
Abstract
Objective
To determine the feasibility of adding coaching sessions to a website (MS INFoRM) that supports self-directed fatigue management for people with multiple sclerosis (PwMS).
Design
Double-blind, parallel-group feasibility study.
Participants and setting
Twenty-six PwMS, who experienced severe fatigue (fatigue severity scale > 5.4), were recruited from participants who were ineligible for the main trial testing on the MS INFoRM website.
Intervention
Six 45-to-60-min sessions of one-on-one coaching plus access to the MS INFoRm website compared to two check-in phone calls plus access to the MS INFoRm website. Both study arms took place over 3 months.
Main measures
Feasibility parameters included proportion eligible of those screened; proportion consented; missing data; retention and adherence rates. Acceptability was explored through qualitative interviews. Secondary outcomes (self-efficacy and fatigue impact) were measured at baseline and post-intervention.
Results
76 people were invited to participate in this add-on study. 40 were interested and screened: 32 were eligible, 26 consented, and were randomized (mean age: 48.5 yrs (SD: 8.7), mean disease duration: 11.5 yrs). Retention was 85% (22 out of 26). Coaching adherence was high (86% attended ⩾ 5 sessions). At 3 months, people in the intervention group showed more improvements in self-efficacy and fatigue impact compared to the comparison group, however, the difference was not statistically significant (p = 0.471 and p = 0.147, respectively). The intervention was well-received by the participants and there were no adverse events.
Conclusion
Combining one-on-one coaching sessions along with web-based interventions is feasible and appreciated by the participants, and worth exploring further in a larger trial.
Introduction
People with multiple sclerosis (PwMS) often experience debilitating fatigue that impairs daily activities and function.1,2 Easy access to interventions that can support fatigue self-management is critical to reducing the impact of this symptom on the everyday lives of people with this disease. Therefore, our team undertook a randomized controlled trial of a self-directed, web-based fatigue self-management intervention (MS INFoRm) for people with multiple sclerosis who experience mild to moderate levels of fatigue. 3 To address the fatigue management needs of those individuals who were excluded from the main trial because of severe fatigue, we launched an add-on study targeting these individuals.
The primary purpose of this add-on study was to examine the feasibility of delivering MS INFoRm + Occupational Performance Coaching (OPC) to PwMS with severe fatigue and to determine if a full-scale study of the effectiveness of this combination was worth pursuing. OPC is a well-developed coaching intervention specifically designed to improve performance in personally valued activities while building skills to address future challenges with activity participation. 4 OPC has a strong potential for application in chronic disease self-management as therapy goals are focused on a change in performance 5 and can assist clients to sustain and generalize performance to other contexts. 4
Our secondary objective was to develop preliminary evidence about the extent to which the MS INFoRm + OPC reduces fatigue impact, and improves self-efficacy for managing multiple sclerosis fatigue, compared to the comparison group who only received access to the MS INFoRm website.
Methods
This feasibility study was approved by the Queen's University Health Sciences & Affiliated Teaching Hospitals Research Ethics Board (ref: 6020674) as an add-on to our original trial. 3 The original trial was registered at clinicaltrials.gov (NCT03362541). The feasibility study was partially supported by a National Multiple Sclerosis Society Mentor-based Post-doctoral Fellowship Award (MB0028). Participant recruitment took a total of 54 days, starting in November 2018, with the first participant enrolled in January 2019. Data collection was completed in May 2019.
Subjects
The original MS INFoRM study targeted PwMS with mild to moderate levels of fatigue. 3 Through the screening process, there were a significant number of PwMS who scored greater than 5.4 on the Fatigue Severity Scale, 6 making them ineligible for the original trial. These excluded individuals were targeted for this add-on study, provided that they had previously consented to be recontacted by the study team.
A trained research assistant (research assistant#1) recontacted and screened individuals to confirm: (a) diagnosis of multiple sclerosis, (b) between 18 and 65 years of age, (c) access to a computer or other electronic device with internet access on which to review MS INFoRm, (d) significant fatigue indicated by a score > 5.4 on the Fatigue Severity Scale (FSS), 6 and (f) living in Canada. Participants were excluded if they: (a) had any major comorbid conditions that might influence fatigue management (lupus, rheumatoid arthritis, chronic obstructive lung disease, chronic fatigue syndrome); (b) had difficulty reading and comprehending English written at a Grade 7 level; (c) demonstrated severe cognitive impairment (score of > 12 on the Short Blessed Test) 7 ; (d) demonstrated severe depression (score of > 2 on PHQ-2)8,9; or (e) had upper extremity or visual impairments that could not be accommodated adequately to enable computer access.
Eligible individuals were sent a study package containing the informed consent documents and a study information sheet, and those who returned the signed consent form were enrolled. Group allocation was assigned by one of the authors (SA) using computerized random number generation, and based on a random permutated block design (blocks of 4), to ensure a 1:1 allocation ratio between the intervention and the comparison group.
Outcome measures
Information on demographics was collected at baseline including age, years since diagnosis, ambulatory disability via the Patient-Determined Disease Steps score, 10 sex, education level, living arrangement, type of multiple sclerosis, medication, and involvement in any other rehabilitation programs.
