
Abstract
Objective
To describe the theoretical development and structure of an occupation-based intervention for people with a surgically repaired distal radius fracture.
Intervention development and rationale
The Early Daily Activity (EDA) intervention uses the performance of strategically selected daily activities as the primary rehabilitative strategy. Occupation-based interventions are recommended for hand injury rehabilitation but are often poorly described and lack explicit theoretical underpinnings. The EDA-intervention was developed from exploratory research that informed the theory and structure. The theoretical principles are that daily activity performance is (i) safe within defined parameters (ii) appropriately self-determined (iii) produces high ranges and amounts of therapeutic movement, and (iv) builds psychosocial competencies.
Intervention description
The EDA-intervention is designed to be commenced within 2 weeks of surgery. There are three key components. The first is activity-specific education to emphasise the safety, benefits, and therapeutic actions of activity performance. A set of parameters for defining safe activities is described to support education. The second component is patient–therapist collaboration to select a range of daily activities that provide a ‘just-right’ challenge. Collaboration occurs at regular intervals throughout the rehabilitation period to incrementally increase the challenge of activities. The third component is performance of activities at-home targeted at improving range of movement and function.
Next steps
The EDA-intervention can be used by hand therapists, but it has not yet undergone effectiveness evaluation. A planned study will explore clinician readiness to adopt the EDA-intervention, inform iterative changes to the protocol and the design of feasibility and effectiveness studies.
Keywords
Background
After surgical repair of a distal radius fracture, the traditional rehabilitation approach to restore movement and function to the affected wrist is exercise-based. In this approach, range of motion exercises are performed at regular intervals throughout the day using prescribed numbers of repetitions.1,2 An alternative rehabilitation approach is occupation-based, where a range of daily activities are performed as the primary strategy for remediating wrist and hand stiffness and for improving function.3–5
Occupation refers to broad categories of daily life activities such as work, leisure, self-care, and social participation, whereas purposeful activities are components of occupations.6,7 An occupation-based intervention is one that uses purposeful activity or occupation as the primary therapeutic agent for facilitating change. 4
Occupation-based interventions are gaining attention in hand injury rehabilitation literature. Hand therapists are increasingly being challenged to move away from medically focused models towards functional, occupation-driven rehabilitation.5,8–10 Evidence is emerging demonstrating the effectiveness of occupation-based interventions in hand rehabilitation with respect to range of motion, function, satisfaction, psychosocial wellbeing, and perceived benefits.8,11–15
Despite occupation-based interventions being advocated in hand therapy, there is a lack of theoretically informed, comprehensively described interventions. Postoperative protocols for surgically repaired distal radius fractures often give broad recommendations to perform light activities as tolerated, but fail to specify parameters for activity types, duration, or intensity.3,16,17 An occupation-based intervention that uses activity and occupation as the primary rehabilitative strategy for surgically repaired distal radius fractures, and that specifies activity parameters is not known to exist.
In response to the lack of an evidenced, occupation-based intervention we developed Early Daily Activity (EDA). The EDA-intervention provides a structured framework for how to use daily activities to facilitate return of wrist movement and function. The EDA-intervention is underpinned by robust theory and is detailed according to the Template for Intervention Description and Replication (TIDieR) framework.
The aim of this paper is to describe the theoretical and conceptual development of the EDA-intervention. The intervention is intended to be used by occupational and physiotherapists practising in the field of hand rehabilitation. The intervention has not yet undergone feasibility or effectiveness testing and the protocol will require future evaluation.
Intervention development
The Medical Research Council framework for the development of complex interventions was used to guide the development of the EDA-intervention and the Equator network ‘Guidance for reporting intervention development in health research’ (GUIDED) checklist was used to ensure comprehensive reporting (Supplementary file 1).18–20 The medical research framework identifies four phases of development that progress in a non-linear fashion from theory development to evaluation and implementation.19,20
This paper focuses on the first Medical Research Framework phases of theory development and defining of the intervention. Theoretical underpinnings are often poorly described in rehabilitation interventions. We therefore wished to make explicit the knowledge and research that informed the development and definition of the EDA-intervention.
