
Abstract
Objectives:
To examine the economic evidence for interventions aimed at family carers of stroke patients.
Data sources:
Searches (limited to those published in English since 1990) were performed in key databases along with hand searches of relevant papers.
Review methods:
Papers were restricted to studies including any economic data (broadly defined) for any intervention targeting carers explicitly or explicitly referring to a carer element, beyond involving carers in the care or intervention for patients (i.e. more than just carers being invited to observe an intervention targeted at the patient). Two reviewers independently screened full papers and extracted data using guidance from the National Institute for Health and Care Excellence, and quality assessment using the Newcastle-Ottawa Quality Assessment Scale (cohort studies), the Delphi list (randomised controlled trials) and guidelines on economic quality from the British Medical Journal. Data were reviewed descriptively as meta analyses were inappropriate due to non-comparability of studies.
Results:
Ten papers were included in the review. These were heterogeneous in their design, intervention and economic analyses making comparison difficult. Only three of the ten papers included economic evaluations. All three reported that the intervention was less costly and had better or equivalent outcomes than the control comparator although two of these were based on the same intervention using the same dataset.
Conclusion:
There is some limited evidence that interventions for family carers of stroke patients are effective and cost effective. However, due to variation in the types of interventions examined, little can be concluded regarding implications for clinical practice.
Keywords
Introduction
Following a stroke, many patients receive vital support from informal carers (also known as family carers), 1 who may be clients themselves 2 with their own clinical and economic consequences arising from their role e.g. depression, inability to cope, forgone opportunities to work. Supporting informal carers may benefit patients as well as carers. Various interventions have been developed and evaluated with the intention of supporting informal carers. Reviews of the effectiveness of such interventions have reported conflicting findings for different interventions and even those concluding positive outcomes report only modest effects.3–8 Only one review has examined the cost-effectiveness of such interventions (within randomised controlled trials; Smith et al. 7 ), finding just one economic study, Kalra et al. 9
To increase understanding of current evidence on cost-effectiveness, this systematic review aimed to examine all economic evidence (not just from randomised controlled trials) for any interventions for informal carers of stroke patients (in terms of patient and carer outcomes), and to explore the case for directing scarce health care resources towards activities of this type.
Methods
This review included studies of any design which incorporated any economic data (described below) for any intervention, providing that intervention included a component which involved informal carers of stroke patients. The intervention had to include an informal carer component but the studies could have reported either carer or patient outcomes, or both.
The inclusion criteria for this review were:
Studies of any design in which the condition of interest included stroke.
Study participants included informal carers (broadly defined as the main person, other than health, social or voluntary care provider, who gives support) for people with a diagnosis of any type of stroke.
Study examined interventions which either targeted carers explicitly or explicitly refer to a carer element, over and above involving carers in the care of patients.
Study explicitly referred to informal carers in the participant selection.
Study included some form of economic analysis, broadly defined as economic evaluations, analysis of costs, resource use, employment impacts, lost productivity, quality-adjusted life years (QALYs) or disability-adjusted life years (DALYs).
Papers with patient groups of mixed diagnosis (e.g., stroke and dementia patients) and papers in a non-English language were excluded.
Only studies published from 1990 onwards were included because formal economic evaluation was rarely conducted prior to this date and the most relevant policy documents focussing on carers were published after this.
Ovid EMBASE Classic and EMBASE (1990 to 2013 June 03), OVID Medline (1990 to May Week 4 2013), Cochrane Library NHS Economic Evaluation Database (1990 to Issue 2 of 4, Apr 2013) and Cochrane Library CRD Health Technology Assessment database (1990 to Issue 2 of 4, April 2013) were searched. Each database was searched using terms related to: ‘carer’; ‘intervention’; ‘rehabilitation’; ‘stroke’; and ‘economic’ (see online appendices 1 and 2 for search terms). Reference lists of relevant papers and existing reviews were also searched for relevant papers. Items which were abstracts only without data were excluded, but for completeness we attempted to contact the lead author to request any related published data.
The search strategy was checked and conducted by an information specialist. Duplicates were removed and one reviewer screened titles and abstracts for relevance. A second reviewer checked a random 10% of exclusions using a random number generator written in Excel. Full texts of all potentially relevant articles were retrieved and examined for consistency with the study criteria by both reviewers. Multiple reports of the same study were linked.
