
Abstract
Objective:
To assess the feasibility of a randomized controlled trial to evaluate music therapy as a home-based intervention for arm hemiparesis in stroke.
Design:
A pilot feasibility randomized controlled trial, with cross-over design. Randomization by statistician using computer-generated, random numbers concealed in opaque envelopes.
Setting:
Participants’ homes across Cambridgeshire, UK.
Subjects:
Eleven people with stroke and arm hemiparesis, 3–60 months post stroke, following discharge from community rehabilitation.
Interventions:
Each participant engaged in therapeutic instrumental music performance in 12 individual clinical contacts, twice weekly for six weeks.
Main measures:
Feasibility was estimated by recruitment from three community stroke teams over a 12-month period, attrition rates, completion of treatment and successful data collection. Structured interviews were conducted pre and post intervention to establish participant tolerance and preference. Action Research Arm Test and Nine-hole Peg Test data were collected at weeks 1, 6, 9, 15 and 18, pre and post intervention by a blinded assessor.
Results:
A total of 11 of 14 invited participants were recruited (intervention n = 6, waitlist n = 5). In total, 10 completed treatment and data collection.
Conclusion:
It cannot be concluded whether a larger trial would be feasible due to unavailable data regarding a number of eligible patients screened. Adherence to treatment, retention and interview responses might suggest that the intervention was motivating for participants.
Trial registration:
ClinicalTrials.gov identifier NCT 02310438.
Introduction
A total of 80% of stroke cases result in hemiparesis, 1 and half this number experience persistent lack of arm function. 2 Effective interventions are lacking, and evidence to support those that are accessible is insufficient. 3 A clear need has been identified for long-term support in the community for people with stroke, but services are limited and few studies have examined home-based interventions and provided sufficient detail of the protocols used. 4
Music interventions may be beneficial for improving arm function following stroke,5,6 and a strong rhythmic stimulus embedded within music may enhance motor performance more than the use of a rhythmic stimulus alone without music. 7 More research is needed to establish the effects of music interventions on arm function, and with the majority of rehabilitation being delivered in patients’ homes it is useful to determine the feasibility of home-based treatment delivery and research. This article reports on the feasibility of conducting a randomized controlled trial where a music intervention, for which there was a clear protocol based on published guidelines,8,9 was delivered in a variety of home environments.
Methodology
For this pilot feasibility randomized controlled trial, patients were recruited following discharge from three community stroke teams into a cross-over design. All participants provided written, informed consent. Ethical approval was granted by the Essex Research Ethical Committee (reference 13/EE/0400). The study was registered with ClinicalTrials.gov, registration number NCT 02310438.
The criteria for inclusion were as follows: (1) >18 years, (2) 3–60 months post stroke, (3) have completed community rehabilitation, (4) able to lift his or her affected arm onto a table while seated and move one or more fingers and (5) able to consent to treatment. Patients were given a letter of invitation by stroke team members and those interested were able to contact the researcher to arrange a home visit and to discuss the research.
Participants were randomized into either the intervention group (therapeutic instrumental music performance (TIMP) followed by rest for nine weeks) or control group (waitlist followed by TIMP nine weeks later) using a computer-generated random list of numbers, managed by an independent statistician (see study consort in Figure 1).
