
Abstract
Objective
The assessment of mood after brain injury is more challenging when people have ongoing severe cognitive and receptive communication impairments. There is no gold standard on how these assessments should be undertaken. This study aimed to reach a consensus on this among specialists working with this population.
Design
Focus groups were completed using a structured nominal group technique. Groups were compared for overlapping themes and agreed processes.
Participants
Five focus groups with a total of 14 participants who work with the population of interest were completed. Participants included 12 clinical psychologists, one psychiatrist and one consultant in rehabilitation medicine.
Results
Each of the five groups reached a consensus on a process for assessing mood in this population. Results overlapped and were combined into a proposed circular and iterative model of assessment that includes: (pre) information gathering, (peri) assessment processes, and (post) treatment; with formulation being seen as a vital part of the process. Standardised measures were not recommended for use with this population. Beyond the consensus processes, three implicit themes were identified: (1) depression is different after severe brain injury, (2) overlapping tasks and roles, and (3) looking at the bigger picture.
Conclusions
A good level of consensus was achieved across the five groups on processes to follow when assessing mood when people have ongoing cognitive and receptive communication impairments after severe brain injury. We recommend that this formulation-based model be followed when assessing people in this clinical population.
Introduction
Brain damage due to traumatic events (e.g. falls, car accidents, and assaults), infection, strokes or hypoxia (e.g. following cardiac arrest), is a growing cause of hospitalizations and disability. 1 Cognitive impairment is a common consequence of brain injury and is related to worse health-related quality of life. 2 Additionally, distress, low mood, and depression are common following acquired brain injuries.3,4 Several UK national clinical guidelines provide advice on screening for the presence of mood disorders following acquired brain injury (ABI).5–9 When patients have persisting severe cognitive and receptive communication impairments after brain injury, these assessments can be complex as patients may be unable to participate in clinical interviews and mood measures may be challenging to administer. The overlap of the common cognitive and physical consequences of an ABI and the symptoms of depression increases the challenge to identify the presence of mood difficulties and distinguish them from other cognitive, physical or emotional consequences of brain injury. This makes observer-rated assessment scales more challenging to use. A previous systematic review by the authors 10 found that no self-report measures had been demonstrated to be valid for this population, and only two observer-rating scales could cautiously be recommended for use with this population (the Stroke Aphasia Depression Scale and the Aphasia Rating Depression Scale). 10
There is no consensus or gold standard on how mood should be assessed in this patient population. Studies completed by the authors, including a survey study (in peer review) and semi-structured interviews 11 with clinical psychologists and medical professionals working with this population, showed some overlap in processes being used but no consensus.
Given the complexity of this patient population and the continued difficulty with the lack of a consensus or gold standard approach to assessment, it would be beneficial if experts assessing mood in the field (such as medical professionals and clinical psychologists) could establish a consensus on the best way to approach this issue.
In this study, focus groups were used with the aim of obtaining a consensus on how to assess mood in people with persisting severe cognitive and receptive communication impairments after severe brain injury that precludes the use of routine mood measures.
Method
Ethics approval was granted by the University of Glasgow College of Medical, Veterinary and Life Sciences Ethics Committee for Non-Clinical Research Involving Human Participants (application 200210142).
Purposive sampling was employed by contacting specialists working with this population who had consented to further involvement in previous studies completed by the authors. Forty-nine respondents in the previous studies provided email addresses indicating a willingness to be contacted about future studies. Given the specialist nature of the population and the small number of clinicians with substantial experience in this area of work, it was envisaged that four to five focus groups of three to six participants would be completed. Small numbers within the focus group would permit more time for all participants to expand on their views and provide richer detail. Participants were contacted via email and were additionally encouraged to forward the invitation for the focus group to other appropriate specialist clinical psychologists and/or medical professionals they work with. Participants were not paid to participate in the focus groups. As participants were from across the UK, focus groups were undertaken using an online platform (Zoom), and a voice recorder application (Recorder App for Android) was used for recording and transcription.
