −0.17, 95% CI [−0.36 to 0.01]). Mode of delivery (in-person versus telehealth) did not appear to influence the effect of education for fatigue.
Conclusions
Fatigue education programs may improve fatigue for people with neurological conditions. One-to-one delivered sessions may have greater benefits than group programs and remote delivery could improve accessibility for people living in regional and rural locations.
Introduction
Fatigue is a common and disabling impairment for people living with a neurological condition. Fatigue affects around 36–78% of people with multiple sclerosis, 1 21–73% of those with post traumatic brain injury and 50% of people living with stroke. 2 While there is no consistent definition for fatigue, neurological fatigue is described as an overwhelming feeling of exhaustion or tiredness, a lack of perceived energy that does not typically improve with rest and is distinct from sadness or weakness.3,4 Neurological fatigue negatively affects participation in activities of daily living, employment and overall quality of life.4–6 With such a high incidence and impact of neurological fatigue, there is a critical need for evidence-based interventions to address this unmet need. 7
Unfortunately for many neurological conditions, fatigue research is either in its infancy, possibly because of the complexity of the phenomenon and lack of mechanistic understanding. 8 Consequently, it is challenging for health professionals to know what to offer patients.9–11 Pharmacological interventions have not shown consistent positive benefits for reducing fatigue and the evidence is low quality in most neurological populations.10,12,13 Education is commonly provided by health professionals and actively sought by people living with health conditions. Clinical guidelines for post-stroke fatigue recommend that health professionals provide education about fatigue but these guidelines are based on consensus level evidence.14–16 Fatigue management related to multiple sclerosis has a more established evidence base that suggests treatment benefits for medications, exercise and importantly, for education. 11
Health-related education is designed to improve knowledge, health literacy and influence motivation. 17 Active education interventions use a variety of behaviour science methods however techniques are challenging to define, differentiate and are often poorly reported in clinical trials. Despite these limitations, education interventions have been shown to improve symptom management and quality of life for people with other complex and challenging conditions, such as chronic pain, 18 lung disease 19 and cancer-related fatigue. 20 Education interventions show promise for people with multiple sclerosis-related fatigue.11,21 However, there is scarce literature around whether people with neurological fatigue from other common neurological conditions such as stroke, Parkinson’s disease or traumatic brain injury would benefit from education for fatigue. Furthermore, given that there are multiple ways of delivering education such as individually, in a group, in person and now more commonly via telehealth, how education is delivered could influence the outcomes for people with fatigue.
Therefore, in this systematic review, we aimed to answer the following research questions:
For people living with a neurological condition;
Are fatigue education programs of benefit for reducing fatigue? Is the effect on fatigue dependent on intervention delivery (one-to-one/group, in-person/online)?
Method
This review was registered with Prospero, the International Prospective Registry of Systematic Reviews (Registration Number CRD42023466070) and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Inclusion criteria were (1) randomised controlled trials that aimed to reduce fatigue, and where fatigue was the primary outcome of interest (2) adults (> 18 years) living in the community with a diagnosis of a neurological condition and experienced self-reported fatigue, (3) at least one outcome measure of fatigue, (4) active education-based intervention and, (5) full text available in English. Eligible interventions were any active education-based intervention that aimed to improve knowledge and promote skill acquisition relating to fatigue management. Education was defined using the World Health Organisations definition, ‘…any combination of learning experiences designed to improve health literacy, including improving knowledge and developing life skills which are conducive to one-to-one and community health. This may involve fostering motivation, skills and confidence necessary to take action to improve health’. 17 Exclusion criteria were non-neurological conditions with fatigue and psychology specific interventions, for example, acceptance and commitment therapy.
A comprehensive search strategy was developed and searches conducted for studies published prior to May 2025 using the following databases: MEDLINE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), EMBASE, and the Cochrane Library and Physiotherapy Evidence Database (PEDRO). The search strategy was developed in MEDLINE and adapted to each database. Medical Subject Headings (MeSH) terms included (but were not limited to), ‘fatigue’, ‘Patient Education’, ‘self-management’, ‘Psychoeducation’, ‘stroke’, ‘Multiple sclerosis’, ‘Parkinsons disease’, ‘Brain injuries’ and ‘randomised control trials’.
Two people independently completed the initial screen of titles and abstracts, reviewed the full texts and assessed risk of bias using the Cochrane Risk of Bias Tool (RoB 1.0). Disagreements were resolved by discussion, and a third reviewer was consulted when required.
