
Abstract
Objective
To use behavioural science frameworks to synthesise evidence on the factors influencing physical activity of patients hospitalised after stroke outside of staff-led rehabilitation sessions.
Data Sources
A systematic review of qualitative and mixed-methods studies. MEDLINE, PsycINFO, CINAHL, and AMED were searched from inception to October 2024 for studies that explored influences on the physical activity of patients hospitalised after stroke.
Review Methods
Data were coded with reference to the Theoretical Domains Framework and the COM-B (‘capability’, ‘opportunity’, ‘motivation’ and ‘behaviour’) model. Thematic analysis was used to group data extracts into themes within each Theoretical Domains Framework domain. Risk of bias was assessed using the Mixed Methods Appraisal Tool.
Results
We identified 17 studies. There was no significant risk of bias concerns. We identified 19 themes across eight Theoretical Domains Framework domains and all COM-B model categories. The most frequently recognised themes were found in three Theoretical Domains Framework domains: Environmental Context and Resources (themes: 1 – availability of sufficient skilled staff to facilitate physical activity; 2 – design and use of the physical environment; 3 – lack of opportunities or incentives; 4 – passivity and institutionalisation; 5 – perceived and actual rules and culture of the ward); Skills (theme: physical impairments); and Social Influences (theme: activity influenced by family and friends).
Conclusions
The review highlights the complexity of the influences on the physical activity of patients hospitalised after stroke outside of staff-led rehabilitation sessions. It is likely multi-component interventions addressing a number of influences will be required to effectively improve physical activity. PROSPERO ID: CRD42022383506.
Background
In the sub-acute phase after a stroke, a higher dose of physical activity is associated with sustained rehabilitation gains, 1 and there is a strong dose–response relationship between therapy and physical recovery in the sub-acute and chronic phases of stroke. 2 The 2023 National Clinical Guideline for Stroke for the UK and Ireland recommends that: ‘people undergoing rehabilitation after a stroke should be supported to remain active for up to 6 hours a day’; this may include up to three hours of activity that is outside of therapist-delivered therapy. 3 Yet in the UK and internationally, objectively measured levels of physical activity in hospital after stroke are consistently shown to be low, especially outside of therapist-delivered sessions. 4
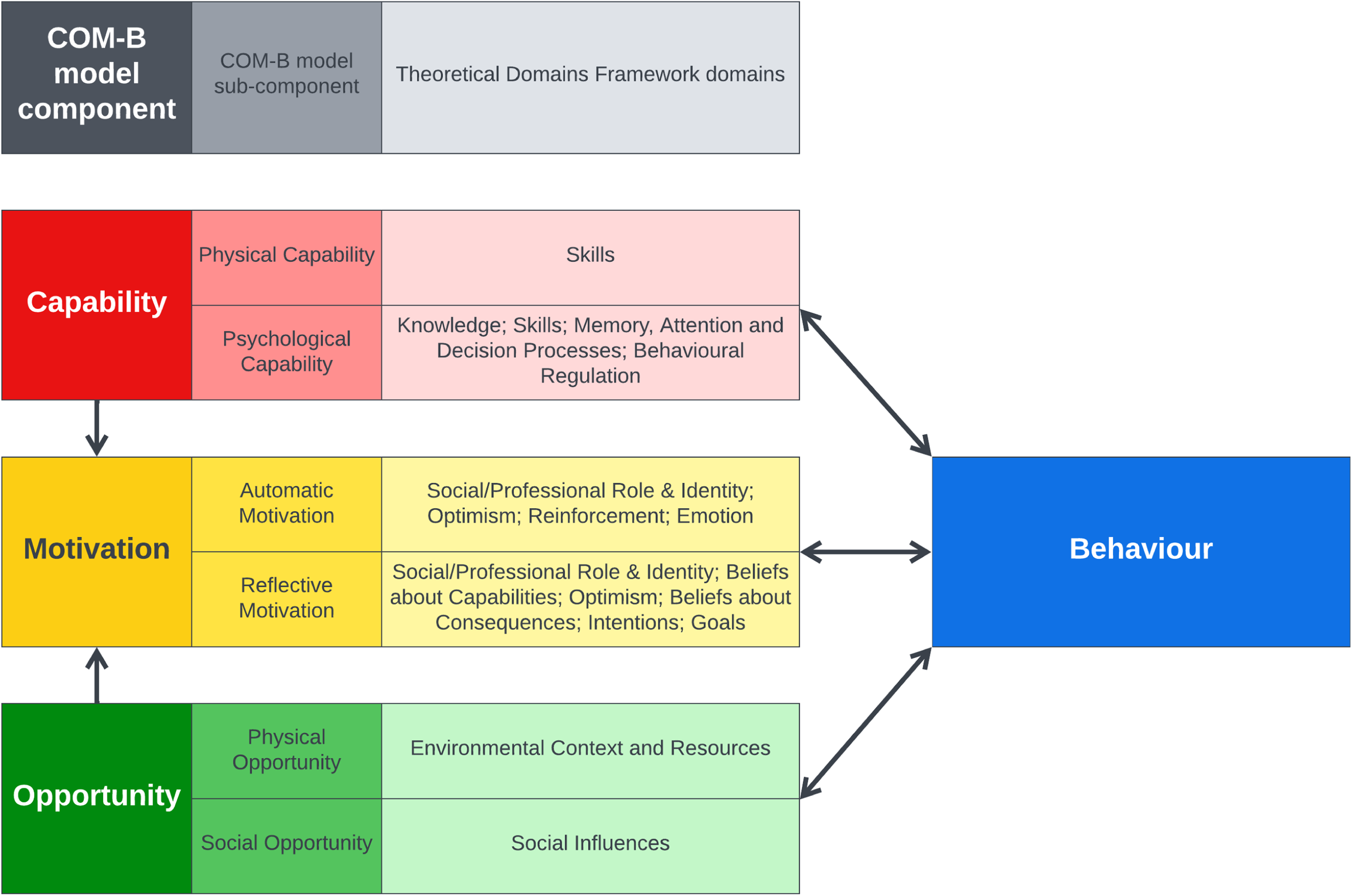
Increasing physical activity in hospital has been shown to be challenging.5–7 The development of complex interventions to increase physical activity in hospital may benefit from the use of behaviour change theory. 8 Behavioural influences can be categorised using various models including the COM-B model 9 and Theoretical Domains Framework.10,11 The COM-B model describes a behaviour in terms of three categories (six sub-categories) that are necessary for the behaviour to be performed: capability (physical and psychological), opportunity (physical and social), and motivation (reflective and automatic). 9 The Theoretical Domains Framework further defines these categories into 14 domains which can be mapped onto the COM-B model (Figure 1).10,11
