
Abstract
Objective
Feasibility test a co-developed intervention based on Acceptance and Commitment Therapy to support psychological adjustment post-stroke, delivered by a workforce with community in-reach.
Design
Observational feasibility study utilising patient, carer, public involvement.
Setting
Online. UK.
Participants
Stroke survivors with self-reported psychological distress 4 + months post-stroke.
Interventions
The co-developed Wellbeing After Stroke (WAterS) intervention includes: 9-weekly, structured, online, group sessions for stroke survivors, delivered via a training programme to upskill staff without Acceptance and Commitment Therapy experience, under Clinical Psychology supervision.
Main measures
Feasibility of recruitment and retention; data quality from candidate measures; safety. Clinical and demographic information at baseline; patient-reported outcome measures (PROMs) via online surveys (baseline, pre- and post-intervention, 3 and 6 months after intervention end) including Mood (hospital anxiety and depression scale (HADS)), Wellbeing (ONS4), Health-Related Quality of Life (EQ5D5L), Psychological Flexibility (AAQ-ABI) and Values-Based Living (VQ).
Results
We trained eight staff and recruited 17 stroke survivors with mild-to-moderate cognitive and communication difficulties. 12/17 (71%) joined three intervention groups with 98% attendance and no related adverse events. PROMS data were well-completed. The HADS is a possible future primary outcome (self-reported depression lower on average by 1.3 points: 8.5 pre-group to 7.1 at 3-month follow-up; 95% CI 0.4 to 3.2).
Conclusion
The WAterS intervention warrants further research evaluation. Staff can be trained and upskilled to deliver. It appears safe and feasible to deliver online to groups, and study recruitment and data collection are feasible. Funding has been secured to further develop the intervention, considering implementation and health equality.
Introduction
Supporting psychological adjustment is the number one priority for Life After Stroke research in the UK,1,2 but we lack evidence-based interventions and have a severely under-resourced applied psychological clinician workforce in the UK (e.g. Clinical Psychologists, Counselling Psychologists and more). 3 Psychological interventions could be provided by other professionals, which may prevent the development of more severe mood difficulties in Life after Stroke. 4
Acceptance and Commitment Therapy is a third-wave, transdiagnostic, cognitive-behavioural psychotherapy. 5 It focuses on supporting clients to develop a psychologically flexible relationship with the present moment and associated challenges, towards committed action in service of personal values. It has potential benefits for supporting wellbeing and preventing depression after acquired brain injury,6–10 and has been delivered as a group-based face-to-face intervention for stroke survivors. 11
Remotely delivered interventions, rather than face-face, may help optimise service delivery, especially in a post- COVID-19 pandemic world. 12 There is a strong case for research into the acceptability and feasibility of remote service delivery models.
In close collaboration with a study-specific patient, carer, and public involvement (PCPI) advisory group and other experts, we built on an existing intervention 10 to co-develop Wellbeing After Stroke (WATerS) between January 2020 and May 2021. WAterS is a highly structured psychotherapy, delivered online to groups of stroke survivors. An adjunct training programme was also developed to upskill staff with the skills and knowledge to safely deliver WAterS (for detailed intervention description see Methods and Supplemental material).
This paper reports results of a feasibility study which had the specific objectives to: (a) evaluate the feasibility of delivering the WAterS intervention: both the staff training and the stroke survivor intervention and (b) explore the feasibility of a future research trial, including: recruitment and retention of stroke survivors; inclusion/exclusion criteria; data quality from baseline and candidate outcome measures; adverse events. A process evaluation, exploring fidelity and acceptability utilising qualitative and quantitative methods and data, is reported separately. 13
Methods
This study was informed by the Medical Research Council's new framework for developing and evaluating complex interventions (development and feasibility phases components), 14 and collaborative-level patient involvement. 15 Ethics approval was secured from the University of Manchester (ref: 2021-11134-18220) who also acted as sponsor. The study is registered: https://clinicaltrials.gov/ct2/show/NCT04655937
A study-specific patient advisory group of four individuals with experience of stroke and caring was set up at the early stages of the study. They met regularly to support initial intervention development, including providing feedback on proposed intervention materials and role-playing the intervention in practice. They advised on participant recruitment and data collection, considering burden for stroke survivors.
