
Abstract
Objective
To examine the experiences of individuals with acquired brain injury and their partners regarding the effects of social cognition problems on their relationships.
Design
Qualitative interview study.
Setting
Interviews were conducted 1 to 5 years post-injury, either in the participants’ home or at a care facility in the Netherlands.
Participants
Nine couples consisting of an individual with acquired brain injury and a partner without acquired brain injury. Scores on neuropsychological tests indicated social cognition difficulties in individuals with acquired brain injury.
Methods
Individual semi-structured interviews were conducted, audio recorded, and transcribed verbatim. Two independent analysts analyzed the data using thematic analysis aimed at finding common themes across the data set. Data analysis was carried out recursively and parallel to data collection to help determine when saturation was reached.
Results
Six themes were generated from the interview data: (1) partners feeling disappointed, lonely, and despondent, (2) individuals with acquired brain injury feeling insecure and ashamed of falling short, (3) relationship roles changing, (4) the aggravating role of fatigue and sensory hypersensitivity, (5) the importance of professional help, and (6) silver linings: increased awareness creating closeness.
Conclusion
Social cognition problems have the potential to strongly affect relationships between those with acquired brain injury and their partners in many ways. Addressing social cognition problems is recommended as it is greatly appreciated by individuals with acquired brain injury and their partners and holds promise for improving their relationship.
Keywords
Introduction
It is well documented that partner relationships are frequently strained after acquired brain injury. Studies report that, following acquired brain injury, relationship satisfaction diminishes1–3 and relationship continuity may be disturbed, 4 in which case the relationship is perceived as essentially altered rather than a continuation of the pre-morbid relationship. Feelings of anxiety and depression are common in both individuals with acquired brain injury and their partners5,6 and there is research indicating increased separation rates. 7
Given the importance of social skills in partner relationships, 8 it is likely that social cognition problems underlie some of the problems couples face after acquired brain injury. Social cognition problems, which occur frequently after brain injury,9,10 refer to the difficulties individuals with a brain injury may experience in understanding the mental states of others and using this information to guide their own social behavior.11,12 Commonly discerned aspects of social cognition are emotion recognition, theory of mind, and empathy. 12
Despite their likely relevance, research on the effects of social cognition problems on partner relationships following acquired brain injury is scarce. The results of two recent literature reviews,13,14 revealing a multitude of factors found to affect partner relationships after ABI, show that social cognition problems have received surprisingly little attention in this regard. The reviews do, however, identify two small-scale quantitative studies investigating the effects of social cognition problems on partner relationships.1,15 Results of these studies suggest that problems regarding empathy 1 and emotion recognition 15 negatively affect relationship quality. In addition, the influence of social cognition problems has briefly been touched upon in qualitative work in which partners of those with acquired brain injury indicated that social cognition difficulties negatively influenced their relationship by making them feel like their significant other was indifferent and unresponsive to their feelings, creating a sense of disconnection.4,16,17 To the best of our knowledge, however, no qualitative studies have specifically investigated the effects of social cognition problems on partner relationships after acquired brain injury.
More insight in the role social cognition problems play in partner relationships following acquired brain injury could help clinicians to optimally support couples following the injury. Such support is crucial as a satisfactory relationship strongly benefits both individuals with a brain injury as well as their partners.18–20 The current study therefore explores the role social cognition problems play in partner relationships following acquired brain injury. Specifically, we aim to examine the experiences of individuals with a brain injury and their partners regarding the effects of social cognition problems on their relationships. We do so using a qualitative approach, which has been deemed ideal for exploring experiences in general and family dynamics and relationships in particular.21,22
Methods
The current study was conducted in an interpretivism paradigm, 23 focusing on the subjective experiences of individuals with a brain injury and their partners. Given the limited existing research on how social cognition problems impact partner relationships after acquired brain injury, the approach to data collection and analysis was inductive.
Participants
The Medical Research Ethics Committee of the Maastricht University Medical Centre and Maastricht University confirmed that the Medical Research Involving Human Subjects Act does not apply in the current study. Additionally, ethical approval was given by the institutional review board of GGZ Oost Brabant.
