
Abstract
Objective
The study purpose was twofold: (1) to develop the Children’s Amputee Mobility Predictor and establish its content and social validity and (2) to determine its intra and inter-rater reliability.
Design
A reliability and validity study.
Setting
Pediatric rehabilitation hospital.
Participants
Content validity study: 10 clinical experts; Social validity study: 24 stakeholders (i.e., children’s parents); Reliability study: 3 physical therapists.
Intervention
Not applicable.
Main measure
The functional capability of 30 children with leg length discrepancy was evaluated using the Children’s Amputee Mobility Predictor. The Intraclass Correlation Coefficient, two-way mixed model, and absolute agreement for a single measure were used to establish intra and inter-rater reliability.
Results
Experts reached a consensus on the relevancy and clarity of all 26 tasks included in the Children’s Amputee Mobility Predictor. The intra- and inter-rater reliability were excellent, Intraclass Correlation Coefficient (ICC)2,1 = .95, with 95% CI ranging from 0.88–0.98; and ICC3,1 = 0.96 with 95% CI ranging from 0.93–0.98, respectively. Parent feedback indicated the relevancy of tasks for children with leg length discrepancies.
Conclusions
The Children's Amputee Mobility Predictor is a comprehensive outcome measure that requires minimal equipment or space. It appears stable over time when used by the same physical therapist and results suggest that it may be used by multiple physical therapists. The Children's Amputee Mobility Predictor appears to measure important and relevant aspects of functional capability and be a meaningful and relevant assessment tool, helping to guide the determination of medical necessity for specific prosthetic and physical therapy interventions.
Introduction
Most childhood leg length discrepancies stem from congenital deformities, and some from traumatic injuries, oncological consequences, and long-term complications of infections. 1 A child with a leg length discrepancy requires a prosthesis or Extension-prosthesis to participate in home, school, and community activities. Typically, the treatment team determines the child's functional capability based on a subjective evaluation of their physical examination, medical history, current condition, including residual limb status, and medical diagnosis. 2 The determined functional capability of the child guides the medical necessity for prosthetic and physical therapy interventions. Standardizing this process necessitates an instrument capable of classifying children with leg length discrepancy based on their functional level and quantifying their abilities.
The physical examination includes a range of motion and manual muscle testing, as well as the assessment of functional tasks like transitioning from sitting to standing, maintaining balance while standing, and hopping on one leg. 2 Additionally, clinicians may use outcome measures such as the Gross Motor Function Measure, 3 Peabody Developmental Motor Scales-2, 4 Pediatric Evaluation of Disability Inventory, 5 Pediatric Balance Scale, 6 Timed-Up-And-Go, 7 2- or 6-min walk,8,9 and the 10-meter walk test. 10 These tests provide clinicians with insight into the child's gross and fine motor skills, balance, and mobility status, but the ability to indicate which skills require enhancement to achieve optimal function is limited. 11
In the adult population with leg length discrepancy, the Amputee Mobility Predictor is employed to assess the functional capabilities associated with the use of a prosthesis. 12 The Amputee Mobility Predictor includes 21 items assessing strength, endurance, balance, postural control, power, speed, agility, and gait. The Amputee Mobility Predictor, while a reliable and valid tool for assessing functional capability in adults, is limited in evaluating the unique characteristics of the pediatric population. In general, children have shorter bone lengths than adults, have a less developed balance system, and their daily routines include unique activities such as transitioning to sit on the floor, kicking or throwing a ball, and running. Thus, there is a need to develop an outcome measure that includes the specific characteristics of this population when evaluating their functional capability.
The purposes of the present study were twofold: (1) to develop an instrument for the evaluation of functional capabilities in children with leg length discrepancy and establish its content validity and social validity and (2) to determine the intrarater and inter-rater reliability among physical therapists using the new instrument.
Methods
The Amputee Mobility Predictor informed and guided the development of the Children's Amputee Mobility Predictor. A research team that included three physical therapists (two specialists in leg length discrepancies in children, one expert in developing outcome measures) and a physician certified in pediatric orthopedics led the development of the Children's Amputee Mobility Predictor. The research team examined the Amputee Mobility Predictor and identified four specific tasks necessitating modifications to better accommodate children's anthropometrics and gross motor developmental milestones (Table 1). All other tasks from the Amputee Mobility Predictor were retained unchanged although the chair size used for the sitting tasks was adjusted based on children's anthropometric measurements to ensure that they could sit with hip and knee angles of 90°. Furthermore, five more tasks were identified as clinically and age-appropriate relevant to assess function in the target population.13–17 Those included (1) kicking a ball, (2) throwing a ball, (3) transitioning to sitting on the floor, (4) transitioning to standing from sitting on the floor, and (5) running.