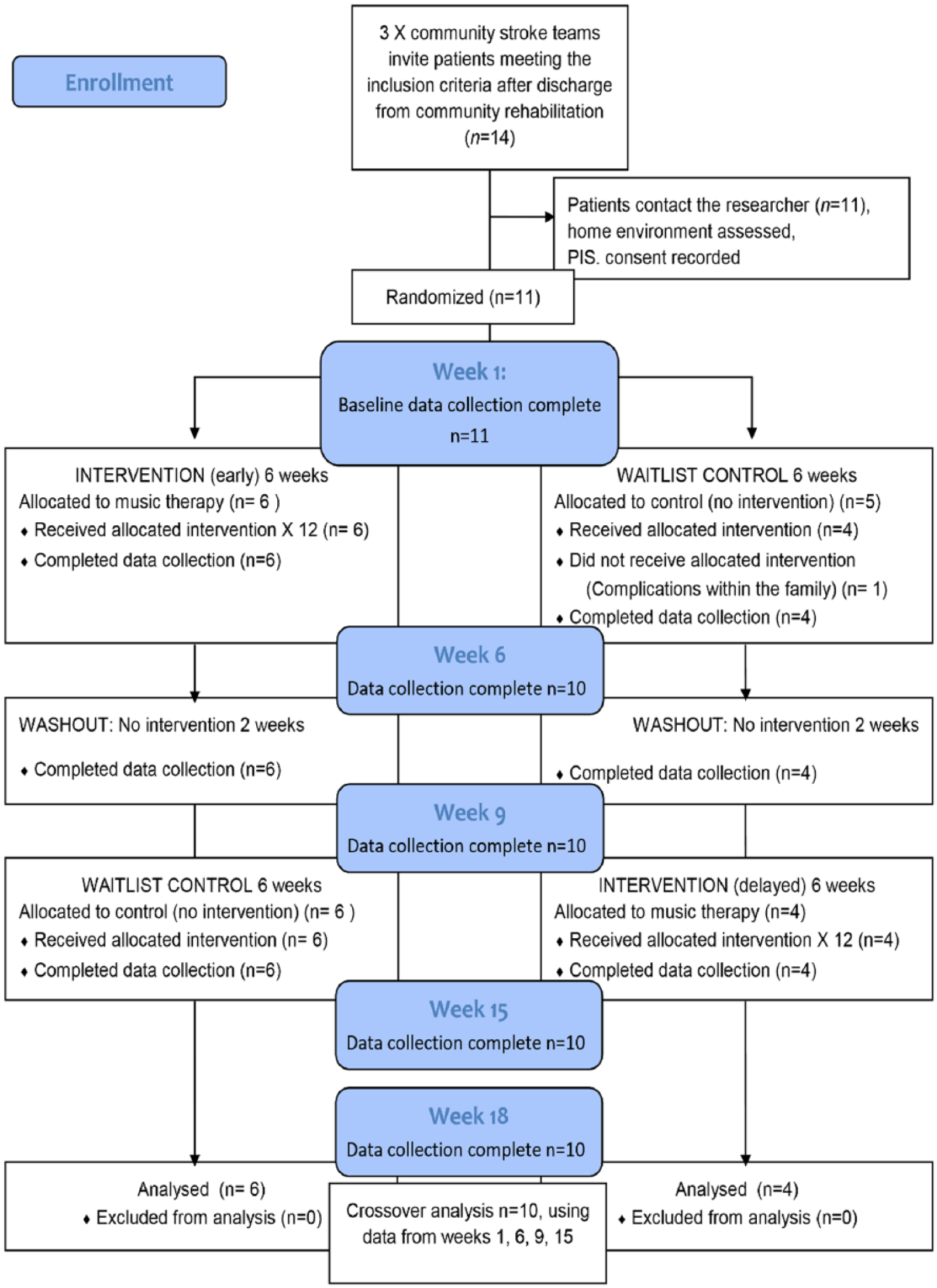
Study flow diagram. Data collection occurred at weeks 1, 6, 9, 15 and 18. Cross-over analysis required data from weeks 1, 6, 9 and 15.
Feasibility was estimated by the number of invited patients who joined the trial over the 12-month period of recruitment, attrition rates, completion of all scheduled clinical contacts and all data collection.
Pre- and postintervention data were collected by a research assistant blinded to participant allocation and study design. Additionally, brief structured interviews were conducted by the researcher/interventionist during both the pre- and postintervention periods to gather data on patients’ perceptions of the intervention, including anticipated challenges or benefits, tolerance, motivation, self-monitoring and preference, as well as any other negative or positive feedback that might guide intervention delivery. Interview questions were formulated in consultation with music therapy researchers, the manager of the rehabilitation programme hosting the study and a public research consultation group comprising members of the public and patients who volunteer to review and comment on research ideas and related documents.
The researcher documented participants’ responses in writing during the interviews, which were on average 5 minutes in duration. Data were analysed thematically by the researcher using interpretative phenomenological analysis as the coding method. 10 Commonalities between participants’ responses were first identified by carefully and repeatedly reading them through. Based on the language that was used by participants to describe preconceptions before treatment and then descriptions post treatment, themes were identified under which related responses were grouped. Preliminary findings were audited by an external music therapy researcher with a sample of data. Superordinate themes were established, from which subthemes were then extracted.
Data on changes in arm function were collected using the Action Research Arm Test.11,12 This measure requires a square-edged table onto which a template is placed, marking the start and end positions from where each different sized object is to be picked up and moved to, using the full range of distal, proximal and finger movement combinations. All participants were seated at the same, specific distance from the table to ensure consistent measurement of arm movements. One home without a squared edged table was adapted by clamping a wooden board onto the table surface, onto which the equipment could be correctly set up. The Nine-hole Peg Test 13 was used as a secondary outcome measure for finger dexterity. Data collection occurred pre and post intervention at weeks 1, 6, 9, 15 and 18. However, only data from the first four data collection points, up to and including week 15, were required for the cross-over analysis.
