
Abstract
Objective
To systematically evaluate the efficacy and safety of acupuncture therapy for neuropsychiatric symptoms in patients with Parkinson's disease.
Methods
We searched eight databases from their inception until 14 April 2024, including PubMed, Cochrane Library, Embase, Web of Science, SinoMed, China National Knowledge Infrastructure, China Science and Technology Periodical Database, and Wanfang Database. The search aimed to find randomized controlled trials assessing the effectiveness of acupuncture for neuropsychiatric symptoms in patients with Parkinson's disease. Literature screening and data extraction were performed independently by the authors. Meta-analysis was conducted using RevMan V.5.3 software, and Stata 17.0 software was used for detecting publication bias and performing sensitivity analysis.
Results
Twenty-eight studies, involving 2148 participants, met the inclusion criteria. The meta-analysis revealed that acupuncture therapy improved depression-related scale scores (standardized mean difference (SMD) = –0.70, 95%CI [–0.98, −0.42], p < 0.00001), anxiety-related scale scores (SMD = –0.78, 95% CI [–1.43, −0.14], p = 0.02), Montreal Cognitive Assessment scores (weighted mean difference (WMD) = 2.74, 95% CI [2.43, 3.05], p < 0.00001), Mini Mental State Examination scores (WMD = 2.36, 95% CI [0.78, 3.94], p = 0.003), Yale-Brown Obsessive Compulsive Scale scores, and Parkinson's Disease Questionnaire-39 scores (WMD = –2.66, 95% CI [–4.83, −0.49], p = 0.02) compared to controls.
Conclusion
This review supports the application of acupuncture to reduce the severity of neuropsychiatric symptoms including depression, anxiety, and impulse control disorders, and to improve cognition and quality of life in patients with Parkinson's disease. The adverse effects associated with acupuncture, either alone or as adjunctive therapy, were relatively minor.
Introduction
Neuropsychiatric symptoms are common non-motor symptoms of Parkinson's disease.1,2 These symptoms have received increased attention in recent years. Reports indicate that up to 87.5% of individuals with Parkinson's disease experience neuropsychiatric symptoms among their non-motor manifestations. 3 These symptoms impact prognosis, pose challenges to caregivers, and affect the quality of life for patients.4,5
Currently, the pathogenesis of Parkinson's disease and its link with neuropsychiatric symptoms are not well understood, and there are no specific curative treatments available.6,7 Levodopa replacement therapy remains the cornerstone of management for Parkinson's disease; 8 however, it primarily offers short-term improvement in motor symptoms and does not effectively address neuropsychiatric symptoms or halt disease progression. Levodopa therapy may even contribute to the development of neuropsychiatric symptoms.9,10 Surgical interventions are an effective adjunctive approach to treating Parkinson's disease; however, their limited availability due to technical limitations, concerns about efficacy, and high costs restrict their widespread application. Adjusting antiparkinsonian drug dosages or using antipsychotic medications are common strategies for managing neuropsychiatric symptoms. 11 Unfortunately, long-term use of these medications often leads to numerous adverse effects, necessitating dose reduction or discontinuation.12,13 Kinesiotherapy, physical therapy, occupational therapy, and psychotherapy are alternative therapies for treating patients with neuropsychiatric symptoms, but more research is needed to fully understand their efficacy. Additionally, significant barriers to accessing these therapies can limit their use and acceptance. Thus, the search for safe and effective interventions to maintain the quality of life for patients with Parkinson's disease is ongoing.
Acupuncture, a therapeutic practice rooted in traditional Chinese medicine, has been extensively used in clinical settings for over three millennia. 14 It is recognized for its straightforward approach, remarkable efficacy, and well-established safety profile, contributing to its broad potential applications and significant research interest. 15 Recent studies have reported the clinical effect of acupuncture therapy in treating neuropsychiatric symptoms in patients with Parkinson's disease. However, there are currently no systematic reviews assessing its effectiveness in addressing these symptoms and improving the quality of life. Hence, the aim of this systematic review is to reveal and present medical evidence regarding the efficacy and safety of acupuncture therapy for Parkinson's disease with neuropsychiatric symptoms.
Methods
This meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 16 and has been registered in PROSPERO (CRD42023462201).
A comprehensive search was conducted across four English-language databases (PubMed, Embase, Web of Science, and Cochrane Library) and four Chinese-language databases (China National Knowledge Infrastructure, Wanfang Database, Chinese Science and Technology Periodical Database, and SinoMed) to identify relevant studies published from the inception of the databases up to 14 April 2024. The search strategy utilized MeSH terms and keywords, with a Chinese translation of the search keywords conducted prior to the Chinese database searches. Details of our search strategies can be found in Supplementary material Tables 1–8. Additionally, a search on clinicaltrials.gov was conducted to ensure no relevant studies were missed. We also reviewed the references of published systematic reviews to identify potentially eligible articles.
Inclusion criteria were as follows: (1) randomized clinical trials reported in English or Chinese; (2) study populations clinically diagnosed with Parkinson's disease; (3) comparisons involving acupuncture versus placebo acupuncture, acupuncture versus standard treatment recommended by guidelines, acupuncture plus other therapy versus other therapy alone, or acupuncture plus other therapy versus placebo acupuncture plus other therapy; (4) reporting of outcome measures relevant to neuropsychiatric symptoms. Studies meeting any of the following criteria were excluded: (1) dissertations; (2) duplicate articles; (3) animal experiments; (4) conference articles; (5) reviews; (6) interventions not relevant to the study; (7) meta-analyses.
Two researchers independently performed literature screening based on predefined inclusion and exclusion criteria. Customized data extraction tables were used. Extracted data included general trial characteristics (name of the first author, date of publication, study period); baseline patient and disease data (sample size, age, disease duration); interventions (type of acupuncture, treatment dose, and duration); detailed adverse reactions; and outcome definitions. Discrepancies were resolved through consensus-building or by involving a third researcher.
Cochrane's risk of bias assessment method was used to evaluate the quality of randomized clinical trials, considering criteria such as random sequence generation, concealment of the allocation sequence, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other potential risks of bias. 17 Risks in each bias category were categorized as low, high, or unclear. 17 Discrepancies were resolved through deliberation.