The nominal group technique (NGT) was used, which is a structured method that encourages each focus group member to contribute individually and allows the group to make decisions on issues and their relative importance by each individual voting on what they view to be most important and ranking items as a group.12–15 This technique involves five steps: introduction, silent generation of ideas, listing ideas, discussion and ranking (see Supplemental Table 1 for details on each step).
Data analysis
Each group was transcribed and transcriptions were used for two levels of analysis: content analysis and thematic analysis. Data was compared across the NGT groups (as opposed to only reviewing the most prevalent content).15 Content analysis included listing the assessment process suggested by the group as well as frequency and prevalence across all groups. Thematic analysis was used to label explicit and implicit themes not captured by the assessment process suggested by the group. An adapted approach to the analysis of NGT group data was used to report on the rankings provided by each group.15
The themes of each group were analysed using reflexive thematic analysis.16–18 The principal researcher (AR) developed the themes by engaging with the data and thus brought their own experience, training and views into the analysis as an experienced qualified clinical psychologist. A constructionist epistemological view of the data was adopted and meaning and understanding were viewed to be constructed subjectively and intersubjectively and within a specific context16,17 Data was coded and analysed using an inductive approach, working with the data from the bottom-up.18
A six-stage approach to completing thematic analysis was used: familiarisation; coding; generating initial themes; reviewing and developing themes; refining, defining and naming themes; and writing up.16,17 This process is not linear and the expectation is that the researcher would need to revisit and review data multiple times. Themes and subthemes were created, with coded extracts of the transcriptions under each. The codes were collated into common ideas expressed by participants in order to identify how these themes related to each other.
The Consolidated Criteria for Reporting Qualitative Studies (COREQ) guidance and checklist were used to guide the reporting of the focus group results.19
Results
Emails were sent to the 49 available email addresses. A total of 18 responses were received to participate in the focus groups. Four of the respondents dropped out on short notice and were unable to reschedule. Five groups were held with two to four participants per group, totalling 14 participants. The participants were deliberately mixed according to their professional level and experience to create disparate groups in order to avoid bias in line with professional training and experience. Only the group members and the principal researcher (AR) were present and no repeat groups were held. All focus group participants were qualified professionals; 12 were clinical psychologists and two were medical professionals (one rehabilitation consultant and one psychiatrist). Only one participant (the psychiatrist) had less than two years of experience with the population of interest. The remaining 13 participants currently worked, or previously worked, in specialist units for those with severe brain injury. The groups took place between 14 July and 11 August 2022 and results were analysed and reported as part of the principal investigator's PhD.
All five groups reached a consensus on a process that should be followed when persisting cognitive and receptive communication impairments are present following severe brain injury (see the Supplemental materials for details of individual focus group results). The consensus views from the five groups all had similar approaches that can loosely be viewed as information gathering (pre), assessment processes (peri) and treatment (post), with formulation being seen as a vital part of the process. Themes and methods overlapped between the five groups and fewer themes were generated as groups progressed, with no new themes being labelled in focus group five that had not already been identified in the first four groups. The overlapping processes across the five groups allowed for a combined model to be suggested. When looking at the most popular methods mentioned in the groups, these were observation, formulation and bespoke creative assessment (see Supplemental Table 1 for frequency of assessment processes across groups).