The researcher/interventionist was a trained neurologic music therapist and experienced in delivering the intervention, which occurred twice weekly for six weeks, resulting in 12 individual clinical contacts in each participant’s own home. Participants were required to play acoustic musical instruments and/or iPads with touchscreen musical instruments as part of fine motor/distal exercises for 20–30 minutes in each session. Arm movements were synchronized with accompanying, strongly pulsed musical patterns played live by the researcher on an acoustic guitar. 9 Equipment set-up time was 15 minutes.
A table of 12 motor exercises and variations with facilitating music for each exercise was developed by the researcher through collaboration with a volunteer with stroke and used throughout the study. 9 The protocol includes detailed instructions for each motor pattern, or movement/movement sequence, and a different facilitating musical pattern for each. Precise periodicity of the pulse, an essential attribute of TIMP, 8 was ensured by the use of a metronome beat audible only to the researcher through an earpiece. Each participant was assessed in the first session by the researcher to determine the most appropriate motor patterns and tempo, with the latter initially set to each participant’s current movement frequency.
For the primary outcome measures for the cross-over design using assessments at weeks 1, 6, 9 and 15, the analysis of variance approach described by Ratkowsky et al. 14 was used, with the computer software application R. The cross-over analysis does not make use of the follow-up values at week 18, because they do not contribute to the assessment of the effectiveness of music therapy in the cross-over design analysis used here.
Results
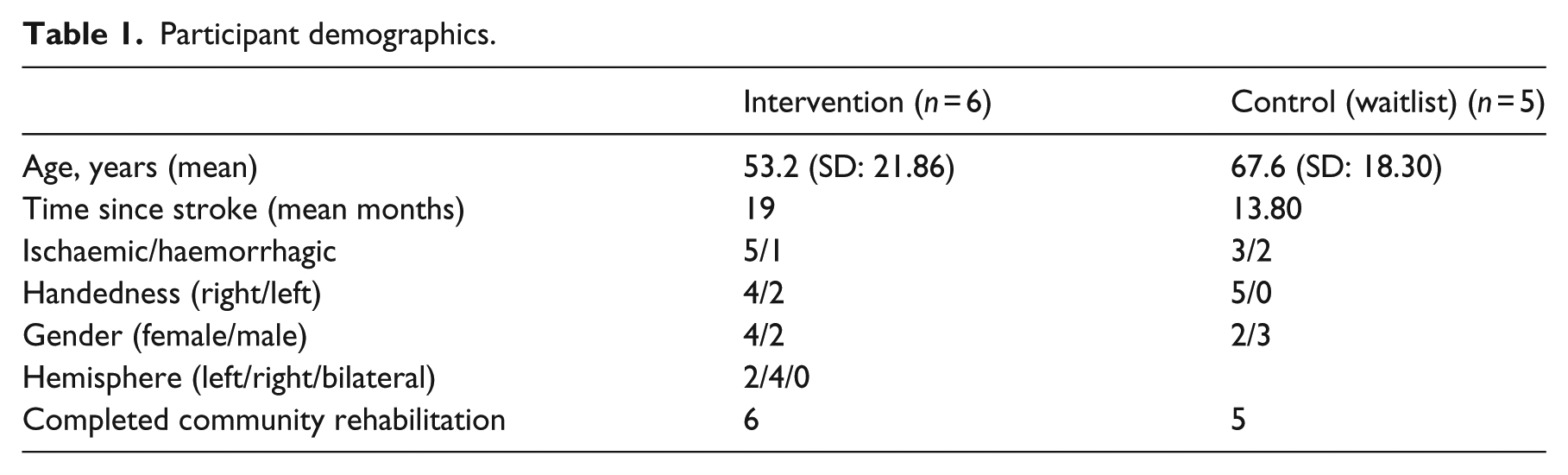
Over the recruitment period from March 2014 to March 2015, 14 patients were identified as eligible for the study from the three community stroke teams and invited to participate, of which 11 were recruited. Table 1 shows the participant demographics. The distribution of invited patients between the three teams was 13, 1 and 0, respectively. One participant withdrew for reasons unrelated to the study. Ten participants completed their 12 scheduled sessions and all data collection over 18 weeks. Participants achieved 20–30 minutes of playing in each session, not including breaks for rest, setting up and repositioning instruments.