The Behaviour Change Wheel supports intervention development by mapping the behavioural influences that have been identified to different intervention options that should affect the influences, and thus achieve the desired behavioural change. 9 Therefore, an understanding of the influences on physical activity behaviour in hospital after stroke would allow for the development of interventions that are targeted at influencing factors that may be amenable to change. The aim of this review is to use the COM-B and Theoretical Domains Framework to synthesise current evidence on the influences on the physical activity of patients in hospitals after stroke outside of staff-led rehabilitation sessions.
Methods
A protocol for this review was registered on PROSPERO: CRD42022383506 (https://www.crd.york.ac.uk/prospero). The review has been reported in keeping with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 13
The following databases were searched electronically between inception and 6 December 2022: MEDLINE via OVID; PsycINFO via EBSCOhost; Allied and Complementary Medicine Database (AMED) via OVID; CINAHL via EBSCOhost. Updated searches were completed on 16 January 2024 and 2 October 2024. The search strategy is presented in full in the online supplementary material. If a conference abstract was identified that appeared relevant, searches were made to identify a full paper; if no paper was found the abstract was excluded. All reference lists of included studies were searched for other potentially relevant studies missed by the electronic search of databases.
The target behaviour of interest is the physical activity of patients in the hospital. The definition of physical activity includes any bodily movement produced by skeletal muscles that requires energy expenditure. 14 Included studies had to refer to physical activity. Studies that included analyses of staff-led rehabilitation sessions were included if they also reported on physical activity outside of staff-led rehabilitation sessions. We excluded studies that only evaluated physical activity during staff-led sessions such as physiotherapy sessions.
We included qualitative and mixed-methods studies that explored influences on physical activity behaviour. We included post-implementation evaluations of interventions if the evaluation of physical activity was not specific to a particular activity or exercise. In addition, we excluded papers only available as an abstract or conference proceedings and non-English language studies.
We included studies that examined the physical activity of adults (18 + years) admitted to hospital with an acute stroke. Data on influencing factors could be gathered from various sources, including observations or interviews with patients, their families or visitors, and hospital ward staff. We excluded studies that evaluated the physical activity of samples, who on average were beyond the subacute phase (i.e., with an average time since stroke of more than 12 weeks) of rehabilitation.
The settings of included studies were inpatient hospital wards, either acute stroke wards (including specialist stroke high dependency units), or inpatient rehabilitation wards. Studies that included critical care units were excluded.
