
Abstract
Objective
To develop a measure of the needs injured children and their families’ needs throughout recovery; The MAnchester Needs Tool for Injured Children (MANTIC).
Design
Tool development, psychometric testing.
Setting
Five children's major trauma centres in England.
Participants
Children aged 2 to 16 years with any type of moderate/severe injury(ies) treated in a major trauma centre within 12 months of injury, plus their parents.
Methods
Stage 1a (Item generation): Interviews with injured children and their parents to generate draft items.
Stage 1b (Co-production): Feedback about item clarity, relevance and appropriate response options was provided by parents and the patient and public involvement group.
Stage 2 (Psychometric development): Completion of the prototype MANTIC by injured children and their parents with restructuring (as necessary) to establish construct validity. Concurrent validity was assessed by correlation with quality of life (EQ-5D-Y). MANTICs were repeated 2 weeks later to assess test–retest reliability.
Results
Stages 1a,b: Interviews (13 injured children, 19 parents) generated 64 items with semantic differential four-point response scale (strongly disagree, disagree, agree, strongly agree).
Stage 2: One hundred and forty-four participants completed MANTIC questionnaires (mean age 9.8 years, SD 3.8; 68.1% male). Item responses were strong requiring only minor changes to establish construct validity. Concurrent validity with quality of life was moderate (r = 0.55, P < 0.01) as was test–retest reliability (ICC = 0.46 and 0.59, P < 0.001). Uni-dimensionality was strong (Cronbach's α > 0.7)
Conclusion
The MANTIC is a feasible, acceptable, valid self-report measure of the needs of injured children and their families, freely available for clinical or research purposes.
Introduction
Traumatic injury in children is a leading cause of death and disability, which can result in a significant health burden. 1 To provide child-centred rehabilitation after an injury it is important to understand and address their needs. However, to our knowledge there are no standardised, objective measures to assess their needs. 2 This paper describes the development of the MAnchester Needs Tool for Injured Children (MANTIC). Need is a broad and complex concept which has been defined in the NHS as ‘the capacity to benefit’. 3 Our previous work has shown that injured children and their families often have needs related to physical, functional, educational, cognitive and psychological problems which continued throughout recovery, particularly after discharge from hospital.4–6 Thus the International Classification of Functioning, Disability and Health (ICF) was used as a conceptual model to identify the injured children's needs.7,8 This has a holistic biopsychosocial base and combines dimensions of health, functioning, disability with personal and environmental factors. 7
Our previous scoping review showed that there are no standardised objectives measures to assess injured children's needs. Valid and reliable measures of related constructs such as quality of life (paediatric quality of life (PedsQL 9 and EQ-5D-Y)), 10 function (functional independence measure (WeeFIM) 11 and disability (PEDI-CAT)) 12 have been developed. However, they are not specific to injured children and exclude important issues such as educational support needs. Possible alternatives are specific measures of dependency or rehabilitation complexity, such as the Northwick Park Dependency Assessment,13,14 or the Rehabilitation Complexity Scale. 15 However, these are designed for adults, rely on completion by healthcare professionals and are used to determine the level of rehabilitation needed in a hospital or a specialised unit.13–15 Thus they are unsuitable for most injured children and for use after hospital discharge. This is important as injured children and their families often have a range of on-going needs when they return home, which are often unmet.2,4,6,16,17 The lack of an effective tool to identify children's (and their family's) rehabilitation needs is recognised as a contributory factor to the poor performance of children's trauma rehabilitation services in the UK, which have been described as inequitable, disjointed and poorly integrated with other services.16–18 Thus, we developed the MANTIC assessment tool to address this gap. The MANTIC is a questionnaire which enables injured children (aged 2–16 years) and their families to self-report their needs throughout recovery. It is designed for children who have sustained one or more injuries to any body part(s) to identify the frequency and type of needs of injured children in both clinical and academic settings. This may help clinicians to plan rehabilitation, signpost children and families to appropriate services, or monitor their needs after hospital discharge. This paper presents the development and validation of the MANTIC.