Participant demographics.
A total of 21 subthemes emerged from thematic analysis of the structured interview data, which were further grouped into nine superordinate themes (Table 2). The findings of the qualitative analysis indicate that although participants expressed some anticipated challenges to or scepticism about engaging in the music interventions, they found it to be motivating, that the facilitating music and instruments were supportive of target arm movements and that tolerance for TIMP was high and fatigue low. The intervention was perceived potentially to be generalizable to non-musical activities of daily living, assisting movement through structure. Participants indicated that self-monitoring was used to assess change in function and reported improvement. In addition to highlighting aspects that enhanced participants’ experience, the shared, interactive nature of the activity was indicated as an important component.
Pre- and post-TIMP themes and illustrative quotes from structured interviews.
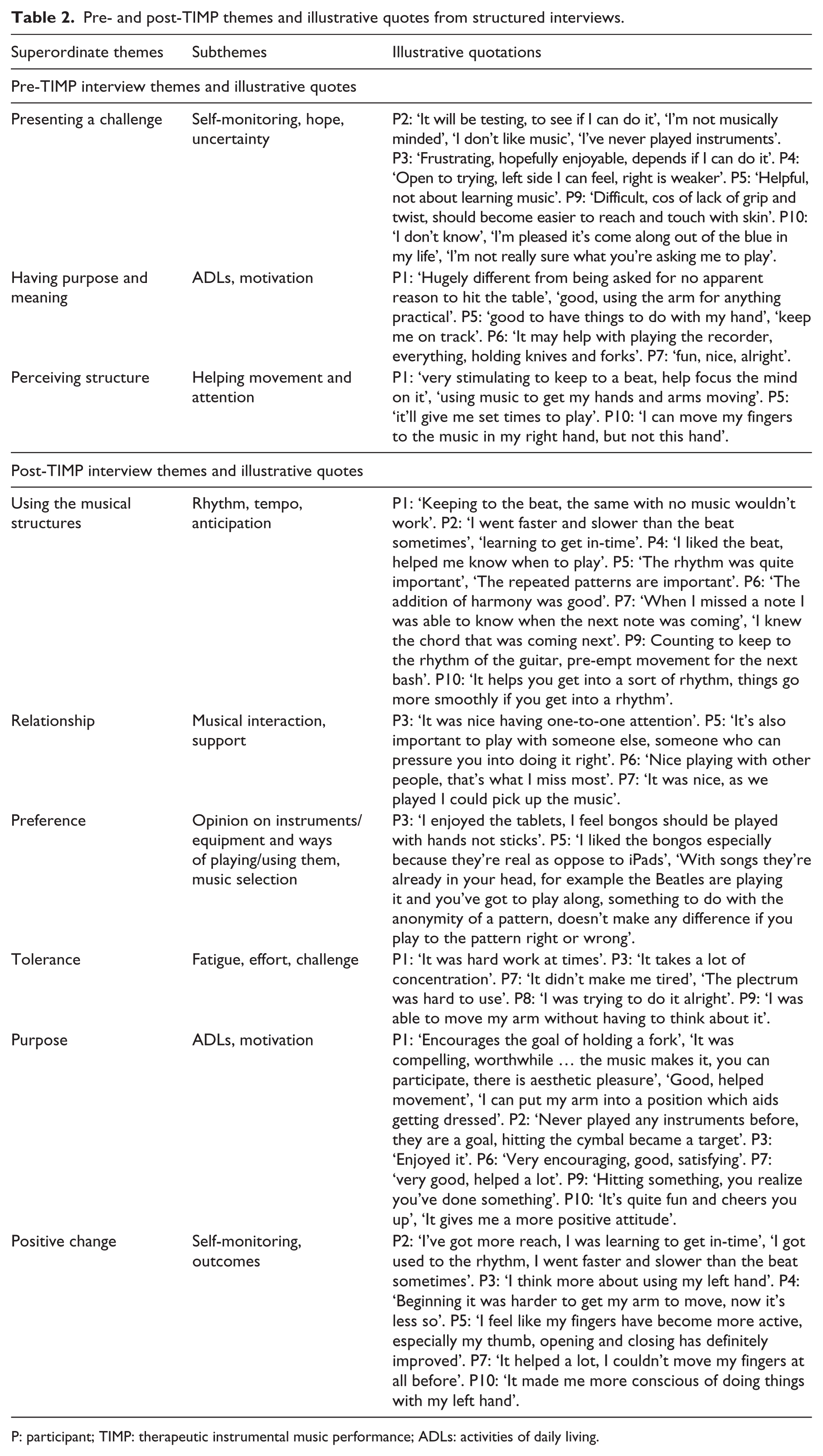
P: participant; TIMP: therapeutic instrumental music performance; ADLs: activities of daily living.