Two reviewers independently examined all titles and abstracts by using the pre-defined eligibility criteria. If a reason for exclusion was not evident, the full manuscript was obtained. Full manuscripts of all the studies that remained after title and abstract screening were subsequently examined independently by two reviewers. Disagreements were resolved through discussion with a third author.
Descriptive data for each included study was extracted by one reviewer and checked by a second. Descriptive data included: study design, aim, setting, methodology, sample size, and participant characteristics (i.e., time since stroke or staff disciplines).
Two reviewers independently extracted details related to physical activity behaviour. Where it was not clear whether quotes or statements within included studies referred to physical activity as opposed to social or cognitive activity, the quotes or statements were not included in the analysis.
The risk of bias was assessed using the Mixed Methods Appraisal Tool. 15 If the analysis plans of mixed-methods studies included the integration of qualitative and quantitative data on influences on physical activity, the mixed-methods tool was used; otherwise, the qualitative tool was used. If a study employed mixed methods for additional reasons to investigate the influences on physical activity and only utilised qualitative data for the investigation of influences on physical activity, the qualitative tool was used, regardless of additional quantitative methods not relating to the aims of this review.
Data synthesis aimed to identify themes in the included studies that describe behavioural influences, and organise themes according to the domains of the Theoretical Domains Framework. Each domain could have multiple or no themes. To achieve this, first, two reviewers independently coded each paper using a deductive approach; that is, data were coded with reference to the Theoretical Domains Framework and COM-B model,10,11 using NVivo software. After coding independently, results were exported to Google Sheets software and merged. The two authors reviewed all data coded under each domain of the Theoretical Domains Framework. Each domain was discussed, and all data were checked for consistency and to resolve any differences. At this point, the two reviewers interrogated the data to determine whether there was agreement that the code excerpts related to physical activity (e.g., as opposed to social activity). Where quotes were coded to more than one Theoretical Domains Framework domain, a final decision was made as to which domain and component the data best reflected. Throughout this process, if disagreements were not readily resolved, a third author was asked to contribute their opinions. Final agreement was then made between all three authors. Thematic analysis 16 was then used to inductively analyse data within each Theoretical Domains Framework domain, to group data extracts into themes. Themes could have a positive, negative, or mixed impact on patient physical activity. Although the COM-B model was not used to categorise themes directly, in certain situations, reviewers referred to its category and subcategory definitions to help select the most appropriate domain within the Theoretical Domains Framework. Specifically, when a theme could be classified under two different domains of the Theoretical Domains Framework, each corresponding to different COM-B subcategories, reviewers took into account the COM-B model's definitions to guide their final decision. The number of studies in which each theme was identified was counted to provide a measure of generalisability.
Results
The search identified 20 studies5,17–35 (Figure 2). For the purpose of counting the frequency of themes across different studies, certain manuscripts were grouped together as they predominantly used the same data from the same participants, meaning the maximum frequency a theme could be recognised in different studies was 17. Three publications referred to the same programme of work, the Collaborative Rehabilitation in Acute Stroke (CREATE) study and were treated as a single study.5,19,23 The study by Kenah, Tavener 32 reported a secondary analysis of data presented in Janssen, Bird, 21 including an extra 25 participants.
