
Abstract
Objective
The objective of this review was to identify barriers and facilitators related to self-management from the perspectives of people with shoulder pain and clinicians involved in their care.
Data sources
CINAHL, MEDLINE, PsycINFO, SPORTDiscus, Embase, ProQuest Health, Web of Science, and Scopus were searched from inception to March 2022.
Review methods
A meta-aggregative approach to the synthesis of qualitative evidence was used. Two independent reviewers identified eligible articles, extracted the data, and conducted a critical appraisal. Two reviewers independently identified and developed categories, with validation by two further researchers. Categories were discussed among the wider research team and a comprehensive set of synthesized findings was derived.
Results
Twenty studies were included. From the perspective of patients, three synthesized findings were identified that influenced self-management: (1) support for self-management, including subthemes related to patient-centred support, knowledge, time, access to equipment, and patient digital literacy; (2) personal factors, including patient beliefs, patient expectations, patient motivation, pain, and therapeutic response; and (3) external factors, including influence of the clinician and therapeutic approach. From the perspective of clinicians, two synthesized findings were identified that influenced self-management: (1) support for self-management, including education, patient-centred support, patient empowerment, time, and clinician digital literacy; and (2) preferred management approach, including clinician beliefs, expectations, motivation, therapeutic approach, and therapeutic response.
Conclusion
The key barriers and facilitators were patient-centred support, patient beliefs, clinician beliefs, pain, and therapeutic response. Most of the included studies focused on exercise-based rehabilitation, and therefore might not fully represent barriers and facilitators to broader self-management.
Introduction
The current management of the majority of shoulder pain presentations is varied and inconsistent, with little standardization of best practice.1,2 While there are clinical guidelines to inform practice,3,4 the optimal treatment for these shoulder pain presentations is unknown. 5 Several systematic reviews have been conducted to identify the most effective treatment for these conditions.5–7 At best, the results of these reviews indicate only short-term benefits for different treatments, over no treatment or placebo. The research to date suggests that shoulder pain is resistant to treatment and possibly recurrent in nature. 8 Therefore, self-management programmes that equip patients with the necessary tools to manage their condition on an ongoing basis may assist them in maximizing their quality of life in the longer term.
Self-management programmes for shoulder pain have produced similar findings to clinician-led interventions for the treatment of several shoulder conditions.9–11 However, similar to clinician-led interventions, self-management programmes tend to show only short-term benefits.9,10,12 A reason for limited success with self-management may be poor patient engagement with the programme.
To identify the barriers and facilitators that may influence patient engagement with self-management of shoulder pain, we conducted a systematic review and qualitative synthesis. As our aim was to perform an aggregative, rather than an interpretive, synthesis of findings from qualitative studies, 13 and to develop practice recommendations, 14 we adopted the principles of meta-aggregation. 15 Accordingly, the aim of this review was to identify and summarize barriers and facilitators related to self-management from the perspectives of people with shoulder pain and clinicians involved in the care of this cohort of patients.
Methods
This review followed the Enhancing Transparency in Reporting the Synthesis of Qualitative Research guidelines, 16 and was registered with the International Prospective Register of Systematic reviews, registration number CRD42018106024. One reviewer (AOS) performed the systematic search (the last search was completed on 7 March 2022). No funding was received to undertake this systematic review.
Eight electronic databases (CINAHL, MEDLINE, PsycINFO, SPORTDiscus, Embase, ProQuest Health, Web of Science, and Scopus) were systemically searched. The search strategy comprised the keywords in Supplemental Appendix 1. The search of Medline is detailed in Supplemental Appendix 2. Grey literature sources were also searched, namely OpenGrey, ProQuest Dissertations & Theses Global, Canadian Agency for Drugs and Technologies in Health, and Google Scholar (limited to the first 100 hits). Reference lists of all included studies were searched using backward and forward citation screening; in addition, experts in the field were contacted to identify additional relevant studies.
The eligibility criteria are detailed in Box 1. We defined barriers as factors that obstruct adherence to, or engagement with, self-management of shoulder pain. We defined facilitators as factors that enable adherence to, or engagement with, self-management of shoulder pain. For the purpose of this review, self-management was defined as ‘the active participation by a person living with a shoulder condition in managing the symptoms, treatment, physical and psychological consequences and lifestyle changes inherent in living with that condition’. 17 Two reviewers (AOS and JMcV) independently screened titles and abstracts to determine whether the papers merited a full-text review, and then independently screened potentially relevant full-text papers by applying the inclusion criteria. Any disagreements that occurred in determining the relevance of a full-text paper were resolved by discussion between these reviewers.
