
Abstract
Objective
Three-phase graded motor imagery (limb laterality, explicit motor imagery, and mirror therapy) has been successful in chronic pain populations. However, when applied to phantom limb pain, an amputation-related pain, investigations often use mirror therapy alone. We aimed to explore evidence for graded motor imagery and its phases to treat phantom limb pain.
Data Sources
A scoping review was conducted following the JBI Manual of Synthesis and Preferred Reporting Items for Systematic Review and Meta-Analyses extension for Scoping Reviews. Thirteen databases, registers, and websites were searched.
Review Methods
Published works on any date prior to the search (August 2023) were included that involved one or more graded motor imagery phases for participants ages 18+ with amputation and phantom limb pain. Extracted data included study characteristics, participant demographics, treatment characteristics, and outcomes.
Results
Sixty-one works were included representing 19 countries. Most were uncontrolled studies (31%). Many participants were male (75%) and had unilateral amputations (90%) of varying levels, causes, and duration. Most works examined one treatment phase (92%), most often mirror therapy (84%). Few works (3%) reported three-phase intervention. Dosing was inconsistent across studies. The most measured outcome was pain intensity (95%).
Conclusion
Despite the success of three-phase graded motor imagery in other pain populations, phantom limb pain research focuses on mirror therapy, largely ignoring other phases. Participant demographics varied, making comparisons difficult. Future work should evaluate graded motor imagery effects and indicators of patient success. The represented countries indicate that graded motor imagery phases are implemented internationally, so future work could have a widespread impact.
Introduction
Phantom limb pain after amputation is complex and multifactorial. The mechanisms contributing to this type of pain are not fully understood, making it difficult to treat and clinically manage.1,2 One mechanistic theory of phantom limb pain is maladaptive plasticity wherein cortical reorganization occurs due to the loss of or changes in sensory and motor input from the amputated limb. 3 Neuroimaging evidence shows that individuals with amputations can experience changes in the sensory and motor maps in the cortex of the brain, which may contribute to the pain experience.3,4
Graded motor imagery is a non-pharmacological treatment that aims to address hypothesized cortical reorganization associated with chronic pain.5,6 Graded motor imagery has shown success in reducing other types of chronic pain and restoring function.7–13 Traditional graded motor imagery protocol includes the three phases of (1) left/right discrimination of limbs or limb laterality, (2) explicit motor imagery, and (3) mirror therapy. 6 In limb laterality, patients are shown images of limbs in different orientations and asked to judge whether the image depicts a left or a right limb. 14 In the second phase of graded motor imagery, explicit motor imagery involves imagined movements without physically moving the body or activating the muscle. Visualizing these movements can activate similar cortical areas as are activated when physically performing the movements. 15 In the third and last phase, mirror therapy, a long mirror or mirror box is traditionally placed between the two limbs, so that the contralateral limb is reflected in the mirror and the painful limb is out of view. When looking in the mirror, the patient receives visual feedback of both limbs moving together pain-free. 16 Graded motor imagery is designed to progress the patient's experience through each of these phases to gradually increase the sensory-motor feedback to the brain. However, treatment can also involve just one phase of graded motor imagery, and there is debate amongst clinicians as to the protocol that constitutes best practice.5,17,18
Mirror therapy has been reported often in individuals with phantom limb pain, and the evidence for mirror therapy has been evaluated in recent systematic reviews.19–21 However, mirror therapy represents just one of three phases of graded motor imagery intervention. The three-phase graded motor imagery protocol may provide more pain relief, but little is known about the evidence supporting the three phases of graded motor imagery as they relate to amputation. Therefore, in order to provide an overview of the current research landscape, a scoping review of the current literature on the three phases of graded motor imagery is warranted. The objective of this scoping review is to explore and describe the extent and type of evidence of three-phase graded motor imagery and its individual phases for phantom limb pain after limb amputation.
Methods
Although three-phase graded motor imagery was originally designed and tested in individuals with phantom limb pain, 9 most published works since then have focused on mirror therapy.20,21 To better understand how others have used the phases of graded motor imagery either in isolation or combination and describe key concepts (e.g. dosing, individual characteristics, etc.), we used scoping review methodology to capture the current landscape of research on this topic. Consistent with a scoping review, there is no intent to analyze the effectiveness of treatment.22,23 Instead, this project was designed to explore participant demographics, treatment protocols (i.e. phases, session structure, and dosing), amputation-specific modifications, and outcome measures to inform future intervention and study design.
This scoping review was conducted according to the JBI Manual for Evidence Synthesis and is being reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses extension for Scoping Reviews guidelines.24,25 The protocol, covering the objectives, inclusion/exclusion criteria, and methods of this scoping review, was registered with the Open Science Framework (https://osf.io/jra9t/) prior to the start of the study.
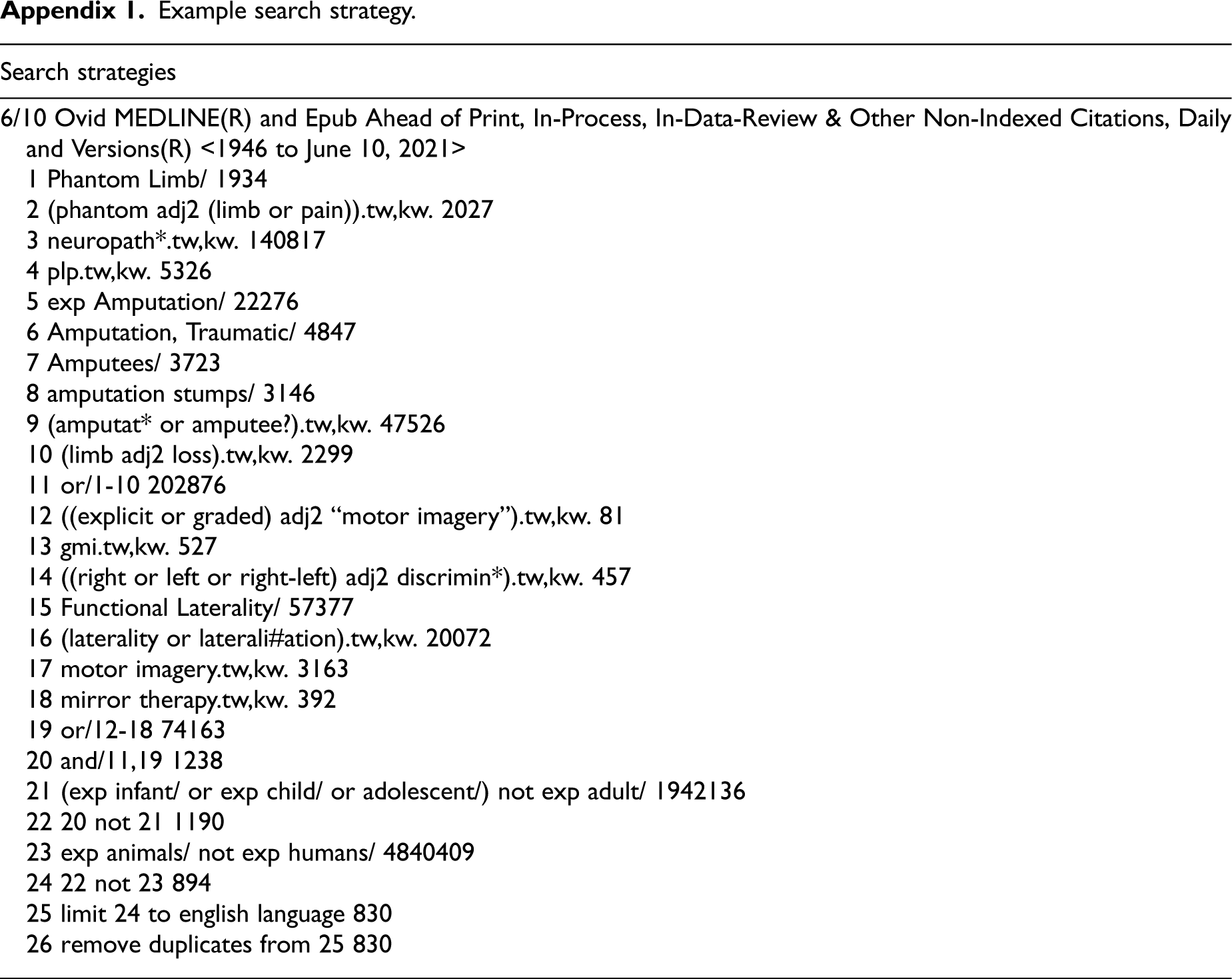
A comprehensive search strategy was created using both natural language (i.e. keywords) and controlled vocabulary (i.e. subject headings) to examine the phases of graded motor imagery. Initial searches were conducted by D.H. from March to June 2021 and were repeated in December 2022 and August 2023. The search strategy was executed across the following databases, registers, and websites: Medical Literature Analysis and Retrieval System Online, Embase, and American Psychological Association PsycInfo (all via Ovid), Cumulative Index to Nursing and Allied Health Literature, ClinicalTrials.gov, the Cochrane Library (via Wiley), Scopus, SportDiscus, Physiotherapy Evidence Database (pedro.org.au/), Occupational Therapy Search, African Journals Online (www.ajol.info), Latin American and Caribbean Health Sciences Literature (lilacs.bvsalud.org/en/), and the World Health Organization International Clinical Trials Registry Platform (trialsearch.who.int/). Filters were used to limit retrieval to studies published in English but not by publication date. The decision not to restrict the search based on publication date was due to the original graded motor imagery work being published in 2006, so no works eligible for this review were expected previous to this date. 9 In accordance with Preferred Reporting Items for Systematic Review and Meta-Analyses guidelines, the full search strategy for one database can be found in Appendix 1. 25 The entire search strategy, including updates, employed for this review can be found on the Open Science Framework (https://osf.io/jra9t/).