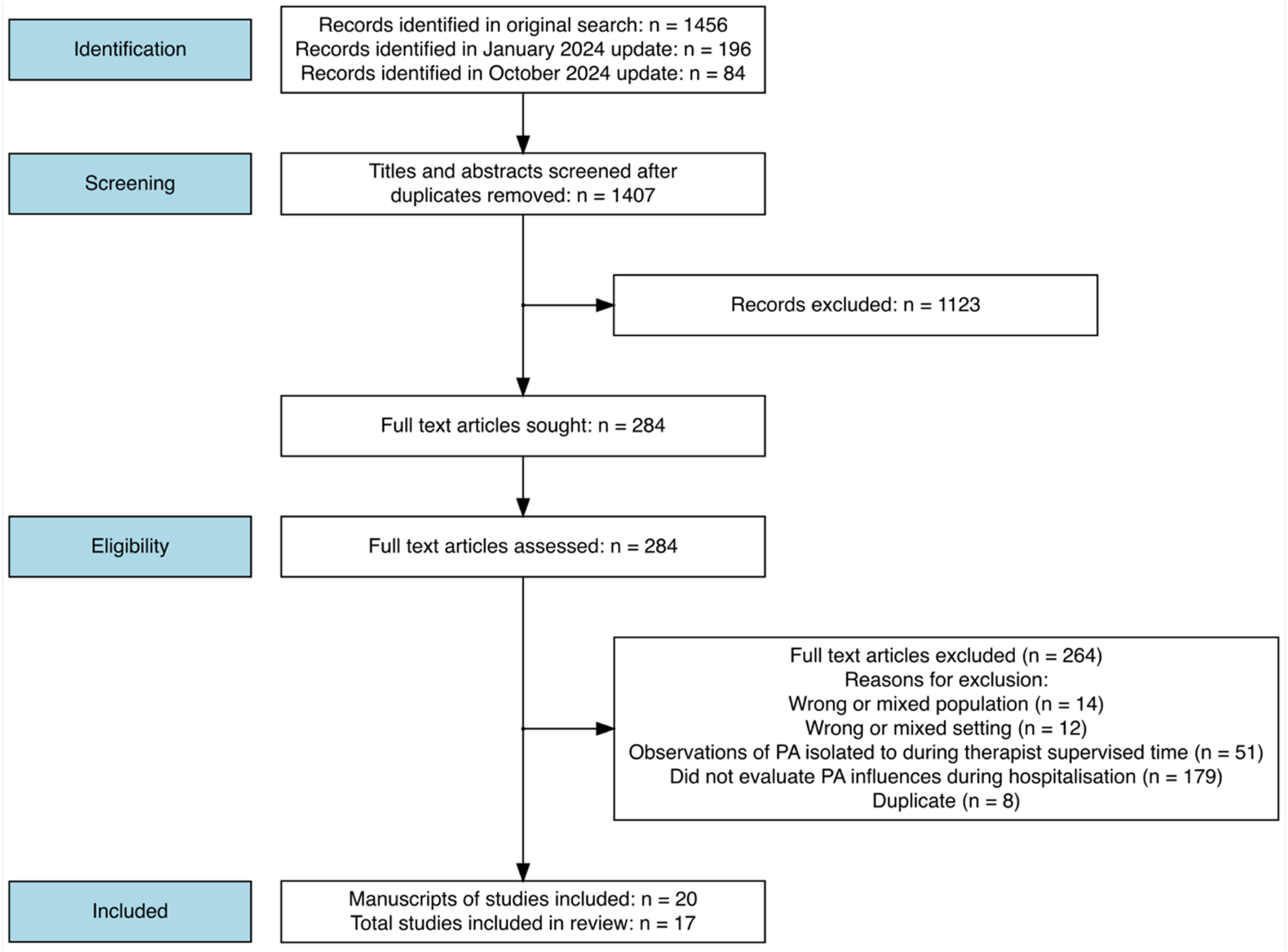
Study flow diagram.
Descriptions of studies are provided in Table 1. Five studies used mixed-methods,17,18,23,26,30,33 10 studies employed qualitative methods.20–22,24–29,31,32,34,35 Morton, Hall 26 examined behaviour across both inpatient and community settings, though we extracted data only related to the inpatient setting.
Study characteristics.
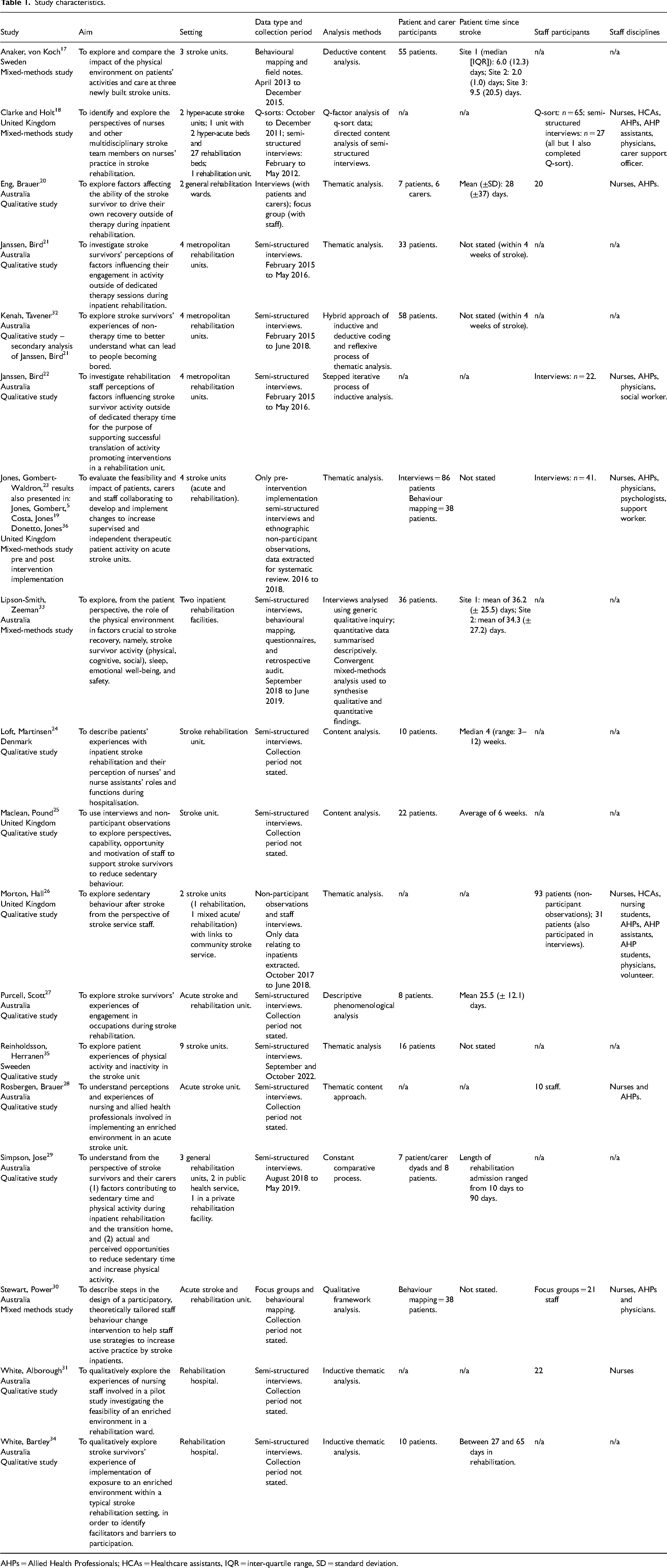
AHPs = Allied Health Professionals; HCAs = Healthcare assistants, IQR = inter-quartile range, SD = standard deviation.
Risk of bias as assessed by the Mixed Methods Appraisal Tool 15 is summarised in the online supplementary material. Although both Morton, Hall 26 and Jones, Gombert-Waldron 23 used mixed methods as part of their wider project aims of developing interventions, for the purposes of this review, only the qualitative data relating to physical activity influences was extracted. As a result, only the qualitative questions of the Mixed Methods Appraisal Tool were assessed. There were no significant concerns with risk of bias scoring. For the qualitative methodological quality criteria, only three studies had domains scored as ‘can’t tell’ due to insufficient reporting,20,25,35 but no other concerns were identified.
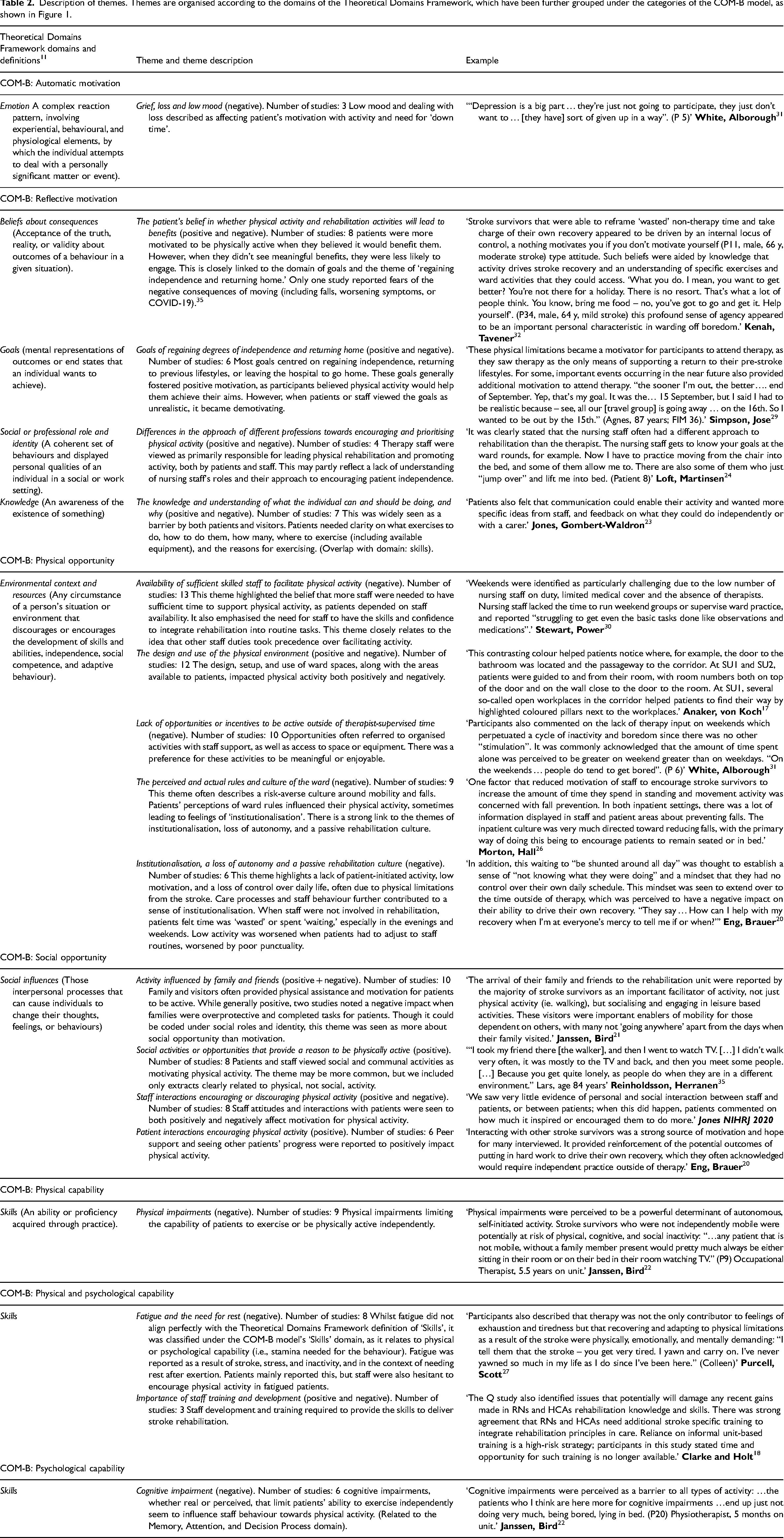
We identified 19 themes across eight Theoretical Domains Framework domains and all six sub-categories of the COM-B model. All themes are described in Table 2, within the text we provide more detail on the six themes that were recognised in over half of the included studies. The people whose behaviour was identified in the themes as influencing the patients’ physical activity, included the patients themselves, staff, and family members.
Description of themes. Themes are organised according to the domains of the Theoretical Domains Framework, which have been further grouped under the categories of the COM-B model, as shown in Figure 1.
Of the eight Theoretical Domains Framework domains, ‘Environmental Context and Resources’, defined as any circumstance of a person's situation or environment that discourages or encourages the development of skills and abilities, independence, social competence, and adaptive behaviour, 11 was the most consistently recognised behavioural influence (16 of 17 studies). We identified five different themes within this domain, including four in at least nine different studies.