Information about the method (i.e. design, participants, intervention, measures) and results (i.e. number of participants, and means (SD) of outcomes related to fatigue) were extracted by one reviewer and checked by another reviewer. The immediate post-intervention scores of the primary fatigue outcome measure were used to obtain the pooled estimate of the effect of the intervention, using a random effects model. Because trials used a range of different outcome measures for fatigue, we used standardised mean differences (SMD) for pooled effect estimates. In the case of co-primary outcomes, we used data from the two most commonly reported measures across trials (Fatigue Severity Scale or modified Fatigue Impact Scale). As specified a priori, we conducted subgroup analyses to look for differences in effects based on neurological condition and on intervention characteristics including setting (one-to-one versus group) and mode of delivery (in-person versus telehealth). Pooled SMD of <0.2 were considered negligible, 0.2 to 0.49 were considered small, 0.5 to 0.79 were considered moderate and >0.8 were considered large. No additional sensitivity analyses were conducted. We used Grading of Recommendations, Assessment, Development and Evaluation (GRADE) criteria for assessing the quality of the evidence.
Results
The electronic search strategy identified 1039 papers of which 293 duplicates were removed. After screening titles, abstracts and reference lists, 85 full texts were retrieved and reviewed for eligibility. Sixty-six papers did not meet the inclusion criteria and 19 trials were included in the final review (Figure 1). The 19 trials (reported in 24 papers) included a total of 1970 participants. Characteristics of the included trials are presented in Table 1. The average age of participants across the trials ranged from 40 to 72 years. Fourteen trials included people with a diagnosis of multiple sclerosis, three included people living with stroke, one included people living with a traumatic brain injury, and one included a mixed population (multiple sclerosis, Parkinson’s disease and post-polio syndrome).
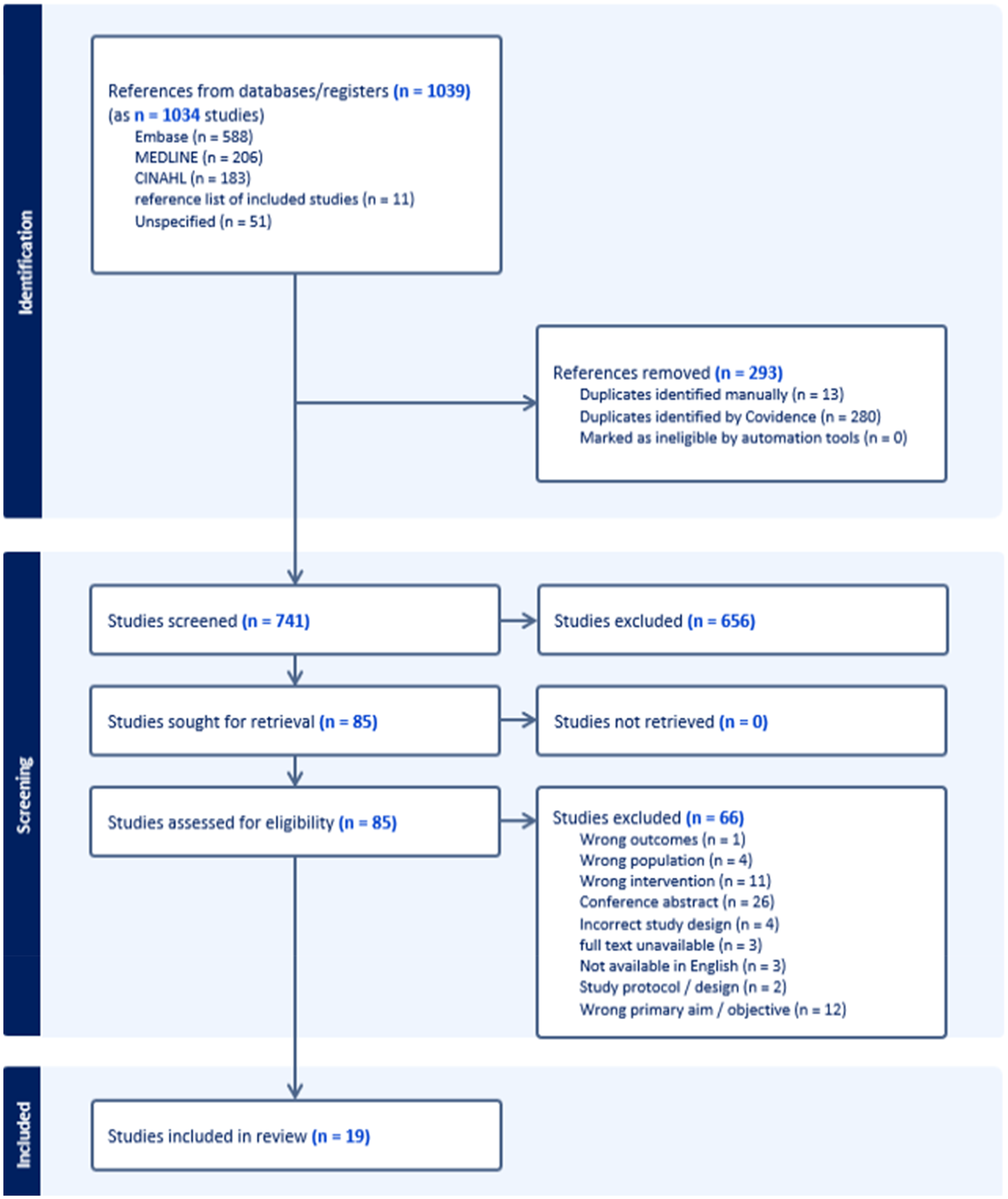
Flow of studies through the review.