Studies were included in this scoping review if the study design involved one or more phases of graded motor imagery for participants over the age of 18 with phantom limb pain due to amputation. Peer-reviewed publications, published conference abstracts, letters to the editor, and similar works were considered for inclusion. Works that may have not gone through a review process, also known as grey literature, were included since the intent of this scoping review was to describe the extent of current evidence and not evaluate the quality of evidence. In the case of clinical trials without an attached publication, authors were contacted in an attempt to gather additional information and obtain any published results. Literature reviews and retrospective analyses of previously published works were excluded, as were published conference abstracts that preceded included peer-reviewed publications in an attempt to eliminate duplicate information. Studies that included participants under the age of 18 were excluded as there is a potential that the mechanisms of pain in pediatric participants differ from those in adults, making comparisons between these groups difficult. 26 Similarly, studies that included participants with phantom limb pain resulting from etiologies other than amputation (e.g. brachial plexus avulsions and complex regional pain syndrome) were excluded from synthesis to design a homogeneous population for this scoping review, unless the work explicitly reported demographic information and results separately for the participants with amputations.
The title and abstract of each work were reviewed for inclusion independently by two authors (KF and HP) based on the criteria listed above. Conflicts in the screening decisions were resolved by a third author (RV). The full text of the remaining items was then reviewed by two authors (KF and HP) to determine final inclusion, and any conflicts were again resolved by a third author (RV). The blinded screening was performed in Rayyan (https://www.rayyan.ai).
Data were extracted from each article independently by two authors (KF and HP). A spreadsheet specifically created for this study for recording data was piloted prior to full data extraction. Each of the two authors recorded data in a separate spreadsheet. The two authors then compared the extracted data and attempted to resolve any conflicts through discussion. Any remaining conflicts after this discussion were resolved by a third author (TR).
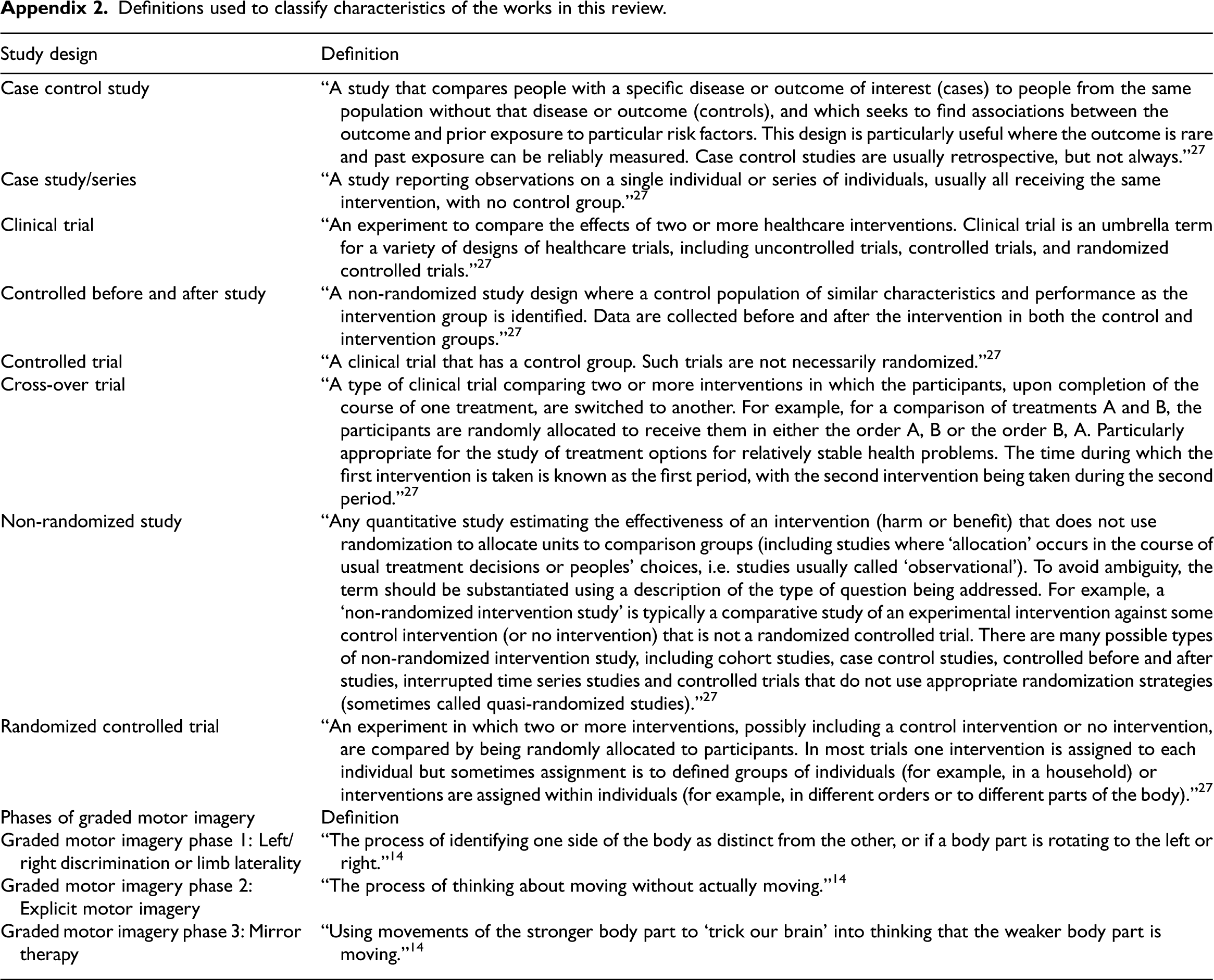
The following data were extracted from each of the included articles: citation information, type of publication, study design, country of study, participant demographics, amputation characteristics (i.e. level of amputation, unilateral or bilateral amputations, cause of amputation, and time since amputation), use of prostheses, use of medications, authors’ definition of acute and/or chronic pain, graded motor imagery phase (i.e. limb laterality, explicit motor imagery, and mirror therapy), dosing of treatment, outcomes studied, outcome measures used, binary report of results (i.e. positive or negative results), and protocol on which the work was based. Working definitions of the study designs were adapted from the Cochrane Collaboration 27 and are listed in Appendix 2 with working definitions of graded motor imagery phases and related approaches. Any data that were not reported from these categories were recorded in the spreadsheet.