Two authors (AP, MH) examined papers and independently extracted data from included studies using a modified version of the data extraction form for economic studies used by the National Institute for Health and Care Excellence. 10 Modifications were additions to the form rather than edits or omissions of existing items. Depending on the study design, either the Newcastle-Ottawa Quality Assessment Scale 11 for assessing cohort and case-control studies or the Delphi list 12 for assessing randomised controlled trials was used to assess the quality of the overall study. We used the well established guidelines for authors and peer reviewers of economic submissions to the British Medical Journal 13 (where applicable) to assess the quality of the economic evidence.
Within this review, intention to treat analysis was defined as all data from all participants who were randomised being included in the analyses, even if the participant dropped out of the trial or were non-compliant with their initial group allocation. 14 Lack of intention to treat analyses could bias findings if characteristics of non-responders differ from those of responders. 15 Intention to treat was considered applicable to all randomised and non-randomised trials. Any disagreements in the screening and data extraction processes were resolved through consensus.
As studies varied widely in terms of methodology (study design, follow-up length, type of economic data/evaluation, economic perspective) and intervention being investigated, meta-analyses were not appropriate and therefore, a descriptive synthesis of the data was undertaken. Any conversion of costs was conducted using the CCEMG - EPPI-Centre Cost Converter 16 using the International Monetary Fund purchasing power parity conversion rates and converting all costs into pounds sterling at 2013 prices.
Results
The searches yielded 2,509 records (Figure 1) (Embase 1,686 records, Medline 806 records, NHS Economic Evaluation Database 17 records and Cochrane Health Technology Assessment 0 records). Adding potentially relevant papers (based on title alone) identified from review papers and reference lists increased total records to 2,539. A total of 1,857 records remained after removing duplicates. 1,640 records were considered not relevant following a title and abstract screening, leaving 217 full texts to assess. Of these, 207 were excluded (see supplementary material Table 1 for reasons) leaving a total of 10 relevant papers to review (only one of which was identified from a reference list rather than the systematic searches).
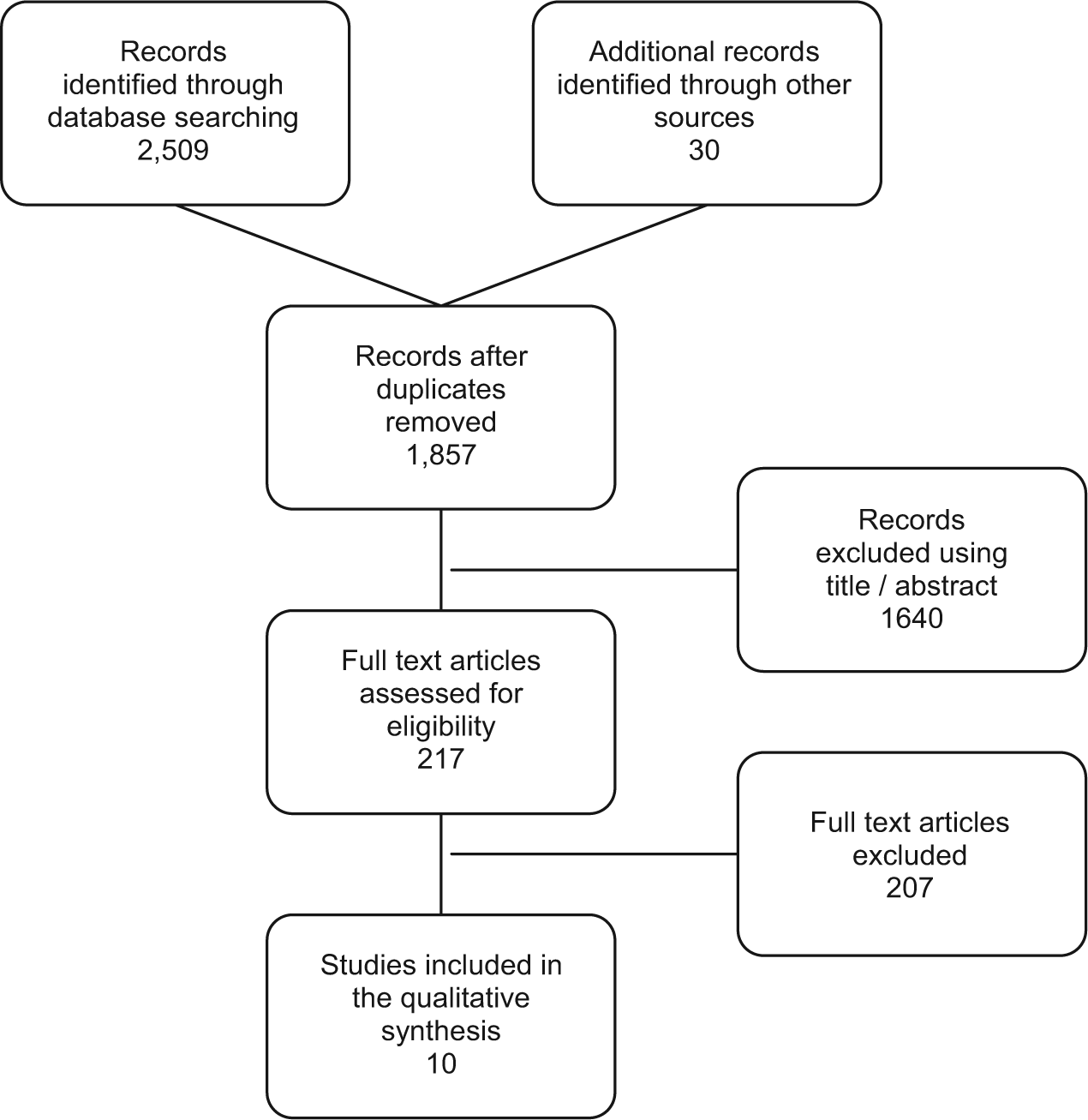
Flow diagram of included studies.