Following approval, we recruited Dutch cohabiting couples consisting of an individual with acquired brain injury and a partner without acquired brain injury. They were recruited regardless of marital status. Participants were recruited in the period between August 2023 and January 2024 from a pool of couples that had previously participated in a cross-sectional study on the consequences of acquired brain injury for partner relationships, for which recruitment occurred through treatment facilities in the Netherlands and via an online recruitment campaign. The inclusion criteria for the cross-sectional study were also applicable to the current study: A couple's relationship had to precede the injury by at least a year, the brain injury had to be confirmed by a physician and had to be sustained between 1 and 5 years ago. Moreover, it was required that the individual with acquired brain injury had undergone or was presently undergoing treatment for the consequences of their brain injury in a rehabilitation center or mental health facility. One additional inclusion criterion was added for participation in the current study: scores on neuropsychological tests needed to indicate the existence of social cognition problems for the individual with acquired brain injury. Individuals lacking the language skills needed to take part in an interview were not eligible for participation.
To assess the presence of social cognition problems, two neuropsychological tests were used: the Emotion Recognition Test 24 and the Faux Pas test. 25 Both were administered by researchers in the previously mentioned cross-sectional study. The Emotion Recognition Test is a computerized test for emotion recognition in which participants are tasked to label the emotions (anger, disgust, fear, happiness, sadness, or surprise) of morphed video clips of facial emotional expressions. The test has been found to differentiate between individuals with acquired brain injury and matched controls 26 and Dutch normative data are available (n = 255), 27 allowing for the calculation of sociodemographic-corrected standardized and percentile scores. The Faux Pas test was used to measure theory of mind and empathy. A short version of this task was used in which participants are presented with 10 short stories and are tasked to detect which stories contain someone making a social blunder (i.e. a faux pas, occurring in half of the stories), thereby measuring theory of mind. The test subsequently investigates whether participants can accurately describe how the faux pas victims would feel in the described situations, thereby measuring empathic ability. Consequently, faux pas detection scores for theory of mind range from 0 to 10 and empathy scores range from 0 to 5. The Faux Pas test has been found to differentiate between individuals with acquired brain injury and matched controls. 28 Provisional Dutch normative data are available (n = 373) 29 suggesting a cut-off score (M-1.5×SD) of 7 for theory of mind scores and 1 for empathy scores. Individuals had to score on or below one of the Faux Pas cut-off scores and/or score very low (percentile ≤ 2) or low (percentile 3–16) on the Emotion Recognition Test in order to be eligible for participation.
Emotion Recognition Test and Faux Pas test scores, as well as injury and relationship characteristics, were collected in the previously mentioned cross-sectional study. This facilitated the identification of eligible couples for inclusion in the current study. Data collection of the current study was carried out concurrently with data collection for the cross-sectional study. Couples who completed the cross-sectional study and were eligible to take part were informed via email or phone about the current study by the researchers and invited to participate. Sample size determination was informed by Braun and Clarke's 30 guidelines and was complemented by simultaneous analysis during data collection to determine when data saturation was achieved. A total of nine couples ultimately participated, for which 13 were invited, as four couples chose not to take part.
Procedure
Interviews were set up with the participating couples. Both the individuals with acquired brain injury and their partners were interviewed. Prior to the interviews, participants provided written informed consent. All participants were interviewed individually to allow them to speak openly about sensitive issues in their relationship that they may not have felt comfortable discussing in joint interviews or focus groups.3,31 Preferably, both members of each couple were interviewed simultaneously by two different interviewers or in close succession to avoid inadvertent influence between the interviews. Most of the interviews took place simultaneously, though three couples were interviewed consecutively by the same interviewer. In these cases, to avoid potential influence and maintain confidentiality, the interviewer did not disclose information from the first interview in the second one. 32 Interviews were conducted face to face either in the participants’ home or at a care facility and were semi-structured, based on an interview guide developed for this study (see Table 1 for an English translation). Interviews were audio recorded and lasted between 28 and 86 minutes (mean duration: 56 minutes).
Interview guide (English translation from Dutch).