Across the five focus groups, three themes were labelled that were not specific assessment processes but were relevant to the assessment process. The first theme was labelled as ‘Depression after severe ABI is different’: All the groups discussed the construct of depression and whether this is different when a person has suffered a severe ABI. Within this theme, the issues of how other non-mood-related symptoms of the brain injury may obscure mood symptoms were discussed (such as appetite and sleep disturbances being caused by the brain injury or associated physical sequelae and cognition obscuring issues with apathy and concentration). It was also frequently raised whether the construct of depression as it is understood by psychology and psychiatry is relevant after a severe ABI. P1.4: ‘The other question that's really important to ask is about cognitive function and whether somebody actually has enough of a cognitive function to be able to experience a mood disorder, whether we need to think of it in a totally different way’ … ‘we think of depression in, and we think of measuring depression in terms of getting numbers out of questionnaires, which clearly isn't appropriate with this group of people. But that's how, often, many of our colleagues in other professions do think about this. And they're not asking the same questions about whether the construct needs to be changed, and I think we should consider that’. P5.3: ‘There's just lots of features of the brain injury, that mean you have to kind of think differently about the sort of construct of what depression is’ … ‘So it's important for people to be aware of the issues, that's probably what the main issue is, is that people aren't aware of the issues’. P3.2: ‘I'd also talked about the abstract nature of the mood measures. So the actual sort of statements that they may include, or some of the most simple ones, were there sort of Likert scales or DISCS or things like that, it would require somebody to have sort of adequate visual processing skills and be able to kind of extract meaning from some of these symbols… which requires a high level of cognitive function, which is likely to be rare amongst a severe ABI population’. P1.4: ‘Because we're all psychologists (group 1 was comprised of only psychologists) but this is not how it works out in normal life, because who owns the mood issue? …In some areas, you're going to be working with psychiatrists and in other areas, you're going to be working with neurologists. And sometimes you've got everybody and their dog involved in this, and everybody's got an opinion. I think one of the most difficult things isn't it doing this bit. It's actually managing all the other people who are involved…’ P1.3: ‘Trying to talk about suicide with somebody who has like very limited language is incredibly difficult, because there's not a great way of making clear what you're asking somebody if you're showing them a picture that's supposed to reflect that. And so it just becomes a really difficult issue’. P5.2: ‘And, you know, that idea of not making assumptions that … just because someone's crying, or they don't fancy their physio session one day means that they're, you know, depressed, it might mean something else’.
In order to summarise the methods suggested across all five groups, and using the top 10 methods reported, a combined visual representation of the suggested method to assess mood in people with severe cognitive and receptive communication impairments was created (see Figure 1 below). This shows the various sources of information to consider before the assessment (Pre), methods to use to assess mood in patients with severe cognitive impairments (Peri) and the overall approach to assessment (separate box, top right), the prominence of the formulation (represented with an arrow and dotted circular shape) and the treatment options (Post). It also includes the caveat that immediate response may be required to manage acute distress (separate box, bottom left) and considerations of the assessor that must be considered when assessing this population (separate box, top left). These considerations refer to the need for there to be specialist neuro experience, and to be aware of bias and possible projections of the assessor's emotions or awareness of others projecting their emotions and experience onto the patient.