Action Research Arm Test pre- and postintervention data for both groups combined are shown in Table 3 in order that clinicians can observe whether the participants are typical of this demographic and the values are within the expected range.
Action Research Arm Test overall score pre and post intervention.
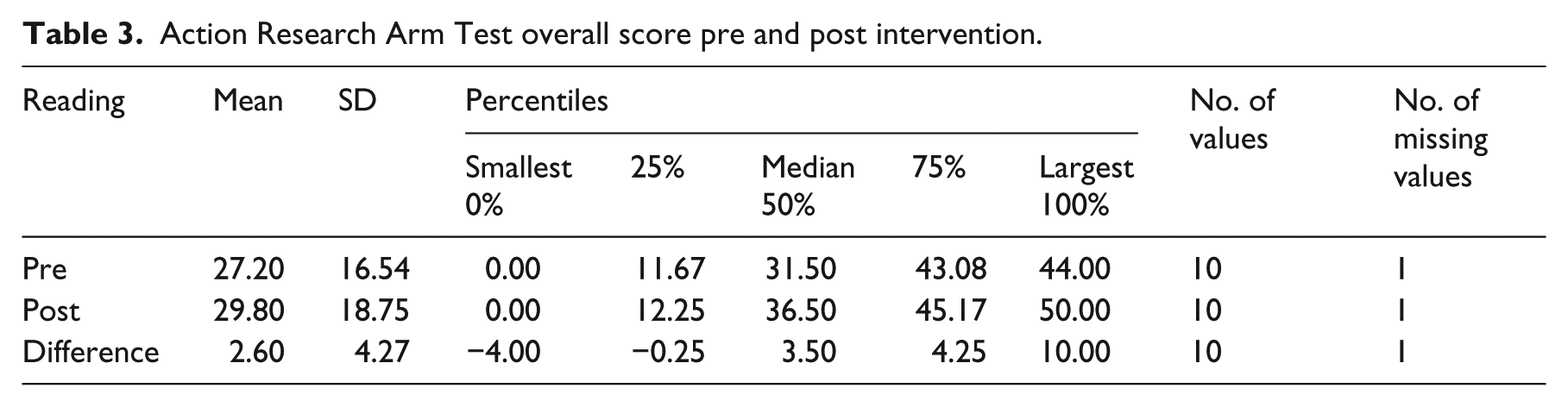
Table 4 shows the initial data descriptions for the overall Action Research Arm Test scores, with standard deviations based on within-group data rather than pooled estimates.
Continuous variables for the Action Research Arm Test by intervention type.
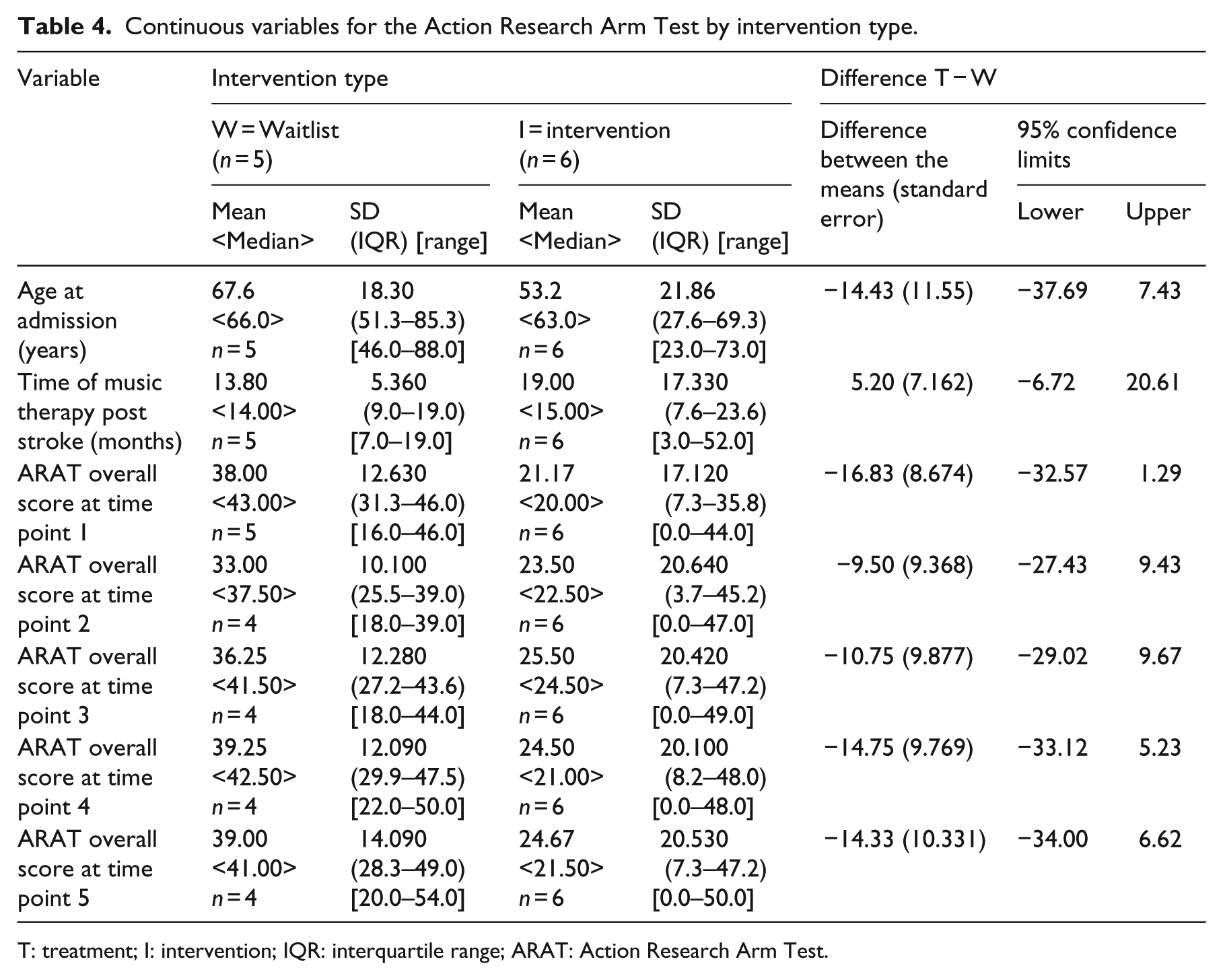
T: treatment; I: intervention; IQR: interquartile range; ARAT: Action Research Arm Test.
The overall Action Research Arm Test scores, analysed using a cross-over analysis of variance, estimate the difference between the two groups (music therapy – resting/waiting) as 1.313 (standard error 0.674, 95% confidence interval: −0.073 to 2.698).
Table 5 shows the initial data descriptions for the Nine-hole Peg Test scores. Analysed using a cross-over analysis of variance, the difference between the two groups (music therapy – resting/waiting) is estimated as 0.169 (standard error 0.823, 95% confidence interval: −1.530 to 1.867). The figures in the ‘mean’ columns for waitlist and treatment indicate mean number of pegs inserted into and removed from a board with nine holes in it (nine in and nine out again) within a maximum time limit of 2 minutes.