Methods
This study was approved by National Health Service, North-West-Greater Manchester South Research Ethics Committee (REC reference 17/NW/0615) and the Health Research Authority. The methodology was designed to incorporate key principles from the United States Food and Drug Administration guidance on the development of patient reported outcome measures (PROMs). 19
The study had two stages. Firstly, interviews with injured children and their families to identify potential items (questions) for inclusion in the assessment tool, and work with children and their families to co-produce a prototype MANTIC. The second stage involved a questionnaire survey of injured children and their families’ needs to develop a final version of the questionnaire and assess the psychometric properties.
Recruitment included children who were admitted to one of five specialist major trauma centres in England with one or more moderate to severe traumatic injury(ies) to any body part (Injury Severity Score > 8) 20 within the previous 12 months. Stage 1 (interview study) included children aged 5 to 16 years, and stage 2 (questionnaire study) included children aged 2 to 16 years. Our patient and public involvement (PPI) group advised that children aged 5 years were the youngest age group appropriate to interview (stage 1), but a younger age limit was used for questionnaire study (stage 2) because parents could complete the questionnaire on their child's behalf. The parents or guardians aged ≥ 18 years of injured children who fulfilled these criteria were also included. Recruitment continued up to 1-year post-injury to capture needs at different points in recovery. All participants needed to be able to read and/or communicate in English.
Babies/infants (less than 2 years old), children with isolated burn injuries (as they were managed by burns service), non-accidental injuries, or those for whom there were significant safeguarding concerns were excluded. Babies and infants were excluded because their needs predominately relate to their care requirements (which equate to their parent's needs). Participants who took part in stages 1a and 1b were excluded from stage 2, as their views may have been influenced by their previous knowledge of the development of the tool.
At each recruiting Major Trauma Centre, local databases were screened to identify potential participants. They were then approached to take part by the rehabilitation co-ordinator either in person (while an in-patient, during out-patient visits, community home visits) or provided with study invitation packs by post (stage 1). Patients in stage 2 were identified and approached using the same method but provided with a prototype MANTIC. This is the first draft of the MANTIC tool comprising of questions tested for validity and reliability in stage 2. A patient information sheet was attached to the front of the questionnaire. Before taking part in an interview (stage 1a/b), informed written was taken from the parent/guardian for themselves and their injured child. Written assent was also taken from the child where possible. In stage 2, a proportionate approach to consent was taken, whereby completion of the questionnaire inferred consent. 21 A paper copy of the MANTIC was given to parents so they could provide overall consent for themselves and their child. In clinical practice, injured children and their parents are considered as a single-family unit because their needs are inextricably linked. To reflect this approach to clinical care, instructions on the prototype MANTIC advised that it could be completed jointly by the child and parent, or solely by the child, or by parent depending on their preference.
Stage 1a: interviews to generate items (questions) for inclusion in the prototype (first draft) MANTIC
Semi-structured interviews explored the injured children's and families’ experiences and needs for care using an interview guide derived from our previous scoping review. 2 The guide was constructed to meet the study aims by exploring the range of needs related to the biopsychosocial model. 22 Interviews were conducted by the lead author (SJ) who has completed specialist training in interviewing children and young people. Participants were given the choice of conducting the interviews jointly (parent and child together) or individually (solely the child or their parent or guardian). Interviews involving children were completed in person, but parents were given the option of a telephone interview. In-person interviews took place at either the hospital, participants’ home or a neutral location depending on their preference. A modified ‘Draucker distress protocol’ was incorporated to identify signs of distress during the interview and suitable follow-up questions, actions, and escalation processes. 23
All interviews were digitally recorded, anonymised and transcribed verbatim. A thematic content analysis 24 was conducted to generate a list of draft items (questions) which reflected the injured children and their families’ needs using their own words. 25 This is called the prototype MANTIC.
Principles of reflexivity were applied to the qualitative component of research of design, as such the authors’ relevant background and experience are outlined. SJ is a clinical academic physiotherapist and completed this research as part of her NIHR-funded doctoral/post-doctoral research in children's trauma rehabilitation including extensive training in mixed methods, questionnaire design and psychometrics. She previously worked as major trauma co-ordinator at one of the participating centres. ST is a physiotherapist and Professor of Rehabilitation. JY is a Professor of Cancer Nursing. Both have long track records in the development, validation and clinical implementation of patient reported outcome and experience measures. All authors collaboratively critiqued, appraised, and evaluated the generated items to assess how their experiences and beliefs influenced the development. 26 The different clinical backgrounds within the research team helped to challenge assumptions, particularly those of the lead author who conducted the study interviews and had clinical expertise in children's trauma rehabilitation.