The extracted data were reviewed to examine similarities and differences between the included works. In particular, comparisons of the participant characteristics, the features of the interventions, and the outcomes measured were examined. This review involved both quantitative methods through frequency counts as well as qualitative methods through overall similarities.
Results
The searches yielded 3028 unique records. Duplicates were identified and removed using Rayyan, leaving 1763 works to be screened based on titles and abstracts. During this screening, 1791 works were excluded, resulting in 151 works for full-text screening. Of those, 61 works fit our inclusion criteria and are included in this review (Figure 1). Six authors were contacted by email to inquire about results from their clinical trials that were not able to be located through publication searches. Three authors responded to the inquiry but had no additional results to share, keeping the final number of works in this review to 61.
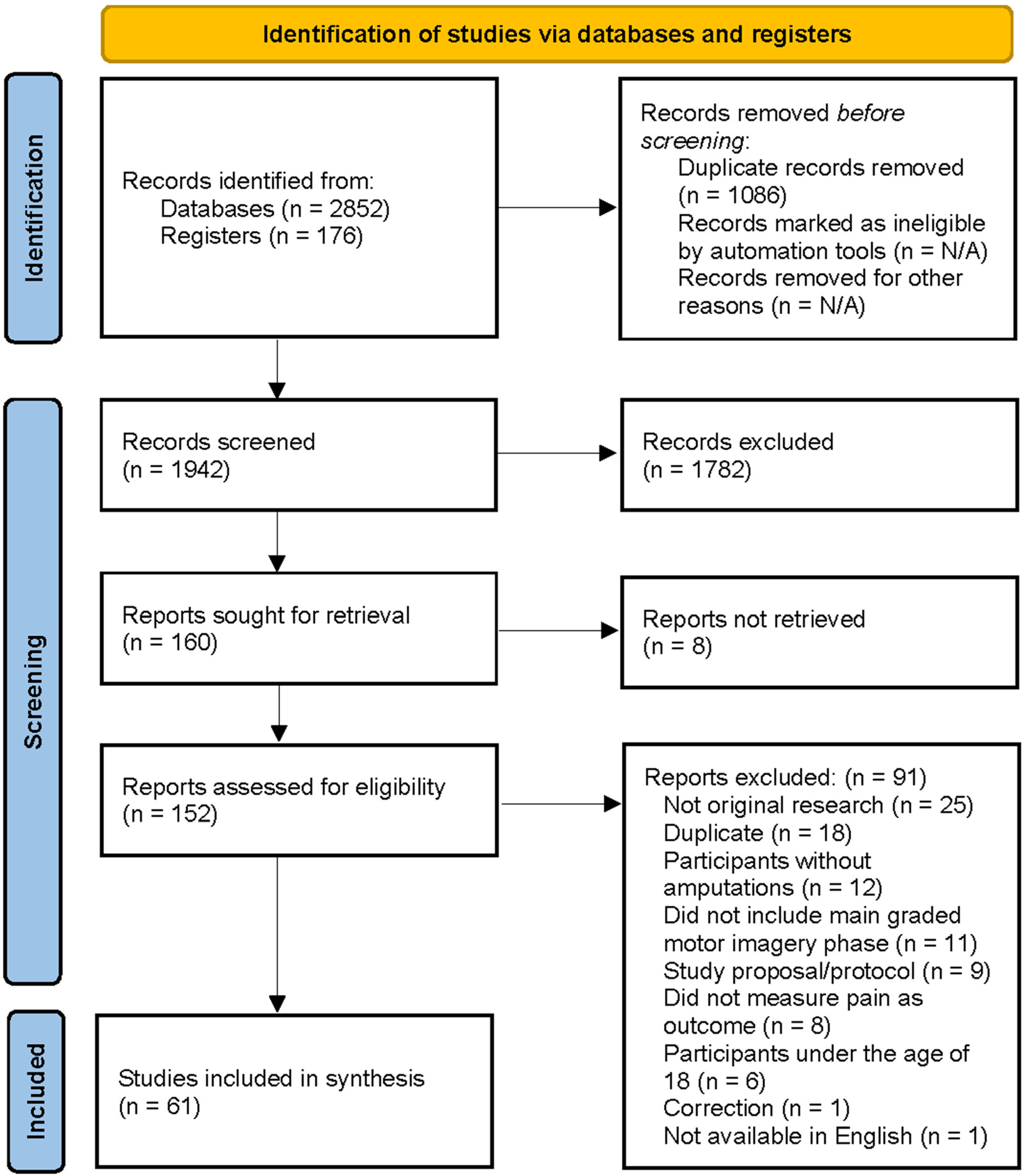
Preferred reporting items for systematic review and meta-analyses diagram of inclusion and exclusion process.
The characteristics of the works included in this review are shown in Figure 2A and B. Looking at the timeline and scope of interest, all works were published between 2007 and 2023 (Figure 3) and were conducted in 19 countries (Appendix 3).
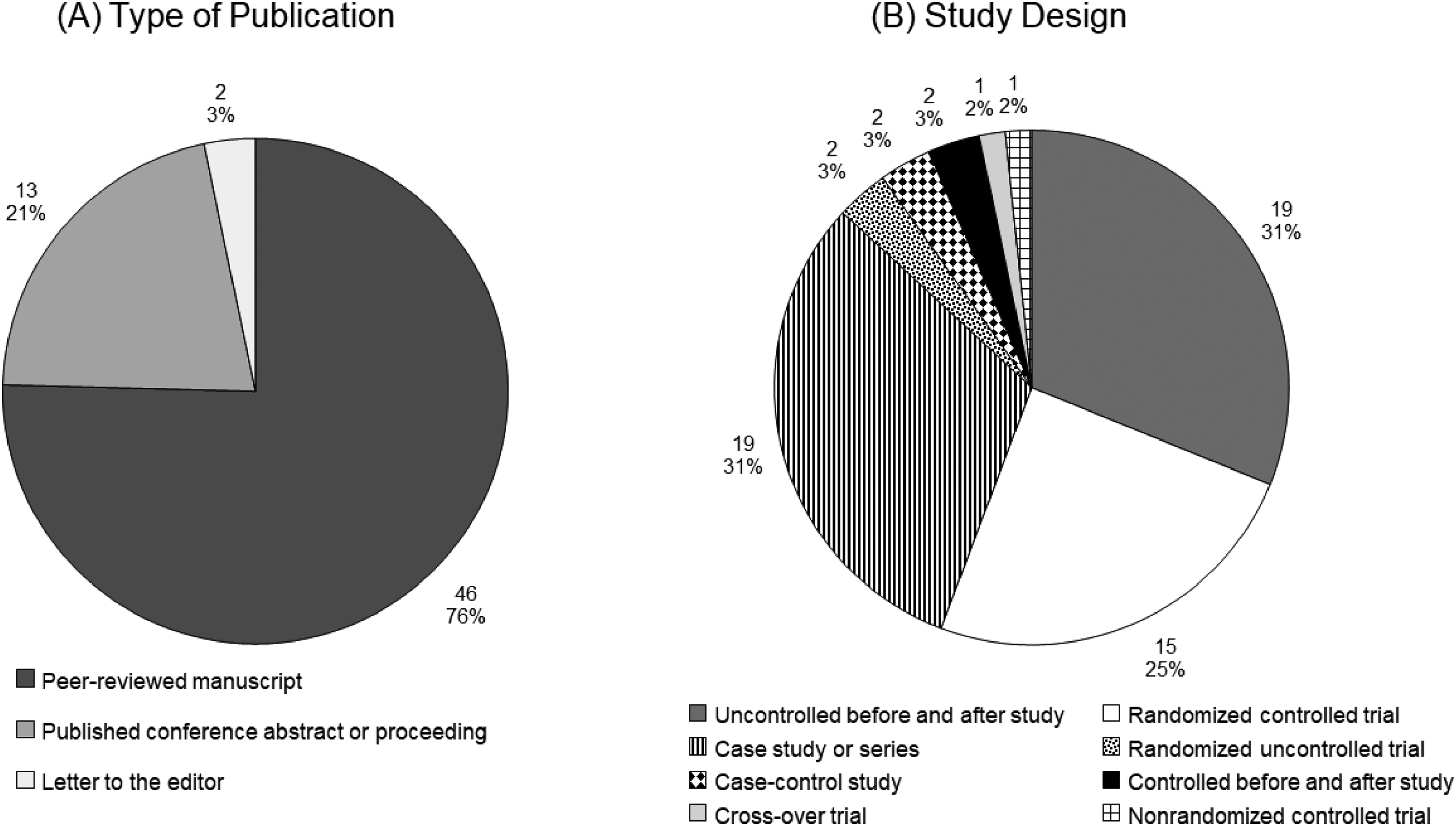
Characteristics of included works (n = 61) including (A) type of publication and (B) study design.