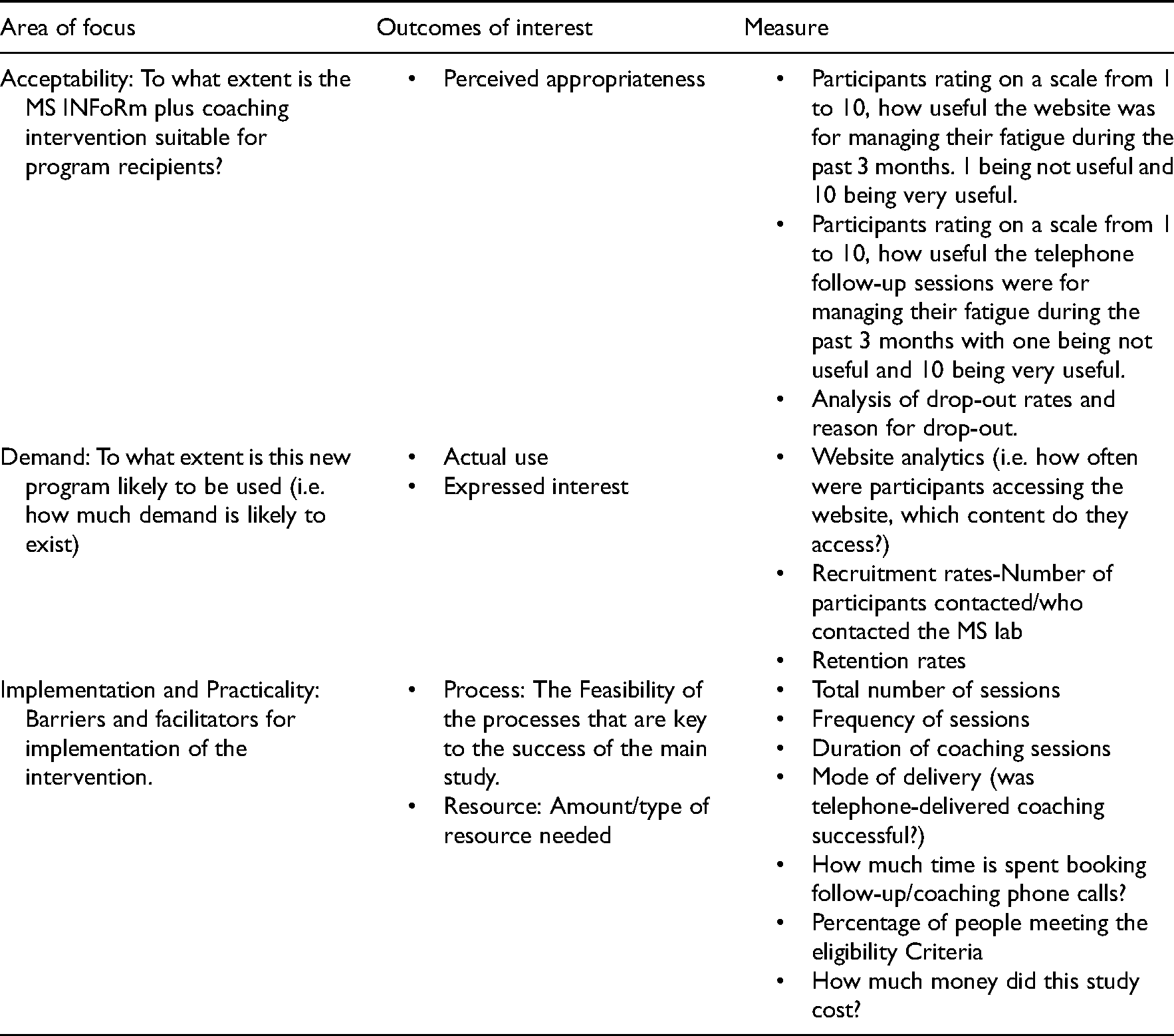
To address the primary objective of the study, measures of feasibility including acceptability, demand, implementation, and practicality were used. 11 Definitions of each area of focus, outcomes of interest, and their measurement processes are provided in Table 1.
Feasibility measures.
To complement our primary outcome measures, we held post-study telephone interviews with participants in both groups, asking about the following topics: their experiences of using MS INFoRm and the telephone support, specific aspect(s) of the study that went well and were found useful, and how we could improve the study in the future.
To address the secondary objective of the study, we evaluated fatigue impact using the Modified Fatigue Impact Scale (MFIS),12,13 and self-efficacy using the Multiple Sclerosis Self-Efficacy Scale (MSSES). 14 Collection of the secondary outcome data occurred at two points: baseline (week 1) and immediately post-intervention (week 12). Outcome measures were administered over the phone by research assistant#1, who was blind to group allocation.
Procedures
After the baseline assessment, both groups received a login and password for the study website, although participants in the groups were directed to different parts of the website. More detail about the website sections can be found in the MS INFoRm trial protocol. 3
Intervention group
The intervention involved 12 weeks of access to the intervention section of the MS INFoRm website and six one-on-one telephone coaching sessions facilitated by a registered occupational therapist (research assistant#2).
