
Abstract
Objective
To study the long-term effectiveness of case-management rehabilitation intervention on vocational reintegration of patients after myocardial infarction (MI).
Design
Blinded simple randomization was used to construct an intervention and control groups that were followed up for two years.
Subjects and setting
151 patients, aged 50.3 ± 5.9 years, who experienced uncomplicated MI and were enrolled in a cardiac rehabilitation program were recruited.
Interventions
included an early referral to an occupational physician, tailoring an occupational rehabilitation program, based on individual patient needs, coordination with relevant parties, psychosocial intervention, intensive follow-up sessions during a two-year follow-up.
Main measures
Return to work within six months of hospitalization and maintenance of employment at one and two years of follow-up.
Results
Return-to-work (RTW) rate in the intervention group was 89% and nearly all maintained employment at one year of follow-up (92%) and two years of follow-up (87%). Moreover, almost all of them returned to and maintained their previous jobs. The corresponding figures were: 98%, 94% and 98%, respectively. The figures for the RTW and employment maintenance for the control group were: 74%, 75%, and 72%, respectively. Only about 75%, in this group kept their previous job. The case-management intervention was associated with increased odds of maintaining employment at follow-up of one year (OR = 5.89, 95% CI 1.42–24.30) and two years (OR = 3.12, 95% CI 1.01–10.03).
Conclusions
The extended case-management rehabilitation intervention had a substantial positive impact on both the RTW of MI patients and their maintenance of employment at one and two years of follow-up.
Trial Registration
This trial is registered at US National Institutes of Health #NCT04934735.
Introduction
Cardiac rehabilitation is a recommended aftercare for patients with established coronary heart disease, 1 with return-to-work being one of its major goals. 2 Long-term follow-up studies of cardiac patients indicate that although the initial rate of return-to-work may be high, ranging between 67–93% during the first year, 3 adverse changes in employment status may occur later. Nearly a quarter of the patients may be detached from employment due to cardiac and non-cardiac reasons. 2 After 2–3 years from the event, about 70–76% of patients are employed4–6 and only 64% of those still employed, are working full time. 4
Mounting evidence suggests that vocational reintegration of cardiac patients is not necessarily associated with cardiac functions but rather determined by demographic (e.g. age and gender), occupational (e.g. blue-collar work), and psychological factors (such as depression and expectations concerning work,.3,7–12 The significance of occupational assessment, provision of individualized clinical data, physical possibilities and vocational information has been shown to increase the return-to-work rate, promote early return-to-work, and reduce medical costs.10–12 In their study, Froom et al. have shown the importance of early intervention by showing a 30% decrease in the chance for full employment 24 months after an acute myocardial infarction for each month's delay in referral. 4
This study draws upon the principles of disability management in the industry, 13 in which case management plays a major role. To date, there is no study that documented the effectiveness of case management for the vocational rehabilitation of cardiac patients. We examined the efficacy of a two-year occupational rehabilitation intervention, provided by a single case manager within an occupational health clinic, aimed to optimize work integration of post-acute myocardial infarction patients. Elements of this intervention included: planning an occupational rehabilitation program, coordinating between all relevant parties, and providing psychosocial support and guidance in coping with the negative medical, occupational, and personal changes that might occur during this period.
The effectiveness of the intervention in facilitating return-to-work, specifically to the same job, and long-term maintenance of employment after a cardiac event was assessed through a randomized controlled trial conducted for acute myocardial infarction patients, who were employed before the event, and enrolled in a cardiac rehabilitation program.
Methods
This trial conforms to the CONSORT statement guidelines (Consolidated Standards of Reporting Trials) and the protocol has been registered in the US National Institute of Health (ClinicalTrials.gov) registry #NCT04934735. The study, conducted between 2007–2011, received ethical approval from the Maccabi Healthcare Services review board, serial number 2006038. This study was supported by the Social Security Services of Israel, “The Fund for Demonstrating Projects”, The Ministry of Labor and Social Affairs, Jerusalem, Israel (Budget item number 21020201), and Maccabi Healthcare Services, Israel. It was supervised by a steering committee, appointed by the supporting fund, and headed by a senior rehabilitating cardiologist
This is a randomized, controlled, and comparative study with parallel groups conducted among patients who experienced an uncomplicated acute myocardial infarction (see Results section) that were either hospitalized for acute myocardial infarction or undergoing cardiac rehabilitation in either private healthcare or a public health fund. Each participant signed a written informed consent before enrollment in the study.