Continuous variables for the Nine-hole Peg Test by intervention type.
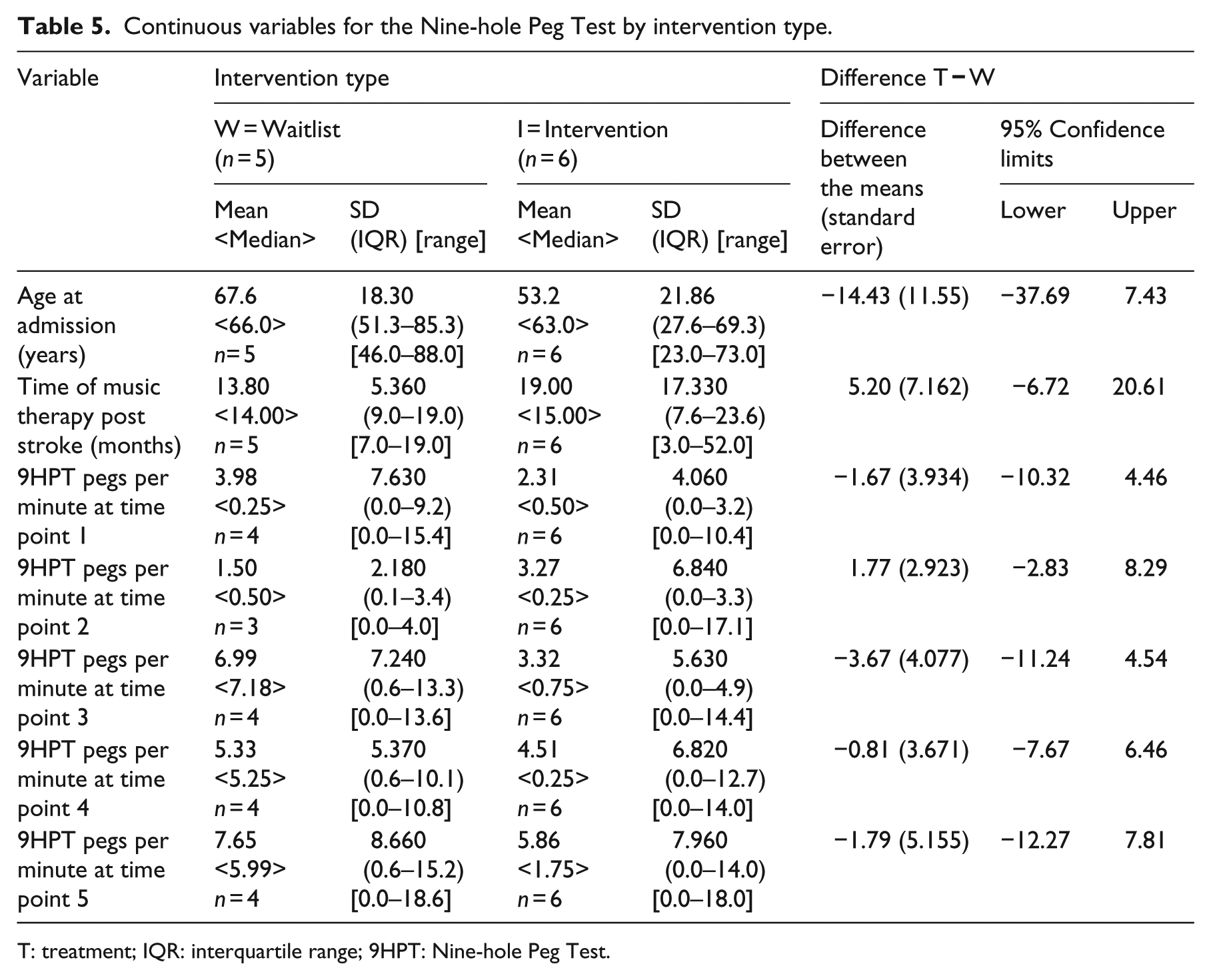
T: treatment; IQR: interquartile range; 9HPT: Nine-hole Peg Test.
Discussion
A randomized controlled trial examining the effects of TIMP on arm hemiparesis in different home environments might be feasible based on low attrition and the high levels of adherence and motivation observed and reported. However, feasibility cannot be conclusive as data were not available regarding the number of eligible patients who were discharged from the three community stroke teams over the period of recruitment. Recruitment of participants may have been positively influenced by the stage at which they were recruited, postcommunity rehabilitation, after which the alternative to participation was no intervention, or privately funded therapy. Since the interventionist conducted the structured interviews, participants may have provided responses that were skewed to the benefits of the intervention and this should be addressed for a larger study. Allocation concealment was not compromised and the data collector remained blinded. Equipment could be set up and data collected effectively in different home environments. Group comparison data from the cross-over analysis cannot be used to make any statistical inferences as the sample size was too much small.
It is not possible to conclude that a larger randomized controlled trial would be feasible as data were not available to report on the size of the recruitment pool, and data on the number of patients screened for eligibility were not collected. One of the three recruitment sites did not invite any patients to participate, while another invited only one. It is known that time constraints within all stroke teams negatively influenced recruitment rates, limiting time both to identify eligible patients and to send out letters of invitation. For a larger study, recruitment from community stroke teams during active community rehabilitation may identify potential recruits more quickly and recruit more successfully. Research assistants with honorary research contracts regularly attending multidisciplinary community stroke team meetings and with independent access to relevant patient data might also improve recruitment rate.
We acknowledge that care should be taken in interpreting adherence to treatment and low attrition in favour of the intervention, as it was delivered after discharge from community rehabilitation, at which point the alternative to participation would have been no treatment. To properly report on these factors, another randomized controlled feasibility pilot might be advisable, comparing the intervention with standard care, which might then lead to a larger, sufficiently powered trial measuring treatment effects.