The theme of the availability of sufficient skilled staff to support physical activity largely related to the perception (of patients, families, and researchers) that staff were often too busy to assist with additional physical activity outside of basic needs and therapist-led rehabilitation. This issue particularly affected patients with more severe physical impairments (i.e., those needing assistance to mobilise), especially during evenings and weekends: In many cases, participants expressed that they were too busy to prioritise facilitating patient access to EE [Enriched Environment] over their other demands. This was despite concerns that patients were often sedentary. (White, Alborough)
31
This factor suggests less-experienced staff endorse the rehabilitation philosophy expressed in stroke units, but these inexperienced nurses and therapists may lack of confidence in RNs’ and HCAs’ [Health Care Assistants’] skills to independently support ADL [activities of daily living] practice. (Clarke and Holt)
18
Therapists reported a need to prioritise tasks that facilitated discharge and impacted on their ability to coach and train stroke survivors to practice with less supervision. (Stewart, Power)
30
…. I was lost every day. Everything looked the same. As soon as I walked out of my room the passages are all painted the same, the doors are the same. I’d go down to the dining room and I couldn’t find my way back to my room. (P2, male, 76 yr)’ (Janssen, Bird)
21
Communal mealtimes were considered to enhance frequent physical activity, for example, walking to and from meals and sitting up for breakfast and lunch. (Rosbergen, Brauer)
28
Site 1 had no shared space (day room) in which patients and visitors could meet, and visitors were cramped by the bedside. Site 2 had a day room but it was used mainly for staff meetings and equipment storage; this was replicated at site 3, which had a garden but it was accessible only through the day room, which patients did not use. At site 4, the day room had become a storage area for wheelchairs and specialist stroke chairs; another seating area was routinely used by staff for taking breaks and storing cleaning equipment. (Jones, Gombert-Waldron)
23
Participants also commented on the lack of therapy input on weekends which perpetuated a cycle of inactivity and boredom since there was no other ‘stimulation’. It was commonly acknowledged that the amount of time spent alone was perceived to be greater on weekend greater [sic] than on weekdays. ‘On the weekends … people do tend to get bored’. (P 6) (White, Alborough)