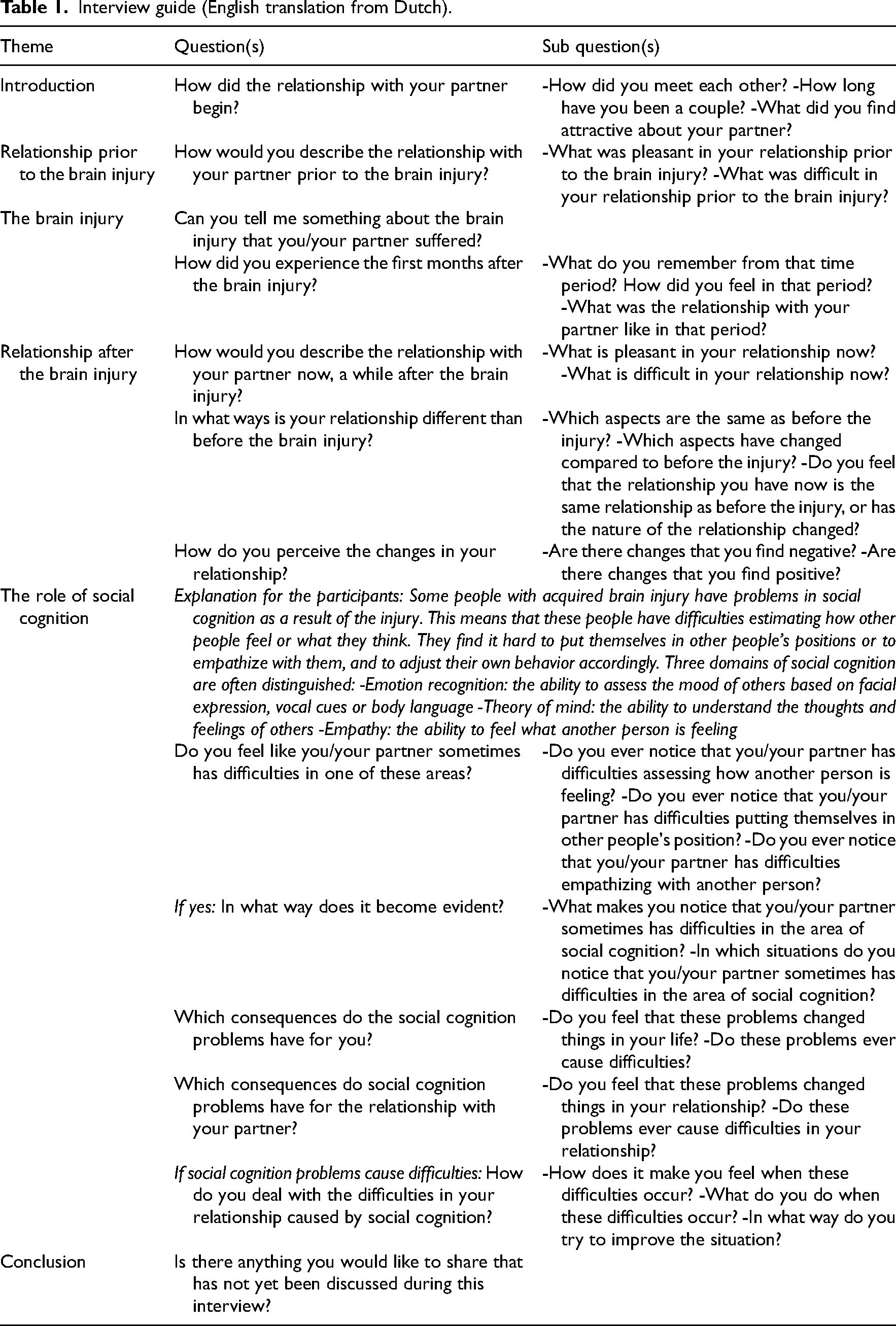
The interviews were conducted by two researchers (BvdB and JM). One of the interviewers (BvdB) was a researcher who had seen participants once before for about 30 minutes to an hour in the context of data collection for the previously mentioned cross-sectional study. The other interviewer (JM) was a psychiatry resident who had not met the participants prior to the interview. In accordance with the interview guide, the interviewers commenced by posing general questions about participants’ relationships (e.g. “How did you meet each other?” and “How long have you been a couple?”). This approach aimed to help participants become adjusted to the interview setting before delving into potentially more sensitive inquiries concerning the impact of the injury and social cognition problems on their relationship.