The extracted data were processed and analysed using Review Manager software (V.5.3). For dichotomous variables, risk ratios (RRs) were used to report outcomes. Results for continuous variables were reported using weighted mean differences (WMDs) if assessment techniques were consistent, and standardized mean differences (SMDs) otherwise. I2 is a metric to evaluate the degree of heterogeneity among studies. Acceptable heterogeneity was identified when I2 ≤ 50%; in such cases, a fixed-effects model was used for analysis. Significant heterogeneity, identified when I2 > 50%, prompted the use of a random-effects model for analysis. When significant heterogeneity was present, subgroup or sensitivity analysis was conducted to explore potential sources. A p-value of 0.05 indicated statistical significance. Egger's test was used to detect publication bias, with p < 0.05 indicating its presence.
Results
Search results
A total of 2420 potentially eligible articles were identified through database searches, from which 1217 duplicate articles were removed. After screening the titles and abstracts, 112 articles were selected for full-text dual review, following the exclusion of 1091 articles based on inclusion criteria. Of these, 84 articles were excluded, with detailed reasons provided in the flow diagram (Figure 1). Ultimately, 28 articles were included in this meta-analysis.18–45 The included articles are listed in Supplementary References. The specific screening procedure is summarized in Figure 1.
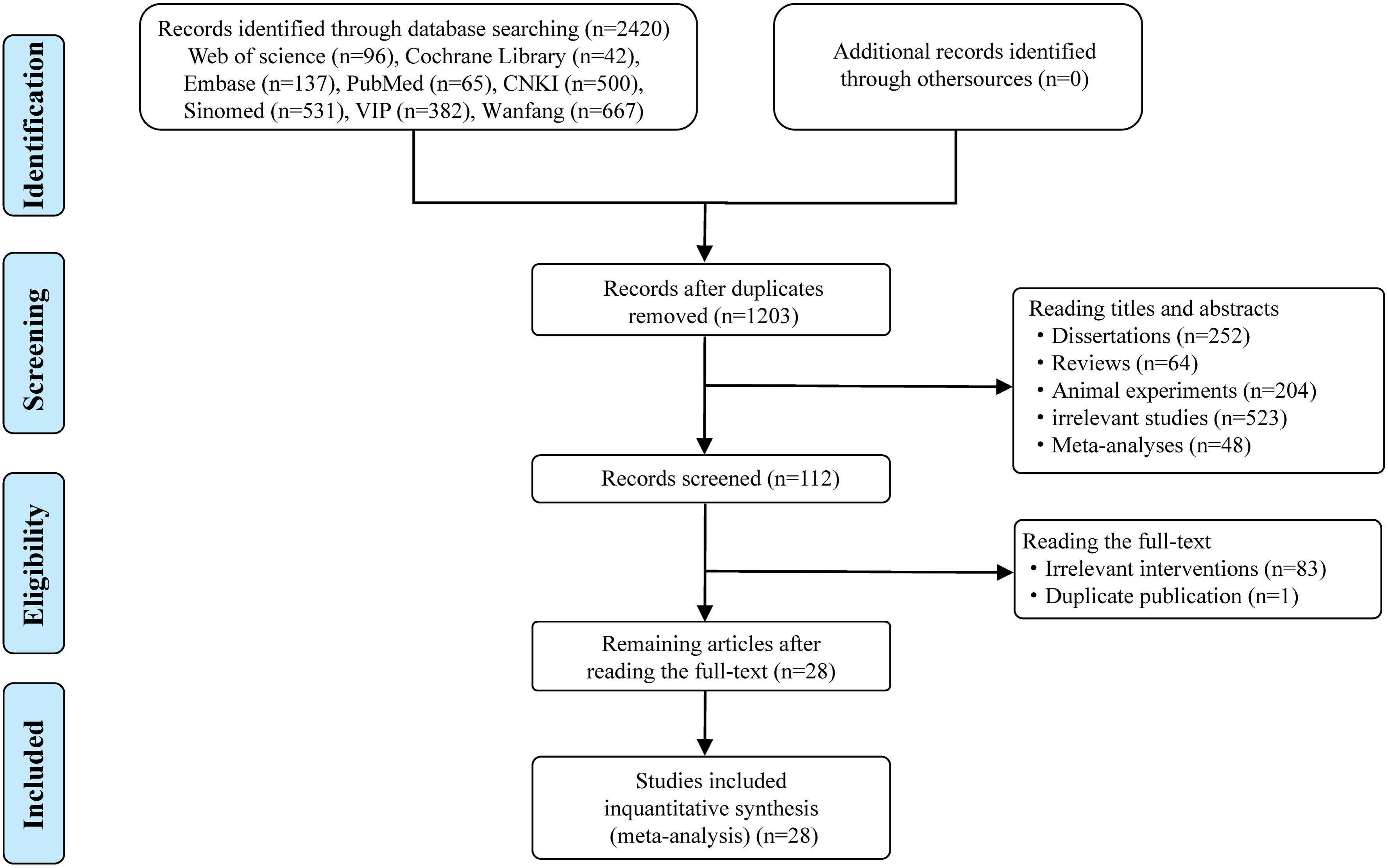
Flow diagram of studies included in the review.
Characteristics of the included studies
The included studies involved 2148 participants with Parkinson's disease, aged 44–84 years. Twenty-two studies18–29,31,32,35–42 were published in Chinese and six30,33,34,43–45 in English. Twenty-five studies were conducted in China, and one each in America, Korea, and Singapore. Among the 28 eligible articles, 20 studies18–29,31–34,42–45 focused on depression, six studies29–31,34,42,44 on anxiety, three studies32–34 on fatigue, eight studies35–41,44 on cognition, one study 42 on impulse control disorders, and three studies30,32,34 on quality of life.
In 2418–29,31,32,35–42,44,45 randomized clinical trials, the experimental interventions consisted solely of manual acupuncture or electroacupuncture, added to control regimens (drug therapy, repetitive transcranial magnetic stimulation, cognitive function training, or medication + cognitive function training). In three33,34,43–45 RCTs, the control groups received sham acupuncture or no treatment, while the experimental groups received acupuncture. In another RCT, 30 both groups underwent drug therapy, with the experimental group receiving acupuncture and the control group undergoing sham acupuncture. Electroacupuncture parameters included both continuous and dilatational waveforms, with frequencies ranging from 2 to 100 Hz. Each acupuncture session lasted between 10 to 60 min, and the frequency of sessions varied from 2 to 7 times per week. The courses of intervention lasted from 4 to 12 weeks. Details regarding the study characteristics are presented in Table 1.