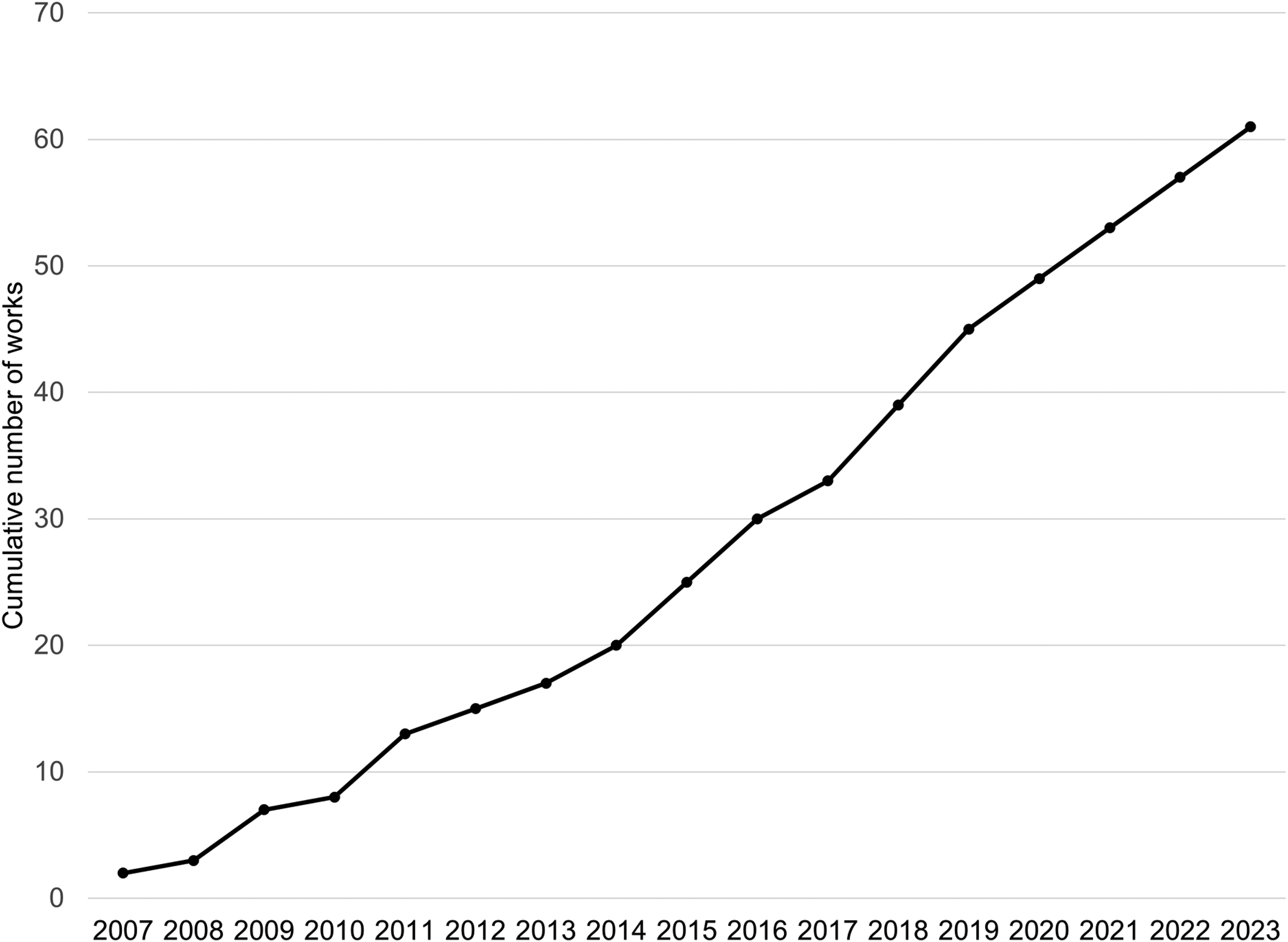
Cumulative works on graded motor imagery phases (limb laterality, explicit motor imagery, or mirror therapy) for phantom limb pain per year (n = 61).
The number of participants included in these works ranged from 1 to 112 participants with a median of 10 participants.28,29 Of the works reporting the sex or gender of participants (85%), there were combined totals of 772 male and 257 female participants.28–80 In 84% of works, no information about the race or ethnicity of participants was reported.28–32,35–48,50,52–60,63–65,67–69,71–74,77–88 Some works included participants within a narrow age range (e.g. 20–30 years old 37 ), while others used a wide age range (e.g. 20–83 years old 31 ), and 36% did not report the age range of participants.28,32,36,41,49,50,53,55,59,62,72,77,80–89 Most works included participants with unilateral amputations.28–36,38–53,56,57,59,61–72,74–81,83–90 In works where participants were bilateral amputations were included, modifications were made to the graded motor imagery protocol to make the intervention feasible without an intact limb.37,54,55,58,60,73 Twenty-four works (39%) reported focusing on participants with amputations due to non-dysvascular causes (e.g. trauma, cancer, and congenital limb differences),28–30,35,38,40,42–44,46,48,57,58,60,64,65,67–71,75,78,79 but many authors (33%) did not report the causes of amputation for their participants.37,47,49,51–54,56,59,61,76,81–89 Information about the level of amputation, time since amputation, prosthesis use, and medication use of participants is summarized in Figure 4A to D.