A series of studies was undertaken to identify existing evidence and extend knowledge about how daily activities act to bring about improvements in wrist movement and function in the early weeks after surgery. Two systematic reviews explored (i) the influence of activity on motor performance and (ii) daily activity recommendations after surgical repair of a distal radius fracture.3,21 Two primary studies conducted in Auckland, New Zealand, explored the causal mechanisms of an occupation-based rehabilitative approach for people with a surgically repaired distal radius fracture.14,22 The key findings from these studies are summarised in Table 1. The findings from these studies are synthesised in this paper to articulate four principles which form the theoretical underpinnings of the EDA-intervention.
Summary of studies that informed the principles of EDA.
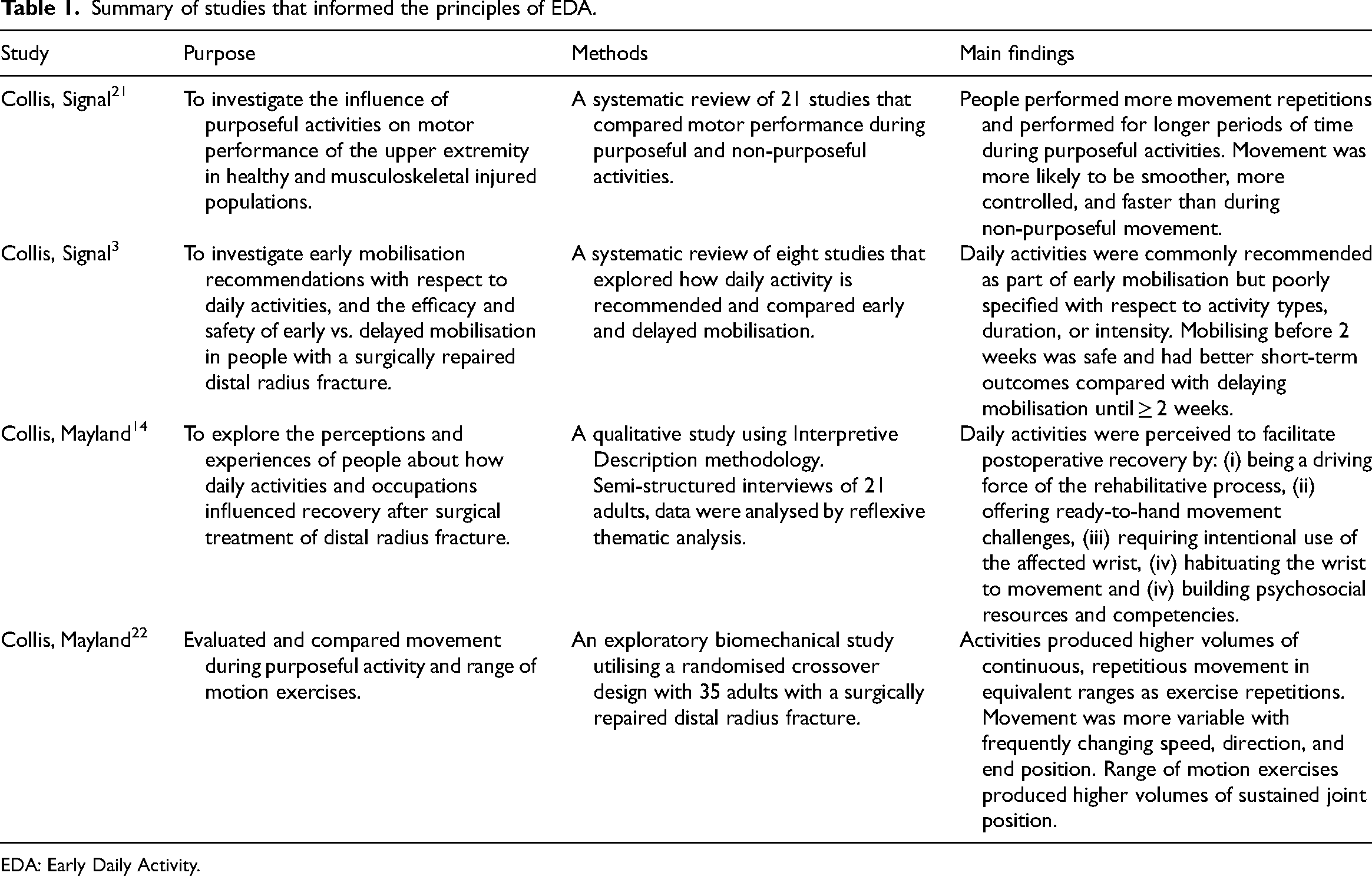
EDA: Early Daily Activity.