Basic characteristics of the included studies.
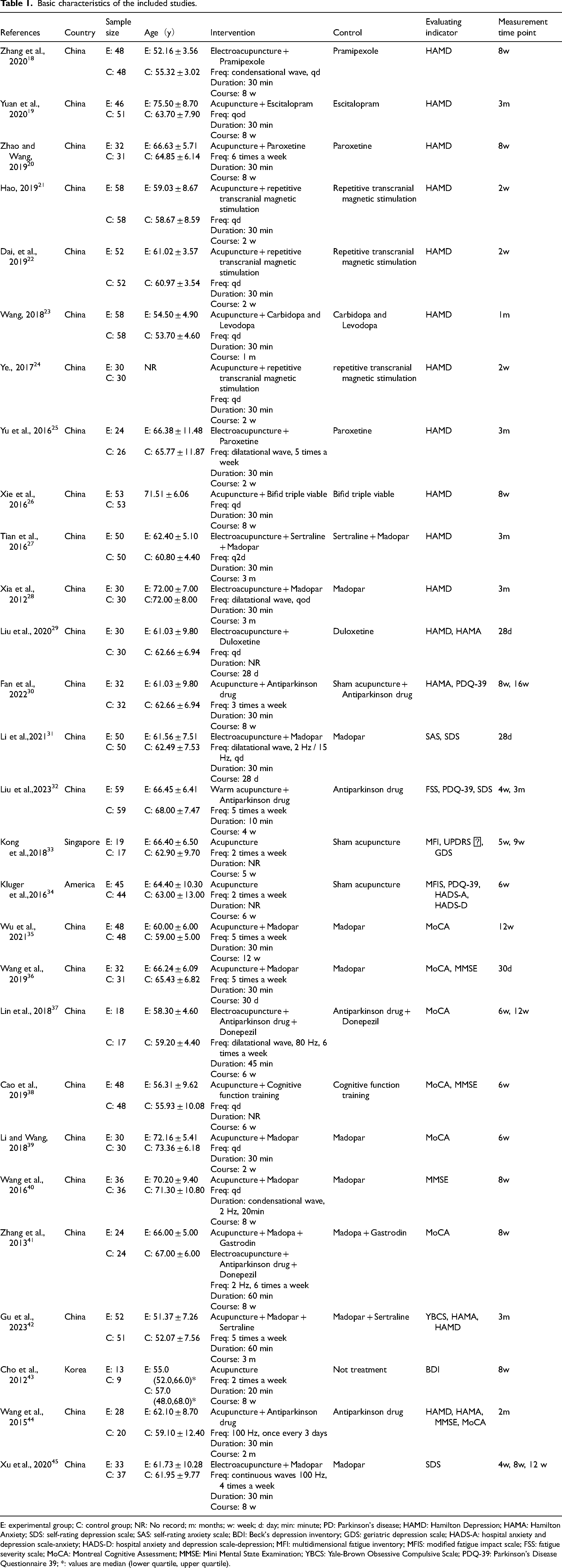
E: experimental group; C: control group; NR: No record; m: months; w: week; d: day; min: minute; PD: Parkinson's disease; HAMD: Hamilton Depression; HAMA: Hamilton Anxiety; SDS: self-rating depression scale; SAS: self-rating anxiety scale; BDI: Beck's depression inventory; GDS: geriatric depression scale; HADS-A: hospital anxiety and depression scale-anxiety; HADS-D: hospital anxiety and depression scale-depression; MFI: multidimensional fatigue inventory; MFIS: modified fatigue impact scale; FSS: fatigue severity scale; MoCA: Montreal Cognitive Assessment; MMSE: Mini Mental State Examination; YBCS: Yale-Brown Obsessive Compulsive Scale; PDQ-39: Parkinson's Disease Questionnaire 39; *: values are median (lower quartile, upper quartile).
Risk of bias
In the 28 randomized clinical trials considered, random number tables were used to generate sequences in 11 studies.20–22,24,27,31,32,35–38 Additionally, one study 19 employed a central system method, two studies30,45 used a computer-generated random number method, and two studies33,34 employed a permuted blocks method for grouping. These methods led us to deem these studies as having a low risk of bias. However, three studies23,28,39 grouped participants according to the order of visits, which we deemed to pose a high risk of bias. Other studies did not disclose the methodology used for generating random sequences. Allocation concealment was performed using opaque, sealed envelopes in one study 45 and an interactive web response system in one study, 33 while 26 studies did not report a specific method for allocation concealment. Overall, 23 studies were judged to have some concerns regarding risk of bias in the deviations from intended interventions domain because most studies did not blind participants and personnel, with only five studies30,33,34,44,45 reporting blinding. All studies had complete data with no missing outcomes, and most reported multiple outcome indicators, resulting in lower attrition and reporting bias. Figure 2 provides explicit details for the methodological quality assessment.