The research team members responsible for all participant-facing procedures were Patchwood and Foote. Remote delivery meant no geographical limits; recruitment was open throughout the UK and all research procedures were conducted by telephone or Zoom.
Staff participants were recruited to deliver the intervention, with two staff per session deemed necessary to ensure patient safety, cover unexpected absence and ensure smooth running of the technology. They worked for a major UK charity specialising in stroke (Stroke Association) and were eligible if they had: at least 6 months experience; capacity to dedicate to the study; experience facilitating groups; no prior experience using Acceptance and Commitment Therapy models. Staff were opportunistically sampled (identified by their senior leaders) and those eligible were provided with study information prior to informed consent, with training commencing immediately after recruitment.
The initial staff training programme was delivered online over four weekly sessions, by a Clinical Psychologist (Hill). After training, support consisted of an online weekly 1-hour group session with a Clinical Psychologist providing opportunities to reflect and troubleshoot with an expert and each other.
Following completion of staff training, stroke survivor participants were recruited for feasibility testing. The eligibility criteria were adults (aged 18 + ) at least 4 months post-stroke, with self-reported difficulties adjusting to their stroke, internet access and sufficient English language (and willingness) to engage in a remotely delivered intervention. Study advertisements were circulated via third sector, research networks and social media, with interested parties self-referring to the research team for information and consent. Eligibility was determined based on self-report and research team clinical judgement. The intervention was stroke survivor focused, but informal carers (e.g. family members or friends) could be invited to support, on request of the stroke survivors. No formal data were collected about informal carers but a procedure for involving them was in place in the interests of data protection, regulation and safety.
Baseline data on staff participants included demographic and employment-related data. Baseline data on stroke survivors included demographic and clinical data as well as patient-reported outcome measures (PROMs). At baseline, the latter were asked to self-rate their cognition and mental health (see Table 2). Researcher-administered assessments were then completed: components of the montreal cognitive assessment, 16 Frenchay Aphasia Screening Test 17 and the Quick Aphasia Battery for Comprehension. 18 Researchers then rated stroke survivor participants on the therapy outcome measures 19 scales for aphasia (activity level) and cognition (impairment level). Participants were then sent a link to an online survey platform to self-complete baseline measures related to: mood (the hospital anxiety and depression scale (HADS)) 20 ; personal wellbeing (ONS4) 21 ; independence in activities of daily living (the Modified Barthel Index). 22 We also asked about other support they were receiving for their wellbeing. Participants could request researcher support to complete online surveys.
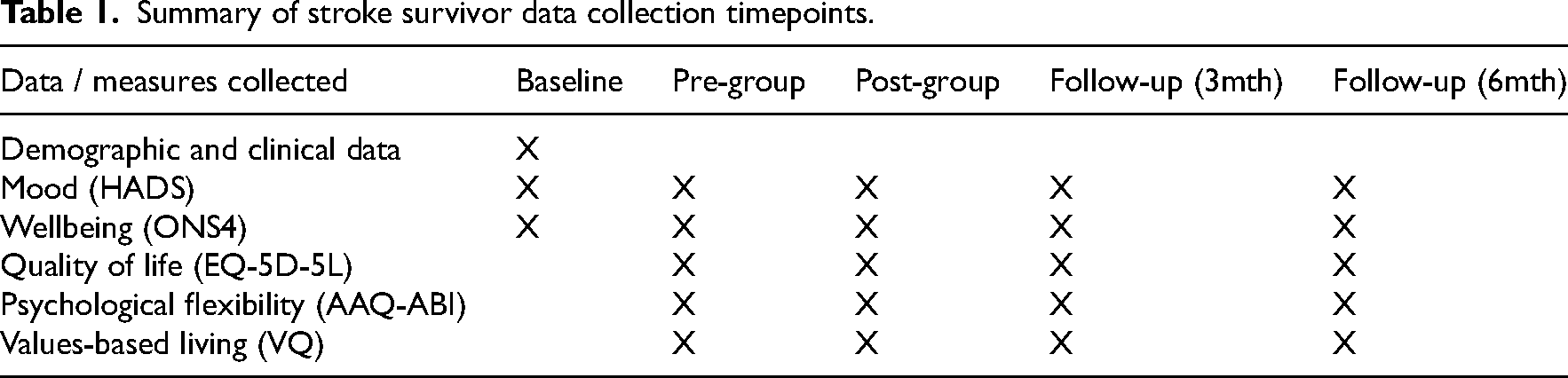
We had capacity to run up to four intervention groups. This was not a randomised controlled trial and there was no control group. As a feasibility study, we did not have a pre-determined sample size but anticipated a minimum of four stroke survivors per group (maximum of eight). After sufficient participants were recruited to run groups, stroke survivors had the choice of joining or declining the intervention. If they declined, they could either withdraw from the study or continue online surveys at regular time intervals, to explore the feasibility of data collection in the absence of intervention (see Table 1). Once sufficient participants agreed to intervention, they were randomly assigned to therapy groups. Participants were sorted according to a random number generator with equal number of participants assigned to the intervention groups (labelled Group A, B, and so on).