Eligibility criteria
Design
Qualitative studies Full-text article in English Mixed-methods studies that reported qualitative data, if the qualitative findings could be extracted separately.
Participants
Adults (aged ≥18 years) with primary shoulder pain, irrespective of diagnostic label Clinicians involved in the care of adults with primary shoulder pain Specific exclusions were participants with:
– rheumatoid arthritis – polymyalgia rheumatica – hemiplegic shoulders – shoulder pain due to cervical or thoracic spine pathology.
Phenomenon of interest
Barriers and facilitators related to self-management of shoulder pain
The data extraction process was carried out by one reviewer (AOS). A second reviewer (JMcV) completed extraction for 20% of the articles and the information extracted was then compared to ensure consistency in the process. The Joanna Briggs Institute data extraction tool was used (Supplemental Appendix 3). The extraction process included findings from each of the included studies. A finding was defined as ‘a theme, category, or metaphor reported by authors of original papers’. 15 Each finding was then assigned a level of evidence depending on the capacity of the data to adequately support that finding (credibility). Using the ConQual criteria, findings were rated as unequivocal (relates to evidence beyond reasonable doubt and not open to challenge), credible (findings that are, albeit interpretations, plausible in light of data; because the findings are interpretive, they can be challenged) or unsupported (findings that are not supported by the data). 15
Qualitative research findings were synthesized using the Joanna Briggs Institute meta-aggregative approach. 15 An aggregative approach allowed a descriptive thematic mapping and synthesis of barriers and facilitators that lends itself to the formulation of specific recommendations for practice. 14 The first stage in the meta-aggregation involved the aggregation of findings with similarities in meaning to generate categories. Two reviewers (AOS and JMcV) independently categorized the findings from the 20 included studies.18–37 These reviewers then met to reach a consensus on the name and content of each category. Two reviewers (JD and CL) who were not involved in the categorization process validated these categories following discussion and refinement.
The second stage of meta-aggregation involved reviewing the full list of categories and identifying similarities in meaning to generate a comprehensive set of synthesized findings. The categories were discussed between three reviewers (AOS, JMcV and JD) and a consensus was reached on the set of synthesized findings. These synthesized findings were then discussed with the whole research team and feedback was provided by the other three reviewers (HS, CL and JS); this process resulted in the generation of a comprehensive set of synthesized findings.
The final stage involved the development of practice recommendations. AOS developed the practice recommendations. These recommendations were discussed with the whole research team and feedback was provided by the other five reviewers. The consensus was then reached on the set of practice recommendations.
Two reviewers (AOS and JMcV) independently assessed the included studies using the Joanna Briggs Institute critical appraisal instrument for qualitative research (Supplemental Appendix 4). Reviewers were blinded to each other's assessment, and assessments were only compared once the initial appraisal of an article had been completed by both reviewers. Any disagreements were resolved through discussion. No study was excluded based on an assessment of methodological quality, as weak studies may still offer relevant findings. 38
The ConQual 39 tool was used to assess the confidence in the synthesized findings, generating an overall score, for each synthesized finding, of ‘high’ (it is highly likely that the review finding is a reasonable representation of the phenomenon of interest), ‘moderate’ (it is likely that the review finding is a reasonable representation of the phenomenon of interest), ‘low’ (it is possible that the review finding is a reasonable representation of the phenomenon of interest), or ‘very low’ (it is not clear whether the review finding is a reasonable representation of the phenomenon of interest). 40
Results
The identification and selection of studies are summarized in Figure 1. 41 Overall, 20 studies were included in this review.18–37 Characteristics of the included studies are described in Table 1. Quality assessment of the included studies, using the Joanna Briggs Institute critical appraisal checklist for qualitative research, is presented in Table 2. In the evaluation of confidence in the synthesized findings, 39 each finding was assigned a ConQual score of ‘moderate’ (Supplemental Appendix 5).
PRISMA flow diagram. 41
Description of included studies.
Methodological quality of included studies.
Q1: Is there congruity between the stated philosophical perspective and the research methodology?
Q2: Is there congruity between the research methodology and the research question or objectives?
Q3: Is there congruity between the research methodology and the methods used to collect data?