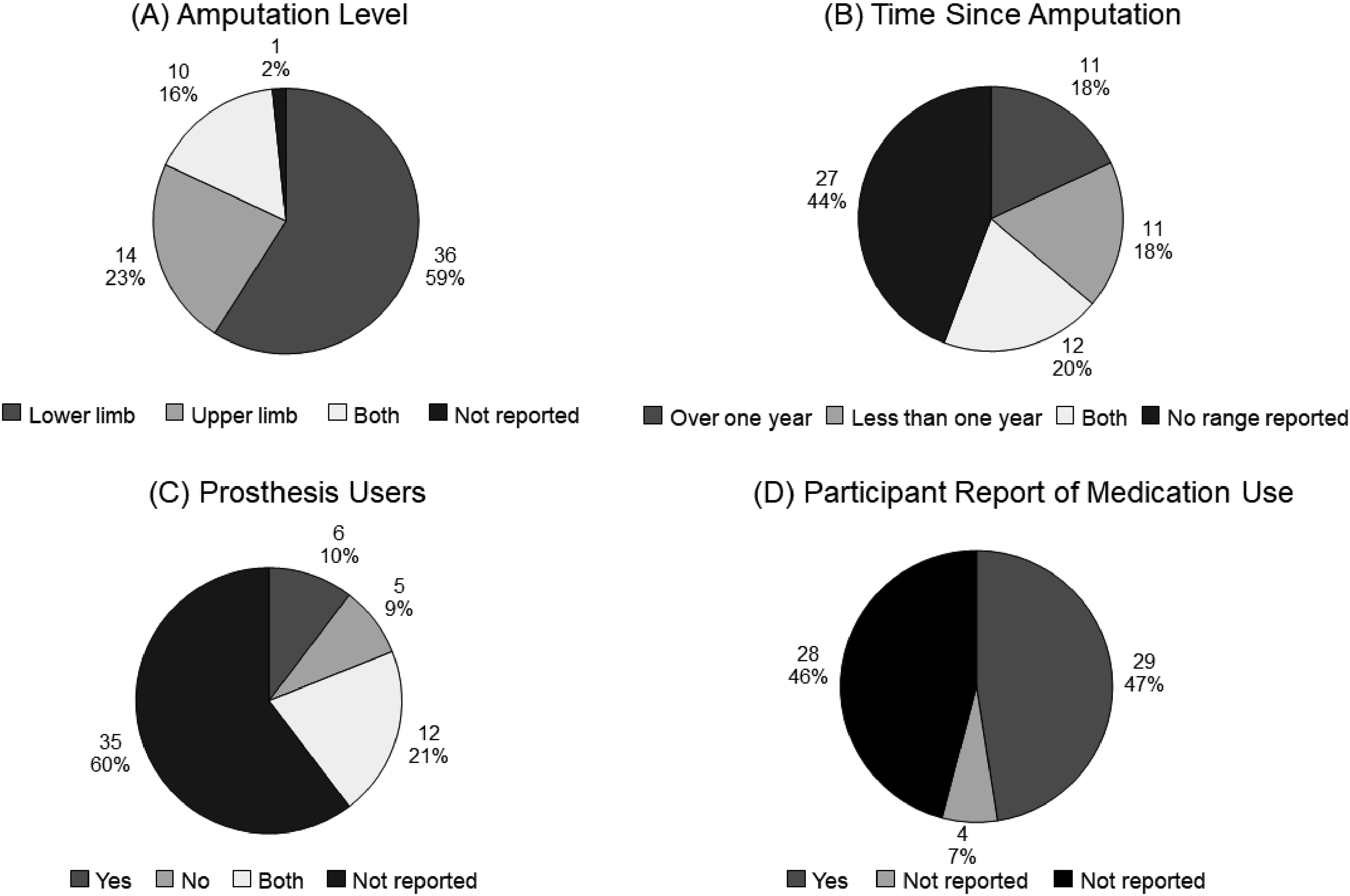
Characteristics of participants in included works (n = 61) including (A) level of amputation, (B) time since amputation, (C) participant use of a prosthesis, and (D) participant report of taking medications.
Three of the works (5%) stated their target population was participants with acute pain,39,73,75 six of the works (10%) aimed to exclusively include participants with chronic pain,28,35,45,49,50,52 and one of the works (2%) included participants with both acute and chronic pain as two separate groups. 33 Authors’ definitions of acute pain ranged from less than 48 hours 33 to less than eight weeks 39 since amputation, and authors’ definitions of chronic pain ranged from more than six weeks 33 to more than two years 45 since amputation.
Fifty-six works (92%) used only one of the phases of graded motor imagery,28–35,37–43,45–60,74,76–80,82–85,87,89 and only two works (3%) used all three graded motor imagery phases.36,86 Figure 5 summarizes the number of works using each phase. Most works (84%) used the mirror therapy phase of graded motor imagery, with 75% using traditional mirror therapy28,29,31,33–36,38–45,49,50,52,53,56,57,59,63–65,67–75,77–89 and 11% using virtual reality as mirror therapy.47,50,51,60,61,76 A detailed list of the graded motor imagery phases used in the individual works is shown in Appendix 4.
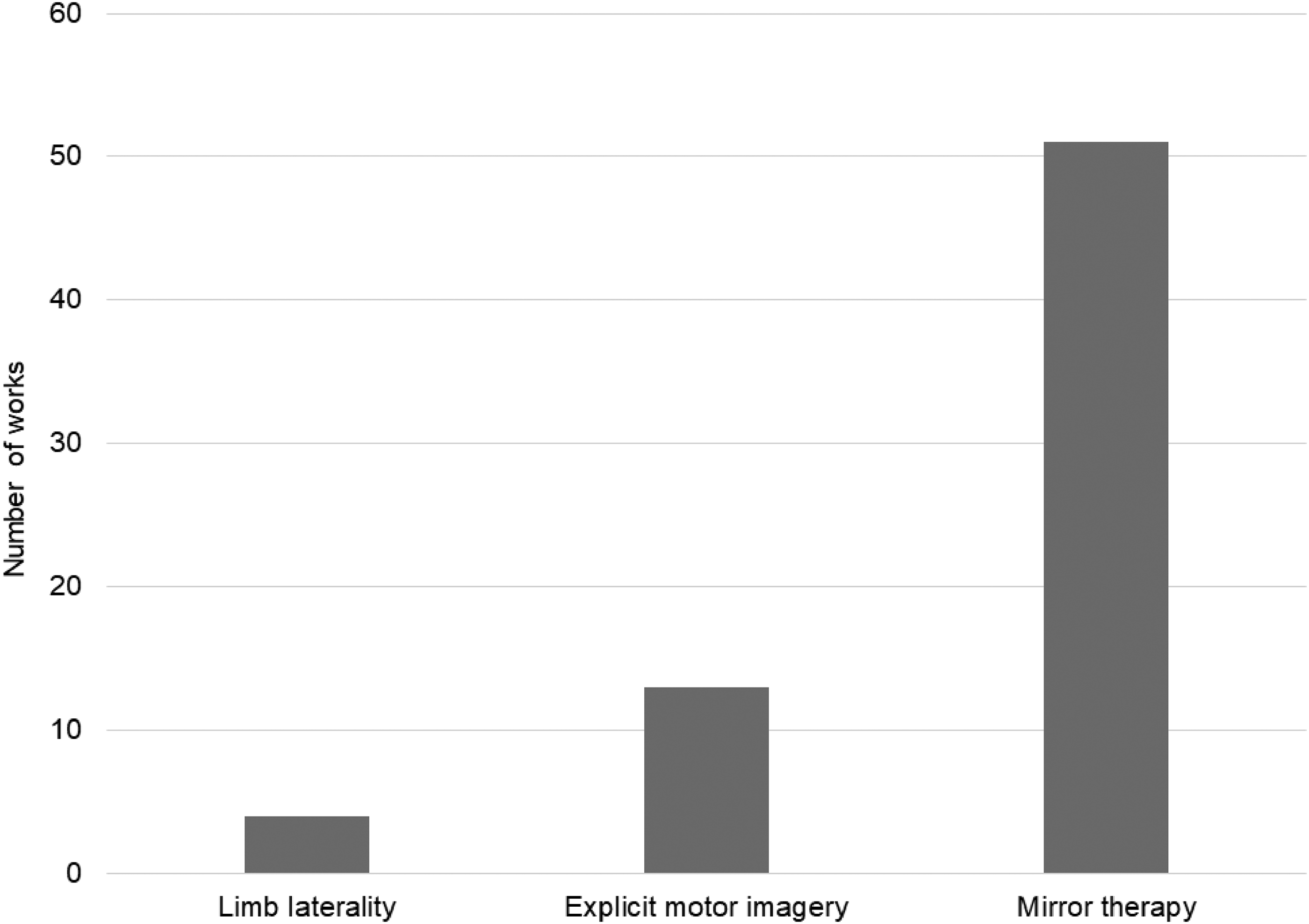
A number of works using limb laterality, explicit motor imagery, and mirror therapy.
The frequency of the treatment sessions ranged from one session per month 47 to 12 sessions per day, 36 with 15% not reporting session frequency.37,49–51,57,85,86 The number of total weeks of treatment ranged from one31,34,38,40,55,75,89 to 24, 87 with 10% not reporting total length of treatment.29,51,57,60,68,69,85 Some works reported a wide range of treatment sessions for different participants; for example, one work reported using between one and 28 sessions. 51 Additionally, some works allowed a wide range for the duration of sessions; for example, one work reported sessions lasting between 4 and 60 minutes. 51 See Figure 6A to C for a summary of the characteristics of the sessions.