Stage 1b: co-production of the prototype MANTIC (working in partnership with injured children and their parents to refine the questionnaire)
Using the draft list of items, cognitive debriefing interviews were completed by the lead author with three parent interviewees of children with injuries to different body parts. In these interviews, participants gave feedback on the importance, relevance, clarity and comprehensibility of each items25,27,28 They were also asked to explain in their own words what the question meant to them and whether they had any additional needs not covered in the draft list. Participants also discussed and chose between two response formats. The first indicated how strongly they agreed with the statement about their level of need: strongly disagree, disagree, agree, and strongly agree. The second indicated the size of the need: no need, a small need, moderate need, a large need, and a very large need. Our PPI group contributed further feedback about the questionnaire's instructions for completion, design, layout, and the response formats, to ensure the prototype design was user-friendly.
Stage 2: psychometric development and production of the final MANTIC
The aim of this stage was to assess the construct validity of prototype MANTIC and amend it as necessary to produce a final version. Construct validity is how well a questionnaire measures the conceptual structure it was designed to measure, 29 which for the MANTIC was the needs of injured children and their families. Following tests for construct validity, concurrent validity and test–retest reliability of the final MANTIC were assessed. Concurrent validity is the correlation between scores from the new measure (the MANTIC) and those of a related or different measure (health-related quality of life), 29 and test–retest reliability is the variability of scores over time.
The selection criteria, recruitment strategies have been outlined above. The sample size was pragmatic, with a recruitment target for stage 2 of up to 150 participants (the approximate number of injured children managed in a major trauma centre in 1 year). 30 This is considered sufficient to pilot a questionnaire, assess its performance and perform an item analysis. 29 The prototype MANTICs were administered either in-person or by post along with a generic measure of children's health-related quality of life (the EQ-5D-Y), 10 to assess concurrent validity).
The prototype MANTIC comprises of 64 items shown in Table S1 of the supplementary material. Information about the child's age at the time of injury, gender, injury(ies) and the time post-injury were also collected.
Firstly, construct validity was assessed by removing items with:
poor response rates (>25% missing responses) low discriminatory power (i.e. high correlations (P=>0.001) between the scores for an item and age, gender, injured body part, and time post-injury) floor and ceiling effects (high endorsement of one response option (≥ 80%, ≤ 20%)) redundancy of items; high inter-item correlations (r=>0.7) or low corrected item-total correlations (r < 0.3).
A final assessment of construct validity was to assess whether the reduced items addressed a single construct (uni-dimensionality) using Cronbach's α for each category and the overall tool. A score of >0.7 indicated good internal consistency.
31
Concurrent validity was assessed by correlating the scores from the MANTIC with those from the EQ-5D-Y using Pearson correlations. Finally, the free text sections of the MANTIC were analysed thematically to inform decision making about the questionnaire development. To determine test–retest reliability (variability of scores across time), participants were asked to complete a second MANTIC, within 2 weeks of the initial questionnaire. The scores were compared using the intra-class correlation coefficient (two-way mixed effects model).
Results
Stage 1a
Thirteen injured children and 19 parents/guardians were interviewed. Five parents participated without their injured child, as they did not wish to participate or were too young to do so. The following interview formats were utilised: five interviews with parents alone, five dyads (joint parent and child), seven dyads (child and parent interviewed separately) and one triad (joint parent interview and the child interviewed separately). Three parent-only interviews were conducted on the telephone and the rest were completed in person. The demographics and clinical characteristics of the children who took part in the interviews are summarised in Table 1. The thematic analysis of interviews generated 64 items categorised into following types of needs: physical needs (21 items), mental health needs (4 items), family needs (2 items), information needs (5 items), service needs (4 items), practical and equipment needs (5 items), discharge planning (4 items) educational needs (5 items), child/young person's social and emotional needs (5 items) and parent/carers needs (9 items). The 64 items and their relevant categories are summarised in Table S1 of the supplementary material. Further details of the participants’ needs, and experiences have been reported in our previous qualitative studies.4–6
Demographic and clinical characteristics of participants completing interview study (stage 1a) and questionnaire survey (stage 2).