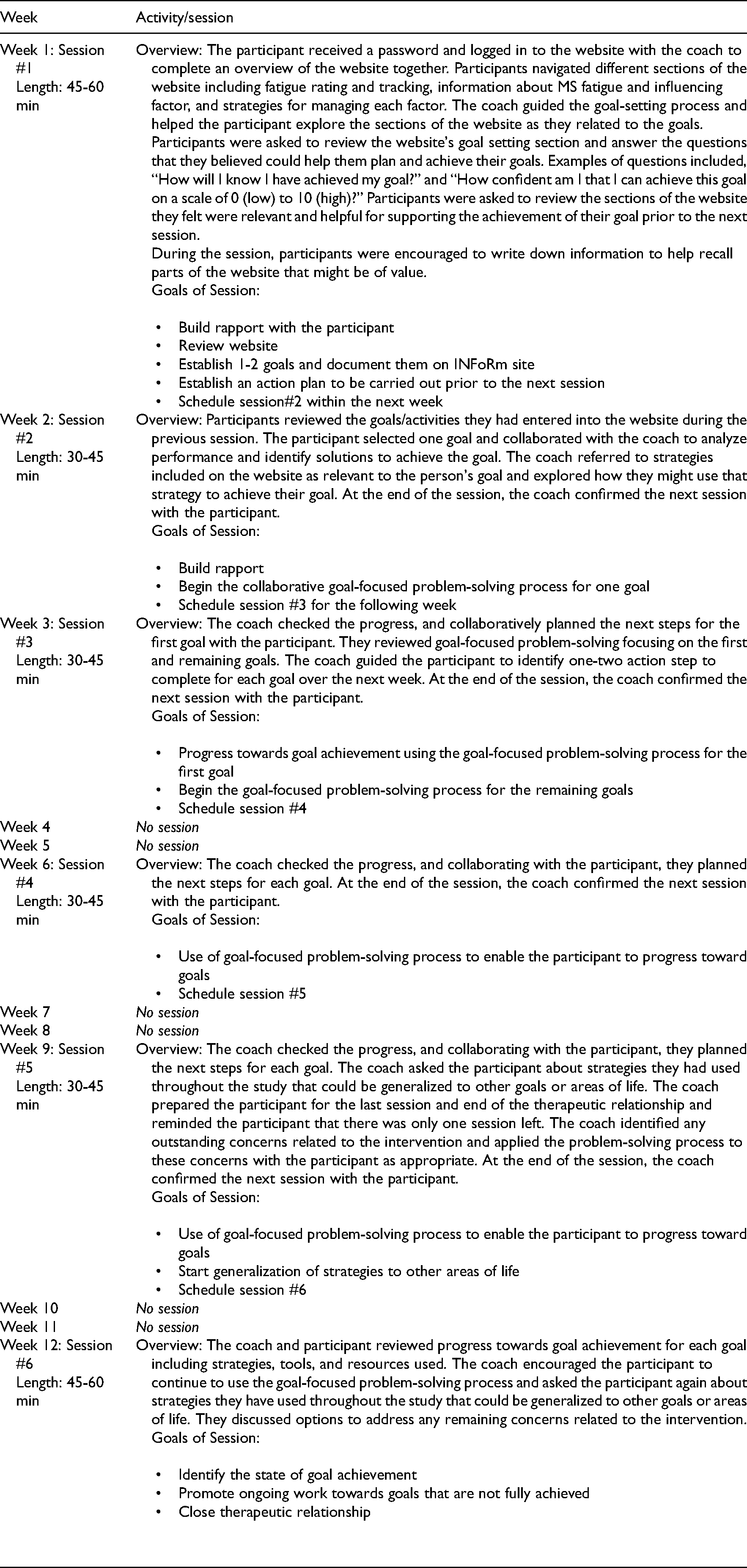
Table 2 illustrates a weekly outline of the points of contact and intervention that participants received. The first three sessions took place within the first 4 weeks in order to build rapport and maintain motivation. The following three sessions took place on a bi-weekly basis to allow the participants to explore strategies at their own pace.
Occupational performance coaching (OPC) sessions outline.
Comparison group
Participants in the comparison group had access to the control section of the MS InFoRm website for 12 weeks. The control website includes links to widely available resources to which clinicians often direct their clients with multiple sclerosis. 3 Individuals allocated to the comparison group received two support telephone calls from a research assistant (research assistant#3) to further mimic usual care. One phone call was made to ensure participants were able to log in and navigate the website without issues. A follow-up phone call was made within two weeks to check in with participants and answer any questions they might have about the website or the content. This process was consistent with what may occur through multiple sclerosis programs, as the distribution of educational materials and follow-up is common for people with multiple sclerosis experiencing fatigue.
