
Abstract
Objective
This study aimed to co-design and develop a user-centred, theory-based eHealth-mediated self-management support follow-up prototype for adults with musculoskeletal disorders.
Design
A three-step system development cycle was employed. Step 1 involved creating intervention features and content, with two focus groups reviewing prioritised eHealth intervention elements based on earlier research. Step 2 involved heuristic testing using Nielsen's 10 heuristic principles. Step 3 incorporated qualitative think-aloud interviews and the System Usability Scale.
Setting
Republic of Ireland.
Participants
Step 1 included adults with musculoskeletal disorders (n = 12). Step 2 involved five reviewers. Step 3 included people with musculoskeletal disorders (n = 5) and musculoskeletal physiotherapists (n = 5).
Results
Participants in step 1 approved four main intervention components, which map to recognised theoretical frameworks, and suggested increased use of visual and interactive elements. Heuristic testing in step 2 identified design and navigation issues. In Step 3, usability testing, additional navigation, content and design recommendations were identified. The overall median system usability score (interquartile range) was 75 (0) out of 100 for adults with musculoskeletal disorders and 77.5 (2.5) out of 100 for musculoskeletal physiotherapists, indicating good usability.
Conclusion
A theory-based, user-centred eHealth-mediated follow-up self-management support prototype has been developed for people with musculoskeletal disorders, with the next steps focusing on feasibility testing in clinical practice, with a more diverse population.
Keywords
Introduction
The burden of musculoskeletal disorders is becoming more profound, leading to a corresponding increase in the demand for rehabilitation. 1 Despite this, significant gaps exist, with rehabilitation services ill-equipped to meet the high demand. 1 The World Health Organisation's ‘Rehabilitation 2030: A Call for Action’ 2 has highlighted this care disparity, with eHealth interventions increasingly recognised as an urgently needed, scalable and cost-effective solution.
Self-management involves patient education and behaviour modification, aimed at teaching people the skills to manage all aspects of their condition. 3 Self-management is not the sole responsibility of the person with the musculoskeletal disorder; 3 the treatment approach is collaborative with the clinician providing continuous support. Given the strain on healthcare systems, there is increasing interest in the role of eHealth to provide this support.
An eHealth intervention is any digital technology applied in a healthcare setting. 4 Based on end-user preferences, 5 for this study, the term refers to an internet-based or mobile application intervention, two of the most common eHealth intervention types. 6 Despite fragmented literature, 6 studies provide moderate-quality evidence that eHealth interventions can reduce pain and improve function for people with musculoskeletal disorders.7–10 However, these benefits are typically short-term, 9 modest, 7 and their long-term efficacy remains unproven.6,8 Although user-centred design is recommended, 11 it is often not adopted in eHealth intervention development, which may contribute to poor engagement and limited impact. 12 This gap may stem from a lack of clear guidance on tailoring this process to suit different aims and settings. 12
This study aims to co-design a theoretically robust eHealth prototype for follow-up self-management support for people with musculoskeletal disorders, based on their preferences. Designing eHealth interventions to change health behaviours is complex and requires a strong theoretical foundation for effectiveness. 13 While many eHealth interventions reference theory, 6 they often fail to clearly link components to theoretical constructs, 14 representing an implementation barrier.12,15–17 This gap has prompted calls for interventions to be mapped against recognised taxonomies.14,17,18 The ‘eHealth: It's TIME’ project is novel in its integration of three key frameworks: the Practical Review in Self-Management Support taxonomy, 3 which identifies broad intervention components such as remote monitoring with feedback, 6 Michie et al.'s 15 Behaviour Change Technique taxonomy, which details distinct behaviour change techniques such as goal setting and self-monitoring, 17 and persuasive system design principles, 19 such as nudges and prompts, to enhance behavioural change. 16 Combining these frameworks and utilising a user-centred design approach, a theory-based, patient-centred prototype for follow-up self-management support has been developed for people attending musculoskeletal primary care physiotherapy services. This project is guided by the Center for eHealth Research Roadmap 20 and the Medical Research Council framework. 21
Methods
The methods are described in detail in the study protocol paper 22 and are outlined briefly below. Reporting of this study was primarily guided by the GUIDance for the rEporting of intervention Development framework (GUIDED), 23 with the reporting of the qualitative components informed by the COREQ checklist. 24
The ‘eHealth: It's TIME’ project is being conducted in the Republic of Ireland, where musculoskeletal physiotherapy services exist within an almost 50:50 two-tier ‘public-private’ model. MK, a female senior musculoskeletal physiotherapist with over 13 years of experience, is leading the project. She holds a taught postgraduate masters in musculoskeletal physiotherapy, works in the public healthcare sector, and is currently a part-time PhD candidate. MK, trained and experienced in qualitative interview techniques, collected all the data. The research team also includes three academic physiotherapists (JMcV, BF and DM), one academic General Practitioner (CB) and one software developer (EO’R).
The Center for eHealth Research Roadmap 20 informed the design and development of the eHealth-mediated follow-up self-management support intervention. This eHealth-specific roadmap, derived from the review of numerous eHealth and development frameworks, fulfils the Medical Research Council framework criteria 21 while offering more practical guidance. Since this project relates to the design and development of an eHealth intervention (rather than the implementation or evaluation), the focus is on the first three phases of the Roadmap. For the contextual inquiry phase, a comprehensive systematic scoping review 6 was conducted to map the current literature, highlighting that people with musculoskeletal disorders are seldom involved in developing eHealth-mediated self-management interventions. For the value specification phase, a qualitative study 6 was conducted to establish stakeholder perceptions on eHealth-mediated self-management support since the COVID-19 pandemic began in the Republic of Ireland (first case: 29/2/20). These interventions were considered broadly acceptable, although primarily as a follow-up option due to concerns about assessment, diagnosis and establishing a therapeutic relationship.