The structure of EDA is described using the TIDieR. 23 The TIDieR was developed in 2014 as an extension to the CONSORT 2010 24 and SPIRIT 2013 25 statements and is recommended for promoting replicability and accurate reporting of interventions. The TIDieR includes descriptions of intervention procedures, delivery, timing, dosage, tailoring, and evaluation of fidelity. 23
Intervention description using the TIDieR framework
Title: EDA-intervention
The name was chosen to highlight the safe performance of light daily activities after surgical repair of a distal radius fracture. Similar terms such as Early Active Mobilisation are commonly used in hand therapy to denote prescribed exercise regimes for fracture and tendon rehabilitation.26,27 The term EDA was specifically chosen as a related but different term which gives prominence to the use of activities and occupation as a rehabilitative strategy.
Why: Rationale
The EDA-intervention uses daily activities as the primary mechanism for producing wrist movement and enhancing psychosocial competencies. There is a deliberate move away from traditional models that focus on intermittent range of motion exercise and constraining of daily activities. Daily activities have been found to facilitate wrist movement beyond the scope of exercise routines alone and are considered a rich source of therapeutic movement quantity and quality. 22 The approach is consistent with evidence that questions the effectiveness of exercise regimens and advocates for early return to routine daily activities.16,17,28,29
The EDA-intervention is intended for rehabilitation after a surgically repaired distal radius fracture where the fixation is stable and early mobilisation (by 2 weeks postoperatively) is appropriate. Mobilisation and performing light daily activities within 2 weeks of surgery is considered safe for the majority of surgically repaired distal radius fractures, including in the elderly. 30 Early mobilisation has been shown to result in sooner return of range of motion and function than delaying mobilisation until 4 or 6 weeks.31–34