Description of modifications to the amputee mobility predictor tasks.
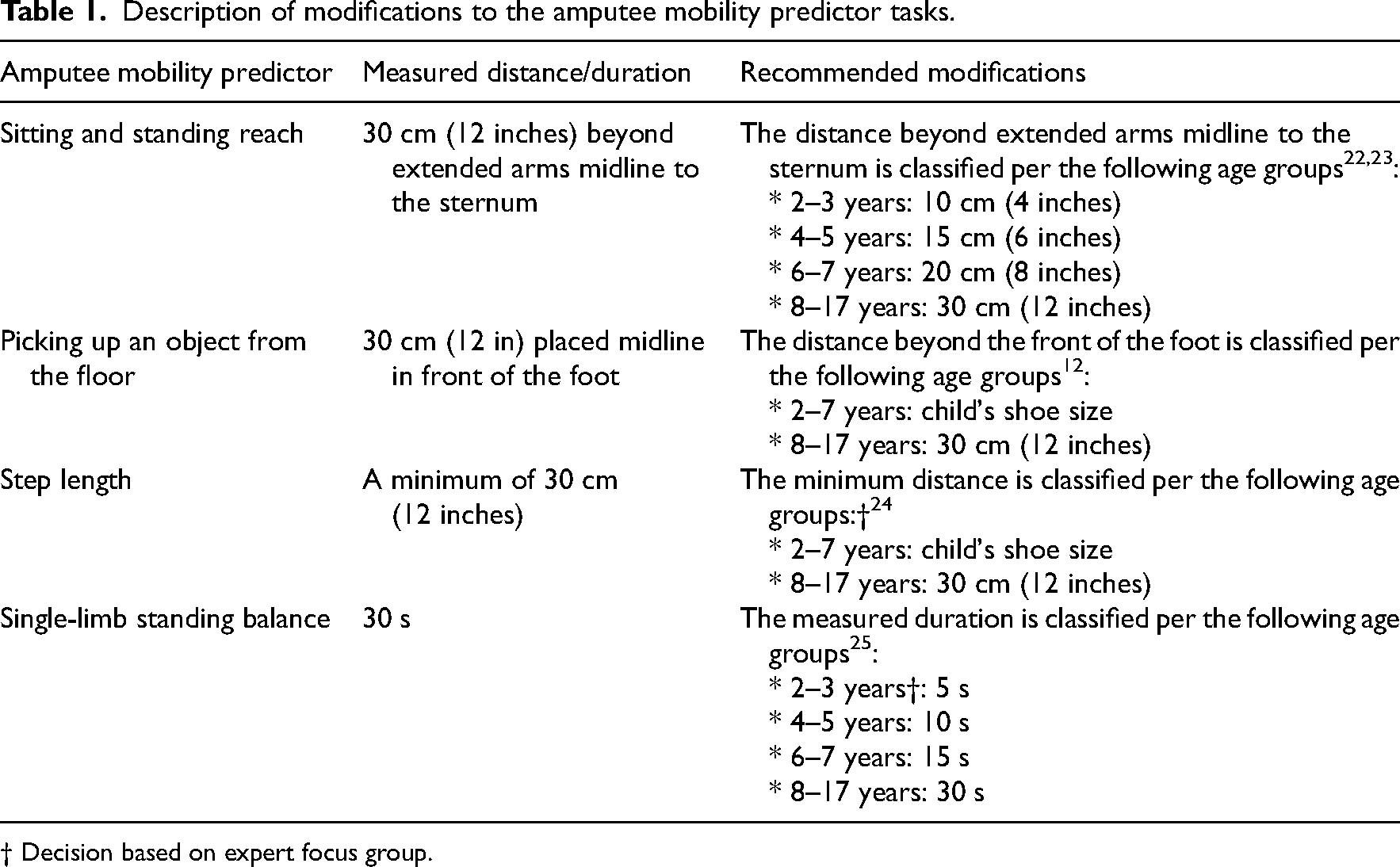
† Decision based on expert focus group.