Analysis
The data were analyzed using thematic analysis, 33 aimed at finding common themes across the data set. The audio recorded interviews were transcribed verbatim. Then, two analysts (BvdB and JM), who had conducted the interviews themselves, familiarized themselves further with the data by repeated close reading of the transcripts and selected interview sections that were related to social cognition problems and their impact on participants’ relationships. Next, initial codes were generated by the two analysts jointly using a data-driven approach. In the subsequent phase, the two analysts jointly sorted the generated codes into potential themes. This phase was followed by reviewing the generated themes; the analysts assessed whether themes were coherent and meaningful and whether there were clear distinctions between different themes. Additionally, the analysts re-read the dataset to check if the themes worked in relation to the data and to code additional data within themes that had been missed in earlier stages. Where necessary, codes and themes were refined. Data analysis was carried out recursively and parallel to data collection to help the researchers determine when saturation—the point in data collection when no additional issues or insights are identified and data begin to repeat so that further data collection is redundant 34 —was reached. Once the analysts concluded that saturation had been reached, the previously described steps were carried out once more and themes were definitively determined and named. Following the definite determination of the themes, one additional couple was interviewed. The analysts concurred on the alignment of the data from this interview with the predefined themes, obtaining further verification that data saturation was achieved. The final themes, along with supporting quotes, were also reviewed by the other three authors.
Results
A total of nine couples participated in our study, their characteristics are provided in Table 2.
Characteristics of participating couples.
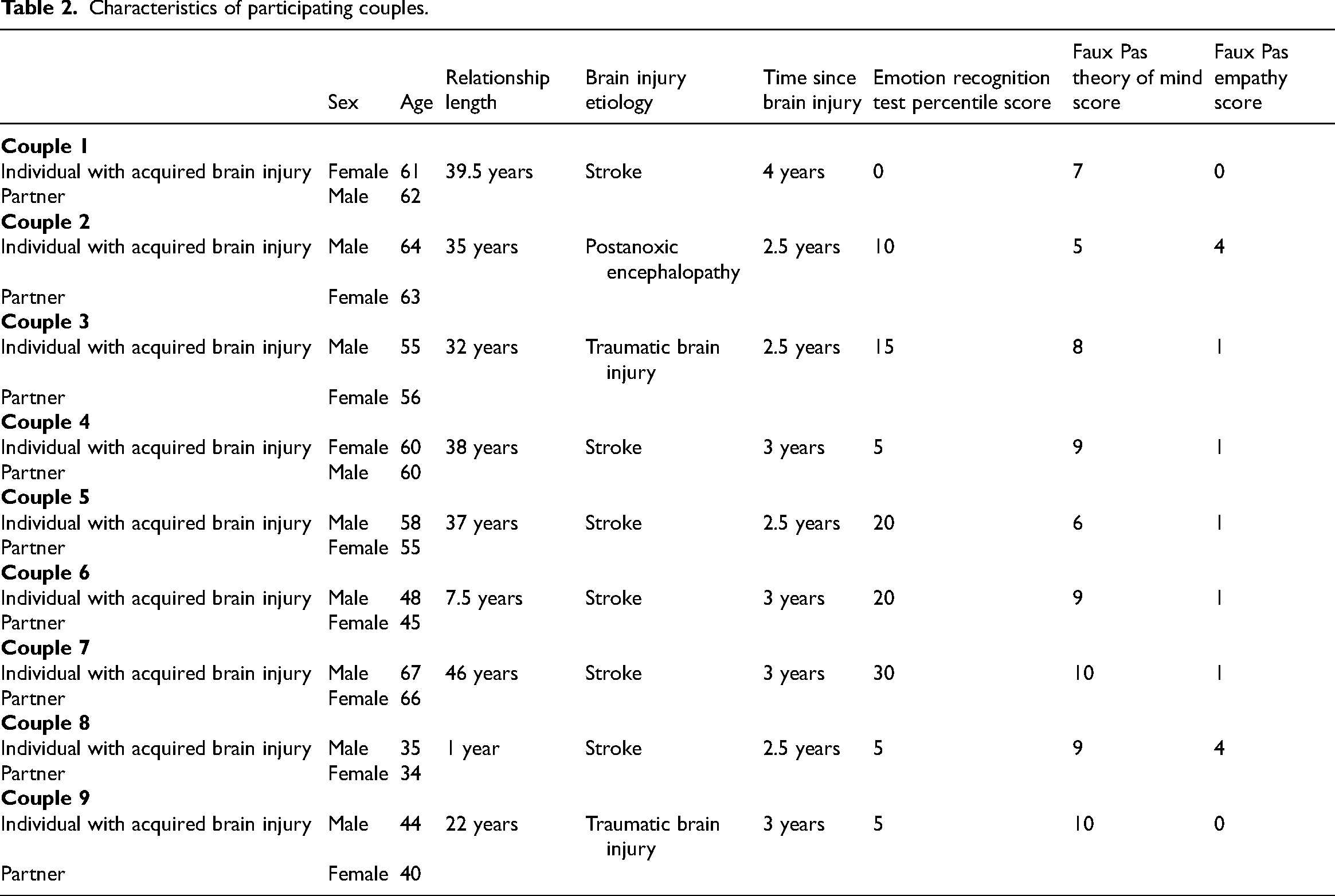
The sample of nine couples follows Braun and Clarke's 30 recommendation of conducting 6 to 10 interviews when employing thematic analysis. Most couples clearly recognized the presence of social cognition difficulties. Couples 1 and 4, however, expressed experiencing minimal difficulties in social cognition. The individual with acquired brain injury in Couple 1 did not recognize any social cognition problems while her partner did recognize them to some extent. In Couple 4, the person with acquired brain injury described experiencing minor issues with social cognition, which her partner did not observe. As such, the perspectives of these couples are not as prominently featured in the themes and the supporting quotations.