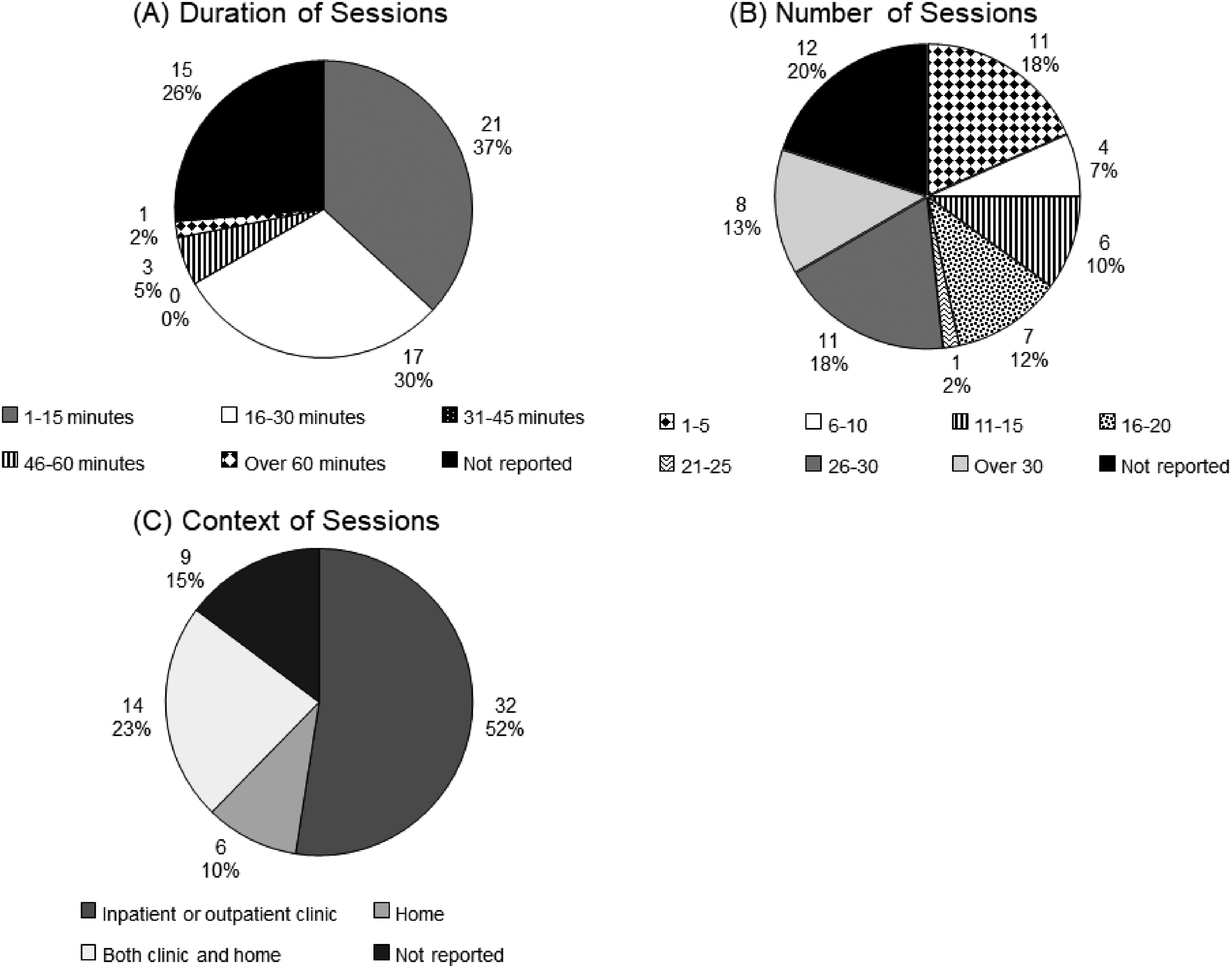
Characteristics of graded motor imagery sessions in included works (n = 61) including (A) duration of sessions, (B) total number of sessions in the program, and (C) context of sessions. Four works used treatment sessions that varied by more than 15 minutes and were unable to be classified into a duration category, so these were omitted from this section (n = 57). The number of sessions used by one work varied from 1 to 28 sessions, so this was unable to be categorized and was omitted from this section (n = 60).
Graded motor imagery sessions were led by physical therapists (20%),28,32,35,36,46,52,53,65,67,72,77,78 research staff (11%),31,33,34,43,44,54,66 unspecified “therapists” (8%),30,45,48,50,74 nurses (5%),39,41,71 and occupational therapists (3%),33,65 although 52% of works did not report the background of the individual leading the graded motor imagery.29,37,38,40,42,47,49,51,55–62,68–70,73,76,79,80–89,91 Although not the primary focus of this scoping review, adjunct therapies such as phantom motor execution, noninvasive brain stimulation, and sensory retraining were paired with graded motor imagery in 36 works (59%). See the full data extraction table for a complete list of adjunct therapies used (Supplemental Appendix 5).
Four works (7%) mentioned that their protocol was adapted from previous work32,38,65,77; these protocols were informed by the work of Ramachandran et al., 92 Ülger et al., 93 Brodie et al., 94 and Siedel et al. 95 Five works (8%) incorporated amputation-specific modifications in their protocols. Examples of amputation-specific modifications include the work of Schmalzl et al. 38 who reported a “stump mapping” component to their program. Brunelli et al. 32 asked participants to describe the position of the phantom limb at the beginning of the treatment session, and participants were asked to place their contralateral limb in the same position. The treatment exercises then began by attempting to move both limbs away from this position. Tung et al. 54 included participants with bilateral amputations, and instead of mirror therapy, the authors asked the participants to observe the limb movements of a research staff member while attempting to follow these movements with their phantom limb. In a study by Rutledge et al., 51 the virtual reality environment involved pedaling with their lower limb prosthesis for a simulated biking experience. Oouchida and Izumi 60 used “imitation training” in which a research staff member recorded movements of their own leg, and the participant then watched these recorded movements while imitating them.
The most common outcomes measured in the included works were phantom limb pain intensity (95%),28–48,50–54,56–60,66,75–81,83–87,89 phantom limb pain frequency (16%),32,33,46,47,50,54–56,81,84 phantom limb pain duration (16%),32,33,47,50,54,56,77,81,84,85 and pain interference (13%).36,49–51,59,64,76,88 Most commonly used outcome measures were the visual analog scale for phantom limb pain (48%),28–31,33,35,37,38,40,42,44,45,50,52,53,56,57,59,64,70,72,79,81,82,85–89 numeric rating scale for phantom limb pain (33%),39,41,43,46–48,50,51,54,61,62,65,67,69,71,73,75,78,80 Brief Pain Inventory (11%),32,33,36,39,59,76,77 and Short-form McGill Pain Questionnaire (8%).37,39,54,77,78 See the full data extraction table for a complete list of outcomes and outcome measures (Supplemental Appendix 5). Positive results through a reduction in phantom limb pain after graded motor imagery intervention were reported in 89% of works.29,30,32–39,41–46,48,50–60,62,64–74,76–88
Discussion
The objective of this scoping review was to explore and describe the extent and type of evidence of three-phase graded motor imagery (i.e. limb laterality, explicit motor imagery, and mirror therapy), and its individual phases for phantom limb pain. The majority of works used only a single phase of graded motor imagery, even though the three-phase graded motor imagery protocol has shown positive effects in other chronic pain populations.7,12,13 It is possible that progressing systematically through the three phases would provide more or longer-lasting pain reduction for individuals with phantom limb pain than only using one phase, but there is not enough evidence to support or refute this idea. Only two works in this review evaluated the three-phase protocol as an intervention for phantom limb pain, one of which is a published conference abstract that does not have a subsequently published full manuscript.36,86 Although both works reported positive results through a reduction in phantom limb pain intensity, additional research is necessary through larger studies to inform the interpretation of this early pilot work.