Summary of stroke survivor data collection timepoints.
The intervention involved activities informed by Acceptance and Commitment Therapy, delivered over 9-weekly sessions online. A client handbook was sent to participants in advance of intervention commencement to support engagement. The handbook included summaries of the session content, worksheets and weekly homework to complete. Each session was facilitated by two trained staff: one designated ‘lead’ to have primary responsibility for delivering; the other ‘support’ to ensure smooth flowing of the session, including technical and safety issues. Support staff could lead in sessions, depending on confidence and the lead/support dynamic. The intervention was highly structured to enhance fidelity and equip non-experts to facilitate (see Supplemental material).
Table 1 summarises the data collected through online surveys from stroke survivor participants at each timepoint: immediately prior to intervention group (pre-group); after final intervention group session (post-group); and 3- and 6-months later (follow-ups). These data included repetition of some baseline measures as well as others exploring health-related quality of life (EQ-5D-5L), 23 and two questionnaires to explore the key targeted processes of change in this psychotherapy: psychological flexibility (AAQ-ABI) 24 and values-based living (VQ). 25
This study was not powered to examine effectiveness. Outcomes were collected to explore feasibility of data collection and inform the choice of a primary outcome for an eventual trial. Serious Adverse Events were collected as they occurred. Figure 1 shows a summary of the study processes and timelines. A parallel process evaluation used quantitative and qualitative methods to explore fidelity and acceptability. 13 Brief, ‘take-home messages’ are included below.
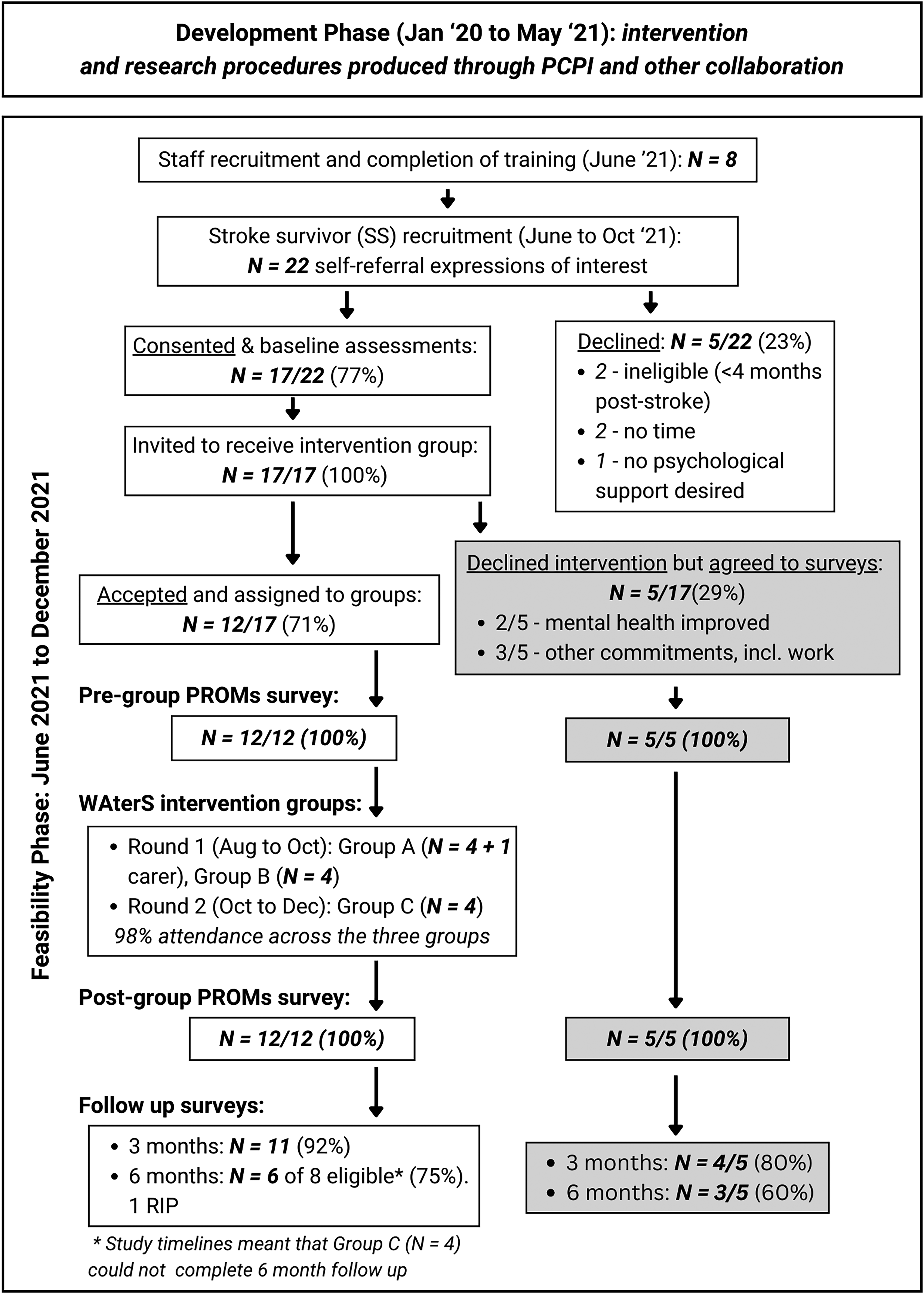
Study timelines and flow of participants.
Results
Recruitment and testing began formally in June 2021. Figure 1 shows the flow of participants through this phase of the study, as well as study timelines.
Eight eligible staff were trained and recruited. All were female, with a mean age of 53 (SD: 7.63) and mean of 6 years working for the organisation (range 1–15). Five staff were trained as lead practitioners, and three as support. The five lead staff had a UK level four counselling qualification. Seven of the eight then supported delivery of the intervention.
Recruitment of stroke survivors appeared feasible using our range of methods, amidst an ongoing pandemic. From 22 expressions of interest, 17 (77%) consented and completed baseline assessments, with one informal carer also involved to support their spouse. When invited to receive intervention therapy groups, 12/17 (71%) accepted and 5/17 (29%) declined groups but agreed to continue completing surveys. Table 2 shows stroke survivor participant characteristics at baseline; separate columns show data for 12 who participated in intervention vs the five survey-only.
Baseline characteristics: intervention participants (N = 12) and survey only (N = 5).