Six interrelated themes were generated from the interview data: (1) partners feeling disappointed, lonely, and despondent, (2) individuals with acquired brain injury feeling insecure and ashamed of falling short, (3) relationship roles changing, (4) the aggravating role of fatigue and sensory hypersensitivity, (5) the importance of professional help, and (6) silver linings: increased awareness creating closeness. Figure 1 provides an overview of the themes and their coherence.
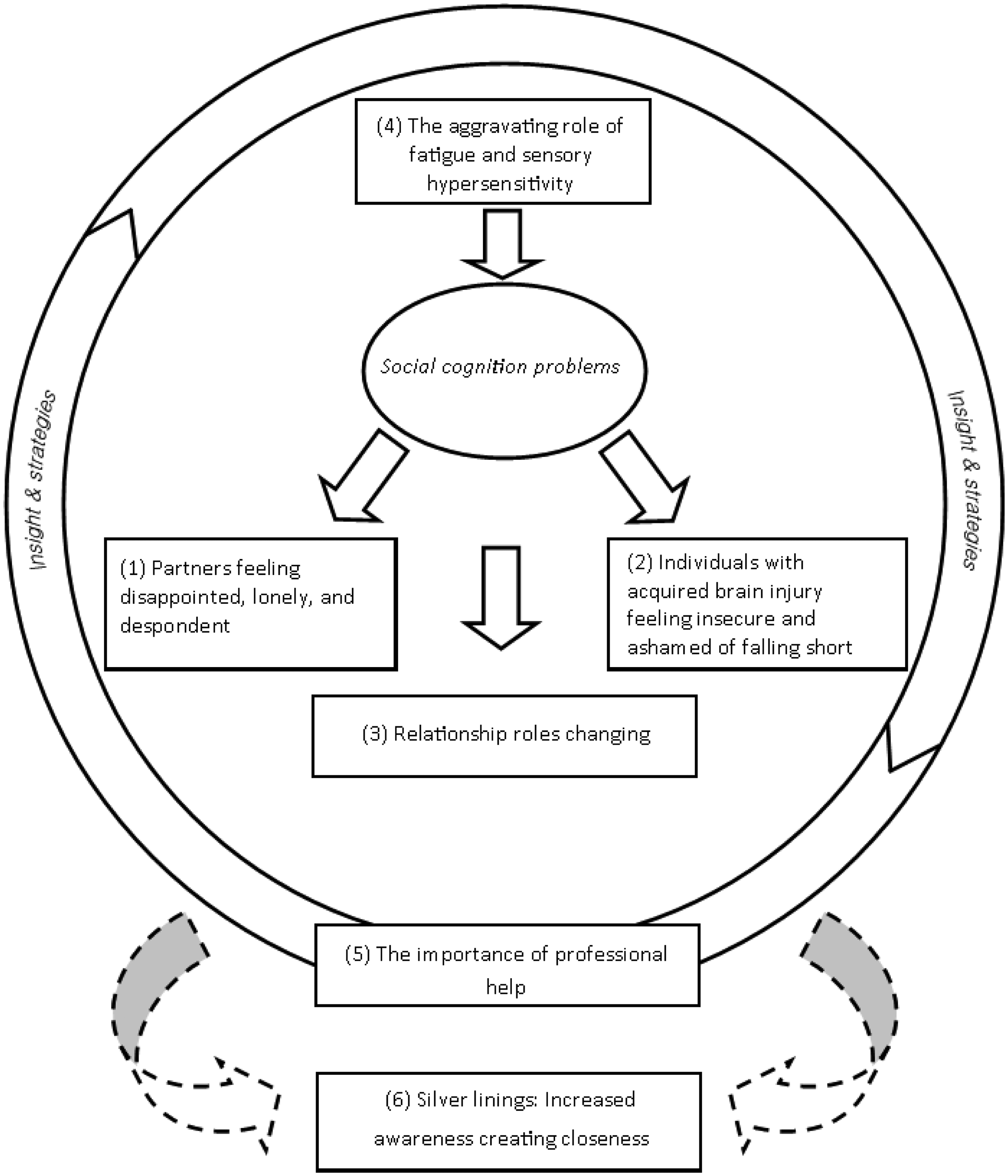
Identified themes and their coherence.
Theme 1: Partners feeling disappointed, lonely, and despondent
The majority of the interviewed partners reported that the social cognition problems of their significant others negatively affect them. They expressed feelings of disappointment stemming from situations in which their significant other is unable to understand their needs or to respond to their feelings, causing them to miss “affection and attention for each other” (Partner 3). —I was telling a story but I got no reaction: no question, no… nothing. And I am quite chatty but at a certain point […] you think: never mind. […] It made me feel disappointed that he did not react in a nice, sociable way. […] I was just really disappointed.—Partner 8 —I did want to talk about things, but it wouldn’t get through. (..) As a result, you sometimes have the tendency not to share things, (…) you think to yourself: well, never mind, because it won't get through anyway. (…) In those moments you’d feel a bit lonely.—Partner 8 —In the end I’ll let it go. Ultimately it's like, well, you know, if you don’t want to understand it, then just don't understand it. Never mind. Then I become a bit dispirited.—Partner 5 —We have never considered leaving each other before, but in the past few years I have questioned whether this is what I want.—Partner 7
Theme 2: Individuals with acquired brain injury feeling insecure and ashamed of falling short
For most individuals with acquired brain injury, it had taken some time to become aware of their social cognition difficulties. They talked about how in the first phase after the injury, they did not always understand how their behavior had changed and how that could have affected their partners. —My behavior developed in such a way that I did respond differently. I was more flat, my wife found it quite difficult to point that out to me. […] And when she did say something […] I thought, well damn, what have I done wrong now? […] I did not understand it at the time.—Individual with acquired brain injury 7 —Sometimes, I am unable to absorb her words. […]. As much as you want to be attentive or hear the whole story. […]. I just think that's a shortcoming. […] You want to be the best version of yourself for the other person. I feel like I’m not always able to do that.—Individual with acquired brain injury 8 —I often think: shit, you’re right, […] I should have seen or done that. [Interviewer: And what emotions does that evoke?] Shame, I don’t know if that's an emotion but sort of: yes indeed, you’re right, I could have done better.—Individual with acquired brain injury 2 —I feel like I do now assess [other people's feelings] quite correctly, but I never dare to act on it. Well, if I didn’t assess it correctly, then it’d be quite unpleasant.—Individual with acquired brain injury 4