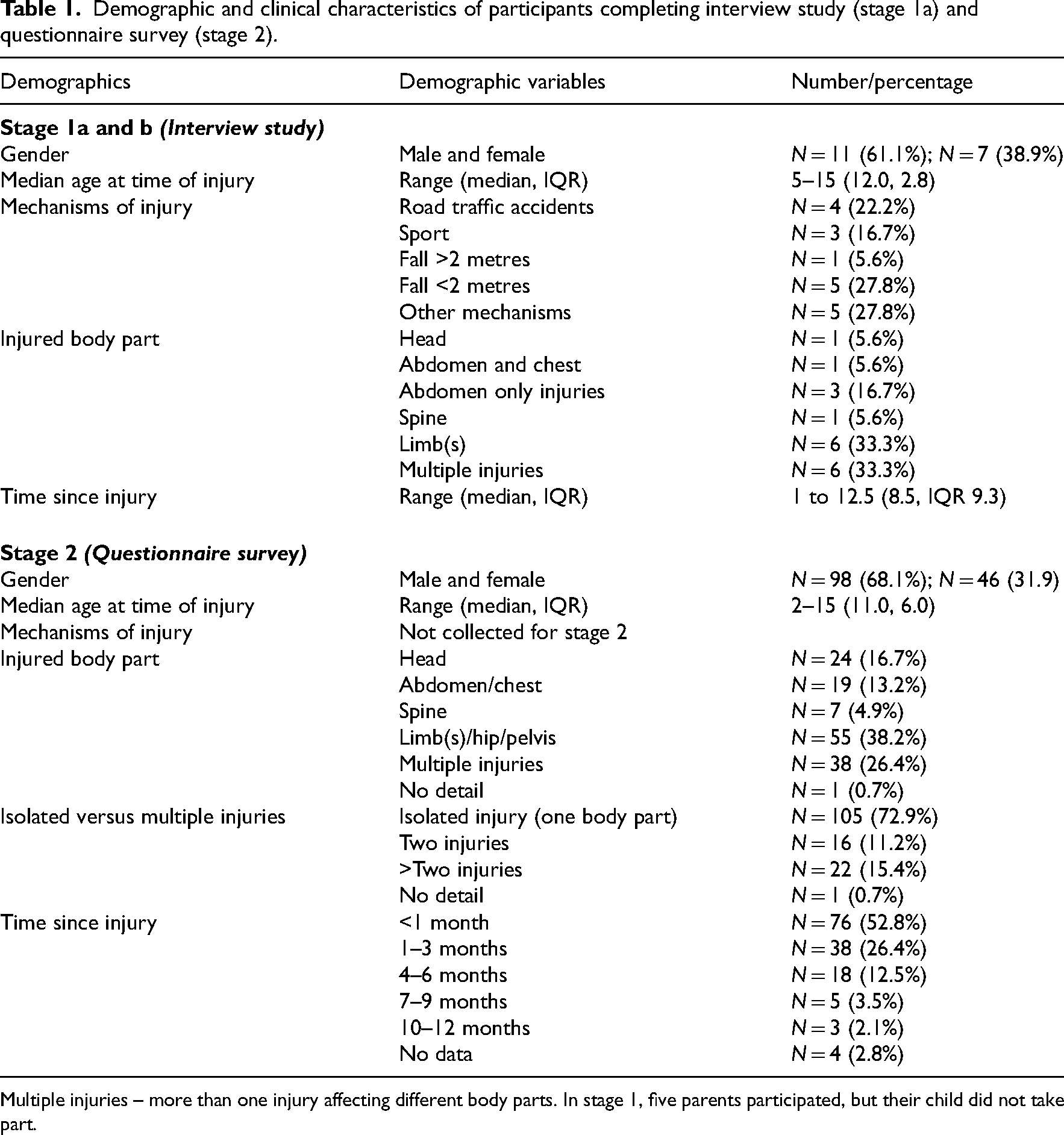
Multiple injuries – more than one injury affecting different body parts. In stage 1, five parents participated, but their child did not take part.