The participant who dropped out of the study, completing only the first assessment, had been randomly allocated into the waitlist group, but was clearly very keen to begin treatment and possibly frustrated by the delay. The participant was also living in an unstable home environment that had limited access from community services. Providing alternative venues for treatment nearer to the participant’s home did not facilitate access to treatment delivery. Such cases present both clinicians and researchers working within community services with challenges that might remain beyond the reach of resources that are currently available and this needs to be considered within both research and clinical practice.
The variables presented by home environments did not compromise standardization of data collection, for example, with different seating and table heights. Setting up instruments in participants’ homes did not present any particular challenges. The homes visited varied considerably in size, with sessions in the smallest home taking place in the kitchen area, while one of the largest had a room reserved specifically for art and music activities. Volume levels from participants’ playing of instruments were not commented on at any point as a potential problem for neighbours, whether in terraced or detached housing. For some properties, there was no parking space available and the researcher/interventionist was required to walk along a path to the property. This makes it essential that equipment can be stored and transported in a robust case with wheels, as was the case for this study. Care needed to be taken not to wheel the case through participants’ homes to avoid marking floors and carpets. Instead, the case had to be carried through the property, or left safely by the door, and the equipment had to be unpacked and carried to the place where the session was taking place. The researcher/interventionist would advise that for a larger study, music therapists delivering the intervention should be given some guidelines to ensure that properties are treated respectfully, with equipment being transported into homes and assembled without causing damage or hazards. Some detail in this regard is provided in the published protocol. 9
Some of the qualitative data indicate that the musical interactions were motivating and enjoyable, and the nature and quality of this interaction appear to be an aspect that is unique when compared to interventions found within standard care. However, as structured interviews were conducted by the researcher/interventionist, participants may have answered more favourably in this regard.
The protocol of exercises and facilitating music designed for this study 9 and the published guidelines 8 for the intervention cannot eliminate all variables. Compared to previous, similar research,5,6 the main variable is presented by the music therapist providing live, facilitating music for movement synchronization. For a larger TIMP study, more interventionists would need to be trained in delivering the protocol. Variations between interventionists, for example, the musical instruments used for accompaniment or how the therapist emphasizes the pulse or manipulates other musical elements to support movement synchronization, cannot all be controlled for. What effect this might have on response to treatment is not known, but it has been suggested that these variable elements may enhance engagement and functional outcomes. 7 Before conducting a larger trial, the feasibility of different music therapists delivering the protocol would need to be established.
For the cross-over analysis, data from only four time points were required to estimate the effectiveness of music therapy. The fifth data collection point is part of the overall data description, collected to observe for any changes in the waitlist group post intervention and washout. Statistical inferences cannot be made based on any of the data collected or the cross-over analysis from this study, as the sample was too much small. A calculation for a larger study could be made based on data from a larger arm rehabilitation trial that used the same outcome measures. 6
Determining appropriate, effective and acceptable rehabilitation interventions that can be delivered in home environments is of particular importance given the changes in healthcare delivery from hospital to home settings.2,4 Some participants in this study were able to associate the movements required to play through the exercises with activities of daily living, which possibly enhanced their adherence and focus. Performing the exercises in their homes may have helped with this, as they were surrounded by familiar materials and objects that they recognized as part of their everyday lives and understood the need to interact with them with improved precision and dexterity to optimize their independence. Treatments caused minimal disruption to daily routines since they did not require participants to leave their homes to receive them, and this may have increased compliance. 1 These contextual and motivational variables combined with an intervention that facilitated high repetition of target movements warrant further investigation to determine quantitative patient benefits. Data collected on quality of life and an economic evaluation of treatment would be a useful addition to a future study, meeting current recommendation for research of this nature. 7
Clinical Messages
Therapeutic Instrumental Music Performance using the Action Research Arm Test to measure responses is feasible in different home environments
Treatment adherence twice weekly for six weeks suggests that the intervention may be motivating, possibly supporting high repetition of target movements
Footnotes
Acknowledgements
The authors would like to thank Cambridgeshire Community Services National Health Service Trust and their three community stroke teams for hosting this research and facilitating recruitment. The trust also funded some of the data collection, for which the authors extremely grateful. Special thanks to Liz Chapman for collecting data. A.J.S. was responsible for obtaining ethical approval, participant consent, literature review, accurately reporting the methodology and results, thematic analysis and writing the discussion. A.B. facilitated the study. W.L.M., A.B., J.F. and H.O.-M. contributed with suggestions for the whole text. H.O.-M., J.F., W.L.M. and A.B. contributed to the study design. W.L.M. contributed to the thematic analysis. M.P. performed all statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.