The eHealth: It's TIME intervention was developed to enhance self-management support for people with musculoskeletal disorders, a key research priority. 25 The development process aimed to co-design and develop an evidence-based and theory-based multi-component prototype for follow-up self-management support via integrated remote monitoring and behavioural change. Based on the contextual inquiry 6 and value specification phases, 5 the prioritised eHealth intervention components (Supplementary File 1) include an information library, a goal-tracking feature, a social forum and a chat function. eHealth: It's TIME intervention will be accessible via computer, laptop, tablet and smartphone. Each person with a musculoskeletal disorder will be provided with a confidential username and password. This intervention is intended for individuals with musculoskeletal disorders who are attending musculoskeletal primary care physiotherapy services, as part of a flexible blended care model. It will be specifically utilised for follow-up care, allowing individuals with musculoskeletal disorders the flexibility to engage in the intervention between face-to-face appointments or towards the end of their care episode, typically before discharge. The feasibility of this approach will be evaluated as part of the next phase of this project.
This study, conducted between January and October 2023, followed a three-step system development cycle study: the creation of intervention features and content (Step 1); heuristic testing (Step 2); and usability testing (Step 3) (see Figure 1). Ethical approval was granted by the Clinical Research Ethics Committee of the Cork Teaching Hospitals (REF: ECM 4 (f) 20/09/2022).
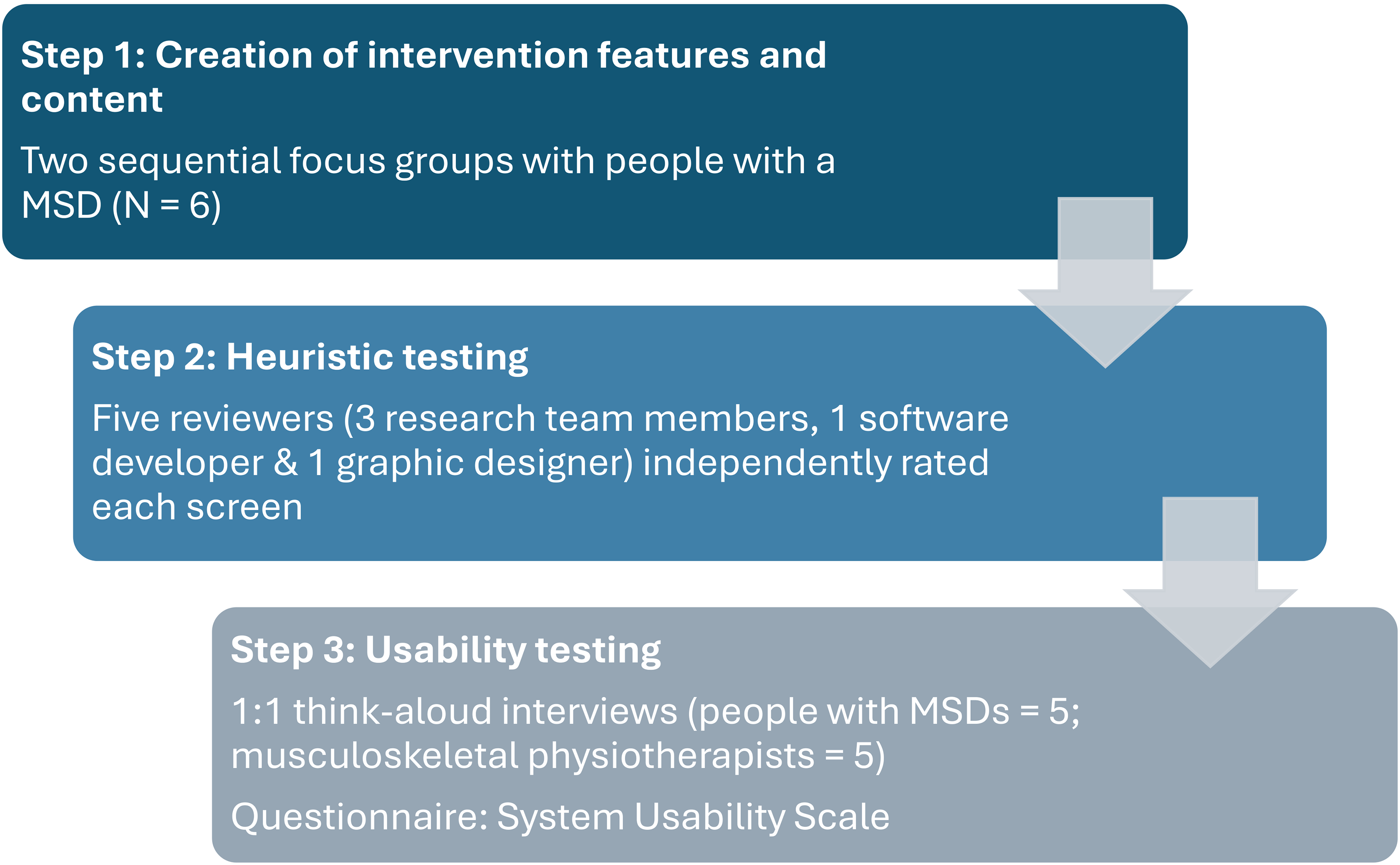
Study overview.
Two of the 22 participants in this study's qualitative component were known to the interviewer, MK, before the study's commencement. Given the challenges associated with this such as the interviewer losing objectivity and participants not being completely truthful in their responses, MK leveraged certain strategies to mitigate these risks. Aware of her personal preference for eHealth, 26 MK completed reflexivity memos throughout the study to avoid projecting her biases and remain open to views that challenged them, aiming to improve the intervention's contextual fit. Other trustworthiness strategies employed within this study are described in the study protocol. 22
Step 1: Creation of intervention features and content
Before the first focus group, paper prototypes of the prioritised eHealth intervention elements were created. The Web Content Accessibility Guidelines 2.1, 27 recognised internationally for enhancing web content accessibility, were considered at each iterative step of the study. In line with recommendations, the readability of content was rated at US grade ≤ 6 (age 11–12 years) with Microsoft Office Software used to confirm this.
All individuals with a musculoskeletal disorder (i.e., target population) met the following eligibility criteria: English speaking (judged by lead researcher MK during pre-interview communication); 18+ years old and can provide electronic or written informed consent. Individuals who had surgery within the past six months, were pregnant or had pain of specific pathological origin (e.g., malignancy, fracture, infection or inflammatory disease); were excluded.