Stage 1b: co-production of the prototype MANTIC
The children of parents who took part in stage 1b of the study had injuries affecting each different body parts: head, abdomen/chest, limbs and multiple injuries. The cognitive debriefing interviews generated only minor changes to the wording of a few items. Participants noted that the MANTIC would have helped them identify and understand their needs after hospital discharge and throughout recovery.
Participants and the PPI group agreed that a response format indicating the level of agreement would be easier and more familar to understand, rather than the amount of need. Thus, a four-point Likert scale with a forced response format (no neutral response) termed as: strongly disagree, disagree, agree, strongly agree was chosen. These were assigned a score of 1 to 4 retrospectively. They also advised that ‘Not applicable’ should be added as a response option because the range of needs is not relevant to all ages and types of injuries. This response was scored as zero. Four items were worded in the opposite direction, so they were reversely scored. Thus, scores for all items could be analysed in the same way with a higher item score indicating a stronger need. The PPI group advised that a space for free text should be provided for participants to make any additional comments about their needs or ways the MANTIC could be improved. This further informed the development of the MANTIC 29 and helped to ensure all needs were comprehensively covered. Finally, the PPI group recommended that information should be provided about who participants should contact if they had concerns about any needs identified during completion of the MANTIC. The prototype MANTIC is shown in Table S1 (Supplementary material).
Stage 2: psychometric development and production of the final MANTIC
One hundred and forty-four injured children and their parents/guardians completed the 64-item prototype MANTIC. The mean age was 9.8 years (SD 3.8) and most (n = 98, 68.1%) were male (Table 1). Sixty-one (42%) completed the questionnaire while in hospital including the ‘discharge from hospital’ section and 83 (58%) completed it after discharge, excluding the discharge section.
Item analysis and decision making
Table 2 summarises each element of the item analysis and decision-making processes. Overall, the items performed well. None had a poor response rate, nor showed floor or ceiling effects and the full range of response options were used for each item. Therefore, none were removed for these reasons. No items demonstrated gender or age bias, indicating that age and gender did not bias item responses.
Summary of the item analysis and decision-making processes.
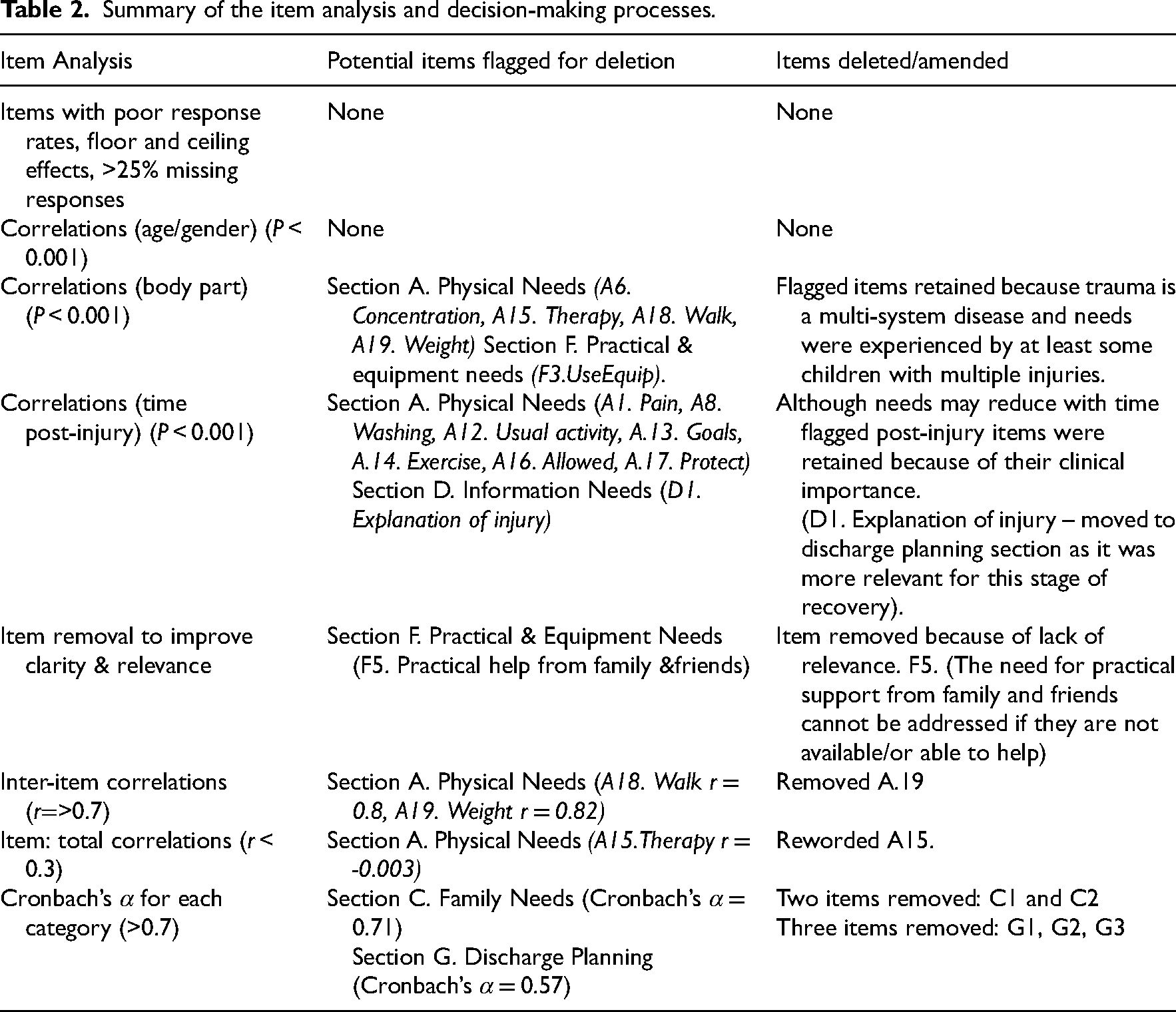