Q4: Is there congruity between the research methodology and the representation and analysis of data?
Q5: Is there congruity between the research methodology and the interpretation of results?
Q6: Is there a statement locating the researcher culturally or theoretically?
Q7: Is the influence of the researcher on the research, and vice-versa, addressed?.
Q8: Are participants, and their voices, adequately represented?
Q9: Is the research ethical according to current criteria or for recent studies, and is there evidence of ethical approval by an appropriate body?
Q10: Do the conclusions drawn in the research report flow from the analysis, or interpretation, of the data? 39
In total, 305 findings were extracted from the 20 included studies and were organized into 12 categories that related to the patients’ perspective and 10 categories that related to the clinicians’ perspective. Further analysis of the categories led to the generation of three synthesized findings relating to the patients’ perspective and two synthesized findings relating to the clinicians’ perspective (Figures 2 and 3). Examples of supporting evidence are provided in Supplemental Appendices 6 to 10.
Patient perspective.
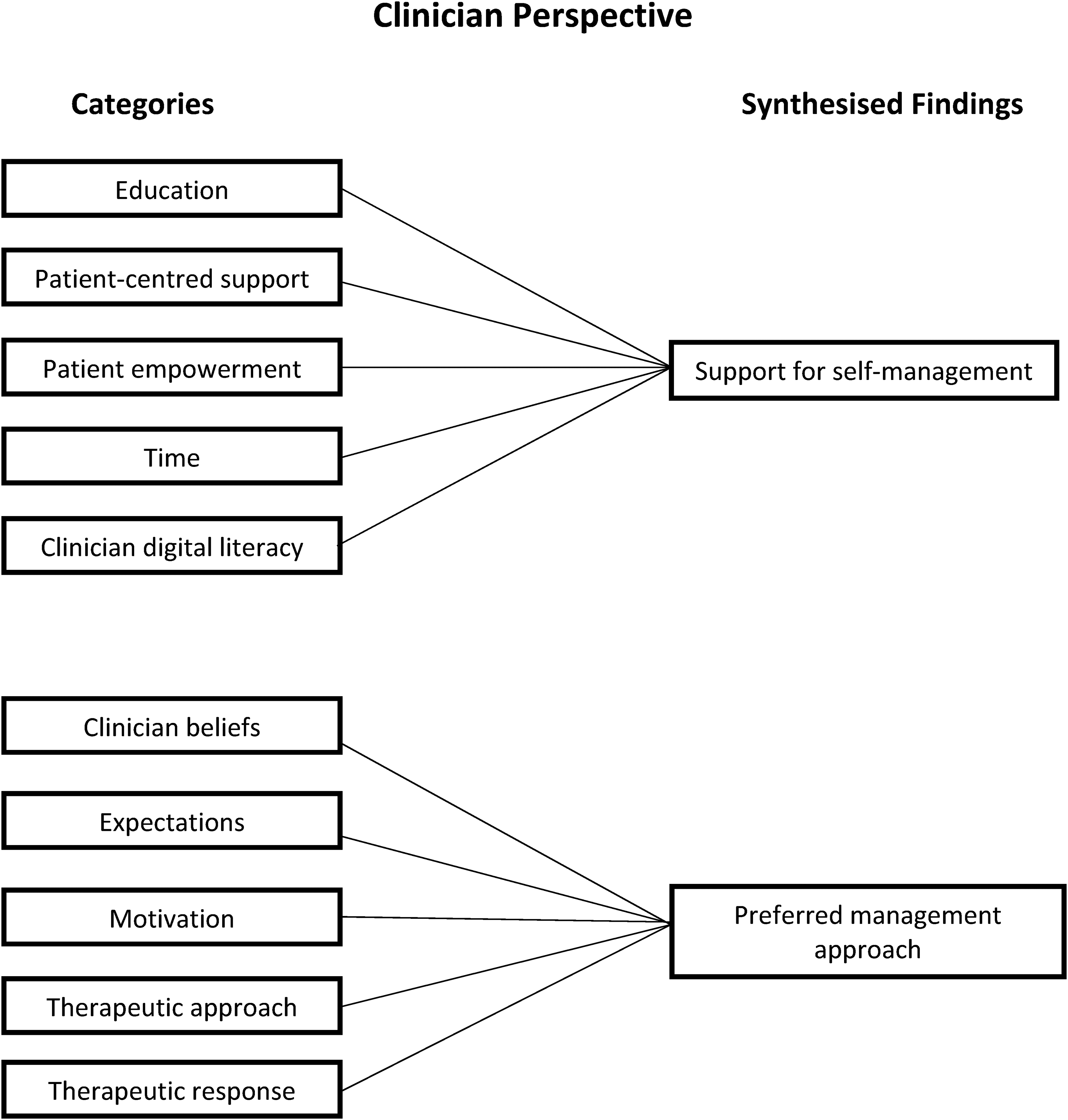
Clinician perspective.