While performance of daily activities is the primary approach in the EDA-intervention, it is important to note that exercise routines and other therapy strategies such as oedema treatments, splinting, manual therapy, or desensitisation are used as needed to support rehabilitation. Similarly, surgeons and therapists will need to collaborate to determine whether the EDA-intervention is suitable for individual cases.
The EDA-intervention builds on the inherent capacity of patients to self-direct activity selection when supported by education that frames activity as safe and beneficial. The intervention is consistent with contemporary approaches for client-centred practice and shared decision-making. Such approaches empower patients to have greater agency in their rehabilitation.15,35 In the EDA-intervention shared decision-making is implicit because patients and therapists work together to negotiate and plan which activities will be used at each stage of rehabilitation.8,11
Why: Theoretical underpinnings
Principle One: Activity during early rehabilitation is safe within defined parameters
The first principle to underpin the EDA-intervention is that performance of light daily activities by 2 weeks after surgery without a wrist orthosis is safe. Systematic reviews and expert opinion show that commencing light daily activities by 2 weeks after surgery is commonly recommended and with complication rates similar to immobilisation.3,17,31 Biomechanical studies support early light loading of the operated wrist by consistently demonstrating the strength of volar locking plates in withstanding the forces of early mobilisation and active use.36–39
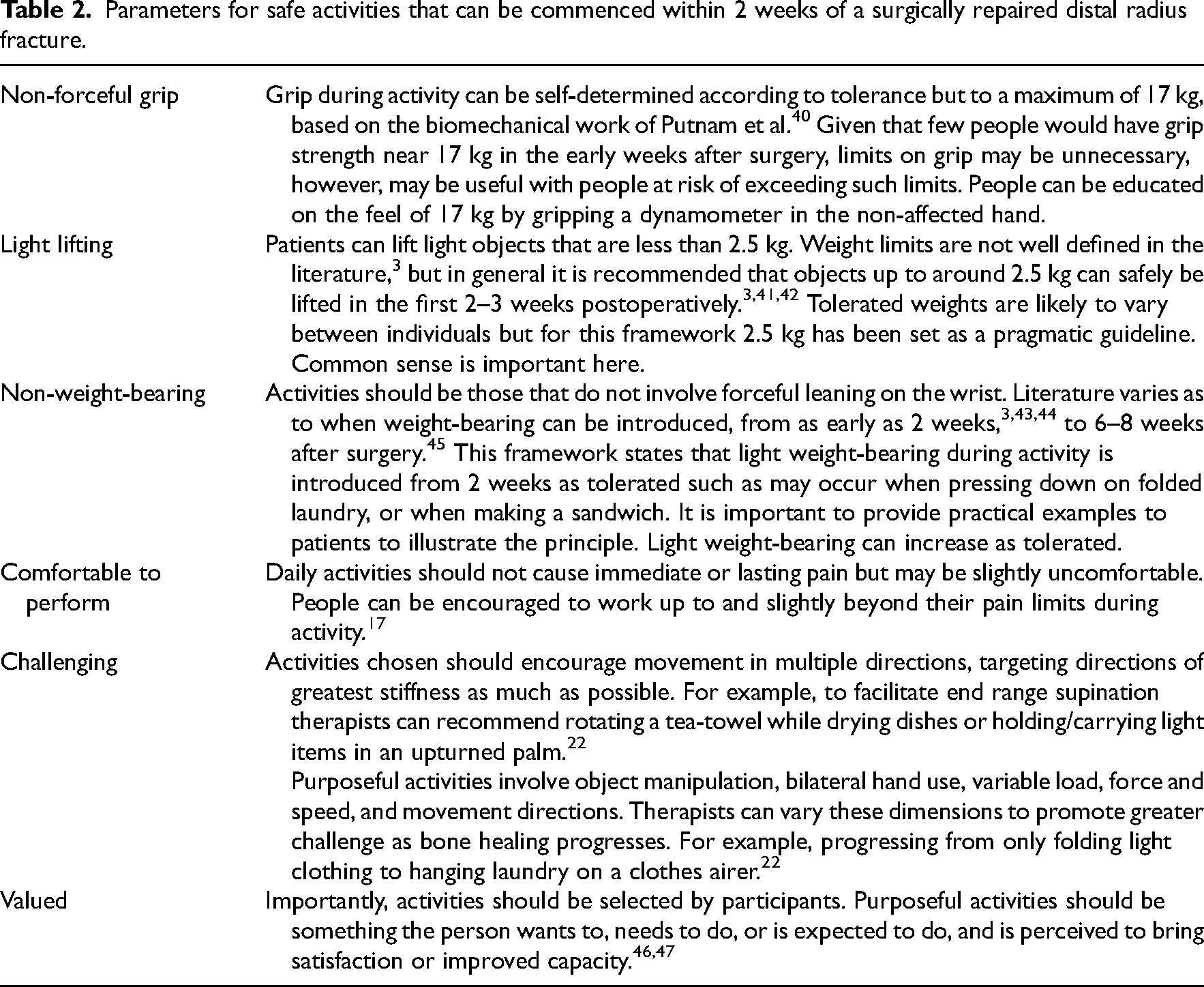
Due to the lack of a clear definition of what light activity means, we developed a set of parameters for safe activity. These parameters are intended to assist patients and therapists in deciding which activities can be safely commenced within 2 weeks of surgery. An activity should involve non-forceful grip, involve only light lifting, be non-weight-bearing, be comfortable to perform, provide appropriate challenge, and be valued. These parameters are detailed in Table 2.
Parameters for safe activities that can be commenced within 2 weeks of a surgically repaired distal radius fracture.