Characteristics of included trials.
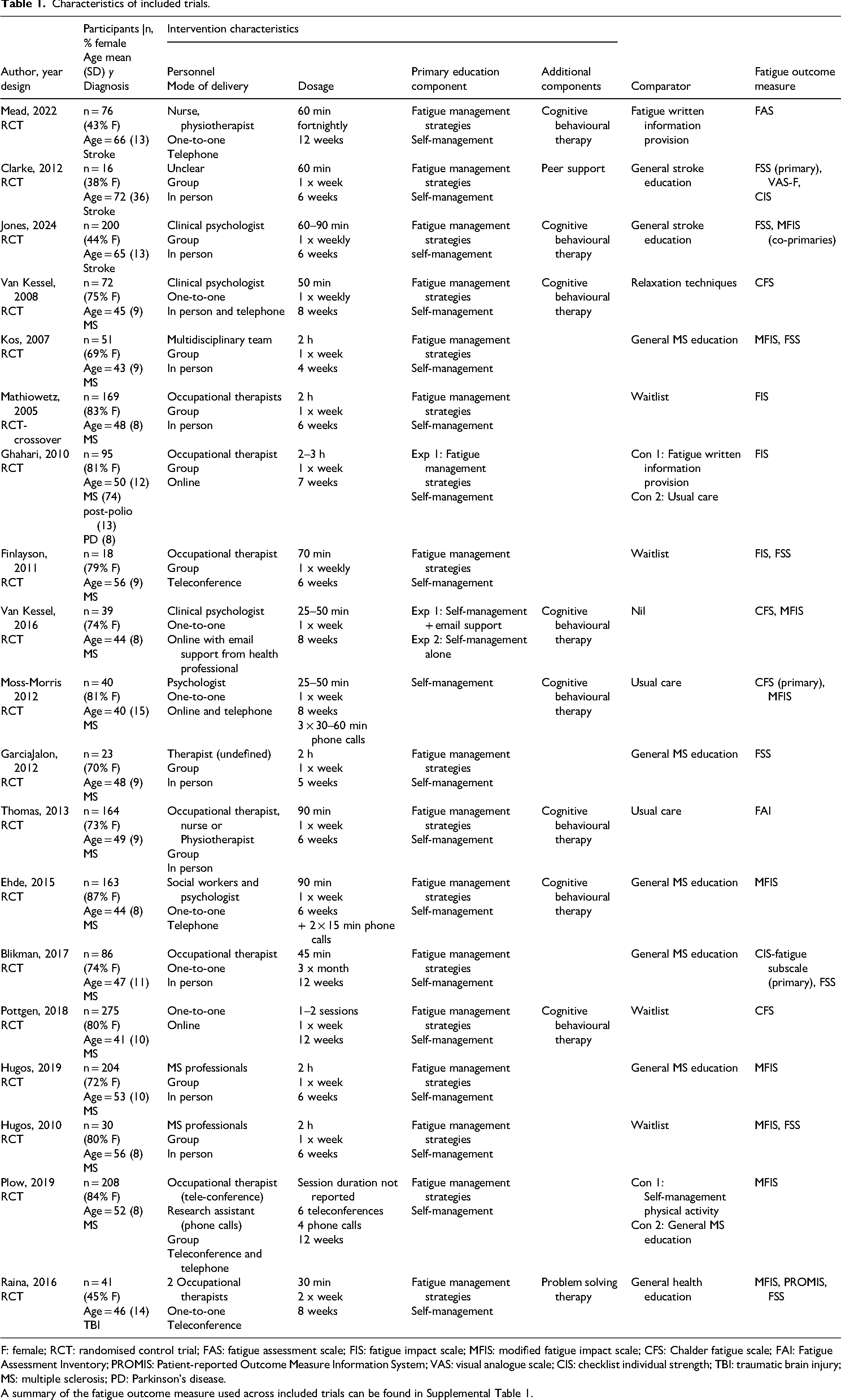
F: female; RCT: randomised control trial; FAS: fatigue assessment scale; FIS: fatigue impact scale; MFIS: modified fatigue impact scale; CFS: Chalder fatigue scale; FAI: Fatigue Assessment Inventory; PROMIS: Patient-reported Outcome Measure Information System; VAS: visual analogue scale; CIS: checklist individual strength; TBI: traumatic brain injury; MS: multiple sclerosis; PD: Parkinson's disease.
A summary of the fatigue outcome measure used across included trials can be found in Supplemental Table 1.