Patient perspective
Support for self-management
People with shoulder pain identified support for self-management as being important; specifically, categories related to (1) patient-centred support, (2) knowledge, (3) time and daily routine, (4) access to equipment, and (5) patient digital literacy (Supplemental Appendix 6).
Patient-centred support
Support from the clinician20,23,26,28,31,34,35 and from family members,23,36 and social support18,35,36 were mentioned as facilitating participant adherence to self-management strategies. Early support from clinicians was valued and as participants progressed through treatment and their condition improved, this high level of support was reduced, and participants were encouraged to self-manage their shoulder pain. 18 Follow-up appointments with the clinician were also reported to facilitate self-management.23,27,29,36 Participants also mentioned that group classes increased adherence to their home exercise programmes.18,35
Knowledge
Participants reported that advice from the clinician on how to manage their shoulder condition,18,34 what to do when it hurts, 23 how to exercise,31,34 advice on rehabilitation timelines,29,34 and pain education30,34 were all seen to facilitate a self-management approach. However, when participants received advice that aligned with the biomedical model of pain, it tended to reinforce ideas of a specific biomedical remedy, including surgery. 19
Time/daily routine
Lack of time was frequently mentioned by participants as a barrier to completing their home exercise programme.23,29,32 Incorporating exercises into their daily routine – for example, doing their exercises while waiting for the kettle to boil – was a strategy that they utilized in order to increase their adherence to a home exercise programme. 29
Access to equipment
Ease of access to equipment facilitated adherence to self-management. 20 When participants lived some distance away from where the equipment was located, they reported that this was a barrier to their engagement with the equipment and therefore a barrier to adhering to their self-management programme. Simple equipment such as resistance bands for exercise was a facilitator, as they could be used anywhere.29,36
Patient digital literacy
Poor patient digital literacy was reported to be a barrier to a self-management programme for shoulder pain based on a web-based application (‘app’). 22 Participants forgot passwords, were unfamiliar with their Wi-Fi setup at home and had difficulty downloading the app, all of which hindered their ability to engage with the app-based programme. Suggestions that were made to facilitate engagement with the app were to introduce it as part of pre-operative care and to have a practice app. It is important to note, however, that only one study focused on patient digital literacy.
Personal factors
People with shoulder pain described several personal factors as being important. Categories identified related to (1) patient beliefs, (2) patient expectations, (3) patient motivation, (4) pain, and (5) therapeutic response (Supplemental Appendix 7).
Patient beliefs
A number of participants who had engaged with a self-management programme, and where outcomes were unsatisfactory, expressed concerns about the nature of their problem and questioned whether a self-managed approach was appropriate for them.23,30 These negative beliefs about self-management were reinforced if the clinician was also sceptical about the potential benefit of a self-managed approach. 23 However, participants who had previously received clinician-led interventions that were unsuccessful were receptive to engaging with self-management. 23
Patient expectations
Some participants who were offered a self-managed exercise programme were disappointed, as they anticipated a poor outcome with this approach. 23 Some attended physiotherapy assuming that it would be unsuccessful, but they had to complete a course of physiotherapy before being referred for surgery. 25 Many of these participants perceived their shoulder problem to be mechanical in nature and so expected an intervention that would fix their problem quickly.26,37 A number of these participants expected hands-on treatment,23,27 while others who had received previous unsuccessful conservative treatment expected surgery. 25
Patient motivation
Some participants admitted to being too lazy to follow their home exercise programme, and some accepted that they did not take responsibility for the programme as they hoped that the clinician would get them better.23,26,35 However, it appears that participants largely agreed that it was their responsibility to adhere to their home exercise programme and to establish new habits that would reduce the impact of their shoulder symptoms.26,30,31,34,35
Pain
Pain was found to have been both a facilitator of, and a barrier to, exercise. 29 Some participants who completed regular exercise reported a reduction in their shoulder pain and, as a result, their motivation to continue to exercise increased. 29 Those whose shoulder condition caused the most difficulty with functional activities demonstrated greater adherence to home exercise programmes. 29 However, others found pain to be a barrier to exercise.29,30,35,37 These participants used pain as a guiding factor to decide when to adjust or skip their home exercise programme and as an indication of when to stop exercise.30,32
Therapeutic response
When participants experienced a favourable therapeutic response with a self-managed approach, they reported being more likely to adhere.18,23,29,36 When previous clinician-led interventions yielded a poor therapeutic response, participants were amenable to engaging with a self-managed approach. 23
External factors
People with shoulder pain described external factors as being important; specifically, categories related to the (1) influence of the clinician and (2) therapeutic approach (Supplemental Appendix 8).