Theme 3: Relationship roles changing
Both individuals with acquired brain injury and their partners expressed shifts in relationship roles stemming from social cognition problems. They talked about how partners feel inclined to offer guidance or to correct the injured individuals regarding appropriate social behavior. —When we go somewhere I’ll tell him: it's good to ask someone else how they are doing as well.—Partner 6 —And regarding social cognition, I notice that [my partner] doesn’t always notice. So I had to teach him that. […] I find that difficult at times. It's like I’m telling him as a mother: “you're not allowed to do this.”—Partner 5 —Sometimes I feel like I’m being patronized, and I don’t like that at all. Even though I do rationally understand it.—Individual with acquired brain injury 7
Theme 4: The aggravating role of fatigue and sensory hypersensitivity
Many of the interviewed individuals with acquired brain injury as well as their partners described that fatigue and sensory hypersensitivity have an aggravating effect on social cognition difficulties and the adverse consequences for their relationship. When faced with fatigue and sensory overload, those with a brain injury reported to become more focused on themselves. This withdrawal was described to inhibit their ability to recognize emotions, read the mental states of others, and engage in social interactions. These effects were evident to partners as well. —If you’re really tired or you’re overstimulated, […] then it also becomes harder to empathize with someone else. Because you’re just fully occupied with yourself, so you have little space left to really empathize with someone else.—Individual with acquired brain injury 8 —I feel like he is less sensitive when he is busy. Because his head is full then and he can’t really process it.—Partner 9 —We now have a better understanding of how things develop and what the cause is and what the remedy is. Sometimes I’ll say: “It's better that I go upstairs and lay in bed for an hour”. Sometimes [my partner] will say: “It would be better if you went upstairs for a bit.”—Individual with acquired brain injury 2 —What I’ll often do is take away stimulants. So I’ll shut down the television and say: “hey listen to me for a bit”. […] That often works better. […] Because I also need my moments every now and then.—Partner 8
Theme 5: The importance of professional help
The professional help individuals with acquired brain injury received following their injury was reported to be invaluable and was greatly appreciated by the interviewed couples. It was described to provide them with crucial insights on the social cognition problems they faced, helping them “start to understand” (Partner 7) what was happening to them. In addition it provided them with useful strategies to “deal with it better” (Individual with acquired brain injury 7). These strategies include consciously pausing and reflecting on social situations before reacting to them, and managing fatigue and overstimulation to avoid their aggravating effects. —That's what I learned: Don’t react immediately, think calmly for a moment, think about what the other person means. [The rehabilitation clinic] provides guidance on how to deal with those kinds of things.