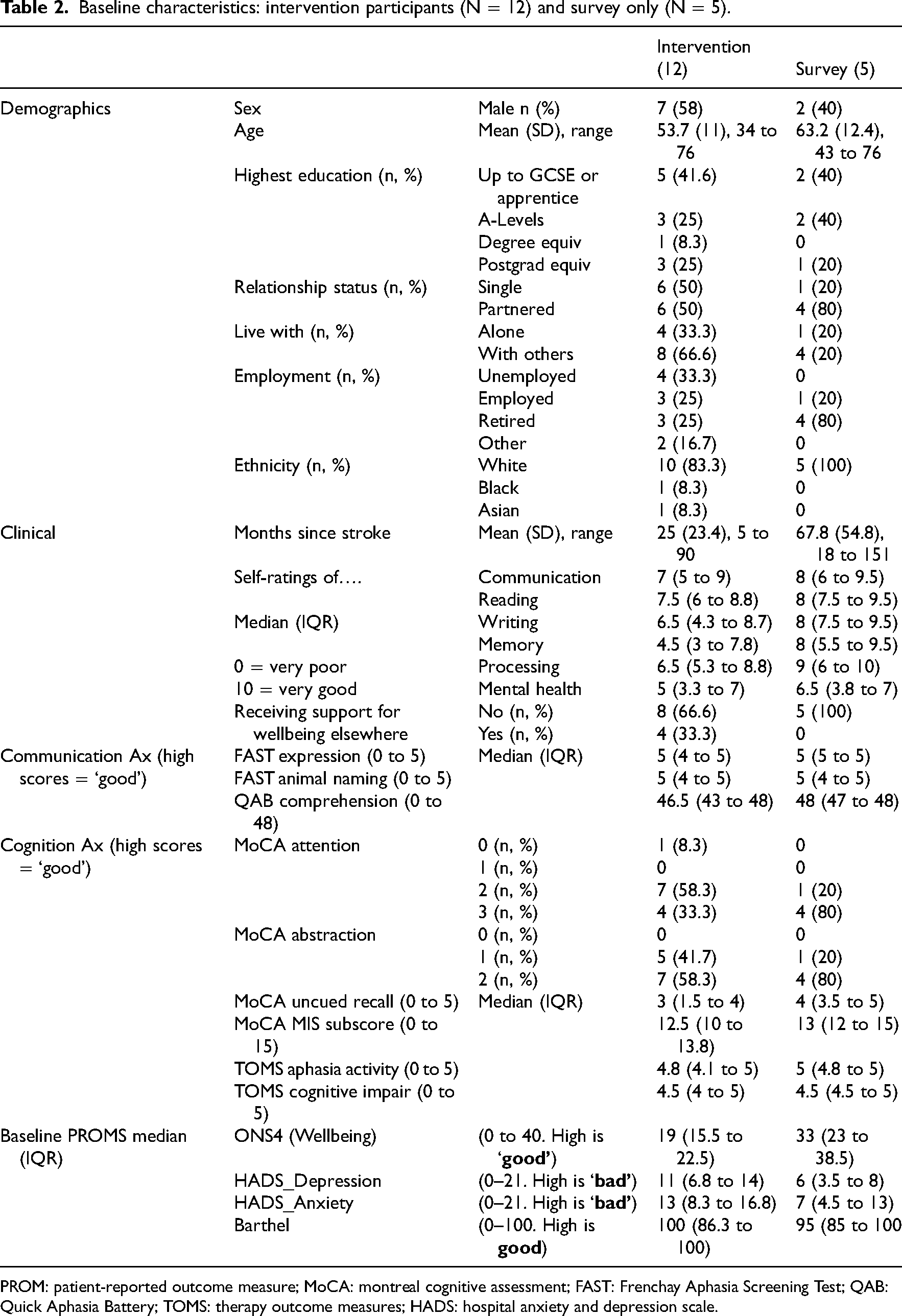
PROM: patient-reported outcome measure; MoCA: montreal cognitive assessment; FAST: Frenchay Aphasia Screening Test; QAB: Quick Aphasia Battery; TOMS: therapy outcome measures; HADS: hospital anxiety and depression scale.
Roughly half the stroke survivor participants were male and the majority were White British. Of the 12 who joined the intervention, the mean (SD) age was 53.7 (11) years and mean (SD) months post-stroke was 25 (23.4). Other measured characteristics indicate that all participants had mild-moderate cognitive and communication difficulties (only 2/12 intervention participants self-reported expressive aphasia).