Content validity of the Children's Amputee Mobility Predictor was assessed by a focus group of experts from various disciplines (i.e., physical and occupational therapy, prosthetics, and physicians specializing in orthopedics, rehabilitation, and pediatric medicine). The focus group discussed the clinical relevance and appropriateness of the tasks included in the Children's Amputee Mobility Predictor. They reached an agreement on the operational definitions of the five new tasks and the recommended modifications to the distance and duration for each of the four specific tasks. The final version of the Children's Amputee Mobility Predictor includes 25 tasks that are scored on a 2- or 3-point scale, where a score of zero indicates an inability to perform a task. For tasks scored on a 2-point scale, a score of one indicates the ability to perform the tasks without any issues. For tasks scored on a 3-point scale, a score of one reflects performance with some issues, while a score of two indicates performance without issues. The use of assistive devices is scored last using a 5-point scale (Supplementary material provides a detailed description of instructions and scoring for each task).
The procedure for assessing inter-rater reliability involved comparing the Children's Amputee Mobility Predictor scores of three physical therapists, while the intrarater reliability involved comparing two assessment scores completed by the same physical therapist. A convenience sample of children and adolescents with unilateral leg length discrepancies were recruited between May 2022 and January 2024 at ALYN Hospital Pediatric and Adolescent Rehabilitation Center. Participants were included if their age was 2–17 years old, their amputation was due to congenital, infectious, oncology, or trauma, and they used a prosthesis or Extension-prosthesis. Participants were excluded if they could not follow instructions or were within less than a year of orthopedic surgery of the involved leg. Parents of all participants as well as participants aged 16 and older, signed an informed consent, approved by the hospital's Helsinki Committee for Human Ethics. All in-person assessments were conducted by an expert physical therapist who was part of the research team. The physical therapist documented participants’ demographics, personal and medical history, as well as prosthetic information. Next, the Children's Amputee Mobility Predictor was administered and scored. Simultaneously, video recordings were captured from a coronal-oblique view as participants performed all tasks, enabling visualization of the participants’ whole body from a perspective that incorporates both the frontal and sagittal planes. After a 1-h tutorial on scoring, two experienced physical therapists independently reviewed the video recordings and scored each participant separately. Two weeks following the in-person assessment, participants returned for a second assessment, where the Children's Amputee Mobility Predictor was administered and scored. A rehabilitation physician reviewed the video recordings and documented each participant’s functional level.
The social validity of the Children's Amputee Mobility Predictor was assessed at the end of the in-person evaluation using a task relevance questionnaire. Parents rated the importance of 18 selected tasks from the Children's Amputee Mobility Predictor in their children's daily activities using a 5-point Likert scale (1 = completely nonrelevant, 2 = nonrelevant, 3 = neutral, 4 = relevant, and 5 = completely relevant). 18
Descriptive analysis included frequencies and percentages for categorical and ordinal data and means and standard deviations for continuous data. The social validity results are described using medians and interquartile ranges. The Intraclass Correlation Coefficient (ICC), two-way mixed model, and absolute agreement for a single measure was used to establish intrarater (ICC2,1) and inter-rater (ICC3,1) reliability. 19 The ICC examines the effects of systematic and random errors on measurement repeatability, and its values range from 0.00–1.00. 20 Values less than 0.50 reflect poor reliability, moderate 0.50–0.75, good 0.75–0.90, and excellent values > 0.90. 19 Agreement between assessments from the two sessions was tested using the Bland–Altman plot to identify the mean difference between ratings and the 95% confidence interval for the limits of agreement. A paired t test was also used to examine differences between the two rating sessions and was used to establish the mean difference, standard deviation, and 95% confidence interval for the Bland–Altman plot.
The minimal detectable change was determined using a 95% confidence interval, calculated as = Standard Error of Measurement × √2 × 1.96. This value signifies the extent of genuine change between measurements required to surpass measurement error and variability. The 95% confidence interval was derived by employing 1.96 as the z-value for two-sided intervals and √2 to accommodate the variance between the two measurements. The standard error of the measurement was calculated as = pooled standard deviation*√1-ICC. 21
The sample size was determined using Arifin's web-based calculator. 22 Key parameters were set as follows: minimum acceptable good reliability (ICC) at 0.75, expected reliability at 0.9023,24 α at 0.05, 1-β at 0.80, k at 3, and a 10% dropout rate. 25 Accounting for the dropout rate, the calculated sample size was 24 participants. Analyses were performed using SPSS 28.0 software (SPSS Inc., Chicago, Illinois). Significance was set at p < 0.05.