—Individual with acquired brain injury 2 —You kind of write a manual for yourself. And I don’t do that alone, I do that at […], a program for people with acquired brain injury. […] You just learn to properly map out your own energy level throughout the days and week and then you ensure that you get back into balance.—Individual with acquired brain injury 8 —I’m also following a partner program […]. There you meet people who recognize it. We try to thoroughly discuss with each other: well, how do you deal with that? And how do you keep your relationship thriving?—Partner 5 —It would have been nice if a got a booklet when I ended up in this situation, […] what you can expect. […] There is an enormous amount of help for those who are going through it, but those next to them […] really just have to figure it out.—Partner 3 —I really should have had a bit more information on: okay this fits with this brain injury, right? Because they were acting like it was completely normal. But I really thought: what on earth is happening here?—Partner 9
Theme 6: Silver linings: increased awareness creating closeness
Besides the complications they faced, several couples also reported that grappling with social cognition problems ultimately fostered positive effects for their relationship. As those with acquired brain injury became aware of and received help for their social cognition difficulties, they started to consciously pay more attention to their own and their partner's thoughts and feelings. Furthermore, the treatment process frequently required the injured individuals to reflect on and talk about their emotions in ways they were unaccustomed to before the injury. This caused some of them to “talk more […] about feelings” (Individual with acquired brain injury 3) and be “more open than before the brain injury” (Individual with acquired brain injury 5). —He has become much more open, much softer […] just talking a lot more about feelings, expressing things, a lot earlier.—Partner 8
—We didn’t used to talk. I’m not that good at talking. I’ve improved a lot after the accident, you know, I’ve really turned a corner. […] I had a good reset with that one bang.—Individual with acquired brain injury 9
Discussion
This qualitative study explored the experiences of individuals with acquired brain injury and their partners regarding the effects of social cognition problems on their relationships. It is the first qualitative study explicitly examining this topic. Our findings confirm that social cognition problems have the potential to strongly affect relationships between those with acquired brain injury and their partners in many ways.