Fidelity assessment
We examined three aspects of treatment fidelity to examine the extent to which the intervention (a) was delivered as intended (delivery fidelity), (b) was received and understood (receipt fidelity), and (c) enhanced the enactment or use of strategies by participants (enactment fidelity). 15 For the intervention group, we tracked time spent on individual sections of the website and the number of returns to sections over time. We considered that delivery fidelity had been achieved if a participant viewed all relevant sections, as related to their goals, of the MS INFoRm site at least twice per month in the three-month intervention period. We considered that receipt fidelity had been achieved if a participant downloaded the fatigue tracking sheet and Canadian Physical Activity Guidelines for multiple sclerosis. 16 We considered that enactment fidelity had been achieved if participants experienced a reduction in the impact of fatigue and increased self-efficacy between baseline and three months, as this would imply that participants are using the strategies effectively in their everyday lives.
Audio recordings of coaching sessions were used to monitor treatment fidelity. The occupational therapist who was completing the coaching and an additional research team member (DK) who is an expert in occupational performance coaching reviewed the session recordings and scored them using a treatment fidelity checklist that was developed for use with occupational performance coaching. 17 Recordings of the first five participants were monitored with DK providing feedback to the coach until she consistently received a rating of 80% fidelity on the treatment fidelity checklist.
Analysis
Descriptive analyses (e.g. means, standard deviations, proportions) were used to summarize sample characteristics and feasibility outcomes. The two groups were compared on baseline measures and key demographic and disease-related variables to test the similarities of the groups and ensure randomization worked. As this was a feasibility study, the level of missing data was documented but no imputation was undertaken. An independent t-test was used to compare the difference in mean outcomes (self-efficacy and fatigue impact) between the two groups. Effect sizes based on a difference in mean scores were expressed as Cohen's d. Statistical analysis of the study results was carried out with SPSS Software 25. 18 The summary of feedback provided by participants during the post-intervention interview has also been reported. For this feasibility study, we sought a sample size of 26. This is consistent with recommendations made by experts in the design of pilot and feasibility studies and was adequate to inform all aspects of the study being assessed for feasibility. 19
Results
Figure 1 (CONSORT diagram) shows the flow of participants throughout the study. Table 3 summarizes the demographic and baseline characteristics of the 26 participants using appropriate summary statistics. The groups were well-matched for all demographic and baseline characteristics, and there was no significant difference between the groups on any of the variables listed in Table 3 (i.e. randomization was successful).
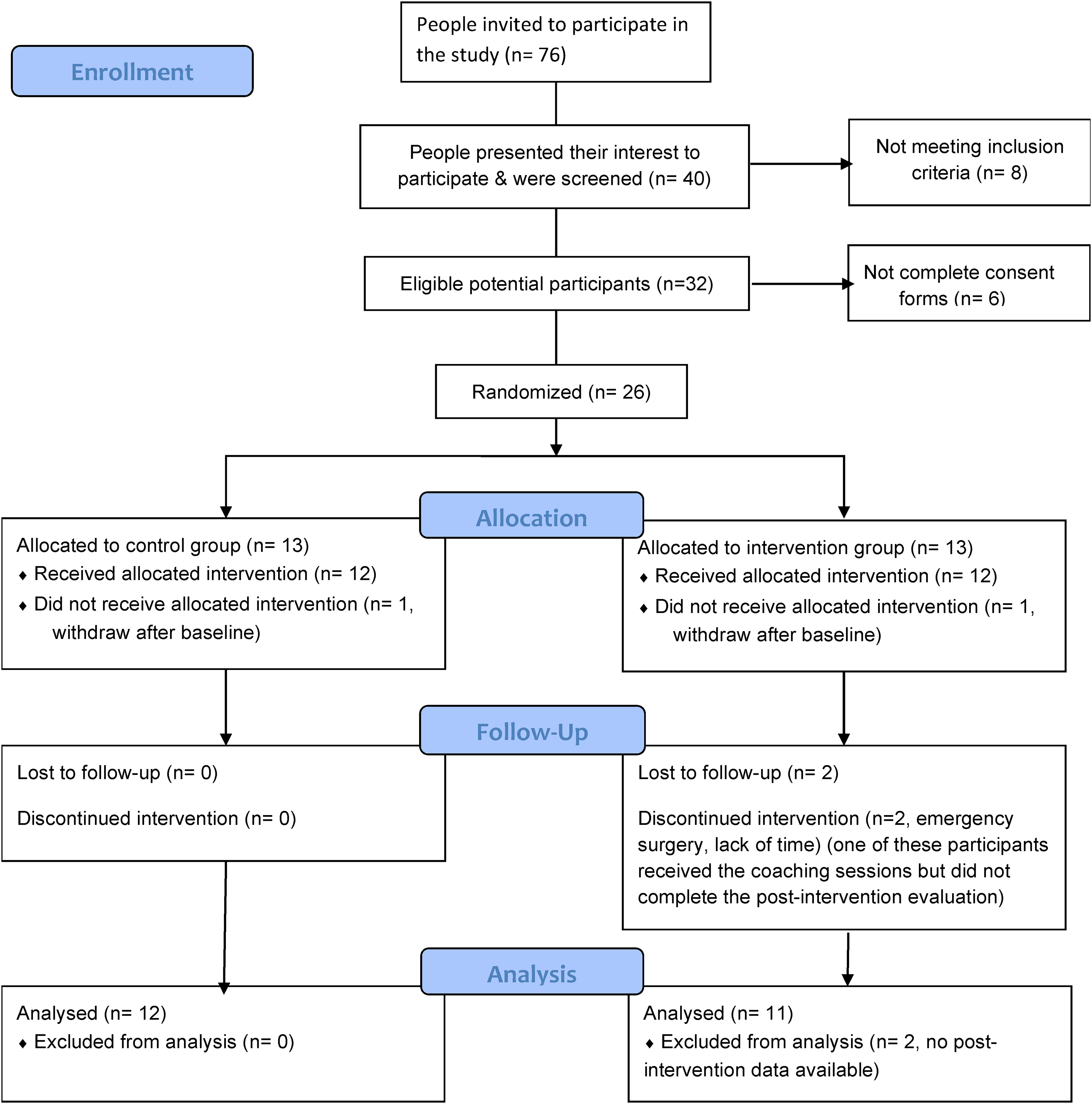
Flow diagram.