Most works in this review focused on mirror therapy, perhaps indicating that mirror therapy is the phase of graded motor imagery with the greatest familiarity or the most interest. Recently, four systematic reviews have been conducted on mirror therapy treatment for phantom limb pain, and all four reviews reported insufficient evidence to support the use of mirror therapy.20,21,96,97 However, our scoping review identified 24 works that were not evaluated in these four systematic reviews. This suggests that there may not be sufficient high-level evidence in the form of well-designed randomized controlled trials with adequate sample sizes to draw meaningful conclusions supporting or contradicting the use of mirror therapy. Additionally, these systematic reviews on mirror therapy for phantom limb pain found inconsistency in dosing among the reviewed studies, which is supported by the results found in this scoping review.
The variation in treatment protocols indicates that no standardization or established best practice exists for these interventions for phantom limb pain after amputation. There were differences between works in this review regarding the specific dosing of the interventions in terms of the frequency, duration, and total number of sessions (Figure 6A to C). There may not be a standard protocol that works for most patients in this population with phantom limb pain following amputation, and the ideal program may be tailored to each individual. A recent Delphi study surveyed clinicians about mirror therapy practices and found no consensus on the frequency or duration of mirror therapy sessions. 98 The authors of this Delphi study suggested that the ideal treatment dosing and setting may depend on the patient's presentation. 98 For example, in a retrospective analysis, Griffin et al. 90 found that the number of mirror therapy sessions necessary to provide phantom limb pain relief was associated with baseline pain intensity, with higher intensity of baseline pain requiring a greater number of sessions.
In addition to variation in treatment protocols in these works, there was also variation in the demographics and characteristics of the study participants (Figure 4A to D), with much information unreported. Overall, the total number of participants included in these works was heavily skewed towards males (75%). This is relevant since prior evidence suggests pain experiences differ between males and females, including greater pain intensity and more frequent pain reported by females, as well as differences in responses to pain interventions and mechanisms contributing to the pain.99,100 Few works reported any information about the race or ethnicity of participants. It is possible that race, ethnicity, and cultural background would affect reports of perceptions of pain and pain treatment as well as beliefs in types of treatments.101,102
The original work in graded motor imagery published in 2006 9 presented a paradigm shift in how patients with chronic pain were treated. Examining the number of works assessing the phases of graded motor imagery for phantom limb pain per year from 2007 to 2023 shows a growing interest in this topic (Figure 3). In addition, a large number of countries were represented in this scoping review, even with the search limited to works published in the English language (Appendix 3). This representation indicates that the phases of graded motor imagery are being investigated as treatment options in many different countries. Graded motor imagery requires low-cost equipment, potentially making the technique more easily available across the world.
Some of the information extracted from the works in this review was unclear and left up to the authors’ interpretation. We attempted to mitigate any errors in interpretation by having two authors independently extract the data and a third author resolve any conflicts. We also attempted to contact authors of some works for further information. Since this project was a scoping review intending to examine the current evidence on this topic, we included works that are not traditionally included in more rigorous evidence syntheses, such as published conference abstracts. Including these types of works may have affected some of the results, particularly with the information that was unreported, as many abstracts are unable to provide all the details. However, this scoping review aimed to capture as much information as possible on the phases of graded motor imagery treatment and related approaches for phantom limb pain, since the evidence on this topic is limited.
Future work could evaluate whether a three-phase graded motor imagery treatment protocol provides more pain relief than a single phase. It would be valuable to investigate this three-phase approach using a high-quality research design. Consideration for multi-site clinical trials may allow for sufficient recruiting and inform best practices (e.g. number, duration, and frequency of sessions). Careful consideration and reporting of participant characteristics can help to allow more meaningful conclusions to be drawn about which patients are most likely to be successful in finding phantom limb pain reduction with this treatment.
Clinical messages Graded motor imagery for phantom limb pain after amputation has primarily focused on the mirror therapy phase. Dosing of graded motor imagery intervention is inconsistent in the amount, frequency, and duration of treatment sessions, with no strong rationale for any particular treatment program. Graded motor imagery is a low-cost intervention, leading to the international use of its phases for the treatment of phantom limb pain after amputation.
Supplemental Material
sj-docx-1-cre-10.1177_02692155231204185 - Supplemental material for Graded motor imagery and its phases for individuals with phantom limb pain following amputation: A scoping review
Supplemental material, sj-docx-1-cre-10.1177_02692155231204185 for Graded motor imagery and its phases for individuals with phantom limb pain following amputation: A scoping review by Kierra Jean Falbo, Hannah Phelan, Dawn Hackman, Rebecca Vogsland and Tonya L Rich in Clinical Rehabilitation
Footnotes
Author contributions
The materials presented here solely represent the views of the authors and do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Rebecca Vogsland teaches on a contract basis providing education about and treatment of pain including graded motor imagery. The remaining authors do not report conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the U.S. Department of Veterans Affairs Rehabilitation Research and Development Career Development Award 1IK1RX003216-01A2 (TR) and was conducted at the Minneapolis VA Health Care System.
Supplemental material
Supplemental material for this article is available online.
Example search strategy.
| Search strategies |
|---|
|
6/10 Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations, Daily and Versions(R) <1946 to June 10, 2021> 1 Phantom Limb/ 1934 2 (phantom adj2 (limb or pain)).tw,kw. 2027 3 neuropath*.tw,kw. 140817 4 plp.tw,kw. 5326 5 exp Amputation/ 22276 6 Amputation, Traumatic/ 4847 7 Amputees/ 3723 8 amputation stumps/ 3146 9 (amputat* or amputee?).tw,kw. 47526 10 (limb adj2 loss).tw,kw. 2299 11 or/1-10 202876 12 ((explicit or graded) adj2 “motor imagery”).tw,kw. 81 13 gmi.tw,kw. 527 14 ((right or left or right-left) adj2 discrimin*).tw,kw. 457 15 Functional Laterality/ 57377 16 (laterality or laterali#ation).tw,kw. 20072 17 motor imagery.tw,kw. 3163 18 mirror therapy.tw,kw. 392 19 or/12-18 74163 20 and/11,19 1238 21 (exp infant/ or exp child/ or adolescent/) not exp adult/ 1942136 22 20 not 21 1190 23 exp animals/ not exp humans/ 4840409 24 22 not 23 894 25 limit 24 to english language 830 26 remove duplicates from 25 830 |
Definitions used to classify characteristics of the works in this review.
| Study design | Definition |
|---|---|
| Case control study | “A study that compares people with a specific disease or outcome of interest (cases) to people from the same population without that disease or outcome (controls), and which seeks to find associations between the outcome and prior exposure to particular risk factors. This design is particularly useful where the outcome is rare and past exposure can be reliably measured. Case control studies are usually retrospective, but not always.” 27 |
| Case study/series | “A study reporting observations on a single individual or series of individuals, usually all receiving the same intervention, with no control group.” 27 |
| Clinical trial | “An experiment to compare the effects of two or more healthcare interventions. Clinical trial is an umbrella term for a variety of designs of healthcare trials, including uncontrolled trials, controlled trials, and randomized controlled trials.” 27 |
| Controlled before and after study | “A non-randomized study design where a control population of similar characteristics and performance as the intervention group is identified. Data are collected before and after the intervention in both the control and intervention groups.” 27 |
| Controlled trial | “A clinical trial that has a control group. Such trials are not necessarily randomized.” 27 |
| Cross-over trial | “A type of clinical trial comparing two or more interventions in which the participants, upon completion of the course of one treatment, are switched to another. For example, for a comparison of treatments A and B, the participants are randomly allocated to receive them in either the order A, B or the order B, A. Particularly appropriate for the study of treatment options for relatively stable health problems. The time during which the first intervention is taken is known as the first period, with the second intervention being taken during the second period.” 27 |
| Non-randomized study | “Any quantitative study estimating the effectiveness of an intervention (harm or benefit) that does not use randomization to allocate units to comparison groups (including studies where ‘allocation’ occurs in the course of usual treatment decisions or peoples’ choices, i.e. studies usually called ‘observational’). To avoid ambiguity, the term should be substantiated using a description of the type of question being addressed. For example, a ‘non-randomized intervention study’ is typically a comparative study of an experimental intervention against some control intervention (or no intervention) that is not a randomized controlled trial. There are many possible types of non-randomized intervention study, including cohort studies, case control studies, controlled before and after studies, interrupted time series studies and controlled trials that do not use appropriate randomization strategies (sometimes called quasi-randomized studies).” 27 |
| Randomized controlled trial | “An experiment in which two or more interventions, possibly including a control intervention or no intervention, are compared by being randomly allocated to participants. In most trials one intervention is assigned to each individual but sometimes assignment is to defined groups of individuals (for example, in a household) or interventions are assigned within individuals (for example, in different orders or to different parts of the body).” 27 |
| Phases of graded motor imagery | Definition |
| Graded motor imagery phase 1: Left/right discrimination or limb laterality | “The process of identifying one side of the body as distinct from the other, or if a body part is rotating to the left or right.” 14 |
| Graded motor imagery phase 2: Explicit motor imagery | “The process of thinking about moving without actually moving.” 14 |
| Graded motor imagery phase 3: Mirror therapy | “Using movements of the stronger body part to ‘trick our brain’ into thinking that the weaker body part is moving.” 14 |
Appendix 3. World map highlighting countries represented by the works in this review.