Results
The physical therapist conducting the in-person assessments had 32 years of experience. The other two physical therapists who observed videos of participants to score the Children's Amputee Mobility Predictor had 5 years of experience. While administering the Children's Amputee Mobility Predictor, two tasks posed challenges for younger participants. Six children were unable to perform Task #13, “Standing with eyes closed,” with five of them aged five years or younger. Task #22, “Variable cadence,” also proved challenging for three children, all of whom were 3 years or younger. Therefore, when calculating the total score, tasks in which the child was unable to comply with the instructions were classified as “not tested.” The total score of the Children's Amputee Mobility Predictor was determined as a percentage of the total score, excluding tasks labeled as “not tested” from the overall calculation, with scores ranging from 0 to 100%.
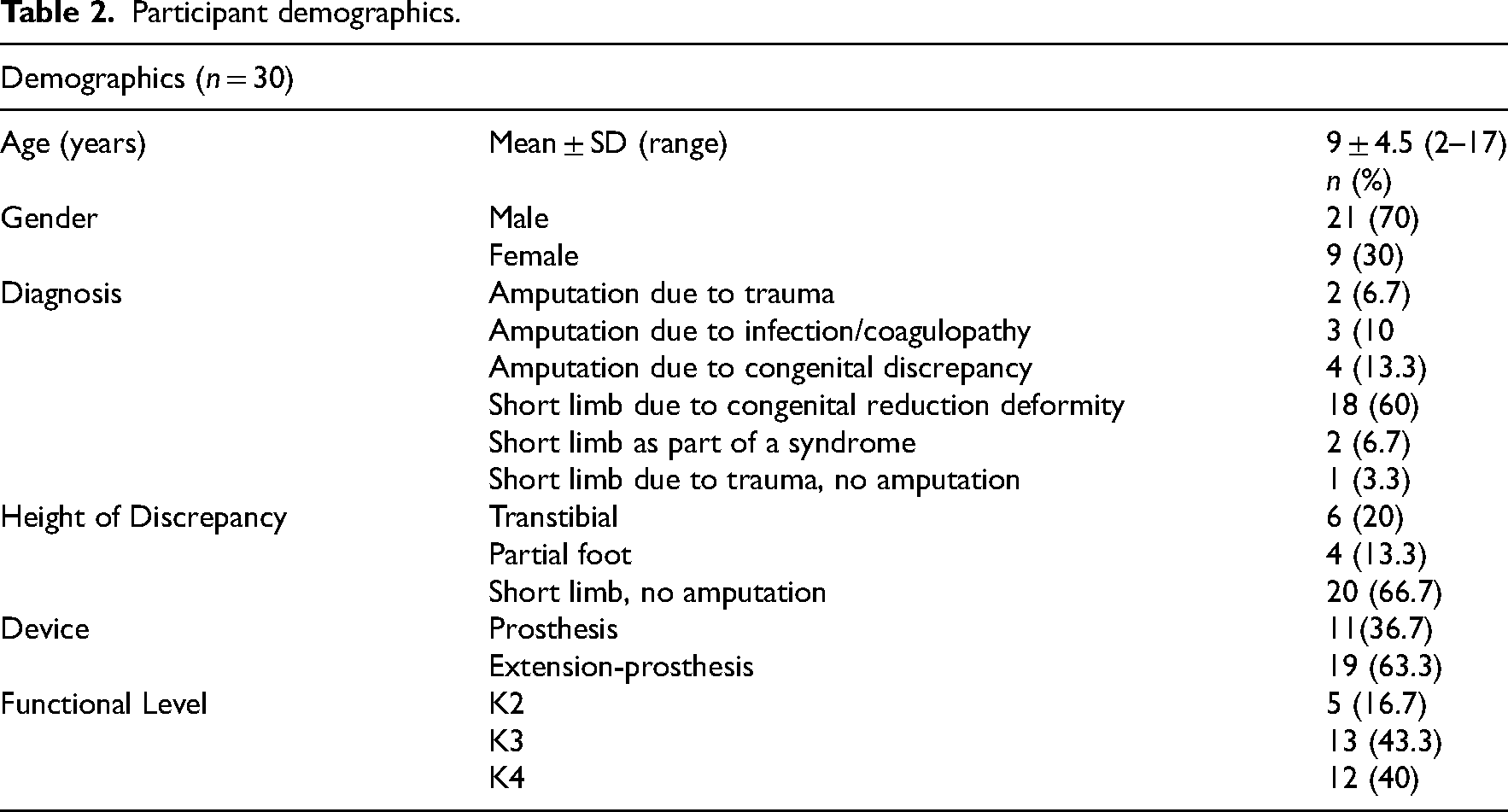
A total of 30 participants with leg length discrepancies who met the inclusion criteria participated in the study, and their characteristics are presented in Table 2. Most participants were male (70%). The leading diagnosis was a short limb due to congenital reduction deformity (60%), and the most common reason for length discrepancy was due to a short limb without amputation (66.7%). Most participants use Extension-prosthesis (63.3%) and are at either K3 (43.3%) or K4 functional level (40%).