The 12 participants consenting to intervention were assigned to three WAterS groups: A, B, C. The five who declined intervention but continued with outcomes appeared to be later post-stroke, were all receiving other support and had less self-reported need. The mean (SD) wait time from consent to intervention start was 31 (14.5) days (min = 14; max = 68). All group sessions happened weekly over 9 weeks as planned, with excellent attendance at 98%. No related serious adverse events were recorded. The experiential exercises did evoke emotional responses from participants, including appropriate levels of distress or discomfort, but these were managed within the group.
Table 3 shows data for intervention group (N = 12) and survey-only cohort (N = 5) collected at the four timepoints after baseline, including numbers to show attrition. Online data collection from stroke survivors was feasible. The mean (SD) time to complete surveys was 19.3 (19.1) minutes (min = 4.1; max = 90). 90 min was with researcher support (for one participant). Fully completed datasets were captured pre- and post-group. At 3-month follow-up, completion was 80–92% across the sample; At 6-month, 60–86% completed.
PROMs data for 4x timepoints. Intervention (N = 12) and surveys only (N = 5).
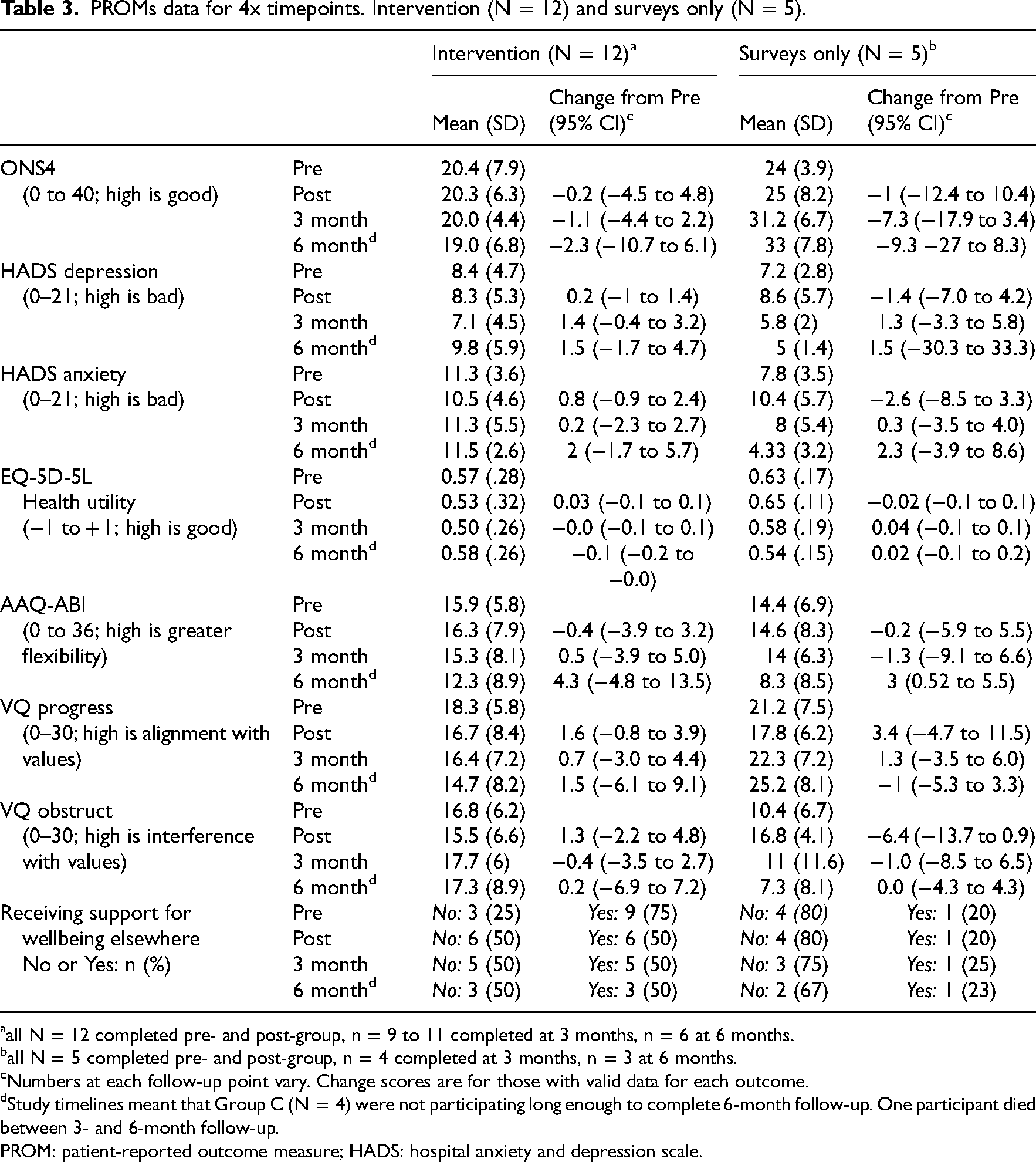
all N = 12 completed pre- and post-group, n = 9 to 11 completed at 3 months, n = 6 at 6 months.