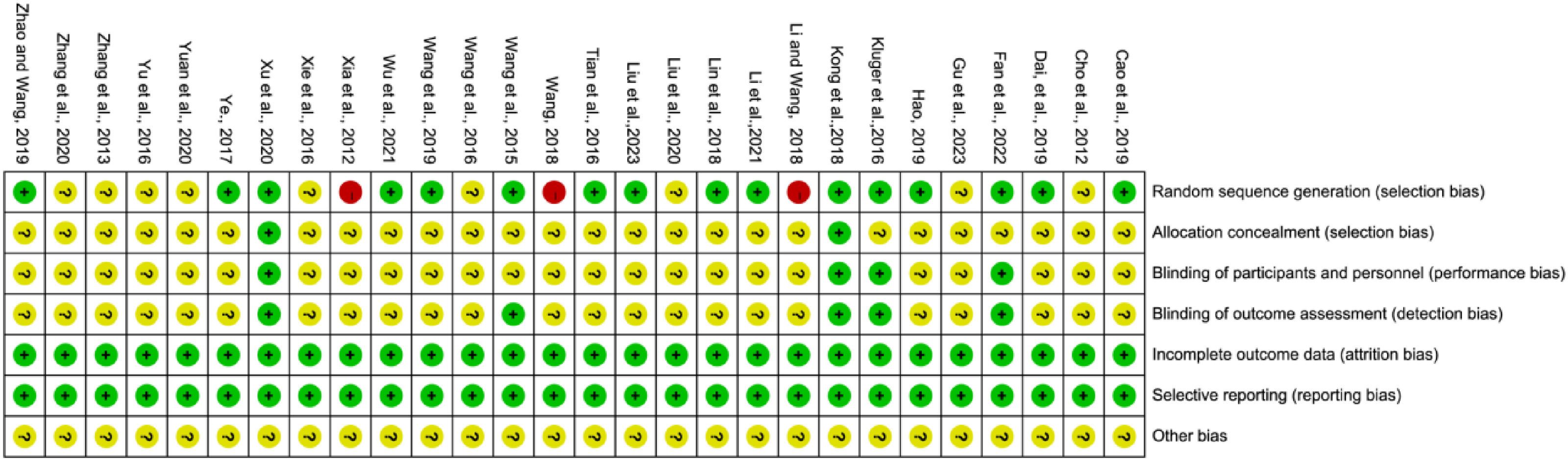
Risk of bias summary.
Results of the meta-analysis
Depression
Twenty studies employed various depression assessment scales to evaluate treatment effects. This research pooled data from 810 patients in the experimental groups and 804 patients in the control groups. Pooled results revealed a significant reduction in scale scores within the experimental group compared to the control group (SMD = –0.70, 95% CI: −0.98 to −0.42, p < 0.00001, I2 = 86%) (Figure 3).
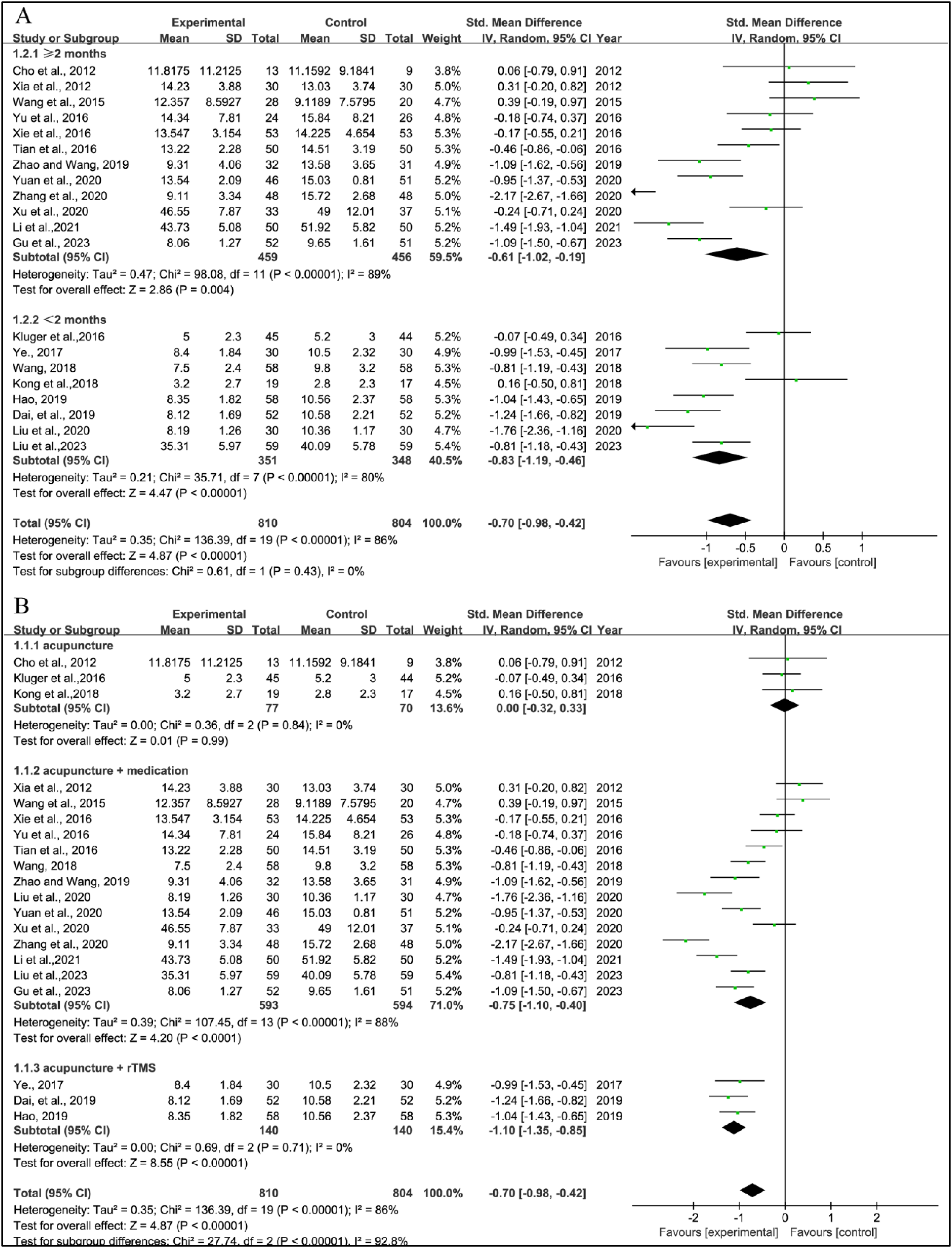
Standardized mean difference (95% confidence interval) of the effect of acupuncture on depression compared to control.
Given the significant heterogeneity, a subgroup analysis was conducted based on the intervention course; studies were separated into those evaluating outcomes within 2 months and those with evaluations extending beyond 2 months. Statistically significant heterogeneity (I2 = 89%) and a statistically significant advantage (SMD = −0.61, 95% CI = −1.02 to −0.19, p = 0.004) were observed in studies with courses longer than 2 months. Similarly, statistically significant heterogeneity (I2 = 80%) and a statistically significant advantage (SMD = −0.83, 95% CI = −1.19 to −0.46, p < 0.00001) were noted in studies with courses within 2 months (Figure 3a).