31
Whilst many participants valued opportunities for rest, for others there was just too much downtime in their therapy schedule which contributed to boredom and frustration that there was ‘nothing to do’ and they were ‘wasting time’ in rehabilitation. (Kenah, Tavener)
32
Similarly, while patients reportedly appreciated therapists’ encouragement to exercise on their own, it was rare to see them doing so. (Costa, Jones)
19
In addition, this waiting to ‘be shunted around all day’ was thought to establish a sense of ‘not knowing what they were doing’ and a mindset that they had no control over their own daily schedule. This mindset was seen to extend over to the time outside of therapy, which was perceived to have a negative impact on their ability to drive their own recovery. ‘They say … How can I help with my recovery when I’m at everyone's mercy to tell me if or when?’ (Eng, Brauer)
20
In hospital, participants consistently reported a strong focus on safety from staff, particularly relating to falls. Many considered that standing and walking were discouraged to reduce this risk. (Simpson, Jose)
29
Engagement in activity was at times influenced by perception of what participants were and were not allowed to do, the perceived and actual ward rules reported to render them powerless to initiate activity autonomously. The perception that the rehabilitation staff needed to know where they were at all times was commonly reported with an awareness to ensure they adhered to any restrictions around independent mobility. ….I didn’t like to leave the room in case they said, ‘Well where is she? Where's she gone?’ So I just sat there and did a crossword puzzle and did that sort of thing. (P1, female, 90 yr) (Janssen, Bird)
21
The Theoretical Domains Framework domain ‘Skills’ refers to abilities acquired through practice and is linked to the capability component of the COM-B model. This domain appeared in 12 studies, with four themes identified, most notably ‘physical impairments’, which was present in nine studies.
Physical impairments consistently limited patients’ ability to be physically active, particularly in terms of independent mobilisation and reliance on others for assistance. These impairments were largely attributed to the stroke: Participants had wide ranging views on what could be offered to enhance engagement in occupations outside of therapy. Many understood the challenge in achieving this due to a combination of