Table S2 of the supplementary material reports the discriminatory power of the items showing items with significant correlations with injured body parts and time post-injury. Items with significant correlations are detailed in bold and asterisked. Five items had a high correlation with the injured body part (P < 0.001) (A.6. A.15, A.18, A.19 and F.3). Except for item A.6 (concentration needs) these items were scored more frequently and higher by children with limb and multiple injuries. These children had greater needs for advice about mobility or how to use equipment, such as mobility aids, while therapy needs were predominately reported by children with head injuries. However, these items were retained because they were experienced by some children with different types of injuries, and it is clinically important to identify and treat them irrespective of the cause.
Eight items from the physical needs section demonstrated a high correlation with time since injury (P < 0.001). Needs relating to pain, advice about how to protect the injury(ies), and ‘what is allowed’ tended to reduce with time. This is to be expected, as symptoms reduce as children recover and they become more confident in their abilities. The items were retained as it was clinically important to know whether these needs were present whatever the stage of recovery. One item relating to information needs (D1. explanation of the injury) was moved from the information section to the discharge section, as it was more highly endorsed by participants who were in hospital.
Items were reviewed for clarity and relevance. Within the practical and equipment needs section, Item F5. ‘We need practical help from family and friends (e.g. transport, child care, shopping)’ was deleted because it is not a need that can be addressed clinically if help from family and friends is not accessible or available. Table S1 of the supplementary material shows the full text for items from the prototype MANTIC, including those items which were removed.
Redundancy of items: item-total and inter-item correlations
Two items relating to mobility had high inter-item correlations (>0.8): ‘A18: advice about how to use walking aids’, and ‘A19: advice about how much weight to place on legs’. Thus, item A18 was retained, and A19 was removed. One item ‘A.15: We are receiving the therapy we need (e.g. physiotherapy, occupational or speech therapy)’ had a low item total correlation (<0.3). The original wording for this item focused on whether participants were receiving the right amount of therapy, but the wording was amended to encompass those participants who may not be having any therapy (yet) but require it. (Table 2)
Internal consistency of items – Cronbach's α each section
Cronbach's α was greater than 0.7 for eight out of the ten categories demonstrating high internal consistency. The family needs section (n = 2) had a lower Cronbach's α (0.71) and was removed. The discharge section (four items) also had a lower score (0.57), and so it was extracted as separate section just to be completed by in-patients who are planning for discharge and three items (G1, G2, G3) were removed, but item G4 (I need help to co-ordinate care after discharge) was retained because of its clinical importance (Table 2).