Further subgroup analysis was performed based on the type of intervention; studies were categorized into acupuncture alone, acupuncture combined with medication, and acupuncture combined with repetitive transcranial magnetic stimulation. Meta-analysis revealed no heterogeneity (I2 = 0%) in the acupuncture alone and acupuncture combined with repetitive transcranial magnetic stimulation groups. However, the acupuncture combined with repetitive transcranial magnetic stimulation group showed statistically significant differences in efficacy for improving depression (SMD = −1.10, 95% CI = −1.35 to −0.85, p < 0.00001), while the acupuncture alone group did not (SMD = 0.00, 95% CI = −0.32 to 0.33, p = 0.99) (Figure 3b). The analysis also revealed significant heterogeneity (I2 = 88%) in the acupuncture combined with medication group, demonstrating statistically significant differences in efficacy for improving depression (SMD = −0.75, 95% CI = −1.10 to −0.40, p < 0.0001) (Figure 3b). These subgroup analyses helped explain some of the heterogeneity observed.
Anxiety
Six studies utilized various scales to assess anxiety treatment effects. This research combined data from 237 patients in the experimental groups and 227 patients in the control groups. Pooled results showed a significant reduction in scale scores within the experimental group compared to the control group (SMD = –0.78, 95% CI: −1.43 to −0.14, p = 0.02, I2 = 91%) (Figure 4). Due to significant heterogeneity, a subgroup analysis was conducted based on the intervention treatment. Pooled results revealed high heterogeneity (I2 = 86%) in the acupuncture combined with medication group but acceptable heterogeneity in the acupuncture alone group (I2 = 42%). The acupuncture combined with medication group showed statistically significant differences in efficacy for improving anxiety (SMD = −1.20, 95% CI = −1.84 to 0.55, p = 0.0003), while the acupuncture alone group did not (SMD = −0.01, 95% CI = −0.45 to 0.47, p = 0.97) (Figure 4).
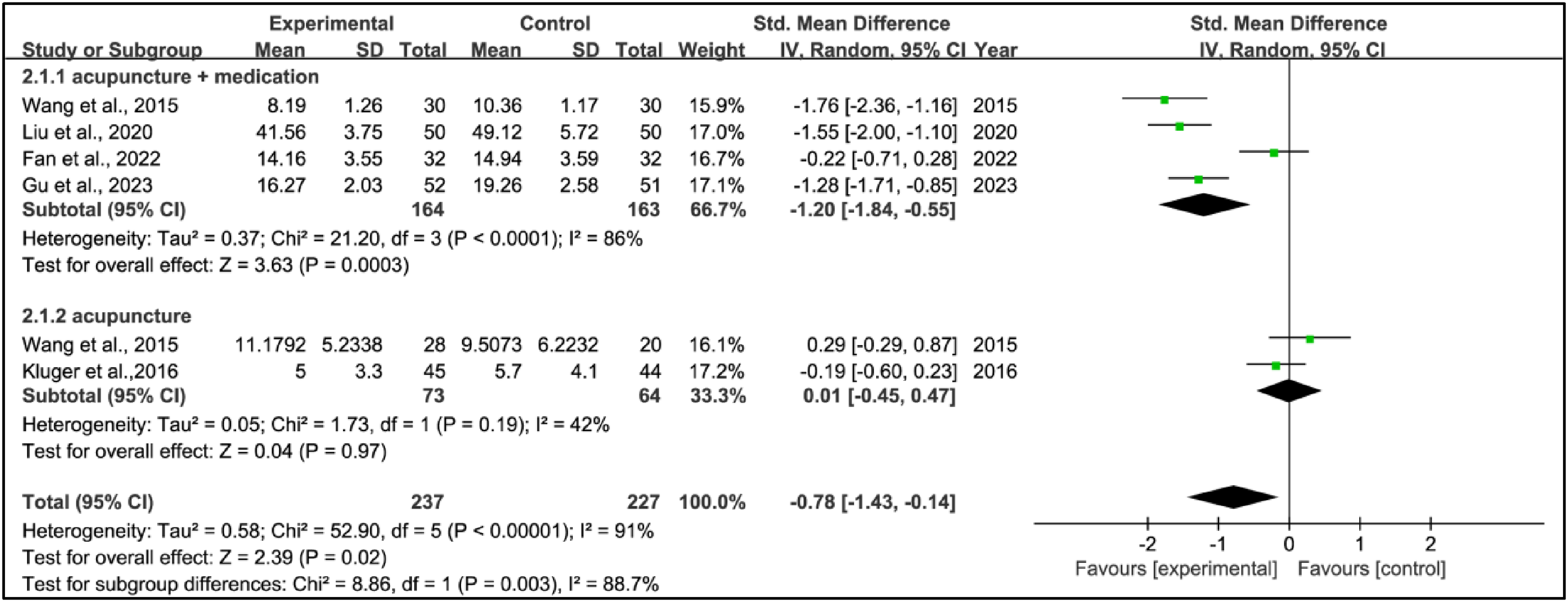
Standardized mean difference (95% confidence interval) of the effect of acupuncture on anxiety compared to control.
Fatigue
Three studies employed different scales to assess fatigue and evaluate treatment effects. This research combined data from 123 patients in the experimental groups and 120 patients in the control groups. Pooled results showed no significant differences in scale scores within the experimental group compared to the control group (SMD = –0.04, 95% CI: −0.51 to 0.43, p = 0.87, I2 = 67%) (Figure 5).

Standardized mean difference (95% confidence interval) of the effect of acupuncture on fatigue compared to control.
Montreal Cognitive Assessment Score
Seven studies utilized Montreal Cognitive Assessment scores to evaluate the treatment effects. This research amalgamated data from 244 patients in the experimental groups and 235 patients in the control groups. Pooled results showed a significant increase in Montreal Cognitive Assessment scores within the experimental group compared to the control group (WMD = 2.74, 95% CI: 2.43 to 3.05, p < 0.00001, I2 = 28%) (Figure 6).