The experimental intervention was fatigue education programs. All trials included some form of behaviour change strategy, such as cognitive behavioural therapy principles and/or self-management principles. Similarly, all trials provided education on energy conservation principles and/or general fatigue management strategies. Personnel involved had a range of experience and/or training in the education tools used, such as cognitive behavioural therapy. In 11 trials the intervention was delivered in a group setting either in person,22–29 or via telehealth.30–32 In eight trials, the intervention was delivered one-to-one by telephone,33,34 telehealth,35–38 or in person.39,40 The intervention duration differed across trials. Ten programs were delivered in six weeks or less, five programs ran for between 7 and 10 weeks and the remaining four programs ran for ≥ 12 weeks.
A range of comparators were used including no intervention (usual care,29,35,41 waitlist control,25,28,30,36), or other intervention (including general health, or disease specific education programs,23,32,33,37,42,43 physical activity self-management, passive fatigue information provision,32,34,41 relaxation program 40 ). Some, but not all of the comparator interventions were attention-matched. One trial compared two active interventions; an online fatigue education program with and without email support. 38 This trial was not included in our meta-analyses. Nine different fatigue outcome measures were used, the most common being Fatigue Impact Scale (seven trials) and Modified Fatigue Impact Scale (six trials) (see Supplemental Table 1 summary of the fatigue outcome measures used across included studies).
Figure 2 presents the results of the risk of bias assessment for each included trial, and Table 2 presents summary of findings and GRADE quality of evidence. The majority of trials (89%) reported appropriate randomisation, allocation concealment (74%) and completeness of outcome data (63%). Due to the nature of the intervention, all trials presented high risk of bias for blinding of participants and personnel. Fifty-three percent of the trials did not clearly report outcome assessor blinding. Other biases included inadequate (42%), or no reporting of statistical power (16%).

Risk of bias.
Summary of findings.
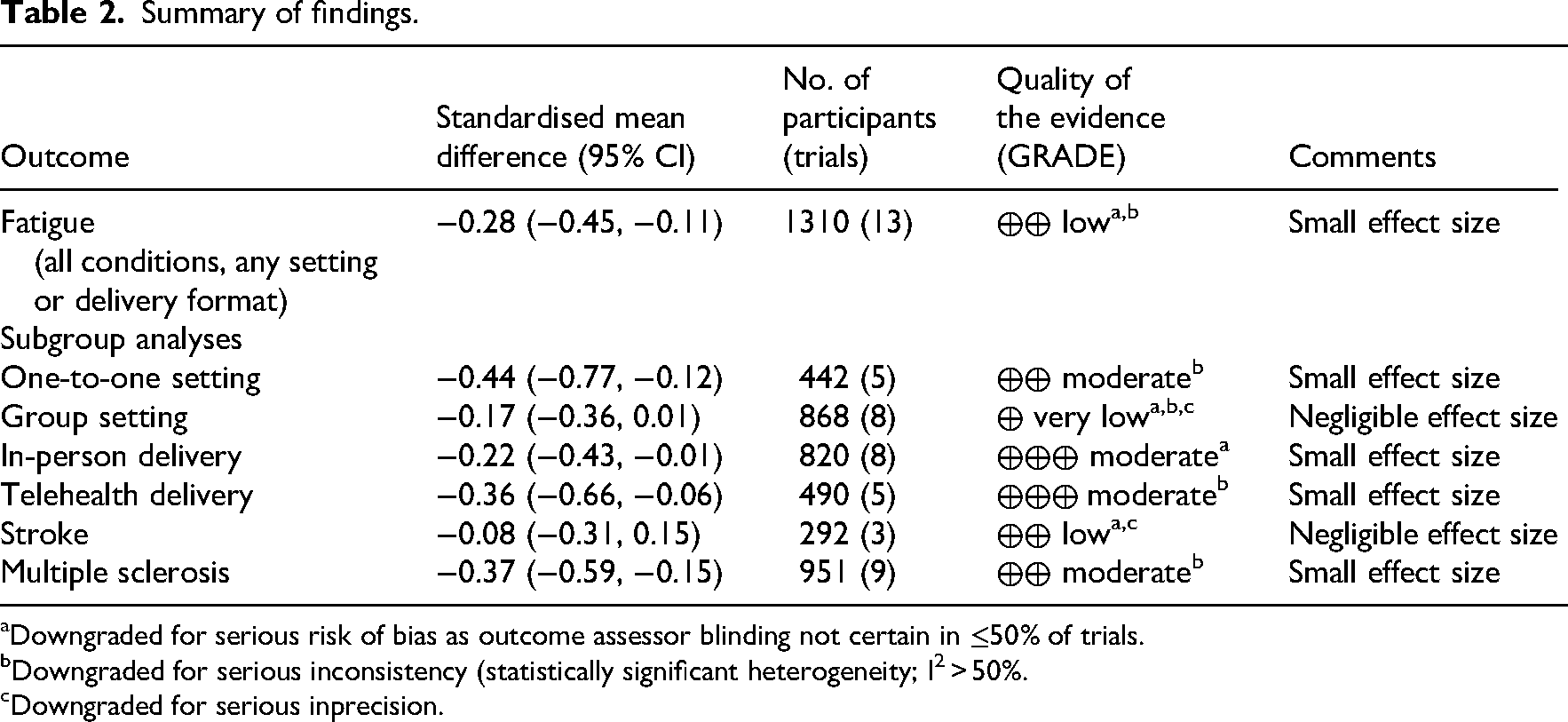
Downgraded for serious risk of bias as outcome assessor blinding not certain in ≤50% of trials.