A convenience sampling strategy was employed for this study. Recruitment was advertised on social media (Twitter/X) and via email requests circulated to primary and secondary care in Cork, Ireland, patient support groups, professional organisations and university staff. All interested participants received the participant information leaflet. At one site, Mercy University Hospital, musculoskeletal physiotherapy staff identified participants, and MK conducted eligibility screening. MK informed potentially eligible participants about the study and provided them with a participant information leaflet. Following a 24-h ‘cooling-off period’, MK telephoned the individual with a musculoskeletal disorder, to confirm their interest in participating.
All participants provided electronic consent via Qualtrics (Qualtrics, Provo, UT). Before the focus group, demographic details and the eHealth Literacy Scale were also obtained via Qualtrics.
The first focus group involved the six participants reviewing the paper prototype (see Figure 2), with a topic guide (Supplementary File 2) utilised to flexibly guide the discussion on element/feature acceptability, least and most liked elements and helpful and unhelpful aspects of other health apps and websites previously used. Based on this feedback, a refined click-through prototype was developed using Figma, an online design and prototyping tool (https://www.figma.com/), for the participants of the second focus group to review. For the second focus group, a semi-structured topic guide (Supplementary File 3) was developed to elicit participant views on the individual website and app pages, the functional elements such as hover-effect and click, and other tailoring features. Due to scheduling difficulties, two of the six participants in the second focus group completed one-to-one interviews utilising the same Focus Group 2 topic guide, in line with the study protocol. 22 Both topic guides were developed by the research team and informed by the study aims and a literature review.
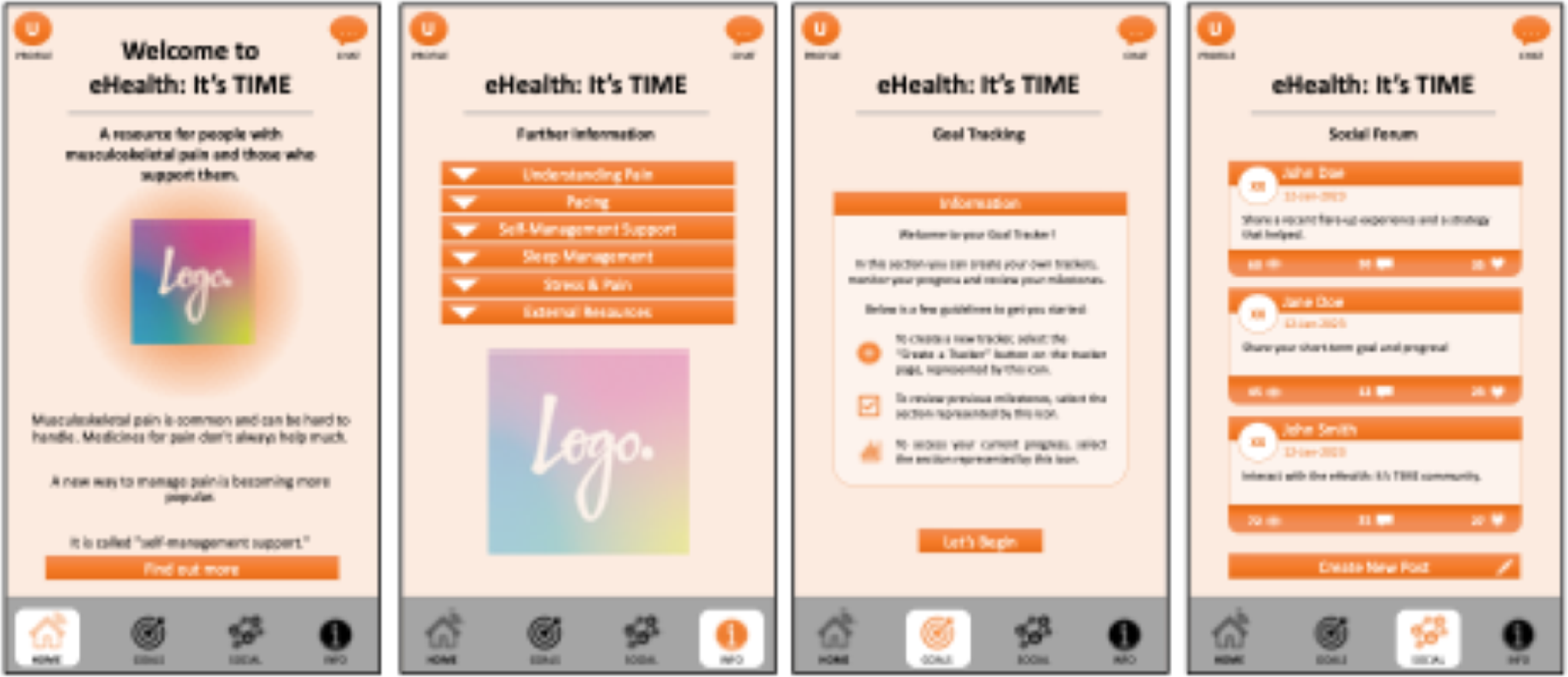
Mobile app paper prototype examples.
All focus groups took place remotely via Microsoft Teams and lasted between 43 and 71 min. Field notes were taken in all focus groups. The focus groups were audio recorded, transcribed verbatim and imported into NVivo. MK completed a descriptive synthesis of the focus group transcripts, 28 systematically summarising all suggestions for prototype refinement. This summary was then reviewed by JMcV and EO’R, who revised the list as required to ensure feasibility within the study's context. The prototype was subsequently refined according to this revised list before heuristic testing.
Step 2: Heuristic testing
Heuristic testing was completed by a panel of five reviewers, consisting of three research team members (BF, DM & CB) and two external experts (a graphic designer and a software developer), none of whom were involved in Step 1. The 10 heuristic principles of Nielsen 29 were used to evaluate the refined web-based and mobile application-based prototype. Each web and application page was independently rated (+1 = complies, −1 = does not comply or 0 = partially complies), with comments provided to justify scores. At a consensus meeting, the ratings were discussed, and an agreement was reached on items to be addressed before usability testing, with the prototype refined accordingly.