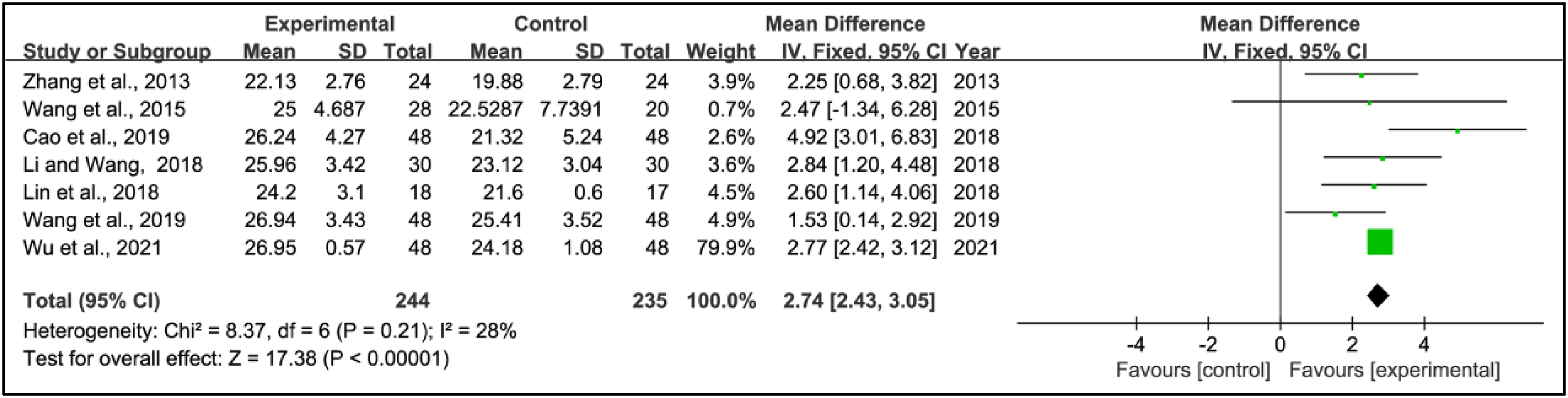
Weighted mean difference (95% confidence interval) of the effect of acupuncture on Montreal Cognitive Assessment score compared to control.
Mini Mental State Examination score
Five studies used the Mini Mental State Examination scores to assess treatment effects. This research combined data from 190 patients in the experimental groups and 182 patients in the control groups. Pooled results showed a significant increase in Mini Mental State Examination scores within the experimental group compared to the control group (WMD = 2.36, 95% CI: 0.78 to 3.94, p = 0.003, I2 = 81%) (Figure 7).
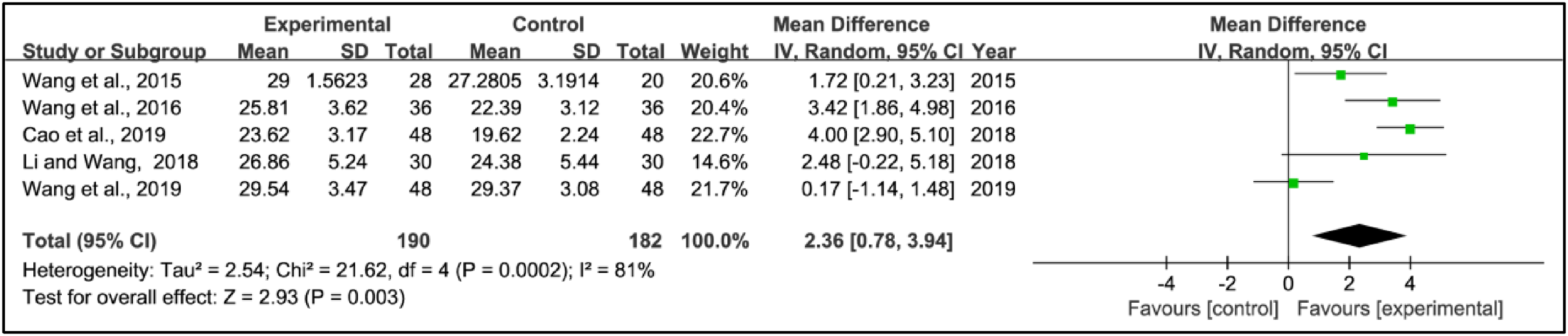
Weighted mean difference (95% confidence interval) of the effect of acupuncture on Mini Mental State Examination score compared to control.
Impulse control disorders
Only one study focused on the efficacy of acupuncture therapy for Parkinson's disease patients with impulse control disorders, so a quantitative synthesis could not be performed. This trial included 103 Parkinson's disease patients in an obsessive state who were randomized to receive 3 months of acupuncture in combination with Madopar and Sertraline or Madopar and Sertraline alone. Both groups exhibited significant improvements in their Yale-Brown Obsessive Compulsive Scale scores. Additionally, the inclusion of acupuncture to medication, compared to medication alone, notably reduced the obsessive state. Consequently, the authors concluded that acupuncture improved treatment outcomes, demonstrating good safety and practical applicability.
Parkinson's Disease Questionnaire 39 score
Three studies used the Parkinson's Disease Questionnaire 39 score to assess treatment effects. This research combined data from 136 patients in the experimental groups and 135 patients in the control groups. Pooled results showed a significant reduction in Parkinson's Disease Questionnaire 39 scores within the experimental group compared to the control group (WMD = –2.66, 95% CI: −4.83 to −0.49, p = 0.02, I2 = 0%) (Figure 8).

Weighted mean difference (95% confidence interval) of the effect of acupuncture on Parkinson's Disease Questionnaire 39 score compared to control.
Adverse reactions
Among the included studies, adverse events were reported in 12 trials. Four studies33,38,43,45 declared no adverse events in their trials. Three studies30,32,34 reported adverse reactions in the experimental group, while no adverse reactions were observed in the control group. Predominantly noted adverse reactions in both experimental and control groups included gastrointestinal symptoms, such as anorexia, nausea, vomiting, diarrhoea, and constipation. Additionally, occurrences of dizziness, arrhythmia, and renal function injury were observed. All adverse reactions were generally mild, with no reports of any serious adverse events. It is noteworthy that, compared to the control group, the experimental group might encounter phenomena like bleeding and subcutaneous haematoma due to the invasive nature of acupuncture treatment; however, these were not deemed serious adverse reactions. Details of adverse events can be found in Supplementary material Tables 9. The meta-analysis concluded that the incidence of adverse events did not differ significantly between the two groups, demonstrating the safety of acupuncture when used as an adjunctive therapy (RR = 1.01, 95% CI: 0.70 to 1.47, p = 0.94, I2 = 4%) (Figure 9).