Influence of the clinician
Some participants described the physiotherapist as facilitating increased self-management by gradually getting the patient to take greater responsibility for the management of his or her shoulder condition.18,34 Some medical personnel may also have facilitated a self-management approach by encouraging patients to trial conservative treatment before surgery. 19 However, when the clinician expressed doubt over the benefit of self-managed approaches, this negatively affected the patient's attitude towards self-management.19,23,37
Therapeutic approach
When the home exercise programme only consisted of one exercise, some participants doubted the potential benefit of the programme. 23 However, others found the simplicity of the exercise programme to be a facilitator, as it was easily incorporated into their daily routine. 23 Many participants expected to receive hands-on treatments, which did not align with a self-management approach and could act as a barrier to engagement. 28
Clinicians’ perspectives
Support for self-management
Clinicians identified support for self-management as being important; specifically, categories related to (1) education, (2) patient-centred support, (3) patient empowerment, (4) time, and (5) clinician digital literacy (Supplemental Appendix 9).
Education
Clinicians agreed that early patient education was essential to get patient buy-in to the home exercise programme and to facilitate long-term self-management.21,33 Clinicians reported that education that focused on clarifying misconceptions about treatment, pain and anatomical structure, and explanation of treatment philosophies were important to engage patients in the management plan. 33 Despite this, clinicians expressed some disquiet about having had no formal training on how best to educate their patients. 33
Patient-centred support
Clinicians recognized the importance of providing ongoing support and monitoring in order to facilitate adherence to a self-managed exercise programme.23,24,33 One way to monitor patient adherence was via an online app, and the app reminded patients to complete their home exercise programme. 20 Clinicians also reported that follow-up appointments were beneficial in facilitating patients’ comply with home exercise programmes in the long term. 29
Patient empowerment
Clinicians reported that it was important to encourage patients to take responsibility for the management of their shoulder condition21,27 and for patients to understand the substantial commitment and significant behaviour change required for exercise management of shoulder pain to be successful. 33
Time
Clinicians reported that limited time was a barrier to supporting a self-management approach.20,22,33 For an app-based self-management programme, clinicians found it difficult to find the time to set up the patient app and explain how to use it during the consultation. 22
Clinician digital literacy
For some clinicians, digital literacy was a barrier. These clinicians were not confident about using new technologies and this affected their willingness to offer an app-based self-management programme to their patients. 22 It was noted that strategies to improve clinicians’ digital literacy and help them to incorporate the app into their everyday practice were important. Clinicians also noted that older patients often have poor digital literacy and might therefore not be suitable candidates for the app-based programme. 22 A practice app was suggested as a way of overcoming this barrier. It is important to note that only one study focused on clinician digital literacy.
Preferred management approach
Clinicians reported that the management approach they preferred in the treatment of shoulder pain was important; specifically, categories related to (1) clinician beliefs, (2) expectations, (3) motivation, (4) therapeutic approach, and (5) therapeutic response (Supplemental Appendix 10).