Step 3: Usability testing
This step employed mixed methods, combining a qualitative think-aloud interview with quantitative data obtained via the System Usability Scale administered at the end of the interview. This approach is recommended to evaluate prototype usability. 12
Participants in this step included both individuals with a musculoskeletal disorder and musculoskeletal physiotherapists. For individuals with a musculoskeletal disorder, with no prior exposure to the eHealth: It's TIME prototype development, the same eligibility criteria and recruitment strategy as outlined in Step 1 were utilised. All musculoskeletal physiotherapists met the following criteria: working predominantly in musculoskeletal therapy (at least 50% of their time) in either the public or private health setting. A convenience sampling strategy was employed with recruitment for the study advertised on Twitter/X and email requests circulated via physiotherapy managers in Cork, Ireland, and relevant mailing list groups within the Irish Society of Chartered Physiotherapists.
All interested participants were sent a participant information leaflet and the consent form via Qualtrics. Demographic details and the eHealth Literacy Scale were also obtained via Qualtrics before the interview, in line with Step 1. A sample of five has been shown to identify 77–85% of usability issues 30 and hence deemed an adequate target for both participant cohorts.
A think-aloud approach was utilised for the interviews; participants were asked to engage with the technology on their preferred device (mobile phone = 5; laptop = 4; desktop = 1) to work through five relevant scenarios (Supplementary Files 4 & 5) while simultaneously verbalising their thoughts, opinions and feelings about each screen.
All interviews except one took place via Microsoft Teams, with one participant preferring to have the interview in person in a private room within the university. The interviews lasted between 38 and 83 min and were audio recorded. MK took field notes during each interview. All interviews were transcribed verbatim, with transcripts imported into NVivo.
The data was analysed using directed (deductive) content analysis, 31 generating themes for suggestions to improve the application and website, relating to navigation, content and design. This process was conducted by MK and cross-checked by the research team. The resultant final list was then utilised by MK and EO’R to further refine the eHealth: It's TIME prototype. The quantitative data (i.e., System Usability Scale scores) was descriptively analysed using Microsoft Excel.
Results
The results of each step of this study are described below, guided by the Template for Intervention Description and Replication checklist. 32
Step 1: Creation of intervention features and content
A total of 12 people (Table 1) participated in one of the two focus groups. Participants were predominately female (83%, n = 10/12), under the age of 65 years (83%, n = 10/12) and held a higher degree or professional qualification (67%, n = 8/12). All participants had a chronic musculoskeletal disorder with 50% (6/12) having more than one musculoskeletal pain site.
Step 1 – People with musculoskeletal disorders (n = 12).
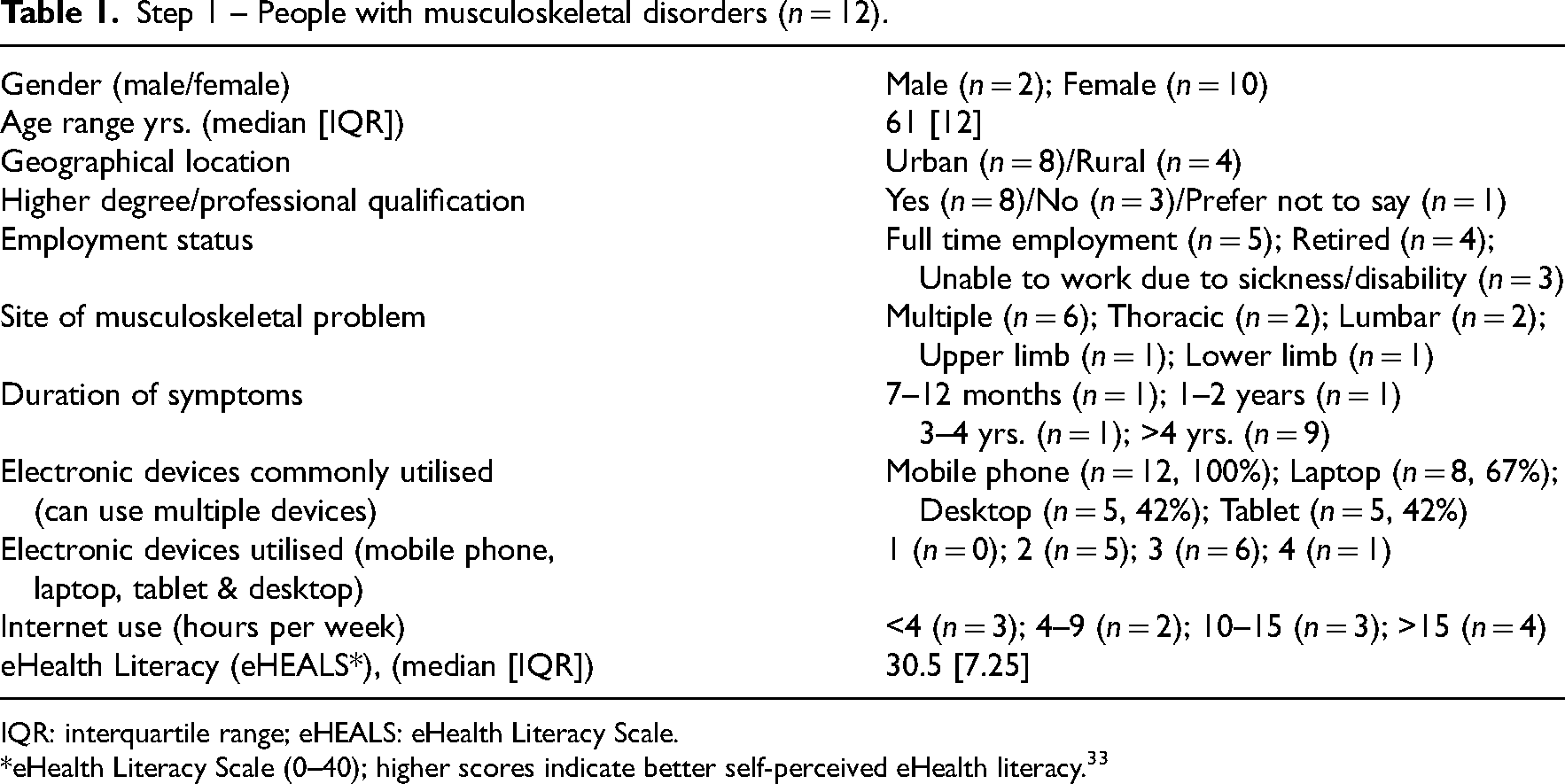
IQR: interquartile range; eHEALS: eHealth Literacy Scale.