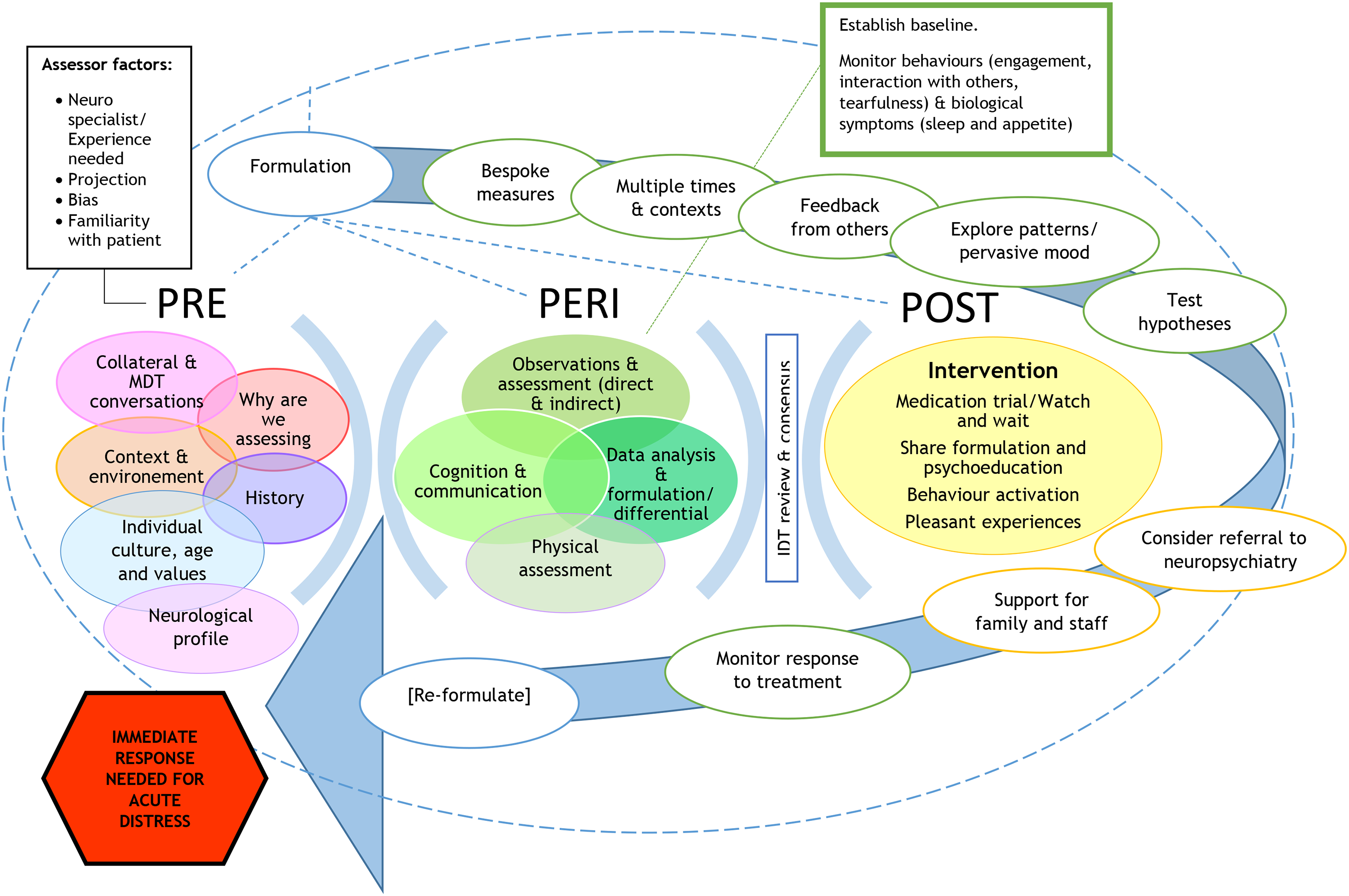
Combined model of the assessment of mood after severe ABI based on data from five professional focus groups.
Discussion
There is no gold standard method of assessment when a person has persisting cognitive and receptive communication difficulties after severe brain injury. Usual methods of assessment, such as clinical interviews and the use of standardised mood measures, are challenging due to the difficulties the person will have with self-reporting. Collateral information is often relied upon, but symptoms of the brain injury may overlap with symptoms of low mood, making it easy to misunderstand and affecting the collateral information. Current guidelines4–9 provide guidance on how to assess mood after brain injury, however, they are not specific about how to assess mood when cognition is severely impaired and they do not capture the complexity of this process. This study consisted of structured focus groups, used to enable experienced professionals in the field to express their views on how assessment should be approached in this population.
The NGT was used to explore views on the methods of assessment and to facilitate working towards a consensus. The method allows all group members to express their ideas. However, it is noted that some data that would naturally arise in conversations may be missed. The traditional NGT procedure involves ranking the ideas generated in order of priority, but in this study, the participants felt unable to do so as they felt it was an overlapping process. The NGT allows the comparison of data across groups, which was useful in this study to identify overlapping methods and processes of assessment. Thematic analysis16–18 allowed for analysis of some of the complexities of mood assessment and the nuanced issues raised by participants.
Participants suggested that the use of standardised mood measures is not recommended in this population. The formulation process agreed upon in each group mirrors approaches taught to clinicians such as clinical psychologists, psychiatrists and other medical professionals. Although this overlap of understanding between professional groups is helpful, training differences between professions create slightly different views and approaches to formulation. In a study exploring psychiatrists’ views on formulation,20 it was found that psychiatrists viewed formulation as contingent on how they were trained and that they prioritised diagnosis and medication. Additionally, some of the psychiatrists that participated in that study20 did not feel psychological understanding was necessary due to difficulties being viewed as purely biological in nature at times. This finding is in opposition to the views of the participants in this study, who emphasised their focus on formulation to understand and not to diagnose. These different views on formulation add to the explanation of how clinicians assessing and treating a patient may still differ in opinion despite sharing the same formulation. The emphasis on multiple processes, including frequent observations/monitoring, highlights the importance of training for frontline staff, particularly nurses, to ensure good knowledge of the formulation process. All members of the multidisciplinary team need to be aware of the key role that they can play in contributing information to build the formulation for each patient.