Clinician beliefs
Physiotherapists reported that they could identify patients during the assessment who they believed would not engage with a self-managed approach.23,33 For a number of physiotherapists, a self-managed approach did not align with their usual practice and they therefore found it challenging to embrace. 24 These physiotherapists expressed disquiet when they were unable to offer hands-on treatments. 24 Similarly, several surgeons believed that rotator cuff tears would not heal without surgery, and consequently believed that surgery was the only effective option. 25
Expectations
Clinicians mentioned that some patients expected the clinician to be more active than the patient during treatment 27 and they thought it unlikely that these patients would engage with a self-managed approach. Clinicians reported that it was important to understand the patient's expectations from the start27,33 and that when patient expectations do not align with self-management, it is a challenge for the clinician to offer this approach.27,33
Motivation
Clinicians described patients with shoulder pain as two distinct groups: those who are highly motivated and adhere to their home exercise programme, and those who need a lot of encouragement to engage and adhere.21,23,27 For the latter group, clinicians reported that it was important that these patients understood their role in the management of their shoulder pain.21,33 Clinicians discussed shared responsibility, whereby the clinician demonstrated exercises and motivated patients and patients were responsible for adhering to their home exercise programme.21,28,33 Regular check-ups were frequently mentioned as a way to motivate patients and increase adherence to their home exercise programme.27,29 Clinicians also mentioned that patients who pay for treatment were often motivated to engage in self-management. 27
Therapeutic approach
The simplicity of a self-managed exercise programme that consisted of one exercise was perceived as both positive and negative. 24 However, when clinicians who were previously sceptical about a self-management exercise programme of this type saw its success, this challenged their current practice. 24 More experienced clinicians were less likely to offer a temporary solution and were more likely to offer education, to obtain patient buy-in to long-term self-management.21,33 Most clinicians would offer hands-on treatment as part of their approach to the management of shoulder pain, which would obviously not align with a self-management approach.23,24
Therapeutic response
Clinicians agreed that providing short-term pain relief assisted in increasing patient engagement with the exercise programme. 21 Clinicians reported that they might use taping to achieve this short-term relief, and such relief demonstrated to the patient the long-term benefits of exercise. 21 When comparing the self-managed exercise programme to other treatment interventions, clinicians reported that it took longer to achieve a worthwhile clinical outcome when implementing the self-managed exercise programme 24 ; this represents a potential barrier to the self-managed approach.
Discussion
The aim of this systematic review and qualitative synthesis was to identify barriers and facilitators related to self-management from the perspectives of people with shoulder pain and clinicians involved in their care. Three synthesized findings were identified by patients as the issues that influenced self-management: support for self-management, personal factors, and external factors. Support for self-management and the preferred therapeutic approach were identified by clinicians as the main influences on engagement with self-management. Similar to the results of this review, education, health beliefs, patient-centred support, social support, therapeutic response, and shared decision-making have all been found to influence adherence to self-management for non-communicable diseases such as asthma, 42 chronic obstructive pulmonary disease, 43 and type 1 diabetes. 44 The findings of our review are also consistent with known theories of behavioural change. Determinants of behaviour change such as professional role, knowledge, skills, beliefs about consequences, and motivation are common components of behavioural change theories, and these determinants are consistent with the findings identified in our review. 45
An important consideration when interpreting the results of this review is that most of the included studies focused on home exercise programmes, and therefore might not fully represent barriers and facilitators related to broader self-management programmes for people living with shoulder pain. The term ‘self-management’ was rarely used in the studies included in this review; interventions that supported self-management were discussed but were not explicitly described as such. These interventions often involved exercise-based rehabilitation. Self-management encompasses more than advice and a home exercise programme, and goes beyond simple dissemination of information on diagnosis and exercise prescription. 46 Rotheram-Borus et al. 47 describe five essential elements required for successful self-management: (1) activate motivation for change; (2) apply information from education and self-monitoring; (3) develop skills; (4) acquire environmental resources; and (5) build social support. Most of the interventions discussed in our review were aimed at providing patients with the knowledge and skills to self-manage. However, most of the included studies did not address critical elements of self-management such as problem-solving, activating the motivation for change, initiating and reinforcing behaviour change, and building social support. Future research studies for shoulder pain should incorporate a broader framework for self-management to investigate the effectiveness and explore patient perceptions of a more person-centred approach.
The findings of this synthesis suggest that educational interventions focused on self-management strategies, such as home exercise, facilitated a self-managed approach. However, most of the education provided was based on the biomedical model of pain. Diagnosis of shoulder pain based on this model tends to reflect a narrow understanding of shoulder pain and is informed by a pathoanatomical diagnosis.48,49 A biomedically oriented educational approach was perceived as acting as a barrier to patient engagement with self-management. Only one of the included studies incorporated a formal education component, which consisted of a one-hour presentation. 30 Patients found this educational session overwhelming and suggested that this information should be delivered over several sessions. In contrast, education programmes for non-communicable diseases such as asthma, 50 chronic obstructive pulmonary disease 51 and diabetes 52 involve several educational sessions. Clinicians involved in the design of self-management programmes for shoulder pain need to take this ‘temporal chunking’ into consideration.