Downgraded for serious inconsistency (statistically significant heterogeneity; I2 > 50%.
Downgraded for serious inprecision.
Effect of education programs on reported fatigue
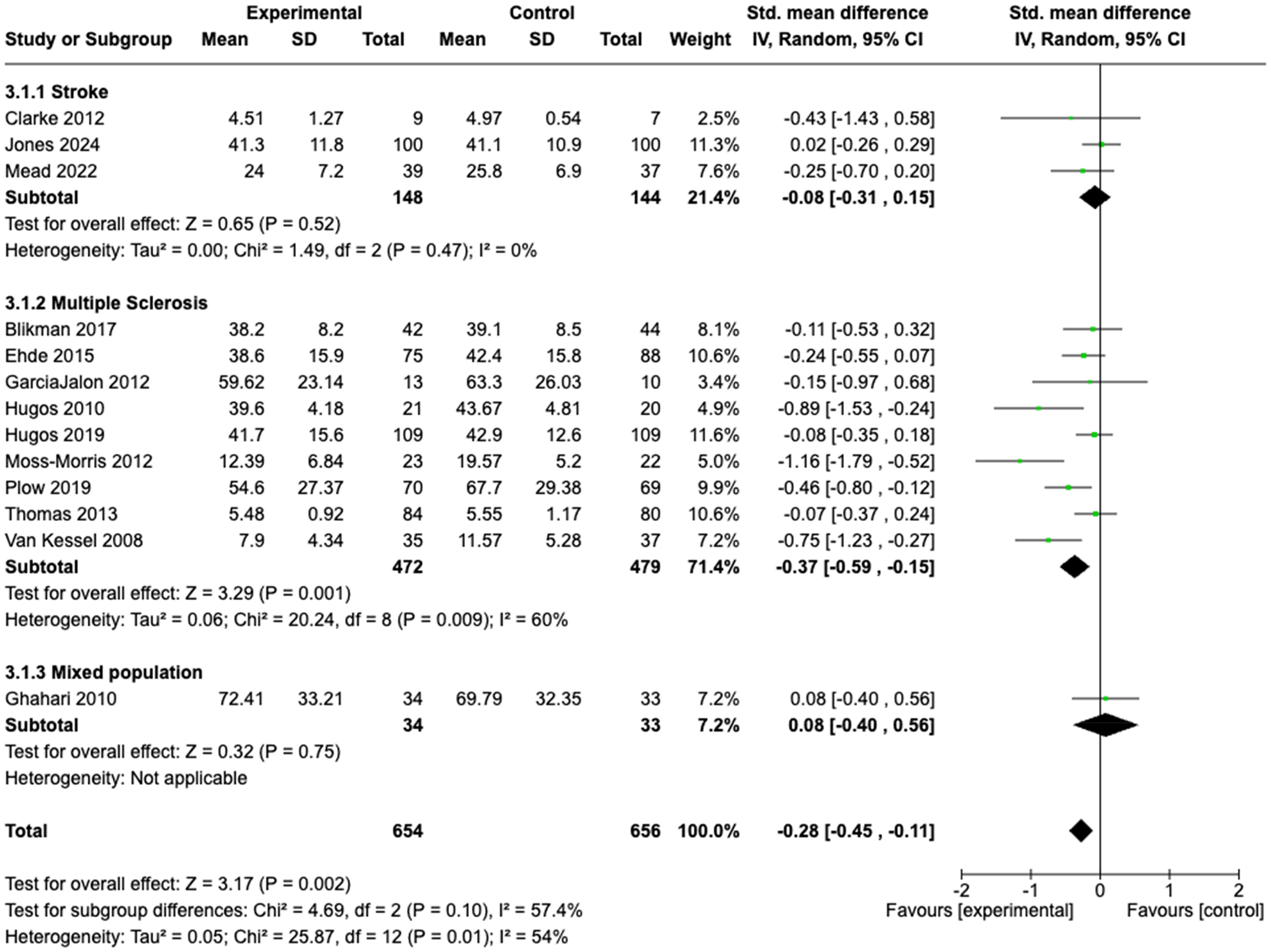
Of the total 19 trials, eight reported statistically significant improvements in fatigue in favour of the experimental group and 11 reported no significant difference between groups. Thirteen trials (n = 1310 participants) had data available for meta-analyses. Figure 3 presents the effect of education programs on fatigue. Panels (a) to (c) present the data according to subgroup analyses for differences in setting (one-to-one versus group), differences in mode of delivery (in person versus telehealth) and differences according to neurological condition.