Principle Two: Activity during early rehabilitation is appropriately self-determined
The second principle of the EDA-intervention asserts that patients can be trusted to make decisions about types of appropriate daily activities. Despite recommendations for early commencement of daily activity, our clinical observations suggested that hand surgeons or therapists may distrust their patient's ability to modulate activity levels. Our research therefore explored how patients make decisions about which activities to perform without a wrist orthosis during the early weeks of rehabilitation. 14 Patient narratives illustrated that people use strategies such as pain thresholds, testing-out, and task analysis to select activities that challenge range of motion, without overloading healing bone. 14
We found that while participants were able to make safe decisions about performing light activities, many people were hindered by conflicting advice from their hand surgery and therapy team. Participants were often given contrary advice about whether to use their wrist without an orthosis. This led to fear of daily activity and slow progress with using the affected wrist. 14 For this reason, a key component of our intervention is clear and consistent education about active use of the hand and wrist without an orthosis. We recommend the use of occupationally positive language that frames daily activities as beneficial and an expected component of postoperative rehabilitation. In this context, people are able to make safe decisions about activity performance.
Principle Three: Activity produces high ranges and amounts of movement
The third principle that underpins the EDA-intervention is the potential of activity to deliver large doses of low-load movement during the early weeks of rehabilitation. Our research demonstrated that performing self-selected activities produced equal or greater volumes and ranges of wrist movement as exercise repetitions. 22 In a 10-min session, activity performance elicited over twice the amount of wrist movement time and numbers of flexion-extension repetitions as range of movement exercises. 22 Systematic reviews support the concept that activities produce more movement than during non-purposeful tasks.21,48 Equally, patients perceive activities to be an important source of wrist movement and report that the more they use their wrist without a wrist orthosis the more quickly range of motion and function return. 14 The EDA-intervention builds on the mechanism of activity in producing movement by using selected activities as the primary strategy for recovery of wrist range of motion rather than range of motion exercise repetitions.
Principle Four: Activity and occupation build psychosocial competencies
The role of occupation in potentiating motivation, building optimism and wellbeing, and reclaiming normality is the fourth principle of our intervention. Performing daily activities is highlighted as being beneficial for improving wellbeing and building psychosocial competencies, most notably optimism and alleviating feelings of loss and anxiety.14,15,49 Patients describe that the desire to return to valued occupations provided a source of positive energy to engage in rehabilitation after surgery.14,15,49 Additionally, achieving success with simple activities builds confidence in use of the wrist and for performing increasingly complex activities. 14