Participant demographics.
A total of 17 participants completed the study protocol twice within a two-week interval. The intrarater reliability was excellent, ICC2,1 = 0.95, and the 95% CI ranged from .88–.98. No statistically significant differences were observed across the ratings between sessions 1 and 2 (p = 0.131). The standard error of means, indicating the extent of measurement error, was 2.36. The minimum detectable change at a 95% confidence interval, representing the smallest discernible difference detectable by the Children's Amputee Predictor and not attributable to chance or measurement error, was 6.52.
The Bland–Altman plot reveals a small systematic negative bias (−1.29 ± 3.34 standard deviation) with a 95% confidence interval between −3.01 and .42 (Figure 1), indicating that, on average, the second assessments (85.1%) were higher than the first assessments (83.8%). From the distribution of paired differences, it seems that there are no systematically meaningful differences.
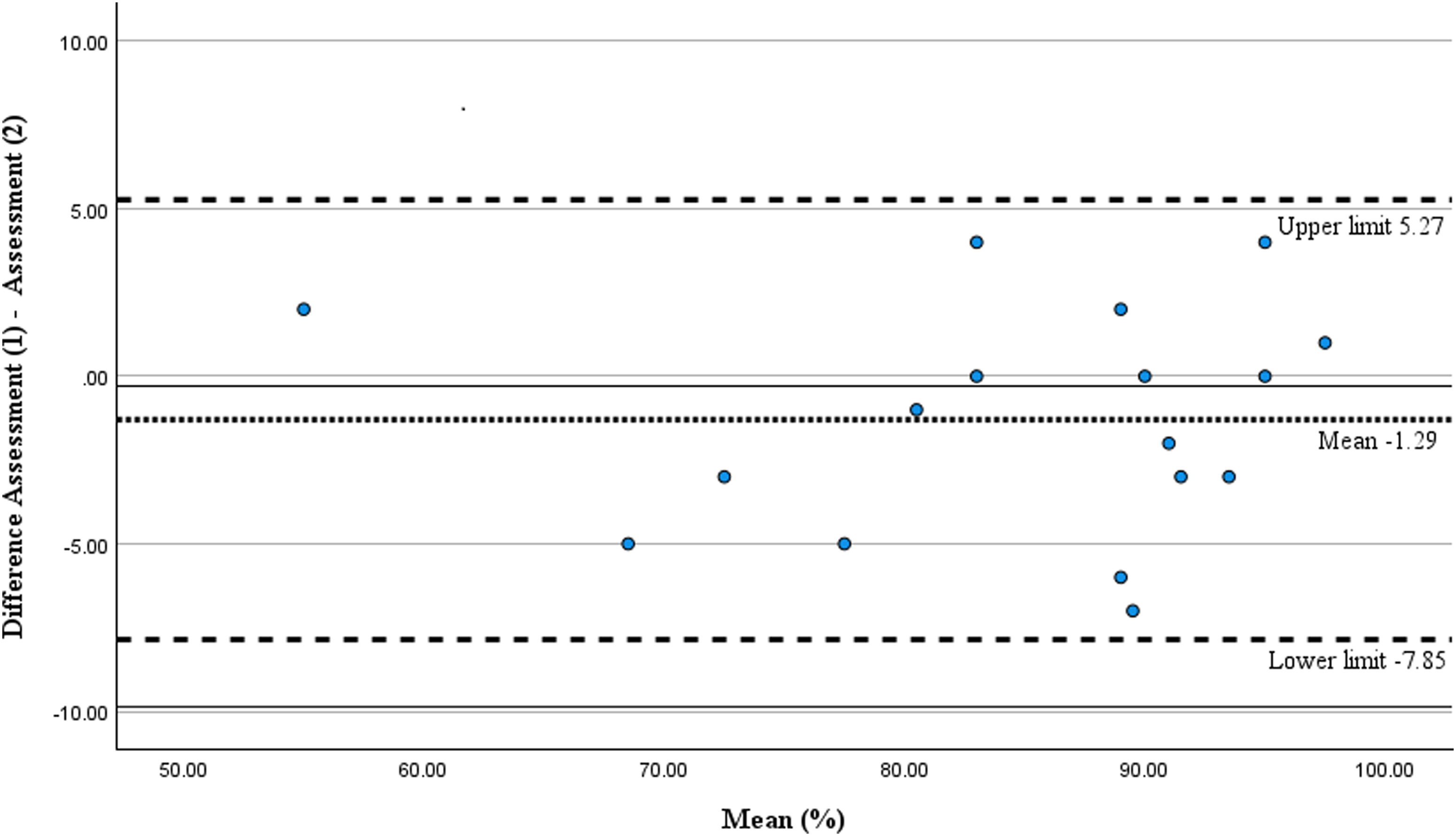
Bland–Altman plot for the differences between assessments from the two test sessions against the mean of the two test sessions for each participant.