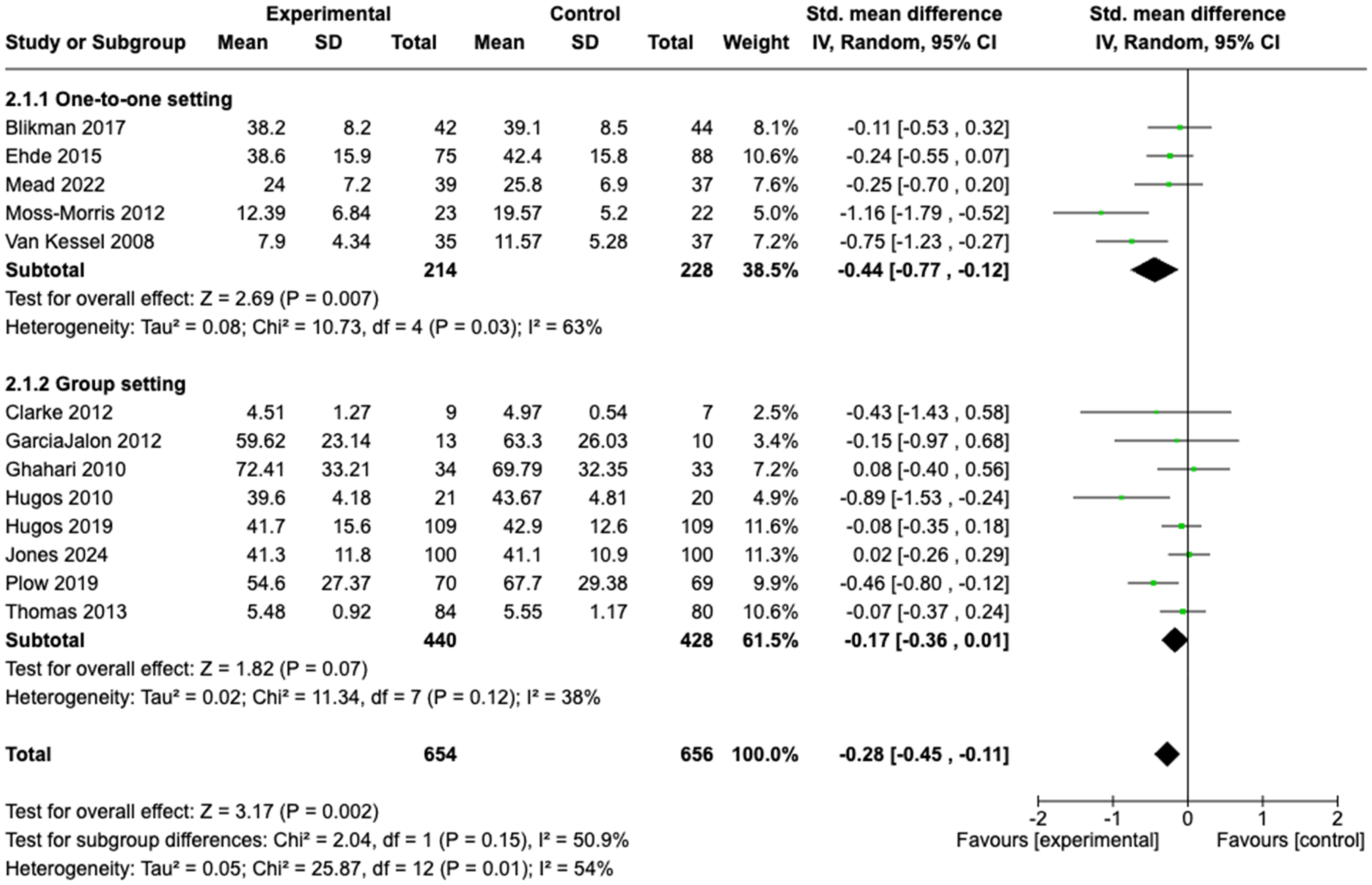
Effect of fatigue education programs: (a) subgroup one-to-one versus group; (b) subgroup in person versus telehealth; (c) subgroup by condition.