The study was designed to prospectively assess the effectiveness of case-management rehabilitation intervention conducted within an occupational medicine clinic. The effectiveness of the intervention was measured by the participants’ return-to-work rate within six months after the event, and by their maintenance of employment at one and two years of follow-up.
During hospitalization or immediately upon entering a cardiac rehab program, eligible patients were given a description (verbal and written) of the rehabilitation program by the program nurse, were asked to sign an informed consent form, and complete a baseline questionnaire as provided by a research assistant. Two weeks after hospitalization patients were referred to an examination by a cardiologist (to obtain a standardized clinical examination for all participants). Following this examination, the patients were assigned to an intervention group and a control group using blinded simple randomization based on a computer-generated random sequence of numbers. The intervention group received an extensive case-management rehabilitation program (described below). The control group received the standard care of cardiac rehabilitation which focuses on improving daily function and reducing cardiovascular risk factors, namely: lowering blood pressure, improving lipid and diabetes control, nutrition counseling, and smoking cessation. 14 The study participants were followed up (through a phone interview) at 6, 12, 18, 24 months after entering the study. The follow-up was conducted by the case manager for patients in the intervention group, and by a research assistant for patients in the control group. Medical data were retrieved from the computerized medical records in the relevant hospitals.
Baseline data included demographic data, occupational characteristics before the event, psychological factors, and medical data. The list of variables studied appears in Tables 1 and 2. Depressive symptoms were assessed by the validated measure of the Patient Health Questionnaire 8 (PHQ8, 15 Cronbach's α coefficient = 0.86). Patients’ subjective expectations (during hospitalization or immediately thereafter) of personal outcome after myocardial infarction, were measured by a 14 items scale, adopted from the 29 items questionnaire of expectations for future functioning. 16 It was comprised of two subscales (7 items each): negative expectation concerning the capability of functioning in daily life, and ability of return-to-work (α = 0.84 and 0.87, respectively). Medical data included: number and severity of myocardial infarction assessed by the New-York Heart Association (NYHA) functional class, 17 ejection fraction, signs of heart failure, and time of angioplasty.
Sociodemographic, occupational, and psychological characteristics of intervention and control groups.
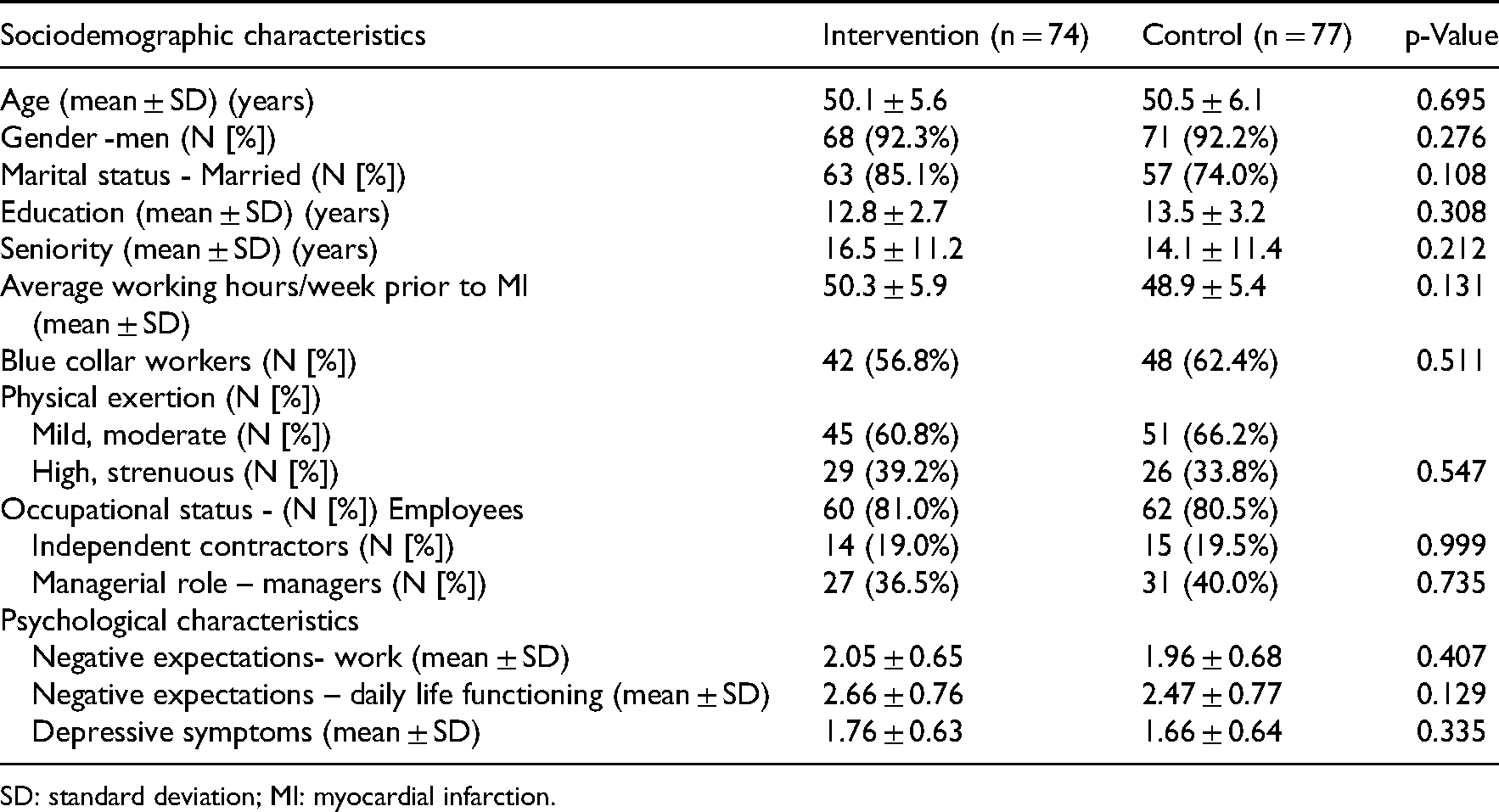
SD: standard deviation; MI: myocardial infarction.
Clinical characteristics of the intervention and control groups.
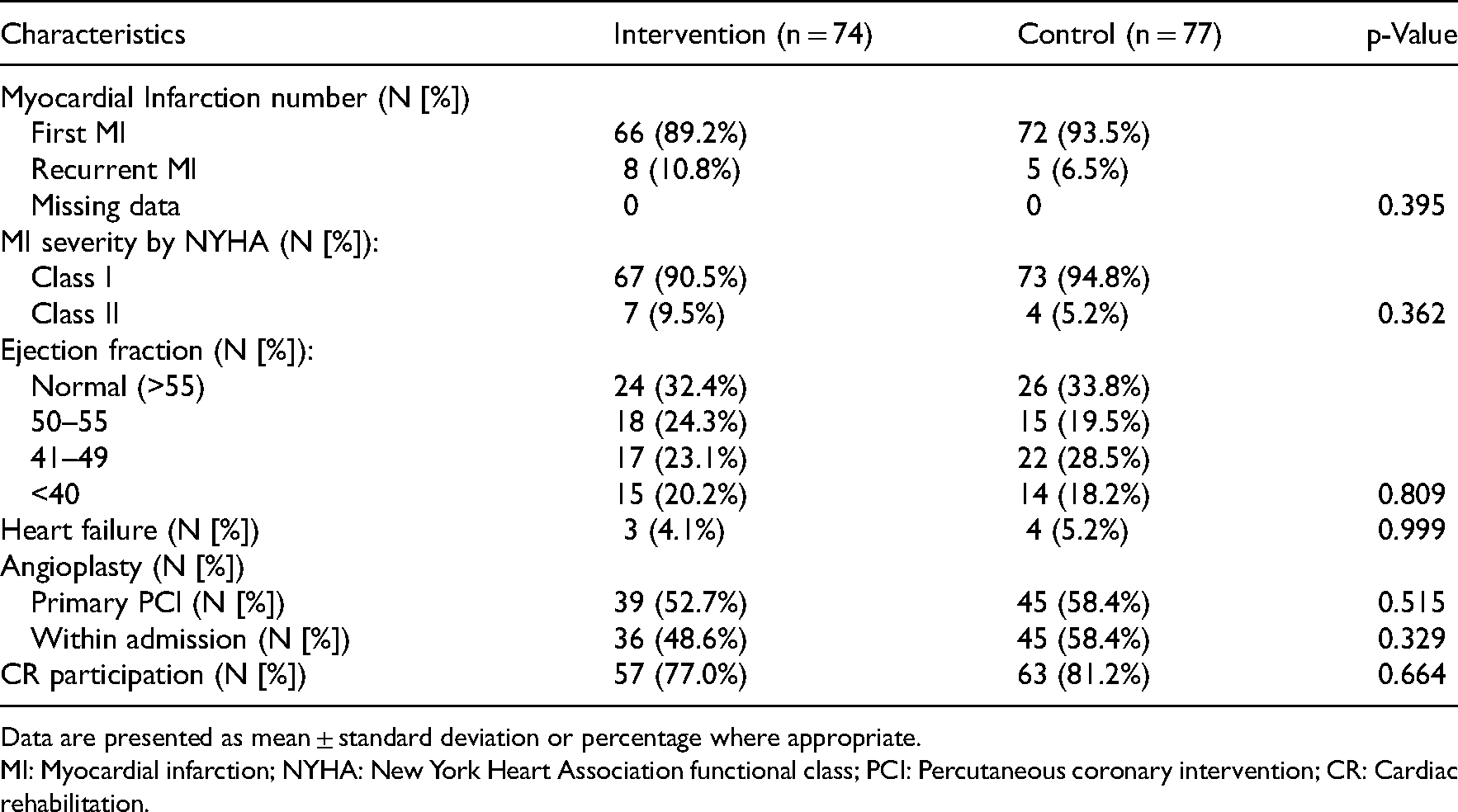
Data are presented as mean ± standard deviation or percentage where appropriate.