The inter-rater reliability was excellent, ICC3,1 = 0.96, and the 95% CI ranged from 0.93–0.98. A total of 24 parents of children with leg length discrepancy completed the task relevance questionnaire. Median values, ranging from 4–5 for the 18 selected tasks, show that overall, parents reported that they were either relevant or completely relevant to assessing the functional capabilities of children (Figure 2).
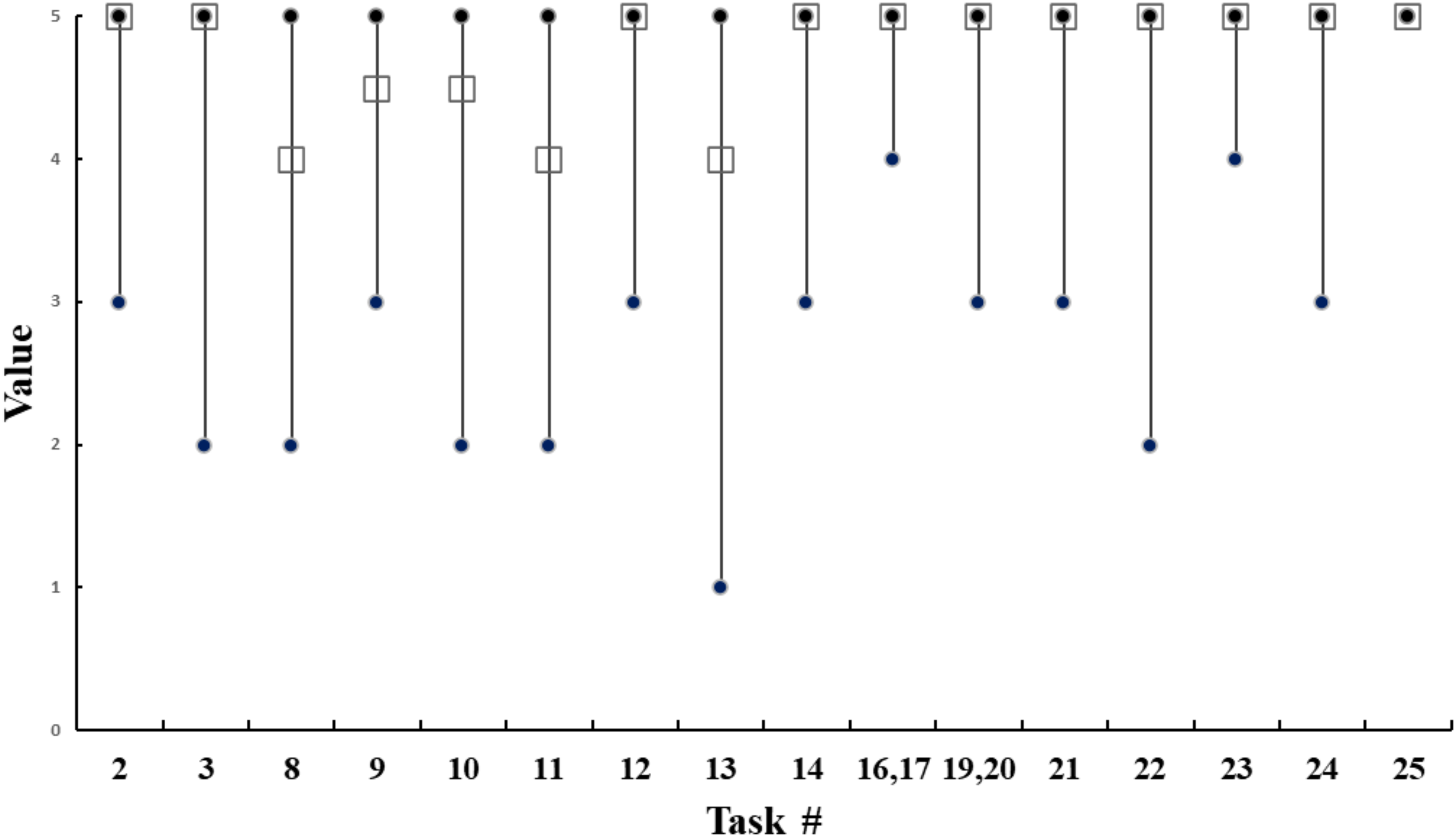
Median, maximum, and minimum values for the social validity for 18 of the Children's Amputee Mobility Predictor tasks. Note: Black open squares represent the median values; black circles represent the minimum and maximum values for each task. The tasks are: 2 = sitting reach, 3 = chair to chair transfer, 8 = single limb standing balance, 9 = kicking a ball, 10 = standing reach, 11 = throwing a ball, 12 = “Nudge” test, 13 = standing with eyes closed, 14 = picking up object off the floor, 16 = sitting down on the floor from standing, 17 = standing up from sitting on the floor, 19 = step length, foot clearance, 20 = step continuity, 21 = turning around, 22 = variable cadence, 23 = stepping over obstacle, 24 = running, 25 = stairs.
Discussion
The present study examined the reliability and validity of a novel outcome measure for children with leg length discrepancies, the Children's Amputee Mobility Predictor. Utilizing a consensus-driven approach within an expert focus group ensured the suitability of the Children's Amputee Mobility Predictor in evaluating the functional capabilities of children with leg length discrepancy. Additionally, feedback from parents indicating the relevance of the 18 selected tasks supports the social validity of the Children's Amputee Mobility Predictor. The excellent intra- and inter-rater reliability suggests that assessing the tasks included in the Children's Amputee Mobility Predictor is stable over time when used by the same clinician and dependable when used by multiple clinicians, respectively.