Table 1 details studies included in the review and their findings. A variety of interventions were reported ranging from basic information-giving to structured assessment to active interventions. The nature of economic data ranged from resource use information related to just the intervention, through to cost-effectiveness analysis with more comprehensive assessments of costs and outcomes. Most papers (8 out of 10) were based on randomised controlled trials (RCTs) and all reported individual-level data. Only one study combined costs and outcomes into a full economic evaluation. Follow-up durations ranged from 3 months to 31 months.
Details of papers included in the review.

RCT: randomised controlled trial, QALYs: quality adjusted life years, CBT: cognitive behavioural therapy.
Interventions were targeted at either carers, or both carers and patients. Six papers evaluated an intervention that targeted carers either exclusively or predominantly9,17-21 (Table 1). Grasel et al.’s 17 comparison of an intensified transition programme with standard transition procedure (Table 1) limited economic outcomes to specific resource use only, collected from patient interviews (perspective not stated). Significantly more patients in the intervention group were living at home and fewer patients were institutionalized or deceased, but there was no difference in carer or patient outcomes. The authors did not attach unit costs to the resources used and performed no formal economic evaluation. However, as institutionalisation is a high cost service, it could be postulated that reduction in use of such services would be associated with cost savings. Nevertheless, this would not necessarily influence overall costs or cost effectiveness if there were impacts on use of other services. The methodological limitations of this and other reviewed studies are highlighted in supplementary material Table 2.
Bakas et al. 18 found some clinical improvements for carers from a Telephone Assessment and Skill-building Kit (TASK) intervention compared to a control attention control group (unclear whether this was ‘treatment as usual’; Table 1). Bakas et al. 18 estimated the costs of running this program (collected from trial implementation staff) and included the following resources in their calculation: staff time; training the staff; staff supervision; carer time; and materials. The authors state that a societal perspective is desirable in most cases but they did not explicitly state that this was used. The mean cost per carer was US$421 (2010 prices; £300 in 2013 prices) for the intervention group and US$286 for the control group (2010 prices; £204 in 2013 prices) largely due to extended training time and longer duration of calls in the intervention group, but there was no statistical comparison of costs.
Pierce et al.19,20 conducted two separate evaluations of an internet based education and support program for rural carers, Caring-Web (Table 1). The first 19 was a cohort pilot study that reported that carers were satisfied with Caring-Web and a cost per participant of US$50 (pricing year not stated) but it is unclear exactly what was included in these costs. No formal economic evaluation linking costs and outcomes was conducted. The small sample size of nine participants is to be expected for a pilot study. The second 20 was an effectiveness study and cost analysis from a health care perspective (although the perspective is not explicitly stated by the authors) of Caring-Web compared to an unspecified control group. The cost analysis reported intervention patients had 33% fewer visits to the emergency department and 66% fewer hospital admissions compared to controls (collected via participant interviews). This resulted in health care cost savings of US$8,684 (£6,461 in 2013 prices) and US$609,000 (£453,097 in 2013 prices) respectively. There were no differences in carer outcomes.