Patients appreciated the responsiveness of clinicians when questions and problems arose and reported that it was important that follow-up appointments were scheduled. Similar to our review, Campbell et al. 53 highlighted that follow-up support for effective type 1 diabetes self-management should be a combination of both structured and responsive individualized follow-up support. Patient-centred support should provide patients with the opportunity to troubleshoot problems as they arise, with appropriately trained clinicians.
Shared decision-making emerges as a common theme across systematic reviews investigating self-management for several chronic conditions.42,54–56 As part of this decision-making process, clinicians need to be aware of patient beliefs and expectations. This current review found that patients’ understanding of their shoulder pain was based on the biomedical model and patients expected hands-on treatment and had an expectation that clinicians will ‘fix’ them.23,25,26 This belief that the patient was a passive recipient of care was identified as a barrier to engagement with self-management for shoulder pain. Main et al. 57 report that patient concerns and mistaken beliefs should be addressed from the outset, which facilitates the development of a mutually agreed management plan. They highlighted that all explanations provided to patients must be in a language and terminology that they understand, as this helps to shape their beliefs and expectations and optimize their coping strategies. 57
Patient motivation was also a key factor underpinning adherence to exercise-based rehabilitation.42,43,53 Clinicians reported that they could identify patients who were not motivated and where self-management would not be effective. However, these studies did not investigate the validity of these expressed preconceptions. Future research should investigate if clinicians can validly identify patients who are not motivated and will not adhere to self-management and require a different approach that aligns with their needs.
The findings from our review suggest that clinicians’ preferred approach to the management of shoulder pain does not align with self-management. Their approach is more consistent with the biomedical model and comprises clinician-led interventions. Given that the evidence to date suggests that shoulder pain is resistant to treatment, clinicians should consider self-management programmes that focus on providing patients with the necessary tools to self-manage their shoulder pain and focus on keeping the patient active. In this context, clinicians are encouraged to switch from the biomedical model to the biopsychosocial model and a model of care based on shared decision-making to facilitate self-management support. 58 Furthermore, Wade et al. 48 report that the biomedical model cannot fully explain many forms of illness and that when patients are provided with a diagnosis they assume that a specific treatment will be provided by the health service, despite contemporary evidence for the use of active self-management in chronic condition care.
This synthesis found that patients and clinicians experience barriers and facilitators relating to engaging with self-management that are reflected in 14 domains of the theoretical domains framework. This framework was originally developed to identify influences on health professional behaviour related to the implementation of evidence-based recommendations. 59 The use of the theoretical domains framework has been extended and it is now used to inform the implementation of behavioural change in patient populations. Behavioural change interventions are increasingly recognized as an essential component of self-management. 60 The theoretical domains framework has also been used to guide the choice of behaviour change techniques and intervention components. 61 Therefore, future studies may benefit from using the theoretical domains framework to inform study design when exploring self-management approaches for shoulder pain. By adopting this framework, the barriers and facilitators relating to self-management can be explored, within the context of behaviour change, thereby identifying how barriers can be avoided or addressed through appropriate intervention strategies.
Strengths of the review include that, through exploring both patient and clinician perspectives, a more comprehensive understanding of the barriers and facilitators related to self-management is provided; in addition, the number of studies in this review provided sufficient evidence to answer the research question. Multiple reviewers carried out each stage of the review to address any potential areas of subjectivity, which enhances the credibility of the review. A range of approaches exist within qualitative synthesis, 62 but as our pragmatic concern was to identify ‘lines of action’ for clinical practice, rather than a more phenomenological understanding of the experience and management of shoulder pain, we adopted an aggregative rather than an interpretive approach.
There were also some limitations in the review process. Given how broad self-management is and the multiple elements encompassed by self-management, it is possible that the keywords searched may not have found all the relevant studies. However, reference lists of all included studies were searched using backward and forward citation screening, and experts in the field were contacted to identify additional relevant studies. Our use of the Joanna Briggs Institute critical appraisal checklist for qualitative research was not assessed for reliability; however, studies were assessed independently, and agreement was reached for all studies. Finally, our review only sought to identify the barriers and facilitators that are related to self-management approaches for shoulder pain. Further research is needed to examine whether overcoming these barriers and extending the framework towards a more person-centred approach will increase adherence to self-management programmes for shoulder pain and improve patient outcomes.