The EDA-intervention therefore strategically uses purposeful activities to build psychosocial competencies. In the intervention, we explicitly draw attention to the positive influence activity performance has on motivation, wellbeing, and optimism.
What: Procedures
The EDA-intervention involves three non-linear components that are part of an integrated whole and are outlined in Table 3:
1. Activity-specific education
Components of Early Daily Activity (EDA).
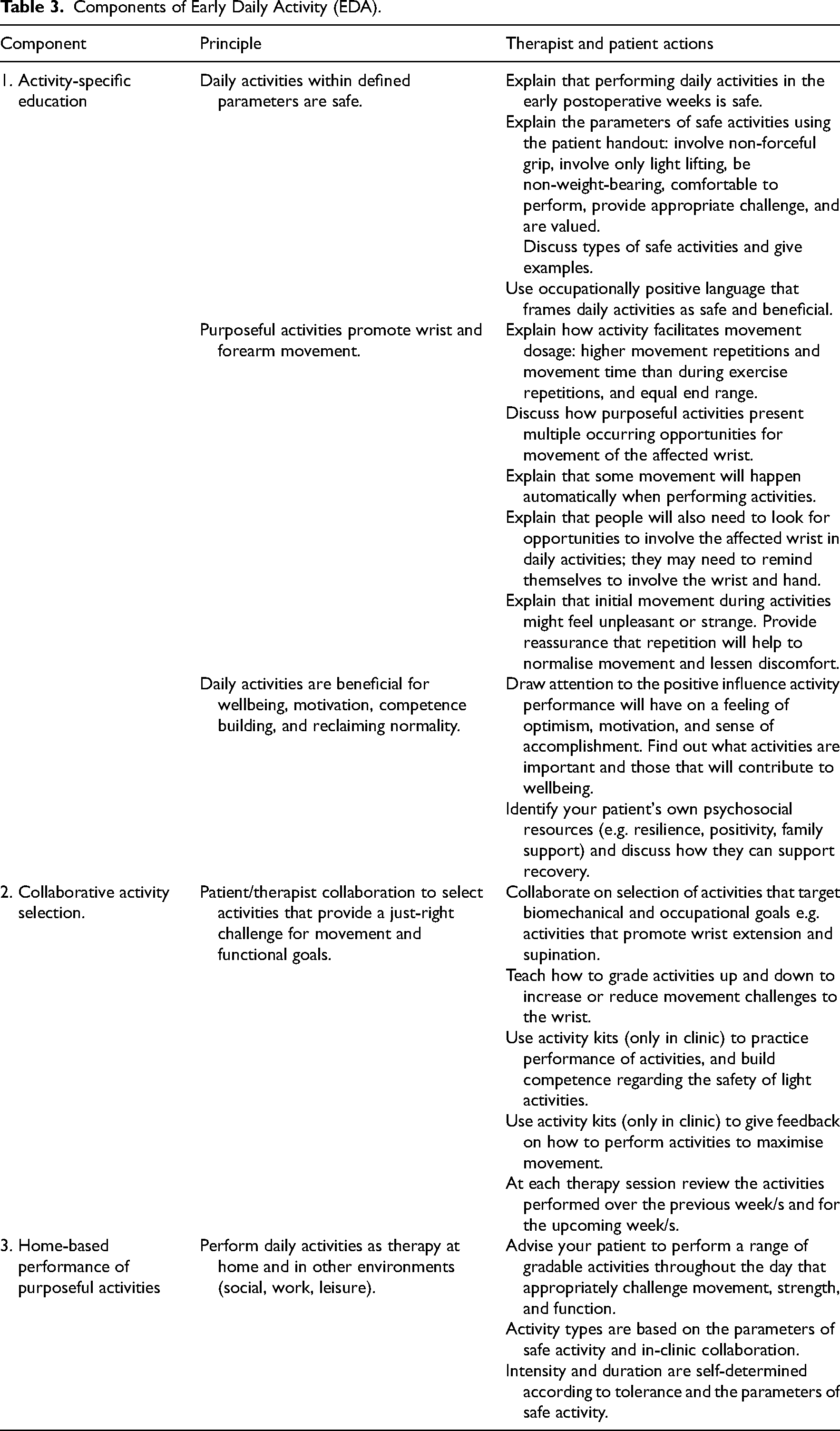
The first component is educative and designed to facilitate understanding of why daily activities are used, what constitutes light activity, and promote confidence in performing light daily activities. The therapist outlines the parameters of safe activity as in Table 2 and explains the rationale for performing daily activities as a rehabilitative strategy. Occupationally positive language is consistently used to avoid narratives of activities as potentially harmful.
2. Collaborative activity selection.
The second component is activity selection and practice with a hand therapist. The therapist and patient collaborate on selecting activities to be performed over the following week/s that target biomechanical and occupational goals and provide a ‘just-right’ challenge.4,50 Activities are then reviewed and modified at each therapy visit to provide appropriate movement and functional challenge.
In the clinic, therapists can prepare patients for the performance of activities at home through practicing simple activities. Clinics can assemble kits that contain a range of everyday items to facilitate such practice. Although performing authentic, self-selected activities is the primary goal in the EDA-intervention, such kits can be used as an adjunctive strategy. Alternatively, patients could bring in their own preferred activities to the clinic. Practicing activities in the clinic builds confidence, helps patients translate the use of activities as a therapy strategy to their own environments, and allows therapists to give feedback on how to maximise wrist movement during an activity.51,52 The use of such kits may be a particularly important strategy for patients who are anxious or uncertain about using their wrist without an orthosis.14,52 Suggested items for self-care, kitchen, and leisure kits are provided in Supplementary File 2.
3. Home-based performance of purposeful activities
The third component is performance by the patient of a breadth of activities throughout the day that appropriately challenge movement, strength, and function. The activities should be those that are meaningful to patients and occur naturally in the context of everyday life.46,47 Examples of activity types include light meal preparation, self-care activities (eating, grooming, washing, dressing), light household activities (hanging or folding laundry, putting away groceries, tidying, dusting, drying dishes, unloading a dishwasher), and leisure activities (care of indoor plants, handcrafts, electronic games, drawing, gardening).