Participants’ characteristics and demographic information.
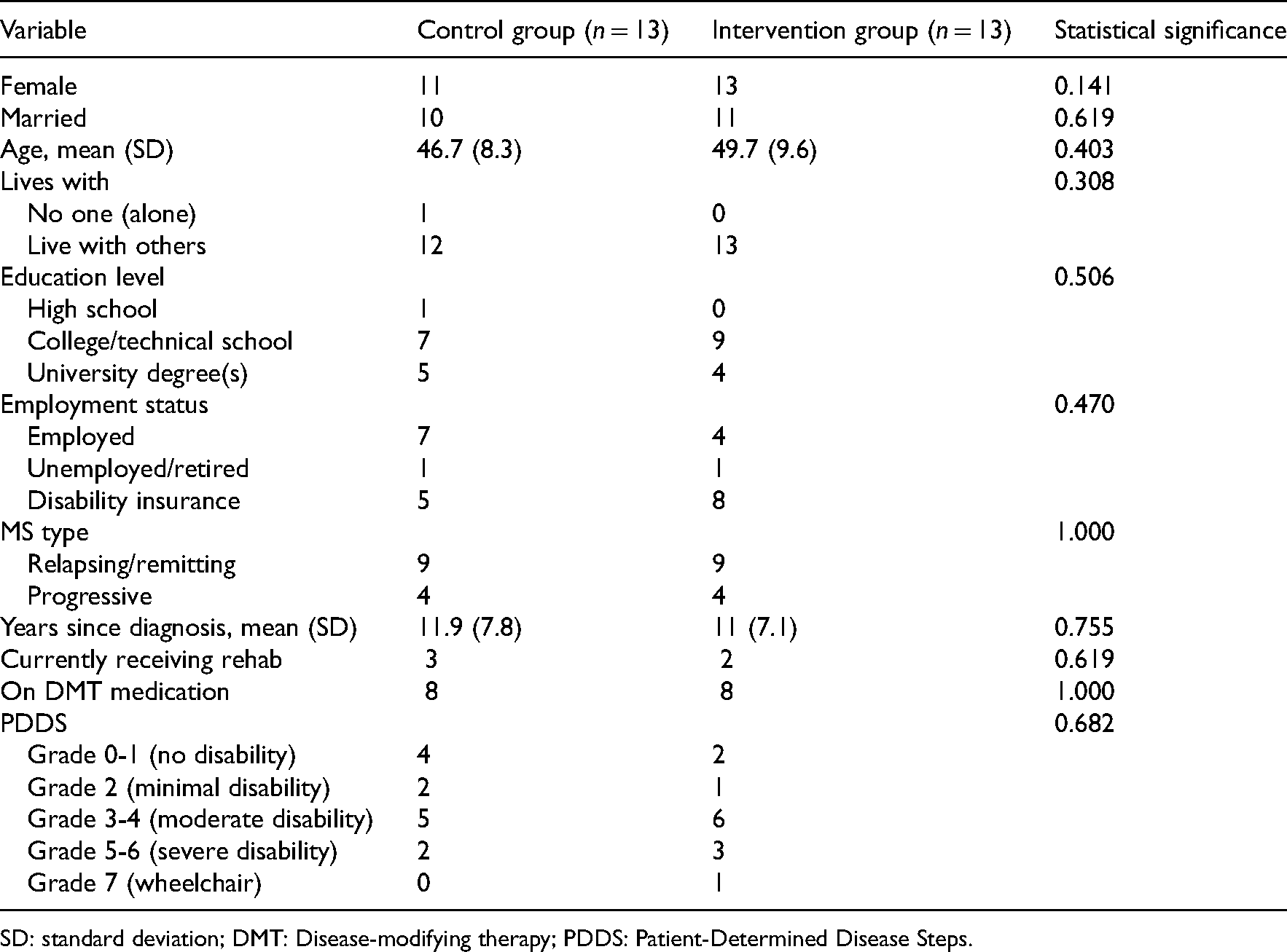
SD: standard deviation; DMT: Disease-modifying therapy; PDDS: Patient-Determined Disease Steps.