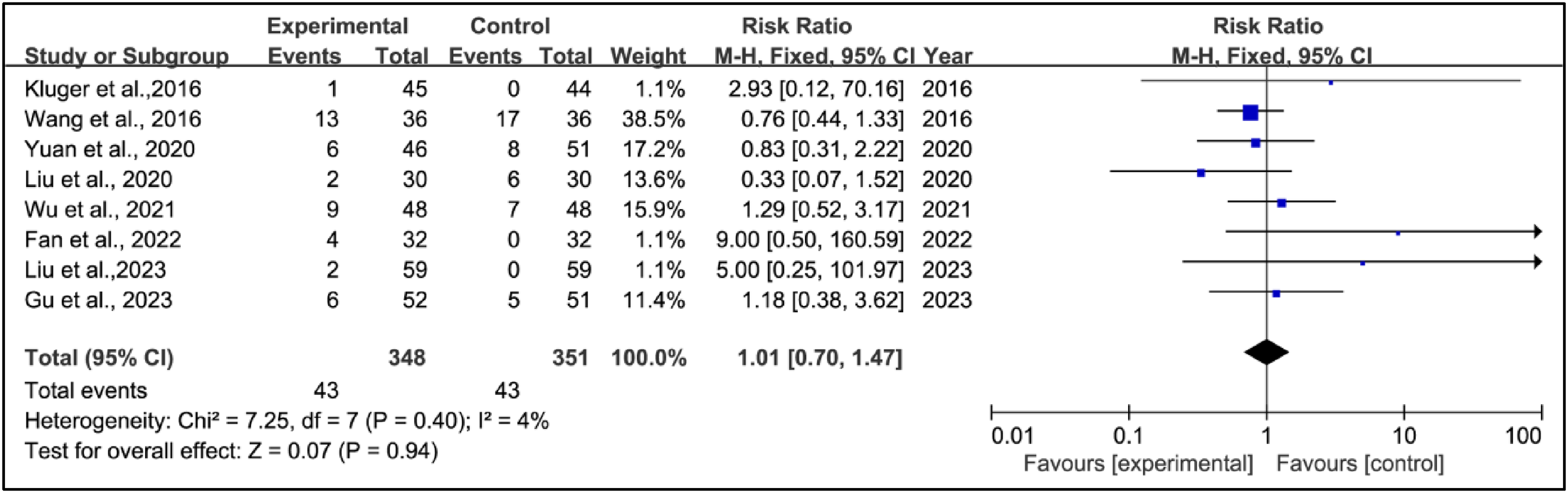
Risk ratio (95% confidence interval) of the effect of acupuncture on adverse reactions compared to control.
Sensitivity analysis
Stata 17.0 software was utilized to conduct a comprehensive sensitivity analysis on the notable heterogeneity outcomes of our study, which included depression, anxiety, fatigue, and Mini Mental State Examination scores. Leave-one-out meta-analysis demonstrated that the effects on depression, fatigue, and Mini Mental State Examination scores were stable, while the anxiety scores were not stable. More details are shown in Supplementary material Figures 1–6.
Publication bias
Probable publication bias for all outcomes was assessed using Stata 17.0 software. According to Egger's test, there appeared to be no publication bias on depression (p = 0.53), anxiety (p = 0.93), fatigue (p = 0.39), Montreal Cognitive Assessment score (p = 0.97), Mini Mental State Examination score (p = 0.78), and Parkinson's Disease Questionnaire 39 score (p = 0.40).
Discussion
In the context of Parkinson's disease, depression is commonly experienced by individuals, with estimated prevalence rates ranging from 20% to 50%. 46 Our study findings indicated that acupuncture treatment, compared to control treatments, yielded a statistically significant improvement in depression. We performed a subgroup analysis based on therapy length, and the results suggested that acupuncture positively influenced alleviating depressive symptoms in Parkinson's disease, regardless of whether treatment duration was less than or more than two months. Additionally, based on intervention treatment, the results showed that adjunctive acupuncture had a better therapeutic impact on depressive symptoms when contrasted with medication or repetitive transcranial magnetic stimulation alone. Although the overall therapeutic effectiveness aligns with several prior meta-analysis studies,47,48 a separate meta-analysis suggested that acupuncture treatment lasting more than 2 months did not demonstrate an obvious benefit in improving depressive symptoms among individuals with Parkinson's disease, 48 implying that the optimal treatment duration may involve maintaining the course within a 2-month timeframe. However, this research indicated that compared to medication alone, the addition of acupuncture did not yield significant advantages. 48 Considering the instability of the results indicated by the sensitivity analysis in Li's research, 48 our research findings might carry more convincing weight.
Regarding anxiety, it is a prevalent symptom in Parkinson's disease that is often ignored or underestimated. Research indicates that approximately 31% of patients with Parkinson's disease manifest symptoms of anxiety. 49 This study was the first of its kind to evaluate the efficacy of acupuncture in treating anxiety in Parkinson's disease patients. Pooled analysis indicated that acupuncture had a beneficial impact on reducing anxiety in these individuals. Furthermore, our subgroup analysis revealed that compared to patients who received medication alone, patients who received acupuncture in combination also had a substantial improvement in anxiety-related scale scores. Although acupuncture could effectively reduce Parkinson's disease-related anxiety symptoms, more robust evidence may be required, as the sensitivity analysis revealed some degree of instability in the results.
In terms of fatigue, pooled analysis revealed a prevalence rate of 50% for fatigue in Parkinson's disease. 50 No meta-analysis studies on the use of acupuncture for the treatment of Parkinson's disease-related fatigue were located. Unfortunately, our analysis did not show a significant effect of acupuncture in reducing Parkinson's disease-related fatigue. However, it is worth noting that this result should be examined with caution due to significant heterogeneity and a small sample size. In fact, acupuncture has been considered an effective and safe treatment for fatigue in conditions other than Parkinson's disease, such as chronic fatigue syndrome, 51 post-stroke fatigue, 52 and cancer-related fatigue. 53 Therefore, it is necessary to fill this gap by conducting high-quality, evidence-based studies to confirm the effectiveness of acupuncture on fatigue, especially Parkinson's disease-related fatigue.