factors surrounding the person, the environment, and the occupation of choice. For example, Mark stated that although there may be many activities that stroke survivors may want to engage in outside of therapy, physical limitations may not make it possible ‘You’ve got to be well enough to be able to be mobile, to get out there, and do something. Some of the people there are not mobile at all. They’re just stuck in bed.’ (Purcell, Scott)
27
Family and friends were often facilitators of physical activity, providing assistance and motivation for walking and exercises. Patients with supportive visitors had more opportunities to stay active: Family and visitors encouraged physical activity in hospital by practising walking, exercises and facilitating community visits. In contrast, people without family or with few visitors lacked such opportunities to be more active in hospital. I had probably three a week [visitors]. They’re all much older than me…they’ve got problems and they couldn’t stay for long…I was available, all bushy-tailed, wide-eyed and waiting [to go for a walk], and it just didn’t always happen [Mary, (60–80y) living alone] (Simpson, Jose)
29
Along with the need to conform to the routines and rules of the hospital environment, a loss of independence with mobility commonly limited stroke survivors from being able to freely leave their bedroom and participate in meaningful activities to occupy their non-therapy time. ‘I kept to the room; I didn’t walk around much on my own. Actually, the greater part of my stay I was not allowed to walk on my own, I only went for walks when my husband came to visit…so I was pretty much restricted until he came in.’ (P23, female, 68 y, moderate stroke) (Kenah, Tavener)
32
Discussion
We identified many positive and negative influences on physical activity outside of staff-led rehabilitation sessions of individuals hospitalised after a stroke. The review highlights the complexity of the behaviour and the challenges in trying to modify levels of physical activity and supports evidence of the benefit of multi-component interventions, targeting multiple behavioural determinants in improving levels of physical activity in this population. 37 Although the most frequently highlighted influences on physical activity referred to three Theoretical Domains Framework domains: Environmental Context and Resources, Skills, and Social Influences, themes were identified in a total of eight domains, with overlap into others.