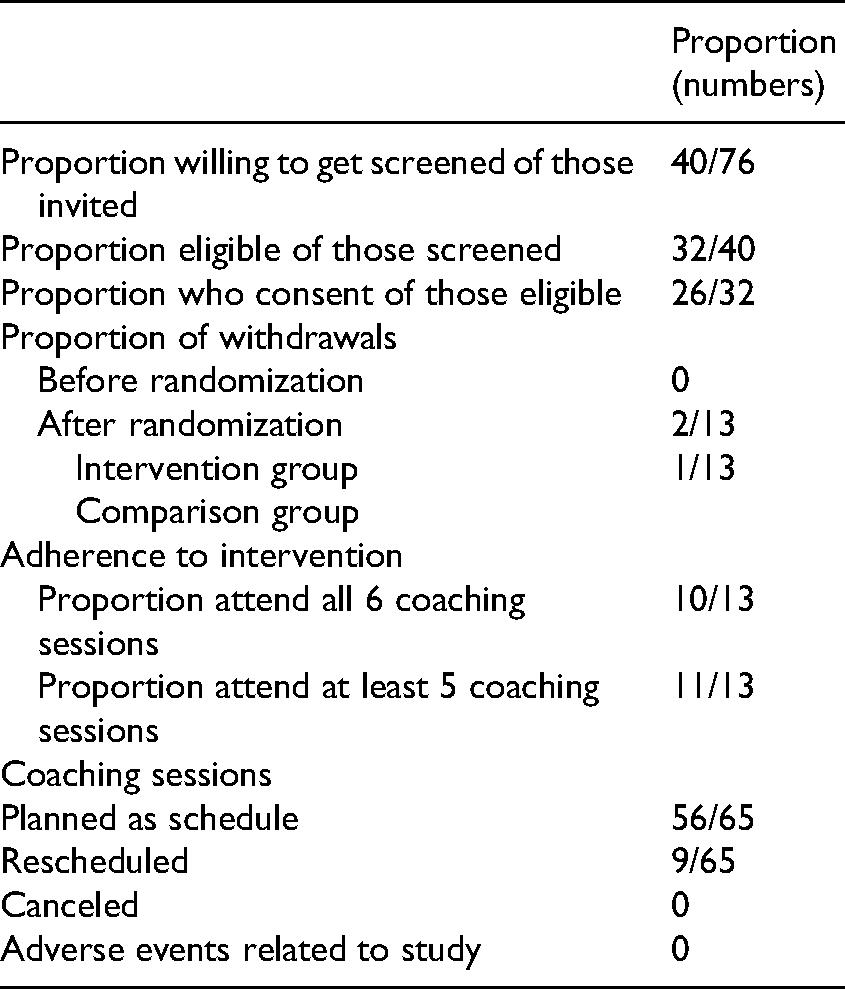
Feasibility of intervention
Table 4 details the feasibility results. Eligibility criteria were clear and not too restrictive. Each coaching session took between 35 and 60 min. The coaching outline was flexible, and the research team did not encounter difficulties scheduling the coaching sessions for participants. Using phone calls to deliver the coaching sessions was very effective as everyone had access to either a landline or cell phone. Having three research assistants enabled our team to be flexible in scheduling the assessment and support phone calls. Booking the next call usually took less than 5 min for each participant.
Feasibility outcomes.
Acceptability of the study was evidenced through qualitative feedback obtained from participants collected post-study via interview, low levels of missing data, and good retention of participants through study completion. According to our participants’ feedback, the structure of the program was generally well accepted, but the type of information presented on the website was perceived as “not new” or “to be more tailored to a newly diagnosed individual than a veteran.”
During the post-study evaluation, participants in the intervention group were asked about the usefulness of the program. On a scale from 0 to 10, the average rating for the usefulness of the intervention for managing fatigue was 8.8 (SD = 1.5; range: 6–10) for the add-on coaching sessions together with the website. The post-study interviews (n = 11) also revealed that most participants appreciated combining the coaching sessions with the website as they expressed the “website on its own would not have been as effective/useful without coaching,” “coach helped make things more clear and attainable regarding goal setting on website,” “the coaching sessions kept me focused on my goals and accountable,” and “ talking to a “live person” and “discussing the details of goals was great.” Participants expressed that the goal setting and coaching sessions were the sections they found most useful out of the intervention.
When asking participants how to improve the intervention program, some participants suggested adding more coaching sessions to have more time to practice and to work to generalize strategies to the other aspects of life. Participants also offered suggestions for modifications to website layout and operation including:
ability to integrate coach notes into the website for the user to access, being able to add to the bank of strategies when coming up with a new strategy specific to your goal, and adding a section for peers to share the experience.
Effect of intervention on fatigue and self-efficacy
Table 5 compares the efficacy of the intervention between the intervention group (n = 11) and the comparison group (n = 12). The coaching intervention showed a moderate effect on improving fatigue in daily life and self-efficacy of people living with multiple sclerosis. The intervention group showed more improvement than the comparison group in fatigue impact; however, the difference between the groups was not statistically significant. The coaching intervention group also showed more improvements in self-efficacy compared to the comparison group; however, the difference was not statistically significant. No adverse outcomes related to the intervention program were reported.