Finally, an additional item was generated from the analysis of the free text as it was frequently highlighted as an issue and added to the discharge planning section: ‘We need to know when we can return to school and/or PE lessons’. Other changes included the addition of words to some items to make them more inclusive for all injury types. For example, the term headaches (which are common after head injuries but less so in other injury types) was added to the item about pain ‘We need advice about managing pain, comfort and/or headaches’. Items in the same section which overlapped or had a similar response pattern were combined. Items and sections were reordered to reflect the logical sequence in which needs may occur (i.e. educational and discharge needs are presented towards the end of the MANTIC). In accordance with guidance on questionnaire development, emotive needs were assigned to the later stages of the questionnaire. 29
Stage 2: psychometric testing
Cronbach's α following item deletion
After item removal, all categories had a Cronbach's α of 0.8, except the practical/equipment needs section and the discharge section, which scored 0.7 and 0.3, respectively. As noted above, the discharge planning category was extracted as a sub-scale for completion by patients who were still in hospital. The Cronbach's α for the entire MANTIC questionnaire was 0.94 demonstrating excellent uni-dimensionality. Note the total MANTIC score is not intended to be summated to provide an indication of the overall severity of the need; rather its purpose is to identify the needs of injured children and their families. Figure S1 of the supplementary material shows the final format of the MANTIC which is freely available for use in clinical practice.
Discussion
The results of this study demonstrate the content, construct and concurrent validity, and test–retest reliability of the MANTIC as a measurement tool enabling injured children and their families to self-report their needs (either separately or together) throughout the full trajectory of their recovery. Working closely with injured children and their families ensured the content was comprehensive, relevant, and acceptable. This was reflected in the high completion rate for all items and low levels of redundancy. Additionally, during the cognitive debriefing interviews participants explained that the MANTIC had educational benefits; helping participants to understand and identify injured children's needs, especially in the early stages of recovery when needs may not be obvious. This is clinically important because standards for the English major trauma system are based on the assessment of rehabilitation needs within 24 to 72 hours of admission and at discharge. 32 Another, potential impact of the MANTIC is that it could empower patients by forming the basis for discussions and joint decision-making with the professionals involved in their care. 33
Given the variation in responses to some items by patients with various types of injuries, we considered developing separate sub-scales for different injuries. For example, advice about how to use aids and equipment was much more frequent for lower limb injuries than other types of injury. However, all needs were present in at least some children with all types and times since injury (except the discharge-related items) so the items were maintained for all patients. Also, clinically it is important to identify whether these needs occur regardless of injury type. For example, injured children without apparent head injuries often have undiagnosed concussion 34 which can cause headaches and cognitive difficulties, so it is important to consider all needs even if they occur relatively infrequently.
We found a moderate correlation between the MANTIC and EQ-5D-Y, 10 demonstrating a significant relationship between low health-related quality of life and higher levels of need. This highlights the importance of identifying and addressing the needs of injured children to potentially improve their quality of life.
To our knowledge this is the first attempt to define the holistic needs for all types of childhood injuries, so comparisons with previous work are limited. However, there is a recent publication of a core outcome set for childhood limb fractures (CORE KIDS) for use in clinical trials. 35 Interestingly, there is some overlap between the outcome domains for the CORE KIDS (solely limb fractures) and categories of need for the MANTIC (all types of injuries). Both include psychosocial and educational domains, and the items from the MANTICs physical needs category reflect most of the remaining CORE KIDS outcome domains: pain and discomfort, return to physical, recreational and baseline activities, and recovery of mobility. 35 The convergence between the CORE KIDS outcome doamins and the categories of need for the MANTIC may be explained by the comparable methodology used in their development and overlap in the population. Although the development of the MANTIC involved children with all types of injuries, limb injuries (femoral fractures) were most common, which reflects the demographics of injuries treated by the English major trauma networks.36,37 Given this convergence it would be interesting to determine whether using the MANTIC to identify the needs of children with limb fractures, improves the CORE KIDS outcome set.