Kalra et al. 9 and Patel et al. 21 both reported on an RCT of a carer training intervention compared with conventional care on a stroke unit (‘treatment as usual’; Table 1). Economic outcome data were collected by participant self-report. Costs were from a societal perspective and included secondary care services (inpatient, outpatients, A&E, day hospital), social services, community based services and informal care. Kalra et al. 9 reported carer training was associated with significant cost reductions over one year (£10,133 v £13,794, 2001-2 prices; £13,591 v £18,501 in 2013 prices) mainly due to lower hospital costs. There were also positive outcomes for carers and stroke patients in a number of domains. Patel et al. 21 supplemented these results with a cost effectiveness analysis linking costs with quality adjusted life years (QALYs) based on utility weights from the EuroQol five-dimensional questionnaire (EQ-5D). Total health and social care costs over one year for patients whose carer received the intervention were significantly lower (mean difference of £4,043, 2001-2 prices; £5,423 in 2013 prices) but there were no significant differences in QALYs between the groups. An incremental cost effective ratio (ICER) was not necessary as the carer training was clearly the more desirable option, with both lower costs and better outcomes.
Generalizability of the studies in this section needs consideration. Bakas et al. 18 describes recruiting from local rehabilitation and acute care hospitals, while Kalra et al. 9 and Patel et al. 21 describe recruiting from stroke rehabilitation units. However, neither study describes the location of their recruitment sites. Grasel et al. 17 recruited in Nuremberg, Fuerth and Erlangen in Germany. Pierce et al.19,20 recruited in Northern Ohio and Southern Michigan and Pierce et al. 19 was targeted at rural carers. Only three of the studies mention ethnicity of their sample,18-20 indicating predominantly white participants, which limits generalisability to other ethnic groups. There was also a predominance of female carers (reported in 5 out of 6 studies), reflecting the dominance of female carers in general. 22
In summary, of studies with an intervention aimed predominately at carers, Pierce et al. 19 reported the cost of implementing an internet based education and support program for rural carers. This study is unable to provide an answer to the salient economic question of how scare healthcare resources can best be used to maximise health gain obtained from them, 23 as it does not report on outcomes or health gains. The other five studies indicate a trend for carer targeted interventions having some value but further research is needed to confirm this, and the generalisability of these studies is limited.
Four studies evaluated interventions that were not clearly targeted to either carer or patient but involved both.24-27 Mant et al. 24 examined the impact of Stroke Association family support compared with a normal care group (not described). Patients’ use of outpatient services and community care (collected by interview with patients and carers) showed only less physiotherapy used in the intervention group. The authors also highlighted that intervention patients used the Stroke Association stroke clubs more and speech and language therapy less but these differences were not significant. 24 There were better outcomes for intervention carers but not for patients.
Glass et al. 25 compared a psychosocial intervention to standard educational material on stroke recovery (usual care) in the United States. The data collection methods for this study were unclear and the authors did not specify the perspective of the economic analysis (resource use) but it appeared to be a limited healthcare perspective. Hospitalisations and nursing home admissions were similar in both groups. Antidepressant use increased slightly over the course of the study in both groups but the statistical significance of this and of the difference between the groups was not reported. No carer outcomes were assessed and there were no differences in patient outcomes.
Forster et al. 26 investigated the effect of reassessing stroke patients using a patient and carer structured assessment system compared to standard care plus a service information pack. Economic evidence (from a health and social care perspective) consisted of an assessment of the cost of resource use (inpatient care, outpatient and community healthcare, day centre use, care home, and aids and adaptations) collected via patient interview plus the cost of the intervention. Intervention arm patients used a median 301 fewer hospital bed days and a median 1,631 fewer care home bed days (26) over 12 months. The total mean cost of the intervention was £219 (2005/6 prices). The authors did not describe the constituent costs of the intervention, only the mean total cost including the intervention costs, which was £2,963 (2005/6 prices) for the intervention group and £3,159 for the control group. The authors report the costs as ‘similar’ but without any statistical significance testing or exploration of uncertainty around this point estimate of difference. There were no clinical benefits to patients or carers. A breakdown of resource use and cost components for each group were reported but there was no indication of statistical significance. 26
Parker et al. 27 compared a home based intervention (Table 1) to an information control group (unclear whether this was ‘treatment as usual’). The paper reported on the resources used, and costs associated with the intervention from a societal perspective. The authors report the hours of resources allocated to staff training per carer, travelling, performing the intervention, meetings as well as the hours of participant recruitment and carer’s time engaged with intervention staff. When these resources were translated into costs, the incremental cost of the intervention was US$2,500 (2009 prices; £1,804 in 2013 prices) per carer. A sensitivity analysis surrounding the cost estimate found a potential cost range of between US$1,700 (£1,227 in 2013 prices) and US$3,500 (£2,526 in 2013 prices). There were no patient or carer outcomes reported and there was no combination of costs and outcomes data into a full economic evaluation. The data in this paper come from an RCT which has some notable limitations. However, as the data are used in a cohort fashion (only the intervention group is reported on), the limitations are not relevant here.