Group difference in fatigue effect and self-efficacy at baseline and post-intervention.
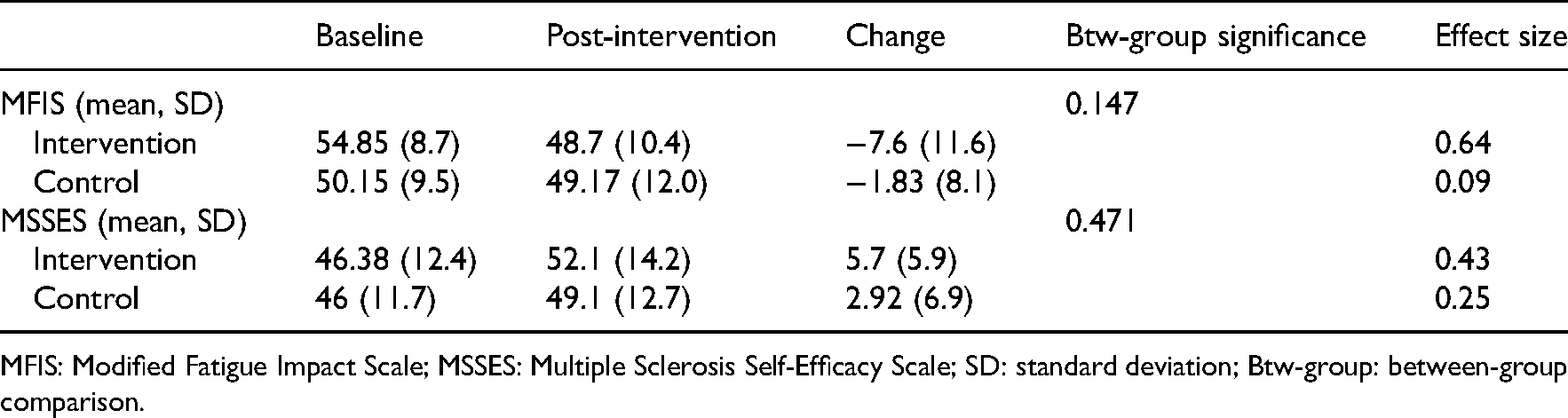
MFIS: Modified Fatigue Impact Scale; MSSES: Multiple Sclerosis Self-Efficacy Scale; SD: standard deviation; Btw-group: between-group comparison.
Website use and intervention fidelity
On average, participants in the intervention group used the website 35 times during the 12 weeks of the study and spent 3 h and 20 min navigating different sections of the website. The most frequently visited sections of the website were: goal setting, management strategies, basics of fatigue, and cognitive fatigue. In comparison, during the same study period, participants in the comparison group used the website an average of 4 times and spent 17 min navigating the information on the website. All participants in this add-on study downloaded the resource files that provide general information about fatigue and its management in multiple sclerosis.
Participants in the intervention arm achieved delivery fidelity on the MS INFoRM website. For 10 out of 11 participants in the intervention group who completed the study, they viewed all relevant sections related to their goals at least twice per month in the three-month intervention period. Receipt fidelity was not achieved as only six out of 11 participants downloaded the fatigue tracking sheet, and three intervention participants downloaded the Canadian Physical Activity Guidelines for multiple sclerosis. 16 However, 10 intervention participants used the website to track their fatigue, and two participants logged in every day during the study period and entered their fatigue rating. Enactment fidelity was achieved as participants in the intervention arm experienced a reduction in the impact of fatigue and increased self-efficacy between baseline and three months; this would imply that participants were using the strategies effectively in their everyday lives.
Coaching fidelity was measured by the occupational performance coaching fidelity measure. Fidelity scores of 80% or higher were reached consistently during coaching with the first five participants.
Discussion
We added-on a feasibility study to a randomized control trial of MS INFoRm in order to examine whether the addition of occupational performance coaching would enable PwMS with severe fatigue to benefit from the website. This combination of coaching and the website is a novel intervention using multi-modal strategies to enable PwMS to better manage their severe fatigue. This study included a fairly homogeneous group of PwMS with moderate self-reported disability and high fatigue severity, as measured by the MFIS. Our study demonstrates that it was feasible to recruit PwMS living with severe fatigue and to retain them in the three-month study. Adherence to the intervention was high, and the study procedure and outcome measures were acceptable for participants. A post-intervention feedback survey suggested that the intervention was well-received and that participants found the intervention useful, especially the coaching section.
Intervention acceptability was evidenced by high adherence, low withdrawal, no canceled sessions, and extensive use of the website. On average, participants in the intervention group used the website more frequently than the comparison group and spent more time navigating different sections of the website. Increased use by those in the coaching group may be explained by the presence of the coach facilitating the use of the information on the website and through making the website content relevant to participants’ individual goals. We had postulated that simple access to the MS INFoRM website for fatigue self-management strategies would not be enough for those PwMS living with severe fatigue. We believed that the presence of severe, disabling fatigue levels would deter PwMS from accessing the website on their own, and would deter them from pursuing and carrying through strategies that might be helpful in reducing fatigue levels.