There are some limitations to this study. The participants broadly reflect the demographics and injury patterns of children with moderate to severe injuries reported nationally. 36 Therefore, we are confident that the content is valid and representative of the clinical population as a whole. However, a potential shortcoming was the recruitment of relatively few patients in the later stages of recovery (beyond 6 months post-injury). This is largely because most injured children make a good recovery and have been discharged from care within 6 months. 36 However, a longitudinal study measuring needs over time would identify the optimal time points for assessment of their needs. Furthermore, we recognise that the sample was limited to the UK, and the needs of children in other cultures and health care systems may differ. We also acknowledge that there may be differences in the types and frequency of reported needs depending on whether the injured child and their parent complete the MANTIC together or separately.38,39 However, the MANTIC was intentionally developed using the most flexible method of completion to account for the different range of children's, ages, abilities, and family dynamics. Furthermore, joint completion of the MANTIC reflects clinical practice in which the child and family are treated as unit. Although validity, feasibility and acceptability have been demonstrated, only moderate retest reliability was established with a small number of participants. The scores may have been influenced by participants’ recovery within the 2-week retest period. For example, removal of a cast or return to school could dramatically change the type or level of needs, particularly in the early stages of recovery. Thus, the retest period needs to be short, but then recall of previous answers may skew responses.
Finally, the response format merely asks whether a need is present (as this was preferred by our patient advisory group). It does not ask whether a need is met, or not, which is important information not only for planning individualised care, but also assessing the quality and effectiveness of service delivery and resource use. In future research we will investigate the addition of this option to item responses. The MANTIC enables the identification of the frequency and type of need; a total score should not be used be used to indicate the enormity or severity of needs.
Clinical messages
The MANTIC is a feasible and acceptable self-report measure of the frequency and type of injured children's and their families’ needs for use in academic and clinical settings.
It demonstrates robust: content, construct and concurrent validity.
Further testing of retest reliability with a larger sample is required.
Supplemental Material
sj-docx-1-cre-10.1177_02692155231158475 - Supplemental material for Development and validation of the MAnchester Needs Tool for Injured Children (MANTIC)
Supplemental material, sj-docx-1-cre-10.1177_02692155231158475 for Development and validation of the MAnchester Needs Tool for Injured Children (MANTIC) by Samantha Jones, Sarah Tyson and Janelle Yorke in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155231158475 - Supplemental material for Development and validation of the MAnchester Needs Tool for Injured Children (MANTIC)
Supplemental material, sj-docx-2-cre-10.1177_02692155231158475 for Development and validation of the MAnchester Needs Tool for Injured Children (MANTIC) by Samantha Jones, Sarah Tyson and Janelle Yorke in Clinical Rehabilitation
Supplemental Material
sj-docx-3-cre-10.1177_02692155231158475 - Supplemental material for Development and validation of the MAnchester Needs Tool for Injured Children (MANTIC)
Supplemental material, sj-docx-3-cre-10.1177_02692155231158475 for Development and validation of the MAnchester Needs Tool for Injured Children (MANTIC) by Samantha Jones, Sarah Tyson and Janelle Yorke in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors would like to thank all the trauma/rehabilitation co-ordinators at the Major Trauma Centres who participated in this study and made it possible. They are extremely grateful to all of the children and family members who participated in the study. They would also like to thank Naomi Davis for her continued support throughout the programme of research relating to children's trauma rehabilitation which resulted in this study.
The assistance Mary Ingram gave with reference management is greatly appreciated.
Author Contributions
All authors (SJ, ST, JY) contributed to the conception and design of the work, monitoring progress, critical appraisal and approval of the final version of the manuscript. Samantha Jones is the guarantor of the study and led the design of the work, data collection, data analysis, interpretation of the data and produced the manuscript drafts. Sarah Tyson and Janelle York contributed to the design of the work, data analysis and interpretation of the data. Sarah Tyson contributed to drafting the manuscripts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Samantha Jones was funded by the National Institute for Health Research (NIHR), (ICA Programme Clinical Doctoral Research Fellowship (Grant reference ICA-CDRF-2016-02-021)) for this research project. This publication presents independent research funded by the National Institute for Health Research (NIHR). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Gurantor
SJ is the lead author and guarantor for the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.