The findings show that difficulties in social cognition may contribute to several of the well-documented problems couples face following a brain injury. In previous work, partners reported decreased relationship satisfaction 2 as well as feelings of loneliness and isolation.4,17 Our study outcomes suggest that social cognition issues may be a contributing factor to such experiences. Similarly, results of the current study imply that social cognition problems may be one of the factors that cause the role changes 35 and disturbed continuity 4 couples experience in their relationship post acquired brain injury. Our results furthermore indicate that problems in social cognition may contribute to the increased separation rates 7 that have been reported, as partners in the current study described that the social cognition difficulties faced by their significant other prompted them to question the durability of their relationship.
The association between fatigue and social cognition reported by the participants in the current study contrasts the findings of a recent quantitative study that found no association between fatigue and social cognition scores in individuals with a stroke. 36 Associations between fatigue and impairments in other cognitive domains have, however, been found in those with acquired brain injury, 37 as well as an association between fatigue and social cognition in individuals suffering from multiple sclerosis. 38 This topic therefore warrants further investigation.
The results of the current study furthermore strongly support the recommendation for clinicians to address social cognition problems in their work with individuals with acquired brain injury and their partners. Firstly, couples emphasized the importance of psychoeducation to help them understand their situation. Partners in particular voiced a desire for greater and more timely information and guidance, feeling bewildered by the changes and unsure about how to navigate them. Additionally, the interviewed couples greatly appreciated efforts to teach individuals with acquired brain injury effective strategies to mitigate their social cognition difficulties. Some of the couples even reported increased openness and intimacy in their relationship as a result of the heightened awareness of and reflection on their social cognitive abilities. Prior research validates the importance of addressing social cognition problems after acquired brain injury, demonstrating its potential to improve relationship quality. 39
A notable strength of this study is the inclusion of both individuals with acquired brain injury as well as their partners, which is crucial to obtaining a complete understanding of the effects of acquired brain injury on partner relationships. 13 An additional strength is that participants were interviewed individually, enabling them to discuss sensitive issues in their relationships openly.3,31
There are, however, some limitations to consider when interpreting the results of our study. First, we did not interview couples who separated following acquired brain injury. Consequently, we did not gain insight into their experiences meaning that there may be a bias in our findings. Presumably though, separated couples may have experienced even greater problems in their relationships than those who remained together and took part in our study. However, we cannot ascertain whether that is the case or whether social cognition issues contributed to their separation. Second, our study sample is characterized by a relatively high degree of uniformity in certain characteristics such as age and sexual orientation. We cannot determine the extent to which the experiences of couples divergent from our study sample align with those documented in the current study. Furthermore, despite the requirement for neuropsychological tests to suggest social cognition difficulties in individuals with acquired brain injury for participation in this study, not all participants recognized these issues to the same extent. Most couples clearly recognized the presence of social cognition difficulties. Couples 1 and 4, however, experienced minimal problems in social cognition. Consequently, the interviews of these couples are less prominently represented in the identified themes and the supporting quotes and the perspectives of these couples were not fully explored. Additionally, while the interviewer made efforts to prevent influence between consecutive interviews with members of the same couple, we cannot entirely rule out the possibility of any influence between the first and second interviews in these three cases. Furthermore, incorporating additional steps, such as member checking, could have enhanced the credibility of our findings and further strengthened the study. Finally, the presented quotes were translated from Dutch. Despite careful consideration, there is a possibility that certain nuances may have been altered to some degree.
Notwithstanding the limitations, this study has shown that social cognition problems can profoundly influence relationships following acquired brain injury and that it is important for clinicians to address social cognition problems when working with individuals with acquired brain injury and their partners.
Social cognition problems can strongly affect relationships between individuals with acquired brain injury and their partners. Fatigue and overstimulation may have an aggravating effect on social cognition difficulties following acquired brain injury. Addressing social cognition problems with both individuals with acquired brain injury and their partners is recommended as it is greatly appreciated by couples and holds promise for improving their relationship.Clinical messages
Footnotes
Author contributions
BvdB, CvH, BB, and SR devised the project and were involved in developing the protocol and gaining ethical approval. Recruitment, data collection, and data analysis were carried out by BvdB and JM. BvdB took the lead in writing the manuscript. All authors reviewed and edited the manuscript and approved its final version.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Medical Research Ethics Committee of the Maastricht University Medical Centre and Maastricht University confirmed that the Medical Research Involving Human Subjects Act (WMO) does not apply in the current study. Additionally, ethical approval was given by the institutional review board of GGZ Oost Brabant.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All participants provided written informed consent.