*eHealth Literacy Scale (0–40); higher scores indicate better self-perceived eHealth literacy. 33
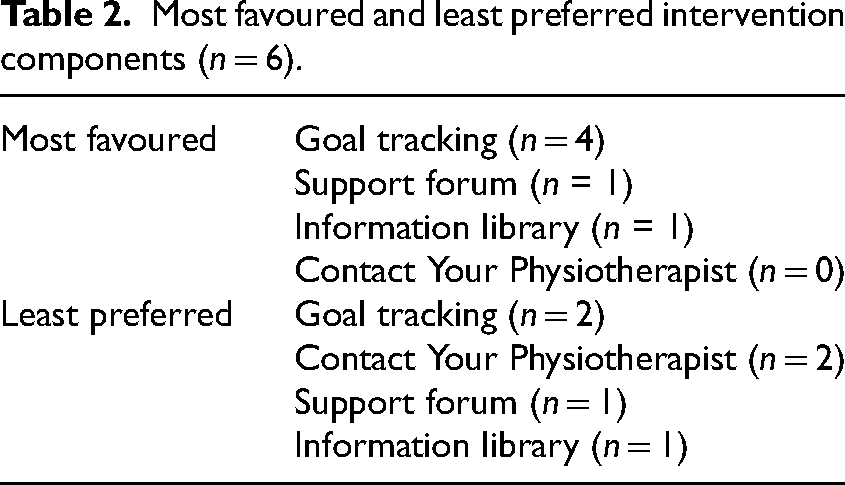
The participants from the first focus group (n = 6) approved the four main prototype components: an information library, a goal-tracking feature, a social forum and a chat function. However, they suggested renaming the latter two components to ‘support forum’ and ‘contact your physiotherapist’. The goal-tracking feature was not only ranked as the most favoured but was also jointly ranked as least favoured alongside the Contact Your Physiotherapist component (Table 2). I'm one of the ones who said the one I liked least [goal tracking] and to be honest, I thought they were all very useful. But I had to pick one…it's just purely I'm old-fashioned in that I just like to write things down and I would tend to do that with a goal, as opposed to having it on any electronic device (Person with musculoskeletal disorder, P2) The reason I didn’t like the goal thing so much was because I already have my Fitbit connected to my phone. So I don’t really need another one. But I do think the information library is invaluable because my pain is dreadful, and my sleep is dreadful (Person with musculoskeletal disorder, P6)
Most favoured and least preferred intervention components (n = 6).
Recommendations included prioritising app development over the website and incorporating a variety of goal templates, alongside a ‘Create your own’ option. Integrating a Chatbot with the ‘contact your physiotherapist’ function was also suggested to address general queries. Now I'm not suggesting that… we take our medical advice from a BOT, but there will be aspects of this like general information…that may well be very suitable for chat BOT (Person with musculoskeletal disorder, P5)
Setting clear support forum rules and implementing some form of moderation were also advised. I know just from my only experience ….they have it very clear….what will and won't be accepted and you sign up to that. And I have seen posts being removed and people being removed from the groups. So if you go down this route, there might be a need for some monitoring (Person with musculoskeletal disorder, P1)