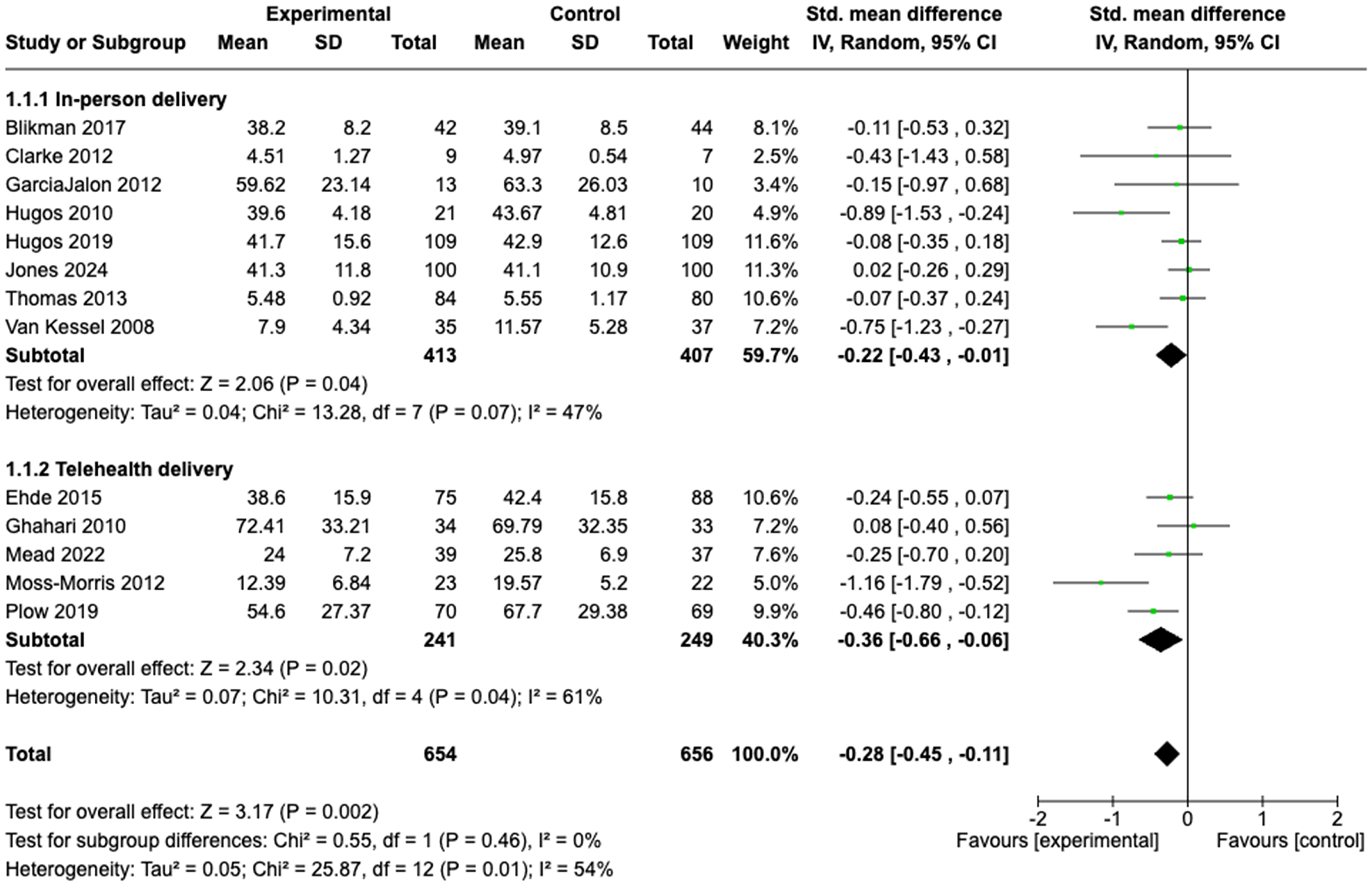
Overall, we found significant between group differences in favour of the experimental group (SMD −0.28; 95%CI −0.45, −0.11). (Figure 3). GRADE quality of evidence is low (downgraded for serious risk of bias as assessor blinding not clear in >50% of trials and downgraded for serious inconsistency due to statistically significant heterogeneity and I2 > 50%).
There were no statistically significant sub-group differences when comparing trials based on the components of the education intervention. However, in terms of intervention setting, interventions provided to participants one-to-one demonstrated a significant, small effect size (SMD −0.44; 95%CI −0.77, −0.12; GRADE quality of evidence moderate) compared with interventions provided in a group setting where the effect size was negligible (SMD −0.17; 95%CI −0.36, 0.01; GRADE quality of evidence very low). Results when comparing interventions delivered via telehealth versus in-person delivery were similar; both demonstrated significant but small effect sizes and GRADE moderate quality evidence (SMD −0.36; 95%CI −0.66, −0.06 and SMD −0.22; 95%CI −0.43, −0.01, respectively).
There were differences in effect based on neurological condition subgroups, albeit not statistically significant. There was no significant intervention effect across the three trials that included people with stroke (SMD −0.08; 95%CI −0.31, 0.15; GRADE quality of evidence low), whereas there was a small, but significant between group effect in favour of the experimental group for trials involving people with multiple sclerosis traumatic brain injury (SMD −0.37; 95%CI −0.59, −0.15; GRADE quality of evidence moderate).
Discussion
In this systematic review, we aimed to determine the effect of education programs for fatigue in people with neurological conditions. Overall, we found low certainty evidence of a small benefit for education programs in reducing fatigue for people living with a neurological condition. Education delivered one-to-one showed moderate certainty of a small effect on fatigue, which was greater than the negligible effect of education delivered in group settings. The benefit of education for fatigue was similar between programs delivered in person and those delivered via telehealth.