Practice recommendations
From the results of this synthesis, three key recommendations were derived that are intended to help to inform the design and implementation of self-management programmes for shoulder pain.
Recommendation 1
Patients’ beliefs, goals and expectations must be considered when developing and implementing a self-management programme. Patients should be involved in the decision-making progress, and accordingly, the benefits and limitations of each treatment option should be explained to them so that they can make informed decisions. If patients’ beliefs, goals and expectations do not align with a self-management approach, then the aims of self-management, such as equipping patients with the necessary tools to manage their condition on an ongoing basis and enabling them to keep active, should be explained to the patient or these aims should be re-oriented to more appropriately support their needs and goals. Similarly, patients should be provided with an education that aligns with their goals and needs. Patient digital literacy should also be considered when developing online or application-based self-management programmes.
Recommendation 2
To increase patient adherence to exercise-based rehabilitation, self-management programmes might consider the potential value, or otherwise, of follow-up support, aimed at empowering the patient, through assessment of progress, goal setting, and problem-solving support. For patients who lack motivation, group exercise classes and alternatives identified by the patient might be appropriate. Where pain is a barrier to adherence, a graded approach to exercise-based rehabilitation could be considered in tandem with recognition of the patient's acceptable symptom response. Programmes should also ensure that patients have adequate access to resources and are provided with strategies to allow them to incorporate the approach into their daily routine.
Recommendation 3
Clinicians should consider their own current beliefs and the extent to which they might facilitate or compromise support for self-management of people living with shoulder pain. As shoulder pain is recurrent in nature and often resistant to current treatments, optimal management should include equipping patients with the necessary tools that align with their goals and needs, and assist them to return to valued life activities. Clinicians may require new skills to support person-centred care and longer consultation times to enable them to incorporate self-management strategies into the management of people with shoulder pain.
Conclusion
This qualitative synthesis identified barriers and facilitators relating to self-management approaches for shoulder pain that might explain, in part, why existing self-management programmes are not always effective. Most of the included studies focused on home exercise adherence and therefore might not fully represent barriers and facilitators related to broader self-management programmes for shoulder pain. Adherence to self-management programmes might be improved by better education of both patients and clinicians to shape helpful contemporary evidence-informed beliefs and expectations about management of shoulder pain as well as shared planning and behavioural support. A greater focus should be placed on the limitations of currently available treatments and the potential to maximize the quality of life over the long term through adherence to a self-management programme. A supportive environment, motivation, adequate resources, and using educational methods that build self-care skills increase engagement with self-management of shoulder pain. Clinicians should review and consider whether any of their current beliefs might compromise support for self-management of people living with shoulder pain. Critically, the results of this review could stimulate informed discussion for the future delivery of self-management programmes for people with shoulder pain and the requirement to upskill clinicians to effectively support patients and implement behaviour change strategies. The challenge now is to incorporate these findings into routine practise and to develop novel interventions to support effective self-management.
Clinical messages
Patients’ expectations and goals must be considered when developing and implementing a self-management programme.
To increase patient adherence to exercise-based rehabilitation, follow-up support, and the patient's acceptable symptom response should be considered.
Clinicians should consider their own beliefs and the extent to which they might compromise support for self-management.
Supplemental Material
sj-docx-1-cre-10.1177_02692155221108553 - Supplemental material for Barriers and facilitators related to self-management of shoulder pain: a systematic review and qualitative synthesis
Supplemental material, sj-docx-1-cre-10.1177_02692155221108553 for Barriers and facilitators related to self-management of shoulder pain: a systematic review and qualitative synthesis by Aidan O'Shea, Jonathan Drennan, Chris Littlewood, Helen Slater, Julius Sim, and Joseph G. McVeigh in Clinical Rehabilitation
Footnotes
Author Contributions
AOS and JMcV assessed eligibility for inclusion; AOS and JMcV undertook data extraction; AOS and JMcV undertook critical appraisal of the included studies; AOS, JD, CL, HS, JS and JMcV undertook data analysis and data synthesis. All authors contributed to and approved the final draft of the manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C. Littlewood was a co-author of three of the studies and J. Sim was co-author of one of the studies included in this review, but neither author was involved in study selection. J. McVeigh was co-author of one included study, and was involved in study selection.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.