The second focus group (n = 6) proposed several enhancements to improve accessibility and usability. These included using more ‘icons, images’ (Person with musculoskeletal disorder, P7) with less text, adding a section on Pain Acceptance and offering content suggestions for the ‘Understanding Pain’, ‘Pacing’ and ‘Self-management Support’ sections. They also recommended changing the colour scheme and enabling users to add qualitative information within the goal-tracking feature to provide context, especially when goals are unmet. Maybe a feature here….say Tuesday the 10th was a particularly bad day and just being able to input a bit of qualitative information….so that there's more of a context around that. (Person with musculoskeletal disorder, P12)
Furthermore, they suggested that posts within the support forum should have a saving or ‘pinning’ feature for users. Useful as well as some mechanism to kind of pin or save a post or a thread that you’d find particularly useful. Because…get lost in the ether after a while (Person with musculoskeletal disorder, P8)
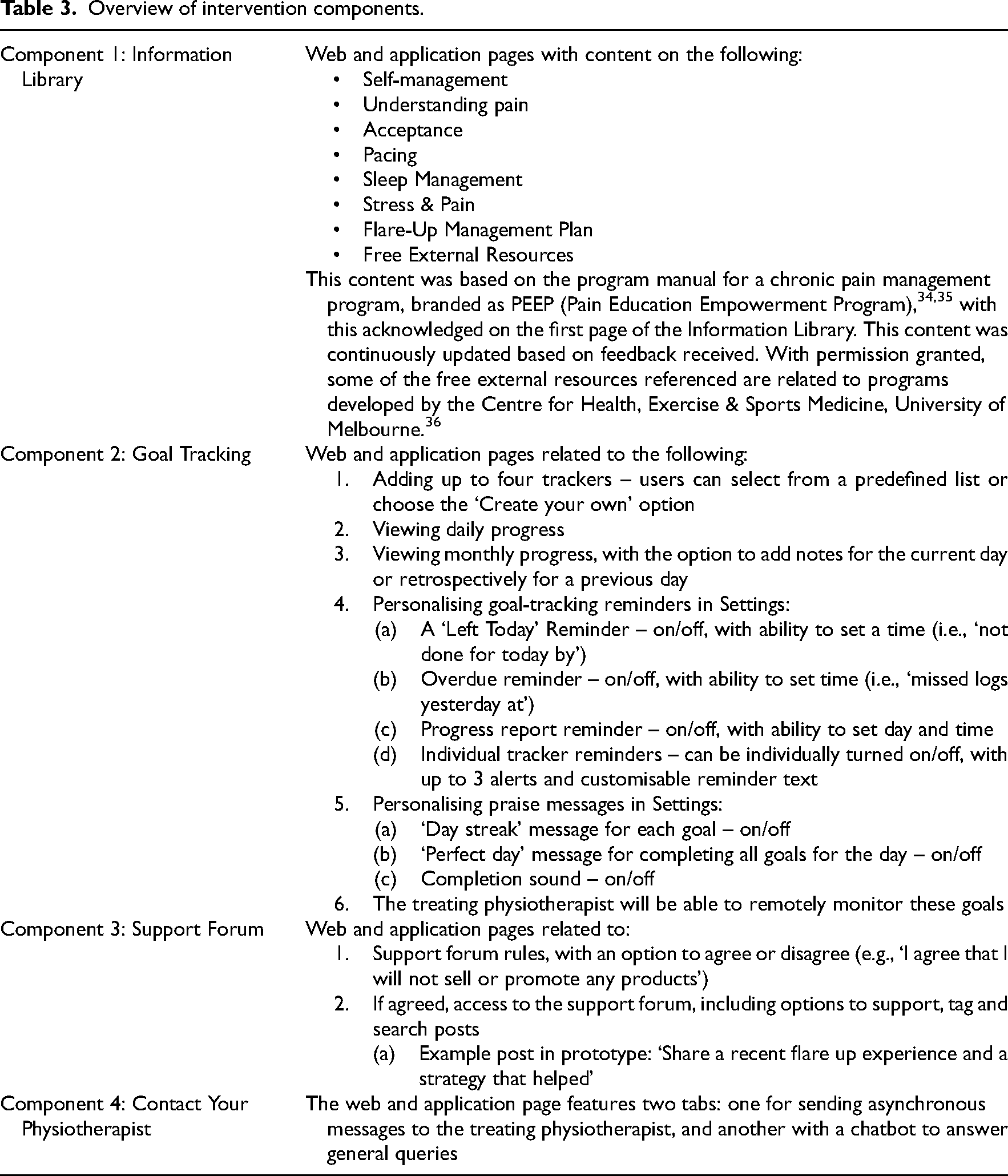
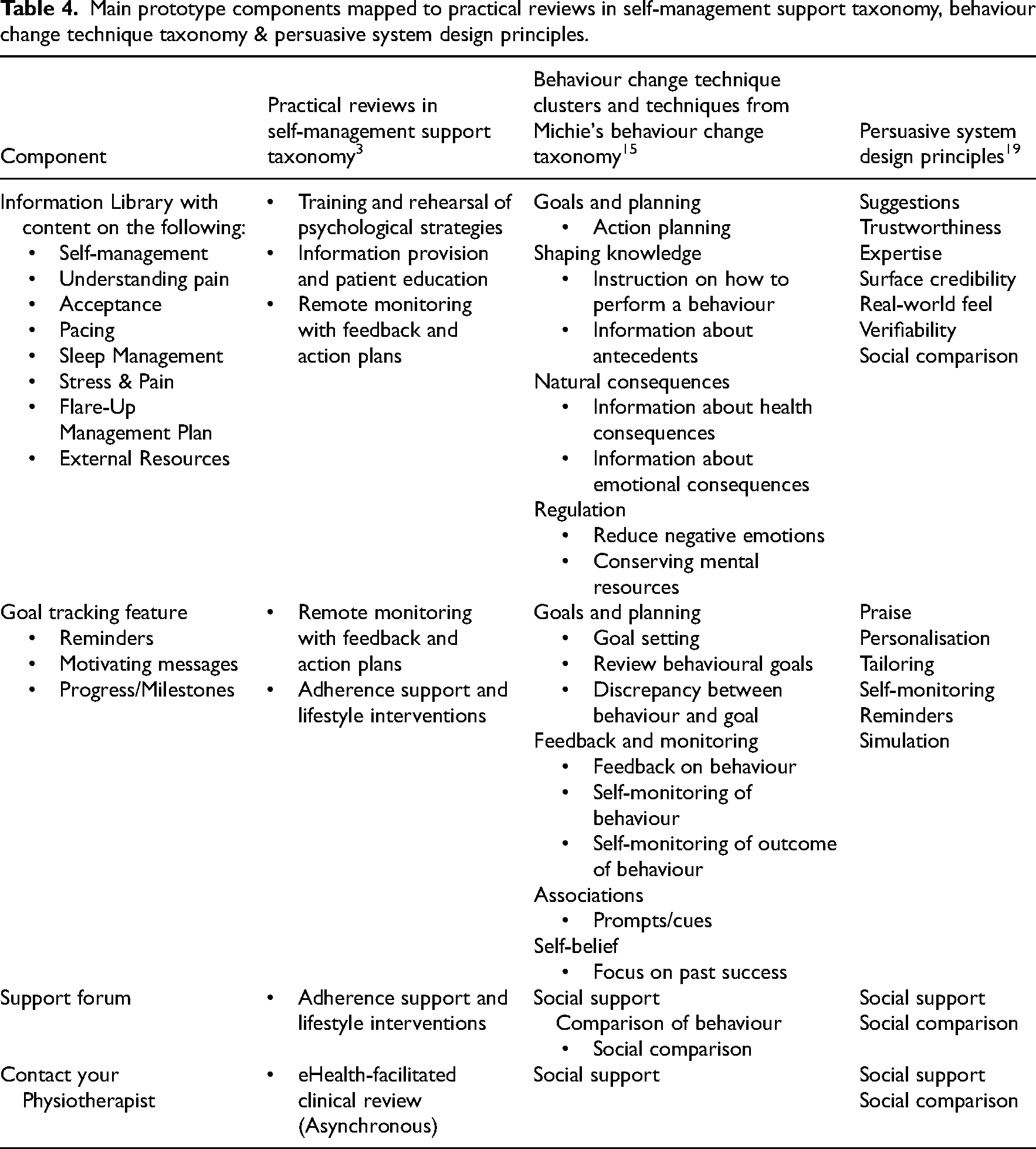
The four approved components are outlined in Table 3 and map to the Practical Reviews in Self-Management Support Taxonomy, 3 behaviour change techniques 15 and persuasive system design principles 19 (Table 4).
Overview of intervention components.
Main prototype components mapped to practical reviews in self-management support taxonomy, behaviour change technique taxonomy & persuasive system design principles.
Step 2: Heuristic testing
At the consensus meeting, an agreement was reached that the main issues to be addressed before usability testing were: (1) the addition of a mission statement highlighting that the intervention is to be used alongside physiotherapy, (2) error prevention (i.e., able to go backwards/cancel), (3) design and (4) consistency across the intervention concerning how users interact with the intervention. Examples of changes implemented include the introduction of more colour with the font changed to improve the overall aesthetics of the prototype.