The method of education delivery is important to people with neurological conditions who report preferences for education delivered via multiple formats.44,45 From a health service perspective, education delivery varies depending on service needs and demands, and these factors may influence the effect of the education. A key finding of our review was that education programs delivered one-to-one appeared to be more effective for reducing fatigue than programs delivered in a group setting. Education delivered one-to-one may provide greater opportunity for tailoring to individual needs. A one-to-one format may also allow for the development of stronger therapeutic relationships, which is important to people with complex health conditions. 46 On the other hand, a group format for education, while efficient, poses greater challenges for personalization and could create a cognitively overstimulating environment that may exacerbate fatigue. However, it is important to note that group-based education may be preferred, 44 and peer support may be beneficial for some people. 20
Interestingly, we found similar benefits for education programs when comparing those delivered via telehealth versus in-person delivery. With advances in technology and growing healthcare demands, telehealth is a useful tool for delivery of health services for people with neurological conditions. 47 For people living with fatigue, the benefits of reducing travel time for appointments and other burdens of in-person attendance may contribute to better outcomes. However, limitations of telehealth such as technical reliability and user confidence for people with neurological conditions need to be considered.
We found that for people living with multiple sclerosis, education was moderately beneficial for their fatigue, whereas for people with stroke more negligible benefits were observed. There are several reasons that this may be. Firstly, most trials included in this review recruited people living with multiple sclerosis. Fatigue education for people with multiple sclerosis (systematic review, n = 10 trials) has shown moderate benefits for fatigue, particularly when delivered one-to-one and for interventions containing psychoeducational components. 21 Our review (n = 14 trials, multiple sclerosis) extends these findings. Research in fatigue with multiple sclerosis is significantly more advanced than for other neurological conditions. The greater number of trials, and the refinement of education interventions over time may explain the differences in outcomes observed. Other reasons could explain the differences observed by condition. Firstly, multiple sclerosis is a degenerative condition whereas stroke is a single event that is thereafter stable. Secondly, there may be differences in the underlying biological mechanisms of fatigue between conditions that remain poorly understood.8,48 People living with neurological conditions experience a diverse array of sequelae including communication, cognitive and sensory processing impairments. These sequelae can all impact on the effectiveness of fatigue education and should be considered in clinical practice.
Our review has strengths and limitations. The strengths of our review included the rigorous systematic review methodology, use of the GRADE criteria to describe the certainty of evidence and the exclusive inclusion of RCTs with a primary focus of education for fatigue management. The quality assessment of the 19 trials included in this review resulted in low certainty of the overall small effect of education for fatigue across neurological conditions. A major source of bias in the included trials was lack of, or unclear blinding of outcome assessors. The certainty of evidence was also downgraded due to heterogeneity across trial results for the main results, and most subgroup analyses. On the other hand, the balance in published trials reporting both positive and equivocal benefits means that publication bias is unlikely, however, we did not formally assess publication bias using a funnel plot or Egger's test. Due to a lack of details reported, we were not able to explore the relative effectiveness of different educational, self-management and/or behaviour change approaches. Future trials should clearly report the components of their interventions using the Template for Intervention Description and Replication. Reporting of long-term follow-up varied across trials and we did not analyse the effect of education on fatigue beyond the immediate post-intervention timepoint. Consequently, the sustained benefits of fatigue education programs remain unclear.
In conclusion, neurological fatigue is complex and an individual experience, therefore a one size fits all approach to management and to education content and delivery is not likely to be effective. However, our findings support the use of education of fatigue management strategies in clinical practice. Fatigue education could be integrated into existing rehabilitation services or built into existing fatigue management clinics, delivered by allied health or by nursing health professionals. One-to-one delivery of education may be most effective, regardless of whether it is provided in person or via telehealth. Further work is needed to understand the core essential components of effective fatigue education programs, particularly for people living with stroke, traumatic brain injury, Parkinson's disease and other neurological conditions.
Clinical messages
Education interventions may be effective in improving neurological fatigue in people with multiple sclerosis however further research is needed in other neurological conditions.
Fatigue education intervention may be more effective when delivered one-to-one rather than in a group setting.
The mode of education delivery (telehealth versus in-person) does not seem to influence effectiveness.
Supplemental Material
sj-docx-1-cre-10.1177_02692155251351510 - Supplemental material for What is the effect of education on fatigue in adults with neurological conditions? A systematic review and meta-analysis
Supplemental material, sj-docx-1-cre-10.1177_02692155251351510 for What is the effect of education on fatigue in adults with neurological conditions? A systematic review and meta-analysis by Alex Delbridge, Owen Howlett, Coralie English and Dawn B Simpson in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors would like to acknowledge Bendigo Health (Victoria, Australia) Stepping into Research Program 2023 and facilitators.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data is available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.