Phases of graded motor imagery used in each work are included in this review.
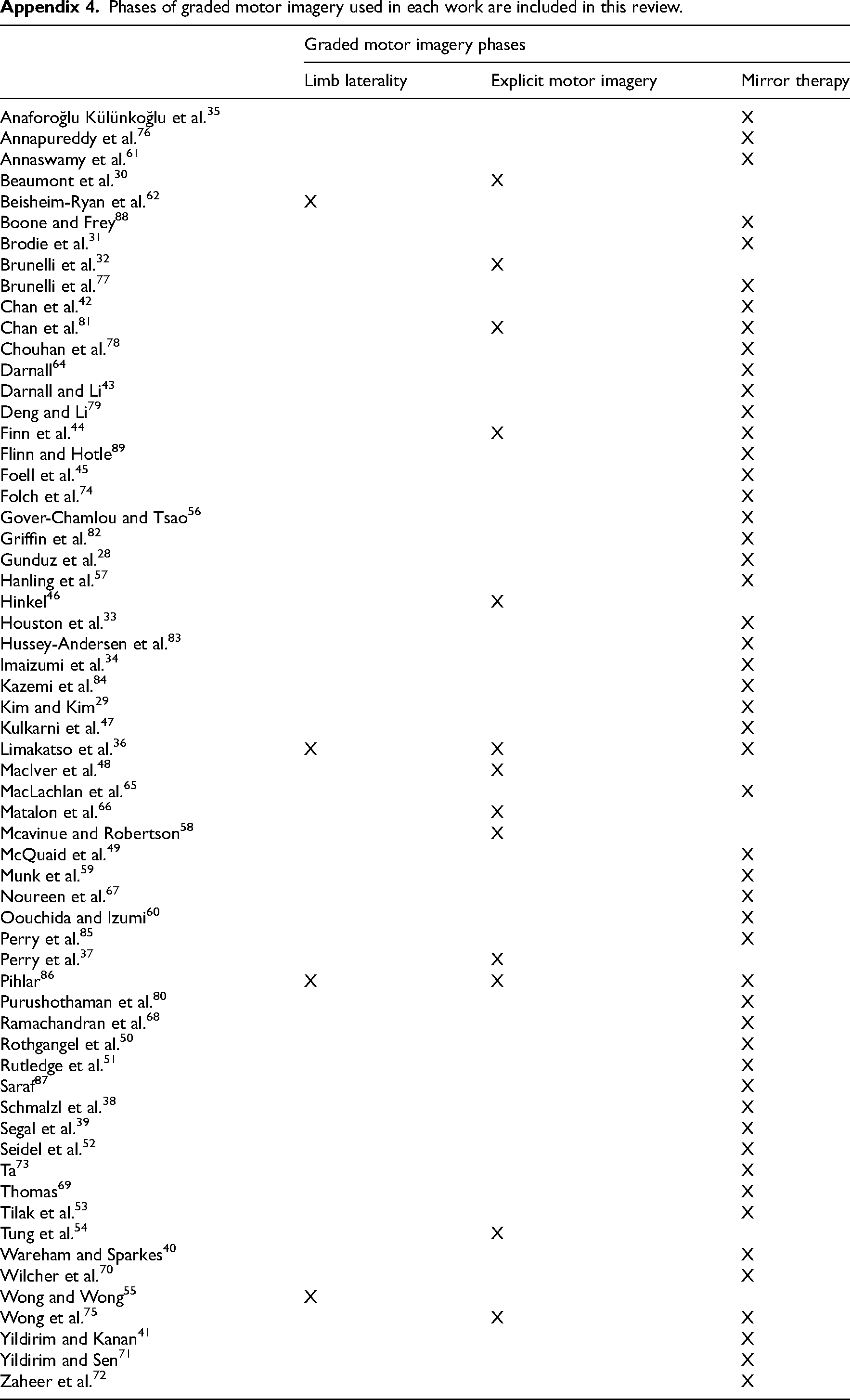
| Graded motor imagery phases | |||
|---|---|---|---|
| Limb laterality | Explicit motor imagery | Mirror therapy | |
| Anaforoğlu Külünkoğlu et al. 35 | X | ||
| Annapureddy et al. 76 | X | ||
| Annaswamy et al. 61 | X | ||
| Beaumont et al. 30 | X | ||
| Beisheim-Ryan et al. 62 | X | ||
| Boone and Frey 88 | X | ||
| Brodie et al. 31 | X | ||
| Brunelli et al. 32 | X | ||
| Brunelli et al. 77 | X | ||
| Chan et al. 42 | X | ||
| Chan et al. 81 | X | X | |
| Chouhan et al. 78 | X | ||
| Darnall 64 | X | ||
| Darnall and Li 43 | X | ||
| Deng and Li 79 | X | ||
| Finn et al. 44 | X | X | |
| Flinn and Hotle 89 | X | ||
| Foell et al. 45 | X | ||
| Folch et al. 74 | X | ||
| Gover-Chamlou and Tsao 56 | X | ||
| Griffin et al. 82 | X | ||
| Gunduz et al. 28 | X | ||
| Hanling et al. 57 | X | ||
| Hinkel 46 | X | ||
| Houston et al. 33 | X | ||
| Hussey-Andersen et al. 83 | X | ||
| Imaizumi et al. 34 | X | ||
| Kazemi et al. 84 | X | ||
| Kim and Kim 29 | X | ||
| Kulkarni et al. 47 | X | ||
| Limakatso et al. 36 | X | X | X |
| MacIver et al. 48 | X | ||
| MacLachlan et al. 65 | X | ||
| Matalon et al. 66 | X | ||
| Mcavinue and Robertson 58 | X | ||
| McQuaid et al. 49 | X | ||
| Munk et al. 59 | X | ||
| Noureen et al. 67 | X | ||
| Oouchida and Izumi 60 | X | ||
| Perry et al. 85 | X | ||
| Perry et al. 37 | X | ||
| Pihlar 86 | X | X | X |
| Purushothaman et al. 80 | X | ||
| Ramachandran et al. 68 | X | ||
| Rothgangel et al. 50 | X | ||
| Rutledge et al. 51 | X | ||
| Saraf 87 | X | ||
| Schmalzl et al. 38 | X | ||
| Segal et al. 39 | X | ||
| Seidel et al. 52 | X | ||
| Ta 73 | X | ||
| Thomas 69 | X | ||
| Tilak et al. 53 | X | ||
| Tung et al. 54 | X | ||
| Wareham and Sparkes 40 | X | ||
| Wilcher et al. 70 | X | ||
| Wong and Wong 55 | X | ||
| Wong et al. 75 | X | X | |
| Yildirim and Kanan 41 | X | ||
| Yildirim and Sen 71 | X | ||
| Zaheer et al. 72 | X | ||
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.