Step 3: Usability testing
Ten participant interviews [people with musculoskeletal disorders (n = 5), and musculoskeletal physiotherapists (n = 5)] were conducted (Tables 5 and 6).
Step 3 – People with musculoskeletal disorders (n = 5).

IQR: interquartile range; eHEALS: eHealth Literacy Scale.
* eHealth Literacy Scale (0–40); higher scores indicate better self-perceived eHealth literacy. 33
Step 3 – Musculoskeletal physiotherapists (n = 5).
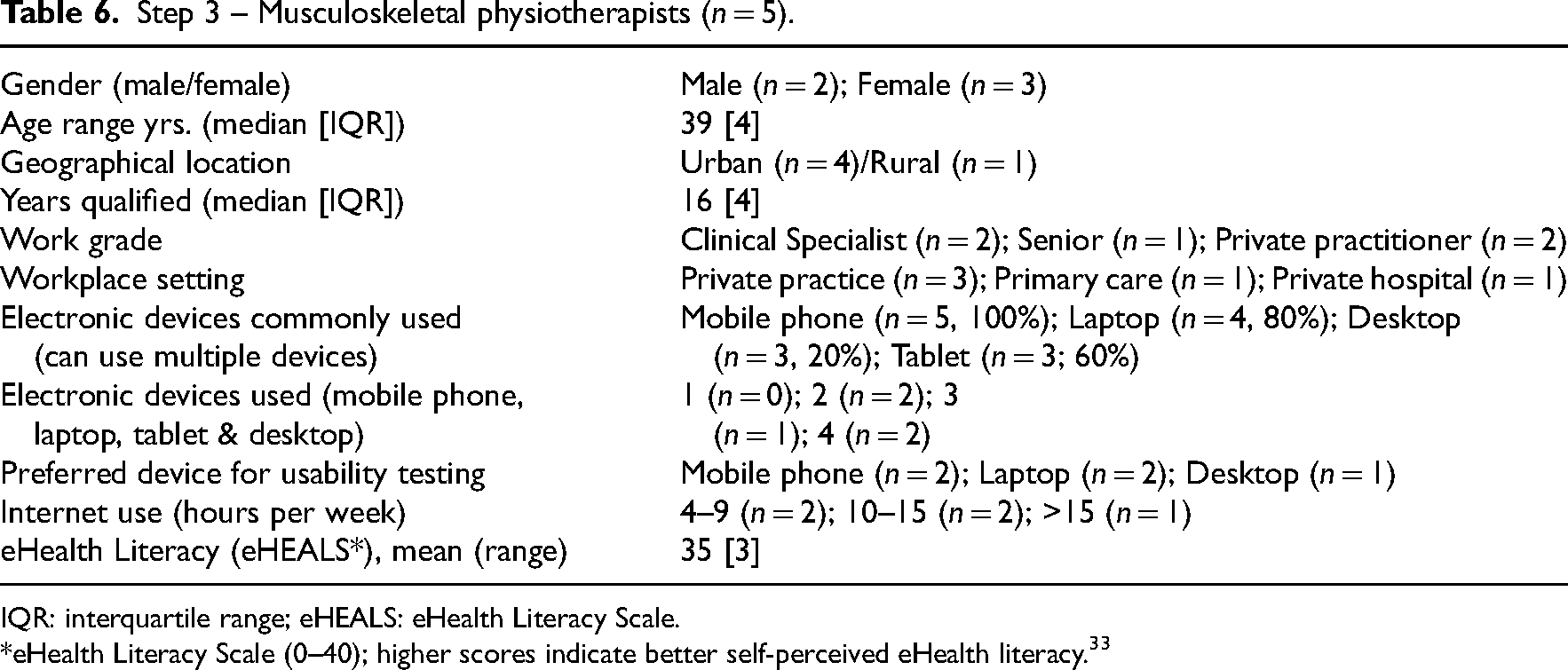
IQR: interquartile range; eHEALS: eHealth Literacy Scale.
*eHealth Literacy Scale (0–40); higher scores indicate better self-perceived eHealth literacy. 33
Similar responses were noted among the participants concerning the prototype's content, navigation and design. All people with a musculoskeletal disorder were female with the majority (80%, n = 4/5) reporting widespread musculoskeletal symptoms. The musculoskeletal physiotherapists were experienced clinicians with a minimum of 14 years qualified, with the majority (80%, n = 4/5) working in the private healthcare setting.