Cognitive impairment, including Parkinson's disease with mild cognitive impairment and Parkinson's disease dementia, ranks among the most prevalent non-motor symptoms of Parkinson's disease. Among patients with Parkinson's disease, as many as 40% experience mild cognitive impairment while approximately 24% to 31% develop Parkinson's disease dementia. 54 In the majority of cases, Parkinson's disease-related mild cognitive impairment has a subtle onset and progresses gradually over time. As the condition progresses, it may eventually transition to Parkinson's disease dementia. 55 The Mini Mental State Examination, as a traditional cognitive impairment screening tool, has gained widespread utilization in clinical practice. 56 In contrast, the Montreal Cognitive Assessment Scale serves as a concise tool for screening cognitive function, primarily employed in evaluating individuals with mild cognitive impairment. Research has substantiated that the Montreal Cognitive Assessment Scale is a more effective discriminative tool for screening mild cognitive impairment within the Parkinson's disease population. 57 Pooled analysis showed that patients in the experimental group saw greater improvements in their Mini Mental State Examination score and Montreal Cognitive Assessment Scale score than those in the control group, suggesting that acupuncture treatment could improve the cognitive function of patients with Parkinson's disease.
Impulse control disorders refer to psychiatric disorders in which patients engage in inappropriate behaviours driven by strong desires for self-gratification. These behaviours often manifest as pathological gambling, hypersexuality, compulsive eating, and compulsive shopping. Research shows that the incidence of impulse control disorders in patients with Parkinson's disease ranges from 10% to 20%, with 1.7% to 7.0% experiencing compulsive gambling, 3.5% exhibiting compulsive sexual behaviours, and 0.4% to 3.0% engaging in compulsive shopping. 58 Among the studies included in this analysis, only one trial reported Parkinson's disease-related impulse control disorders. This particular trial involved 103 patients with Parkinson's disease who exhibited obsessive states, and it indicated that acupuncture treatment had a beneficial impact on these obsessive states. 42 Similarly, acupuncture treatment has also shown promise in refractory obsessive-compulsive disorder in those without Parkinson's disease. 59 Therefore, acupuncture holds promise as a potential treatment for Parkinson's disease-related impulse control disorders, particularly in addressing compulsive behaviours. However, given the limited availability of data for quantitative analysis, it is imperative to conduct additional high-quality evidence-based studies to conclusively verify its effectiveness.
The Parkinson's Disease Questionnaire 39 has been widely used as an instrument to measure the quality of life experienced by patients, where lower scores indicate a higher quality of life. 60 This review demonstrated that acupuncture could decrease scores on the Parkinson's Disease Questionnaire 39, implying its effectiveness in improving patient quality of life. This positive outcome may arise from acupuncture-induced improvement of neuropsychiatric symptoms, thereby contributing to an overall improvement in the quality of life.
This study serves as a valuable reference for clinical practice; however, it is important to acknowledge its inherent limitations. Firstly, due to language limitations, our study exclusively incorporates research published in Chinese and English, introducing a potential for selection bias and inadvertently excluding reports published in other languages. Through rigorous literature screening, only 28 articles were included. Such a number was far from adequate to comprehensively observe the efficacy of acupuncture in treating various neuropsychiatric symptoms of Parkinson's disease. This limitation was particularly noteworthy as only a handful of these articles focused on observing the effectiveness of acupuncture in treating neuropsychiatric symptoms such as anxiety, fatigue, and impulse control disorders. Secondly, most of the included literature focused on the treatment of Chinese patients, which may not fully represent the efficacy of acupuncture for neuropsychiatric symptoms among patients with Parkinson's disease globally. Thirdly, most of the included studies exhibited unclear risks of bias concerning allocation concealment and blinding, potentially resulting in imprecise evidence. Given the nature of acupuncture, achieving blinding for both participants and personnel poses challenges. However, if outcome assessors could be successfully blinded, it would mitigate potential measurement bias. Fourthly, many studies did not conduct patient follow-ups, which consequently hinders the assessment of acupuncture's long-term effectiveness in managing neuropsychiatric symptoms. Therefore, it remains imperative to conduct more randomized clinical trials with larger sample sizes, higher methodological quality, using innovative sham acupuncture devices, and extended follow-up periods to further substantiate the effectiveness and safety of acupuncture in treating Parkinson's disease with neuropsychiatric symptoms.
In conclusion, based on current research findings, acupuncture may provide short-term improvement in the symptoms of depression, anxiety, cognition, impulse control disorder, and quality of life among patients with Parkinson's disease. Thus, acupuncture holds the potential to be widely adopted as a complementary and alternative therapy for Parkinson's disease.
Clinical messages
Acupuncture may provide short-term improvement in the symptoms of depression, anxiety, cognition, and impulse control disorder among patients, thereby elevating their overall quality of life.
Acupuncture has not yet demonstrated significant effectiveness in addressing Parkinson's disease-related fatigue.
Acupuncture's mild side effects suggested it was a safe alternative treatment for Parkinson's disease.
Supplemental Material
sj-docx-1-cre-10.1177_02692155241258278 - Supplemental material for Efficacy and safety of acupuncture therapy for neuropsychiatric symptoms among patients with Parkinson's disease: A systematic review and meta-analysis
Supplemental material, sj-docx-1-cre-10.1177_02692155241258278 for Efficacy and safety of acupuncture therapy for neuropsychiatric symptoms among patients with Parkinson's disease: A systematic review and meta-analysis by Weiqiang Tan, Fengxi Xie, Jixi Zhou, Zhaoquan Pan, Muxi Liao and Lixing Zhuang in Clinical Rehabilitation
Footnotes
Author contributions
W.T. and F.X. originated the research, devised its methodologies, and drafted the initial manuscript. J.Z., Z.P. and W.T. formulated the search approach. Each author contributed to screening the research articles and assessing the included papers. M.L. created the flowchart and processed the data. L.Z. supervised the implementation of the entire project.
Declaration of conflicting interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China, Natural Science Foundation of Guangdong Province, Sanming Project Medicine in shenzhen Nanshan, (grant number 82174486, 2023A1515011411, No.SZSM202103010).
Statement of ethics
The current study is not necessary because it did not include individual participants. Instead, it focused on conducting a systematic review and meta-analysis of existing publications without collecting primary data. As there were no patients involved, concerns related to individual privacy do not apply.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.