The most frequently recognised theme was the availability of sufficient skilled staff to facilitate physical activity. This theme, along with the lack of opportunities or incentives to be active outside of therapist-supervised time, was especially evident on weekends when fewer therapists are typically present. These themes are indirectly supported by quantitative evidence from several studies showing lower physical activity levels on weekends compared to weekdays.38–44
The theme of perceived and actual ward rules and culture often referred to a risk-averse approach that limits independent physical activity to reduce falls, which can cause serious physical and psychological harm. 45 Many stroke patients in the hospital are at high risk of falling and may not fully appreciate or adjust to this risk. 46 However, falls prevention strategies may not only be ineffective but can also restrict physical activity and overall autonomy.47,48 This may worsen issues like institutionalisation, loss of autonomy, and a passive rehabilitation culture.
The second most common theme was the design and use of the physical environment. The validity of the theme is supported by studies showing that design elements like single rooms versus multi-bed bays are linked to activity levels.17,49 Similarly, communal activities, such as shared meals, are also associated with increased physical activity. 50
The availability and involvement of family and visitors can reduce reliance on staff for facilitating physical activity. Research supports this, showing family presence is linked to increased activity.51,52 However, this influence is complex. As seen in the studies reviewed25,29 and other work, family involvement can both help and hinder rehabilitation. 53 While many families wish to be involved in their relative's recovery,54,55 this can strain relationships. 54 Given the stress on relatives,55,56 more research is needed to find ways to better support and include them in rehabilitation. Additionally, social frailty may worsen health inequalities, requiring consideration of equitable rehabilitation support for patients without visitors to assist with physical activity.
The link between physical and functional impairments and activity levels after stroke is well established.41,44,52,57–69 This issue, largely related to capability, is hard to separate from the environmental and social factors discussed earlier. Evidence on improving physical activity post-stroke primarily focuses on patients with mild symptoms, with limited research on those with severe impairments, cognitive deficits, or post-stroke fatigue. 37 This highlights the significant role of the COM-B model's capability category in determining activity levels after stroke.
A key limitation of the evidence in this review is the difficulty in consistently distinguishing between physical, social, and cognitive activity. While we focused on physical activity, it is possible that not all data were correctly classified. Similarly, while the review excluded data related to staff-led rehabilitation sessions, distinguishing between these and other activities was not always clear due to the nature of the data and analysis methods used in the primary research. As a result, some themes may have been unintentionally influenced by data or interpretations from staff-led sessions.
The synthesis of qualitative research has limitations, as we rely on the detail, context, and interpretation provided in the included manuscripts without access to the original data. Some nuances may have been missed or misinterpreted, leading to decontextualised findings. 70 We took a pragmatic approach by focusing on the most frequently identified themes, though these may not represent the most influential factors and should not be viewed in isolation.
Intervention development should account for all identified factors. Although not highlighted in this review, complex micropolitics within healthcare teams 71 may have shaped the behavioural influences and efforts to address them. Addressing these critical contextual factors is likely crucial for the success of future quality improvement or research initiatives. 71
We used the COM-B and Theoretical Domains Framework to synthesise current evidence on influences affecting patient physical activity after stroke outside of staff-led rehabilitation sessions. Identified influences span all COM-B components and at least eight Theoretical Domains Framework domains. This review provides a theoretical foundation for future complex interventions and may aid the understanding of the barriers and facilitators to increasing patient physical activity. Recognising the complexity and interconnectedness of these factors may lead to more effective approaches for improving activity levels.
Supplemental Material
sj-docx-1-cre-10.1177_02692155241293269 - Supplemental material for Influences on the physical activity behaviour of inpatients after stroke outside of staff-led rehabilitation sessions: a systematic review
Supplemental material, sj-docx-1-cre-10.1177_02692155241293269 for Influences on the physical activity behaviour of inpatients after stroke outside of staff-led rehabilitation sessions: a systematic review by Peter Hartley, Katie Bond, Rachel Dance, Isla Kuhn, Joanne McPeake and Faye Forsyth in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155241293269 - Supplemental material for Influences on the physical activity behaviour of inpatients after stroke outside of staff-led rehabilitation sessions: a systematic review
Supplemental material, sj-docx-2-cre-10.1177_02692155241293269 for Influences on the physical activity behaviour of inpatients after stroke outside of staff-led rehabilitation sessions: a systematic review by Peter Hartley, Katie Bond, Rachel Dance, Isla Kuhn, Joanne McPeake and Faye Forsyth in Clinical Rehabilitation
Footnotes
Data Availability Statement
The corresponding author will make data available upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical approval was not required as the review did not include any primary data collection.
Funding
Peter Hartley is supported by Homerton College and the Health Foundation's grant to the University of Cambridge for The Healthcare Improvement Studies Institute (THIS Institute). THIS Institute is supported by the Health Foundation, an independent charity committed to bringing about better health and health care for people in the UK.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.