all N = 5 completed pre- and post-group, n = 4 completed at 3 months, n = 3 at 6 months.
Numbers at each follow-up point vary. Change scores are for those with valid data for each outcome.
Study timelines meant that Group C (N = 4) were not participating long enough to complete 6-month follow-up. One participant died between 3- and 6-month follow-up.
PROM: patient-reported outcome measure; HADS: hospital anxiety and depression scale.
In terms of our process evaluation exploring fidelity and acceptability, 13 our brief ‘take-home’ messages are that: staff reported feeling prepared and motivated to deliver the intervention and so we can upskill a wider workforce to deliver; WAterS was delivered with good fidelity to clinical protocols and consistency with the ACT theoretical model; WAterS was an acceptable and valued intervention for those stroke survivors that received it.
Discussion
This study demonstrated the feasibility of delivering the WAterS online, wellbeing group intervention, and of evaluation using online data collection. Accessibility to the intervention, and the study, benefitted from a study-specific PCPI panel. The intervention was feasible to deliver using a third sector workforce with no previous experience of Acceptance and Commitment Therapy, following the WAterS staff training and supervision programme. Study recruitment was successful, despite the pandemic. Attendance at the online groups (98%) was excellent for those who opted in, and future work will focus on widening access, mindful of health inequalities.
Recruitment for stroke survivors required self-referral following online advertisement. We have useful descriptive data on our sample but a limitation of the study is that we do not have data on the proportion of people who saw the adverts, were potentially eligible, and did not self-refer. Understanding rates of eligibility in a population helps power and inform future trials, 26 so methods of recruitment may need to be enhanced in future work e.g. utilising stroke healthcare pathways to recruit through healthcare professionals. However, study recruitment using digital platforms is becoming more common. 27 It can increase reach to certain communities, including those likely to opt into an online intervention, but is threatened by digital poverty and may result in a sample that is skewed towards lower stroke morbidity and higher social economic status, which may limit findings.28,29 We recruited a predominantly white (83%), well-educated, mild-to-moderate morbidity sample. This racial profile is similar to existing studies in stroke but reflects issues with equity of access, considering the well-documented health inequalities in stroke.30,31 Future work must carefully consider how to engage a more diverse range of stroke survivors.
All 12 intervention group participants – including the two with self-reported (and observable) expressive aphasia – were able to engage in the intervention. Eligibility was explored via self-report and researcher judgement, without use of cut-off scores on assessments of mood or cognition. A limitation of our data may be that they simply describe who took part and are not sufficient to comment, post-hoc, on whom this intervention might be best-suited. Offering psychotherapeutic support to individuals with sub-threshold psychological disorders may help prevent mental health crises.7,32 Assessing perceived readiness or willingness to engage in this kind of psychotherapy may be more important than assessing mood or impairment when considering eligibility. 33
As anticipated for a mental health intervention, the experiential exercises evoked some appropriate and expected emotional responses from participants. Both facilitators and peers provided support (e.g. exploration of the triggering experiences) to contain and ‘heal’. The intervention appeared safe in this study. It is important not to conflate safety with ‘no distress experienced’; participants sometimes reflected that emotional responses could lead to adjustment and positive transformation. Qualitative interview data exploring stroke survivor experiences in detail are discussed elsewhere, 13 suggesting that both staff and stroke survivors found the intervention acceptable and valuable, with fidelity to clinical protocols achieved. We had not anticipated recruiting lead staff with counselling qualifications to facilitate (i.e. it was not an original eligibility criterion) but the added counselling skills may have contributed to the safety and success in this study. Exploring the minimum requirements for staff to deliver this intervention safely – and with fidelity – is an avenue for future research.