What: Materials (provider, participant, and equipment)
Supporting materials include a patient education handout and suggested items for activity kits (Supplementary files 2 and 3). The patient education handout explains the intervention, outlines the parameters of safe activity, and illustrates types of suitable activities. The activity kits contain items and materials from everyday activities and were based on activities performed by participants in our studies in the early weeks of rehabilitation.14,22 The items are not prescriptive and should be assembled according to the cultural setting where they will be used. Similar kits that could be used to inform contents of an activity kit are described in other studies.12,53
Who provided (expertise, training needed)
The intervention is intended to be delivered by occupational therapists or physiotherapists with expertise in hand and upper-limb rehabilitation. Known as hand therapists, these individuals have undergone postgraduate training to acquire advanced knowledge and skills in the field of hand and upper-limb injury rehabilitation. 54
Although the intervention should be delivered by a therapist experienced in hand injury rehabilitation, it is important to recognise that the EDA-intervention must be endorsed by all members of the multidisciplinary team. Inconsistent or confusing advice about daily activities leads to anxiety and distress, whereas clear information that promotes engagement in meaningful activities is empowering during early rehabilitation.14,15,55 To adopt the EDA-intervention surgical and therapy teams will need to discuss which patients EDA will be used for, how language around daily activities needs to be modified, and strategies for ensuring consistent advice. We emphasise that a cohesive team approach is crucial in the implementation of the EDA-intervention.
How: Method of delivery
The first two components of the intervention (activity-specific education and collaborative activity selection) are delivered by a hand therapist, usually on an individual basis. Component one is delivered via verbal explanations supported by the patient education materials. Component two is delivered through discussion between therapist and patient. For this component, patients should be given the opportunity to practice activities using the occupation kits. This is an important step; if therapists were teaching range of motion exercises patients would be asked to repeat the exercise to demonstrate understanding and technique. Similarly, patients should practice simple daily activities with the therapist to demonstrate understanding of how to use activities to facilitate wrist and hand movement.
Component three is performed by the patient in their own environments.
Where (locations of the intervention)
Components one and two can be delivered face-to-face in a clinic. In this case, occupation kits may be used to support education and for practice. Alternatively, these components can occur via telehealth using a patient's own everyday items. Education materials can be made available during the face-to-face visit or via electronic methods for telehealth. Component three of the EDA-intervention is designed to be performed in the patient's home and other environments (work, leisure, social).
When and how much (frequency, duration, dosage)
The first component of the EDA-intervention (activity-specific education) should be implemented at the first postoperative therapy appointment ideally within 14 days postoperatively. Patients are advised that they can perform as many light daily activities throughout the day without a wrist orthosis as desired but within their comfort level and the parameters of light activity. Initially, activity sessions should be brief with rest periods in between and can increase as tolerated.
Component two (in-clinic practice and collaboration) will occur at each visit. Visit one will result in mutually agreed activities to be performed over the following week/s. At each subsequent visit, activities will be reviewed and graded up or down accordingly and the challenge of activities increased as fracture healing progresses.
Component three (performance of purposeful activities at home) occurs throughout the entire period that the intervention is implemented.
Tailoring the intervention
The intervention is not designed to be highly prescriptive rather relying on the patient's inherent ability to determine safe activity. For patients perceived to be at risk of over or under performance of daily activities, therapists should use their judgement to provide further education on the associated risks. Patients and therapists should iteratively refine therapy goals and selected activities at subsequent therapy sessions. As an example, an agreed activity may have been hanging out laundry on a clothes airer and folding clothing. This activity could be graded down if a patient reports pain or swelling to include hanging out of only small items or only half of the laundry items. The same activity could be graded up to include hanging out of larger items (towels, heavy clothing) if range of movement and pain has improved.
For the EDA-intervention to be successful therapists must adopt a flexible, creative approach. Because daily activities are inherently more variable than range of motion exercises, it may initially be challenging for therapists who are used to prescriptive exercise-based therapy.