Beyond the consensus themes on the process of assessment, three additional themes were identified; ‘Depression is different after severe acquired brain injury (ABI)’ refers to discussions amongst professionals that the presentation of symptoms and the construct of depression in people with cognitive and receptive communication impairments after severe brain injury is different to how depression is thought of in people with mild to moderate brain injuries. This view is of relevance to clinicians working with this population and further research into the symptom presentation and theories of depression after brain injury when severe cognitive and receptive communication impairments are present would benefit the understanding and assessment of mood in this population. The second theme, ‘Overlapping tasks and roles’, sheds light on the complex nature of the assessment process, how the consensuses were reached, and how this was challenging when attempts were made to prioritise tasks (as the participants felt all the tasks were important). The third theme, ‘Consider the bigger picture’, adds to the context of assessing mood difficulties and the complexities that can arise. These additional complexities strengthen the argument that a gold standard would benefit this population and that current guidelines are likely not fit for purpose for this population.
In terms of limitations, this study had a small number of participants (specifically medical professionals) which may limit the extent of its generalisability. Additionally, as participants have worked together or in similar settings, there is a risk of bias towards a similar way of conceptualising without sufficient critical appraisal (i.e. groupthink). The NGT was used to try to control groupthink and enable individual expression as much as possible. It is promising that the themes were overlapping despite this, including within mixed groups where medical professionals were present. In the absence of a gold standard, it is useful to have consensus from different professionals working in the field on how this issue should be approached. The participants had direct relevant experience and expertise working with this population and it was encouraging to see similar results arising within each group. It would have been beneficial to have had a better balance between clinical psychologists and medical professionals; however, it remained encouraging that agreement was reached. Further research is needed to include the views of others who are involved in assessing mood in patients following brain injury (such as nurses and other multidisciplinary team members).
When considering the complexity of assessment of mood in those with severe cognitive and receptive communication impairments after brain injury, self-report measures cannot be recommended 10 and professionals should consider a separate process of assessment for this population. This study's consensus-based formulation model, developed via focus groups with experienced professionals, provides guidance on how mood should be assessed in this population and further progresses the complex issue of accuracy in assessing and addressing issues with mood when severe cognitive and receptive communication impairments are present.
Supplemental Material
sj-docx-1-cre-10.1177_02692155241287770 - Supplemental material for Working towards consensus on the assessment of mood after severe acquired brain injury: Focus groups with UK-based professionals
Supplemental material, sj-docx-1-cre-10.1177_02692155241287770 for Working towards consensus on the assessment of mood after severe acquired brain injury: Focus groups with UK-based professionals by Alexandra E Rose, Breda Cullen, Sarah Crawford and Jonathan J Evans in Clinical Rehabilitation
Supplemental Material
sj-pdf-2-cre-10.1177_02692155241287770 - Supplemental material for Working towards consensus on the assessment of mood after severe acquired brain injury: Focus groups with UK-based professionals
Supplemental material, sj-pdf-2-cre-10.1177_02692155241287770 for Working towards consensus on the assessment of mood after severe acquired brain injury: Focus groups with UK-based professionals by Alexandra E Rose, Breda Cullen, Sarah Crawford and Jonathan J Evans in Clinical Rehabilitation
Footnotes
Author contributions
Alexandra E. Rose: Conceptualisation, design, data collection, data extraction, writing-original draft preparation, editing and final review of manuscript; Breda Cullen: Visualisation, design, final review of manuscript and supervision; Sarah Crawford: Visualisation, design, data reviewing as second reviewer, editing, final review of manuscript and supervision; Jonathan J. Evans: Visualisation, design, manuscript reviewing, final editing and review of manuscript, and supervision.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Alexandra E. Rose has received funding from the Francis and Augustus Newman Foundation as part of her PhD fellowship with the Royal Hospital for Neuro-disability.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.