Five stroke survivors (29%) declined the intervention but completed online follow-ups; two due to self-reported mental health improvements and three due to lack of availability to attend sessions (see Figure 1). The latter barrier may have been overcome with availability discussed in detail during recruitment. The former is interesting, since all participants initially reported difficulties with their mental health and a desire to receive support. However, their baseline data show lower self-reported anxiety and depression levels in these five compared to the 12 who opted to join a group. Future work could explore the value of providing a little more time for stroke survivors to decide whether their self-reported needs warrant intervention. Space to normalise their feelings may be sufficient for some and preferential to the treatment burden of a 9-week intervention.
Online data collection appeared acceptable and feasible, although one participant required support to complete (taking 90 min), which may be unfeasible in a larger trial. Our choice of outcomes was informed by the literature 34 and PCPI. This small study was not powered to explore measurement outcomes. All change scores must be viewed with caution. However, HADS depression may be a candidate measure for primary outcome in future research; it was lower on average by 1.4 points at 3-month follow-up (8.5 to 7.1; 95% CI −0.4 to 3.2). Minimal clinically important difference (MCID) on HADS are not available for stroke, but research in cardiovascular disease suggests MCID of 1.7 points. 35 In addition, other studies using this therapeutic model in acquired brain injury have suggested that the HADS is sensitive to change.6,36
In conclusion, the co-developed online WAterS group intervention was feasible to deliver to stroke survivors using a trained workforce and had a high adherence rate. Further in-depth data on fidelity and acceptability are reported elsewhere.
13
Success with study processes, online data collection etc., suggested further research evaluation is feasible and warranted with enhancements to recruitment routes and outcome measures. Further funding has been secured to develop the clinical and research protocols for WAterS, focused on addressing aspects of health inequalities and widening the workforce. This future funding will gather more data to inform the choice of baseline and outcome measures and ultimately work towards a robust randomised controlled trial with process evaluation.
The WAterS psychotherapy is feasible to deliver remotely in research contexts. We encourage clinicians to promote stroke survivors’ participation in future research. Non-clinical staff can feasibly be upskilled to deliver psychotherapies. Clinicians should consider standardised tools for mood - HADS depression may be a candidate primary outcome for future trials.Clinical messages
Supplemental Material
sj-docx-1-cre-10.1177_02692155241239879 - Supplemental material for Wellbeing After Stroke (WAterS): Feasibility Testing of a Co-developed Acceptance and Commitment Therapy Intervention to Support Psychological Adjustment After Stroke
Supplemental material, sj-docx-1-cre-10.1177_02692155241239879 for Wellbeing After Stroke (WAterS): Feasibility Testing of a Co-developed Acceptance and Commitment Therapy Intervention to Support Psychological Adjustment After Stroke by Emma Patchwood, Hannah Foote, Andy Vail, Sarah Cotterill, Geoff Hill, and Audrey Bowen in Clinical Rehabilitation
Footnotes
Acknowledgements
This independent research was funded by a Stroke Association Postdoctoral Fellowship Award (Ref SA PDF 18100024). The views expressed are those of the author(s) and not necessarily those of the Stroke Association. Authors also acknowledge funding from The University of Manchester Research Impact Scholarship (MC). Funders had no role in study design, execution, analysis or results interpretation.
The authors extend thanks to patient participants, therapy and research staff, and our dedicated PCPI patient advisory group. Our PCPI group members are listed as co-authors and include: Mrs Ann Bamford, Mr Stephen Taylor, Mr Nigel Bamford, Ms Loretta Hanley.
Data Availability
All data produced in the present study are available upon reasonable request to the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Manchester, Stroke Association, (grant number Research Impact Scholarship, SA PDF 18100024)
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.