The qualitative data from the usability testing was categorised into three predefined categories: navigation, content and design. A navigation-related recommendation was to use pop-up messages within the application to inform users when they are directed to resources outside the app. If they get a bit lost if they start clicking a back button and they can’t get back to the app. As long as they know that it's opening in a different section (Physiotherapist, PA)
Regarding content, users suggested that the ‘Flare-Up Plan Template’ be editable and saveable within the application or website. A lot of the time when you’re in severe pain you can’t think properly…..that they have it all in one place yeah (Person with musculoskeletal disorder, P15)
For design, there was a strong recommendation for the addition of a logo and consistent branding. The first thing is I don’t like the background and there's no logo… ….Branding experts can nail this (Physiotherapist, PC)
The overall median System Usability Scale score (interquartile range) was 75 (0) out of 100 for people with a musculoskeletal disorder and 77.5 (2.5) out of 100 for musculoskeletal physiotherapists, indicating usability was good. 37 System Usability Scale scores of 71.4, 85.5 and 90.9 correspond to overall usability ratings of ‘good’, ‘excellent’ and ‘best imaginable’, respectively. 37
Discussion
This study provides insight into a user-centred, systematic, multi-method approach for designing and developing a prototype for adults with musculoskeletal disorders. The prototype facilitates follow-up self-management support, integrating remote monitoring with the four main intervention components mapping to recognised behavioural change taxonomies. 16 Informed by the evidence-based Center for eHealth Research Roadmap, 20 this study provided an opportunity to clarify and build on the findings from the contextual inquiry 6 and value specification phases. 5 By employing a user-centred, iterative approach, the eHealth: It's TIME prototype is expected to demonstrate improved usability, greater user satisfaction and better clinical outcomes, compared to those developed using traditional methods. 38
This study details a three-step iterative co-design approach which contributes to the knowledge base on involving stakeholders effectively in the development process, with this knowledge gap considered a possible explanation for the lack of user involvement within the eHealth literature. 20 This study employed a multi-method approach, incorporating focus groups, think-aloud usability interviews, heuristic evaluation and the System Usability Scale, in line with recommendations, with these methods commonly occurring in the design phase of the Center for eHealth Research Roadmap. 12 By incorporating these diverse methods, the study aimed to achieve an optimal fit between the technology, stakeholders and context, thereby enhancing the potential uptake of the eHealth: It's TIME intervention in clinical practice. 12
Based on the preferences of people with musculoskeletal disorders and musculoskeletal physiotherapists, the eHealth: It's TIME prototype incorporates four main components: an information library, a goal-tracking feature, a support forum and a ‘contact your physiotherapist’ feature. This complex intervention includes all five eHealth-suitable components 6 of the Practical Reviews in Self-Management Support taxonomy. 3 While approximately 36.5% of eHealth-mediated self-management support interventions for people with musculoskeletal disorders included all five components, 6 to our knowledge, no systematic review has evaluated their effectiveness or impact within musculoskeletal healthcare. In other disease areas, no single component has been identified as ‘optimal’ or essential’, although consensus suggests that a range of components is necessary for significant improvements in disease self-management. 39
This study provides evidence supporting the use of recognised behaviour change taxonomies in the eHealth: It's TIME follow-up self-management prototype, aligning with the NICE evidence standards framework for digital health technology. 18 Although often not explicitly reported,14,16 these taxonomies are commonly employed during the design phase of the Center for eHealth Research Roadmap. 12 This approach aims to enhance self-efficacy, improve self-management skills and increase overall intervention effectiveness. 16 To achieve this and support sustained behaviour change, the Behaviour Change Technique taxonomy 15 and the Persuasive System Design model 19 were applied alongside the Practical Reviews in Self-Management Support taxonomy. 3 This application of behaviour change taxonomies is relatively novel in the musculoskeletal eHealth literature with getUBetter 40 being the only other example to our knowledge. This app incorporates 25 behaviour change techniques and several persuasive system design principles, with preliminary results indicating improved symptoms, disability and self-management ability. However, a large-scale randomised controlled trial with economic evaluation is necessary to confirm its effectiveness.
The challenges of poor uptake and implementation of eHealth interventions in clinical practice are widely acknowledged. 41 The principal strength of this study is the theory-informed, user-centred iterative design and development approach, which is expected to enhance future implementation. This study resulted in the development of a multicomponent eHealth-mediated self-management support follow-up prototype for people with musculoskeletal disorders. The aim is to improve long-term self-management support while minimising the demand on clinicians’ time, in line with stakeholder preferences. 5 Several limitations are acknowledged, with the homogeneity of the study population being foremost. Most people with musculoskeletal disorders were female, held higher degrees or professional qualifications and reported good levels of self-perceived eHealth literacy. Consequently, this sample likely does not represent the diversity of the future end-user population. The next step is to test the feasibility of the refined high-fidelity prototype within clinical practice. 22 Guidelines for evaluating the feasibility of recruitment of diverse populations will be followed, 42 with interviews embedded within the trial design to gain insight into the participants’ overall experience utilising the prototype. A second study limitation is that the prototype is changing rapidly. Despite meeting the prioritised elements, the current version is relatively simple, with further development necessary.
The next step is to conduct a feasibility trial to acquire more information on feasibility, acceptability and preliminary efficacy to support self-management. This research will also analyse the perceived impact and actual usage (e.g., through log data analysis) of the different components to optimise and tailor the eHealth intervention. Following this, a large-scale randomised control trial will evaluate the long-term effectiveness and economic impact of the eHealth intervention.6,17 The trial will include a process evaluation to explore whether the identified intervention components, behaviour change techniques and persuasive system design principles contribute to facilitating sustainable behaviour change and self-management. 17
Based on end-user preferences and utilising a systematic iterative process, an eHealth-mediated follow-up self-management support prototype has been developed for people with musculoskeletal disorders. The next phase of the project involves testing the feasibility of this prototype within clinical practice, utilising a diverse population.
Clinical messages
There is a need for more effective self-management interventions for musculoskeletal disorders, with growing interest in the role of eHealth.
It is recommended that individuals with musculoskeletal disorders be actively involved in the development of eHealth interventions, which should be grounded in theory.
A new eHealth-mediated self-management support intervention is being co-developed with patients, based on theory.
Four main components to support self-management have been identified: an information library, goal-tracking, a support forum and a ‘contact your physiotherapist’ feature. These have been included in the prototype intervention.
Supplemental Material
sj-docx-1-cre-10.1177_02692155241289097 - Supplemental material for Design and development of an eHealth intervention to support self-management in people with musculoskeletal disorders: ‘eHealth: it's TIME’
Supplemental material, sj-docx-1-cre-10.1177_02692155241289097 for Design and development of an eHealth intervention to support self-management in people with musculoskeletal disorders: ‘eHealth: it's TIME’ by Marie Kelly, Brona M. Fullen, Denis Martin, Colin Bradley, Eoghan O’Riain and Joseph G McVeigh in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors would like to thank Katharine Beaumont and Jonathan Leahy Maharaj for their assistance with the heuristic testing and all those who participated in the study.
Author contributions
MK: Conceptualisation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project Administration, Writing – Original Draft Preparation, Writing – Review & Editing; BF: Conceptualisation, Formal Analysis, Investigation, Methodology, Supervision, Writing – Review & Editing; DM: Conceptualisation, Formal Analysis, Investigation, Methodology, Supervision, Writing – Review & Editing; CB: Conceptualisation, Formal Analysis, Investigation, Methodology, Supervision, Writing – Review & Editing; Eoghan O’Riain: Software, Writing – Review & Editing; JGM: Conceptualisation, Formal Analysis, Investigation, Methodology, Supervision, Writing – Review & Editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Granted by the Clinical Research Ethics Committee (CREC) of the Cork Teaching Hospitals (REF: ECM 4 (f) 20/09/2022).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MK was supported by a research bursary from the Chartered Physiotherapists in Musculoskeletal Therapy (CPMT), a clinical interest group of the Irish Society of Chartered Physiotherapists (ISCP).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.