While content validity is evaluated by experts to ensure the tasks adequately sample the content universe of functional capability, social validity provides insight into what parents consider important and relevant for evaluating the functional capability of children with leg length discrepancy. These two viewpoints do not necessarily align, as experts may focus on comprehensive coverage of functional domains, while parents might prioritize practical relevance. For instance, experts decided to include Task #12, the “nudge” test, due to its crucial role in restoring balance during daily activities, despite concerns from some clinicians about potentially intimidating participants, in particular younger children. Conversely, families rated this task as highly important without expressing concerns, acknowledging its practical significance in their child's daily life, where they encounter challenges to their balance during games, sports activities, and dynamic play scenarios. These perspectives highlight the importance of considering both expert assessment and parental perspectives in developing effective functional assessments for children with leg length discrepancies.
The current study results demonstrated excellent intra- and inter-rater reliability for the Children's Amputee Mobility Predictor. The Bland–Altman plot showed a small systematic negative bias (−1.29) between the two assessments completed by the same physical therapist. The negative sign of the bias indicates that scores on the second assessment tended to be higher. When compared with the minimal detectable change (6.52), this small bias was found to be nonmeaningful. This suggests that the administration and scoring of the Children's Amputee Mobility Predictor by the same rater is stable over time. In this study, two methods were used to score participants’ performance: in-person and while observing participants’ video recordings. In-person scoring allows for close observation of the child's immediate reactions and interactions, providing insights into their comfort level and ease with each task. This can be important as subtle cues such as hesitation, adjustments, or discomfort may indicate underlying challenges. However, given that the Children's Amputee Mobility Predictor employs a straightforward scoring system, this complexity should not have posed a significant challenge for the physical therapists who used video recordings for scoring.