Mant et al. 24 recruited from hospitals in Oxford, while Parker et al. 27 recruited from hospitals in Houston, Texas, Glass et al. 25 recruited from acute care and rehabilitation hospitals in Boston, Massachusetts and Forster et al. 26 recruited from stroke units in the United Kingdom. Again, studies which reported demographics reported a predominance of women24,26,27 and a predominance of white participants.25,27 Therefore, generalisability to other demographic groups is unclear.
As with the carer centred interventions, the economic data in these carer and patient targeted interventions, focus on resource use and costs without combining these costs with outcomes. This limits the value of the evidence for informing decisions where cost-effectiveness is an important consideration. Three out of four of the findings are based on RCTs and findings were mixed. Mant et al. 24 found positive clinical outcomes from the intervention but mixed economic outcomes; Glass et al. 25 found negative clinical outcomes from the intervention and no difference in economic outcomes; and Forster et al. 26 found no difference in clinical outcomes but positive economic outcomes. Parker et al. 27 made no comparisons and reported no outcomes. Among the methodological limitations, it is important to note that the interventions target both patients and carers and it is therefore impossible to tell to what extent outcomes were due to the carer component of the intervention.
Discussion
There are few full economic evaluations of interventions targeted at carers of people with stroke, leaving the evidence base for such interventions unclear. Of the 10 papers reviewed, many examined resource use but not associated costs. Few examined resource use or costs from a broad perspective (e.g. societal) therefore potentially missing any cost-shifting between sectors. Only three studies9,20,21 linked cost data with outcome data within the framework of a ‘formal’ economic evaluation; each of these found that the intervention was less costly and had better or equal clinical outcomes than the comparator but two of these were based on the same intervention using the same dataset. These studies examined caring-web and carer training.
More general limitations of the reviewed papers included limited reporting of methods, low follow-up rates, short follow-up lengths and statistical under powering. Further, many studies report on resource use data which are not included in the costs, but there is no rationale of excluding of these resources from the costs. Additionally, many studies did not explicitly state information such as location of research and currency. Although this can often be assumed (or ascertained through contacting authors), failure to report such information as standard is poor practice.
Our search identified protocols for four studies which have not yet published their results28-31 and may usefully add to this evidence base in the near future. Our search also identified abstracts for five studies which appeared relevant, however, full papers were not available (even after contacting the authors) to allow a full assessment of eligibility, nor to include the study in this review.32-36
Previous systematic reviews have concluded that most interventions for informal carers have some clinical benefits on patients, carers, or both.3,4,7,8 However, effects are often small to moderate and often clinically insignificant. Further, these studies were often of low quality, preventing firm conclusions being drawn. To draw conclusions about the cost-effectiveness of such interventions, more high quality full economic evaluations are needed.
This review suffers from a number of limitations. A major challenge with reviewing evidence in this area is the heterogeneity and complexity of the interventions 37 and the differing target participants (carer focussed, patient and carer focused, and patient focused). As interventions are multicomponent, it is not possible in this review to identify the active ingredients. This is especially challenging for interventions that focus on both carers and patients. Other variations limiting the comparisons that can be made included: study design; inclusion criteria; levels of patient disability; evaluation perspectives; period to which costs related; differences in health care systems; currency; and country. In addition to the potential positive reporting bias that may affect all literature searches, we may further have biased our review by excluding grey literature and non-English language studies.
The need for stroke carer based interventions is clear. From those studies that have conducted full economic evaluations, there is some limited evidence that these interventions are cost effective compared to existing alternatives. It is difficult to draw firm conclusions on cost-effectiveness for informing clinical practice due to the variation in the types of interventions and comparators examined in different studies. Similarly, a number of methodological limitations undermine the conclusions that can be drawn where evidence of relevance to the issue of intervention cost-effectiveness is reported. As the evidence reviewed comes mainly from the United Kingdom and United States its applicability outside of these countries also remains uncertain.
To extend knowledge on the effectiveness and cost effectives of interventions for carers of stroke patients, and to distinguish the impact of carer interventions compared to interventions which focus on patients and carers, further research is needed using well-designed RCT-based economics evaluations, focusing solely on the carer component of these interventions.
Clinical messages
Few studies have conducted economic evaluations of interventions for informal carers of stroke patients.
Of the studies that have conducted full economic evaluations, there is some weak evidence that these interventions (caring-web and carer training) are effective and cost effective.
Footnotes
Acknowledgements
We would like to thank Deirdre Andre, Information Specialist, University of Leeds for conducting the systematic searches for this review.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.