Low attrition and high completion rates (85%) suggest that the study procedure and outcome measures were acceptable to the participants. Similar to our study findings, a teleconference-delivered fatigue management program for people living with multiple sclerosis 20 reported a completion rate of more than 90%, and a study on multiple sclerosis TeleCoach designed to enhance physical activity levels to improve fatigue in people living with multiple sclerosis had a completion rate of 76%. 21 Therefore, our completion rate is consistent with other studies. Possible reasons for our high coaching intervention arm completion rate in addition to achieving outcome measures, include having an occupational therapist trained in delivering occupational performance coaching in addition to a trained research assistant experienced in communicating with people with chronic disorders, and in using an assessment package with scripted instructions.
According to Henson (2016), “between 64% and 82% of people with multiple sclerosis seek health information online” 22 (p. 948). Accordingly, these individuals may need assistance to interpret and incorporate this information into their daily life through active collaboration with a professional, especially those PwMS living with severe fatigue. Participants in the MS INFoRm + coaching group were provided with online evidence-based information but were also able to explore its meaning and application to their lives during coaching sessions with an occupational therapist. Although the outcome data in this feasibility study are only indicative, they showed positive changes for people who received coaching, which may suggest that therapists or coaches are the active ingredients of the treatment process and its effects.
Telephone delivery of the intervention appeared to be acceptable to all participants. Recruitment targets were met quickly, suggesting that PwMS with self-reported high levels of fatigue are self-motivated to receive such treatments. Qualitative feedback was largely positive, with many participants finding MS INFoRm + coaching very helpful in setting their goals and managing their fatigue. The telephone coaching sessions were also seen by most as a critical component of the intervention. Some participants recommended updating the content of the website to keep the users up to date. Additional feedback was given to improve the intervention; the suggested revisions and adding features to the website will improve the intervention for future users.
The adherence data suggests that participants could complete the program within 12 weeks. However, some participants suggested adding more coaching sessions, so they could practice generalization with the coach's support. This may be needed for an individualized approach to fatigue management for PwMS, and as people move along unique trajectories in addressing their needs. Other coaching studies also consisted of 6–7 coaching sessions in a 12-week period. 23 Continued efforts to further refine such coaching programs will help to optimize the role of add-on coaching in multiple sclerosis self-management programs.
The MS INFoRm + coaching intervention, like other telerehabilitation interventions, has the potential to be flexible regarding time and location of delivery, to be complementary to existing rehabilitation and healthcare services, and to stimulate self-management skills in PwMS. In this study, supplementing access to the MS INFoRm website with coaching sessions conducted by an occupational therapist enabled the participants to talk about personalized goals with the therapist, and to find ways to adapt general strategies introduced on the website to their real-life, unique situations. Coaching skills likely influence the intervention effects 24 ; coaching support in this study was provided by a registered occupational therapist trained in delivering occupational performance coaching sessions.
Our study results provide preliminary evidence to support the benefits of combining online fatigue self-management strategies contained within the MS INFoRm website and coaching sessions. This was suggested, particularly in fatigue impact levels and self-efficacy scores after 12 weeks of intervention for severely fatigued PwMS. These findings are consistent with other studies that showed the effectiveness of coaching on self-efficacy. 25 However, larger studies are needed to fully explore the impact of combining directed fatigue coaching over a short-term period (3 months) with self-management strategies recorded on a fatigue management website such as MS INFoRM.
The current study was a small feasibility trial of people living with multiple sclerosis recruited from those with fatigue levels too severe to participate in a larger study examining the effects of using the MS INFoRM website to help manage mild to moderate levels of fatigue. This was designed to examine the feasibility of delivering add-on coaching to those very disabled from their severe fatigue over the short term of 3 months. Therefore, there was no long-term follow-up data on the effectiveness, feasibility, and impact of add-on coaching. A larger trial, with at least 80 participants (calculated based on the estimates of effect size), is now needed with longer-term follow-up to allow a quantification of the effects of the MS INFoRm + coaching upon the lives of PwMS with severe fatigue and an assessment of maintenance of treatment gains over longer time periods. In addition, an add-on trial of coaching to MS INFoRM website access to those PwMS living with mild to moderate levels of fatigue might also provide useful information on how to best help PwMS living with any amount of fatigue. The eligibility criteria, allocation and evaluation process, number of coaching sessions and coaching protocol, and the delivery of coaching were strengths of the study. It is suggested to add an outcome measure for goal achievement to better compare the groups and the effectiveness of the intervention such as the Goal Attainment Scale.
Clinical messages
Adding occupational performance coaching to a web-based fatigue management resource is feasible.
Findings suggest that a trained coach can support people with multiple sclerosis to better understand and apply the evidence-based information to manage their fatigue.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National MS Society Mentor-based Post-doctoral Fellowship Award (grant no. MB0028) granted to Dr Finlayson to cover the time of Dr Sorayya Askari.