During the administration of the Children's Amputee Mobility Predictor, two tasks presented challenges for participants. Notably, Task #13 “Standing with eyes closed” was particularly difficult for children aged five years and younger. The National Institutes of Health Toolbox assesses standing balance with eyes closed across ages 3–85 years for 50 s. 26 During task development, experts in the focus group expressed concerns that 50 s may exceed the capabilities of young children whose proprioceptive and vestibular systems may not yet be fully developed for maintaining balance without visual input. 27 In the absence of supporting evidence for age-specific durations, experts agreed to test all ages for the 30-s duration specified in the Amputee Mobility Predictor. However, future research should explore appropriate age-specific durations to better align with children's abilities in this task. Similarly, Task #22 “Variable cadence,” presented challenges, especially for children aged three years and younger. This task demands motor coordination and control, requiring participants to adjust their walking speed, a skill that younger children may still be refining.28,29 Also, variability in cadence necessitates cognitive processing and adaptability, which may exceed the developmental capabilities of very young children, further complicating their performance in this task. 29 This observation led the research team to provide the option to designate a task as “not tested” and exclude it from the total score calculation. This enhances the precision of assessing children's functional abilities across different developmental stages.
Three limitations should be considered when employing this study's results to make clinical decisions. First, content and social validity represent a low level of validity evidence. 30 They rely primarily on subjective assessments, which may not accurately reflect the measure's ability to comprehensively capture the functional capabilities of children with leg length discrepancy. Therefore, future studies should aim to establish higher levels of validity evidence, such as construct validity and criterion-related validity, by using objective data and statistical analyses. Second, caution should be exercised when interpreting the intrarater reliability results, as the sample size in this study was limited; further research with larger cohorts is warranted to confirm these findings. Third, the examination of inter-rater reliability involved three physical therapists, two of whom solely observed video recordings to score participants’ performance without administering the outcome measure. During task administration, raters can introduce errors such as random inconsistencies in their observations, biases that consistently affect outcomes, and deviations from standardized procedures. 31 These errors may affect the test scores and reduce the instrument's reliability. Future studies should examine the impact of different raters administering the test to understand how administration variations may influence inter-rater reliability.
The Children's Amputee Mobility Predictor is a comprehensive outcome measure characterized by a straightforward scoring system that can be administered in about 30 min, depending on the child's age, understanding, and abilities. Additionally, it requires minimal equipment and space. Its excellent intra- and inter-reliability suggests that multiple physical therapists could use it with results that are consistent over time. The content and social validity of the Children's Amputee Mobility Predictor indicates that it accurately measures relevant aspects of functional capability and is perceived by parents and clinicians as a meaningful and appropriate assessment tool for children with leg length discrepancies. Because it provides objective information on the child's functional capabilities with prosthesis or Extension-prostheses, it may help guide the medical necessity for specific prosthetic and physical therapy interventions.
Children's Amputee Mobility Predictor is a comprehensive outcome measure featuring simple scoring requiring minimal equipment/space. It has excellent intra- and inter-rater reliability. Its content validity indicates that it measures essential and relevant functional capabilities in children with leg length discrepancies. Its social validity demonstrates a meaningful and relevant assessment.Clinical messages
Supplemental Material
sj-pdf-1-cre-10.1177_02692155241295991 - Supplemental material for Children's amputee mobility predictor—Assessing the functional capability of children with leg length discrepancy
Supplemental material, sj-pdf-1-cre-10.1177_02692155241295991 for Children's amputee mobility predictor—Assessing the functional capability of children with leg length discrepancy by Sharon Eylon, Nurit Stern, Itai Schurr, Itzhak Siev-Ner, Patrice L. Weiss and Anat Kristal in Clinical Rehabilitation
Footnotes
Acknowledgments
The authors would like to thank Dr Robert S. Gailey for his permission to use the Amputee Mobility Predictor as a guide in developing the Children's Amputee Mobility Predictor, and for the valuable advice and guidance he provided. The authors also thank the participants, their families and the expert members of the focus group.
Author Contributions
Conceptualization, S.E., N.S. and I.S.; methodology, S.E., A.K. and P.L.W.; formal analysis, A.K.; investigation, S.E., N.S., A.K. and P.L.W.; writing-original draft preparation, S.E., P.L.W., A.K.; writing-review and editing, S.E., A.K., N.S., P.L.W., I.S.-N., I.S.; visualization, A.K. and P.L.W.; supervision, S.E.; project administration, S.E.; funding acquisition, S.E. and P.L.W.
Availability of Data and Materials
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The research protocol was approved by the ALYN Hospital Ethics Committee in accordance with the accordance with the provisions of the World Medical Association Declaration of Helsinki (approval number 043-21). No information that could identify subjects will be published. Parents of all participants, as well as participants aged 16 and older, signed the informed consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Leona M. and Harry B. Helmsley Charitable Trust, (grant number 2207-05386).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.