Modifications
A process of stakeholder consultation and early trialling was undertaken in the development of the EDA-intervention. Consultation with hand therapists and surgeons at Counties Manukau Health in Auckland, New Zealand, took place in 2022. The primary researcher (JC) met with the teams to present the intervention and seek feedback. Surgeons and therapists supported the concepts and procedures of the intervention and provided suggestions that were used to iteratively modify patient education materials. EDA is currently being used in the Counties Manukau Health hand therapy clinic.
Future modifications will be informed by a planned study. The aim of that study is to explore clinician perspectives on the implementation of EDA in rehabilitative practice and readiness to adopt an occupation-based approach in wrist fracture rehabilitation.
Intervention fidelity: planned and actual
Methods for evaluating fidelity and facilitating uptake of the EDA-intervention will be explored as an additional aim in the above-planned study.
Next steps
In this article, we described the development of EDA, a theoretically driven, occupation-based intervention that uses light daily activities as the primary rehabilitative strategy after a surgically repaired distal radius. The rationale for the EDA-intervention is supported by an emergent evidence base that draws attention to the untapped potential of activity performance as a primary rehabilitative strategy. Our occupation-based intervention differs from existing postoperative protocols in that it specifies types, loads and intensity of daily activities, is supported by education that endorses rather than constrains daily activities, and directly aims to enhance psychosocial competencies.
The subsequent steps of intervention development according to the Medical Research Council are feasibility, evaluation, and implementation.19,20 We are planning a mixed methods study that will use focus groups and questionnaires including the Theoretical Framework of Acceptability Questionnaire
56
to seek clinician perspectives, inform therapist training requirements, and identify barriers to the uptake of the EDA-intervention. A feasibility study to define appropriate outcome measures, measures of fidelity, test recruitment and retention procedures, and obtain estimates of effect sizes to inform sample size calculation for a randomised controlled study should then be undertaken.
EDA is an occupation-based intervention designed to be commenced within two weeks of a surgically repaired distal radius fracture. The EDA-intervention is an alternative to exercise-driven rehabilitation that utilises the unique mechanisms of activities and occupation in facilitating wrist movement, hand function, and building psychosocial competencies.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155241258296 - Supplemental material for Early Daily Activity: Development and description of an occupation-based intervention for surgically repaired distal radius Fractures
Supplemental material, sj-docx-1-cre-10.1177_02692155241258296 for Early Daily Activity: Development and description of an occupation-based intervention for surgically repaired distal radius Fractures by Julie M. Collis, Elizabeth C Mayland, Nicola Kayes and Nada Signal in Clinical Rehabilitation
Supplemental Material
sj-pdf-2-cre-10.1177_02692155241258296 - Supplemental material for Early Daily Activity: Development and description of an occupation-based intervention for surgically repaired distal radius Fractures
Supplemental material, sj-pdf-2-cre-10.1177_02692155241258296 for Early Daily Activity: Development and description of an occupation-based intervention for surgically repaired distal radius Fractures by Julie M. Collis, Elizabeth C Mayland, Nicola Kayes and Nada Signal in Clinical Rehabilitation
Supplemental Material
sj-docx-3-cre-10.1177_02692155241258296 - Supplemental material for Early Daily Activity: Development and description of an occupation-based intervention for surgically repaired distal radius Fractures
Supplemental material, sj-docx-3-cre-10.1177_02692155241258296 for Early Daily Activity: Development and description of an occupation-based intervention for surgically repaired distal radius Fractures by Julie M. Collis, Elizabeth C Mayland, Nicola Kayes and Nada Signal in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors wish to thank hand therapists from Counties Manukau Health for their support in the development of EDA.
Author contributions
The authors confirm contribution to the paper as follows:
Substantial contribution to the concept or design of the article: JMC, ECM, NK, and NS. Manuscript preparation: JMC. Revised the manuscript critically for important intellectual content: JMC, ECM, NK, and NS. All authors reviewed the results and approved the final version of the manuscript. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable.
Supplemental material
Supplemental material for this article is available online.
Correction (June 2024):
Article type has been updated since its original publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.