MI: Myocardial infarction; NYHA: New York Heart Association functional class; PCI: Percutaneous coronary intervention; CR: Cardiac rehabilitation.
Follow-up data were obtained through a short phone questionnaire concerning: working status (yes/no), time of return-to-work from the myocardial infarction, employment in the same job (yes/no), employment status (full time, part-time job), meeting with an occupational physician (yes/no), the occurrence of cardiac events during the preceding six months.
The case-management rehabilitation program was conducted using face-to-face meetings, by a clinical social worker within the occupational medicine clinic and included several components:
Intake by a case manager covering information relevant for tailoring the rehabilitating program according to the needs of individual patients, assessing the patients’ perception of their illness and the impact of the event on their life and family. Also included were: familiarization with the patient's occupational background, assessment of motivation, expectations, perceived efficacy and difficulties concerning return-to-work, and the identification of areas of intervention. Referral to further evaluation and treatment by a psychologist/psychiatrist was up to the case manager's discretion. Referral to an occupational physician was within one week of the intake. Charting an occupational rehabilitation program and timing the return-to-work date, not later than 35 days from hospital discharge. This time period was chosen being the earliest possible intervention window after the clinical rehabilitation. Before their return-to-work date, patients were invited for an additional meeting with the case manager to facilitate their readiness to return to work and make any necessary arrangements. Coordinating between the patients and their family, treating physicians, the employer, community services, and meeting with the patient's family – all on a needful basis. Provision of a guidance booklet for employers, produced by the National Institute of Environmental and Occupational Health, on the return-to-work of cardiac patients. Patients could read it by themselves and/or hand it to their employer. The psychosocial intervention was tailored to the patient's emotional state, occupational needs, and specific requests. When needed, short-term (up to four sessions) psychotherapeutic treatment was provided by the case manager to help alleviate anxiety and other debilitating concerns, illness misconceptions, family issues, and occupational wavering regarding when to and if to return to the same work. Intensive follow-up sessions, by the case manager aimed to ensure that the rehabilitation program was carried out as planned, were conducted two, four, and six weeks after the beginning of the psychosocial intervention. Patients who had return-to-work within three months after discharge from the hospital, received follow-up calls as follows: two weeks from the start of the case-management intervention, every two months during the first six months, and once every six months thereafter (as outlined above). If needed, one or more of the above interventions were applied.
Intervention during follow up included:
Patients who had not returned to work within six months after discharge, due to psychosocial or employer-related issues received up to 12 intensive intervention sessions, in which the relevant parties were involved. Upon successful return to work, the six months follow-up calls were resumed.
Patients who had not returned to work after six months for the above reasons and were assessed as having rehabilitation potential (were physically capable and expressed an explicit desire to return to work), were referred to the National Social Security rehabilitation services and were followed up monthly for one year. The case-management intervention was ended for patients without rehabilitation potential. For both groups, follow-up calls continued for six months.
Results are presented as mean ± standard deviation (SD) for continuous variables and as frequencies for categorical variables. Data were analyzed using the SPSS statistical package (Version 26, SPSS Inc., Chicago, IL). Student's t-test was used to test for a difference between the means of two groups on a continuous dependent variable. The Chi-square test of homogeneity was used to test for a difference between two proportions. For small groups, it was replaced by Fisher's exact test
A multiple logistic regression model was used to investigate the relationship between employment status (employed/unemployed) at one year and two years of follow-up and case-management program participation. Adjustments were made for factors that were found in previous studies to be associated with vocational re-integration and that could have confounded the findings of this study. A list of the possible confounders is presented in Table 4. Statistical significance was determined by p < 0.05.
Differences of the sociodemographic, occupational, and psychological variables by employment status at one and two years of follow-up (n = 151).
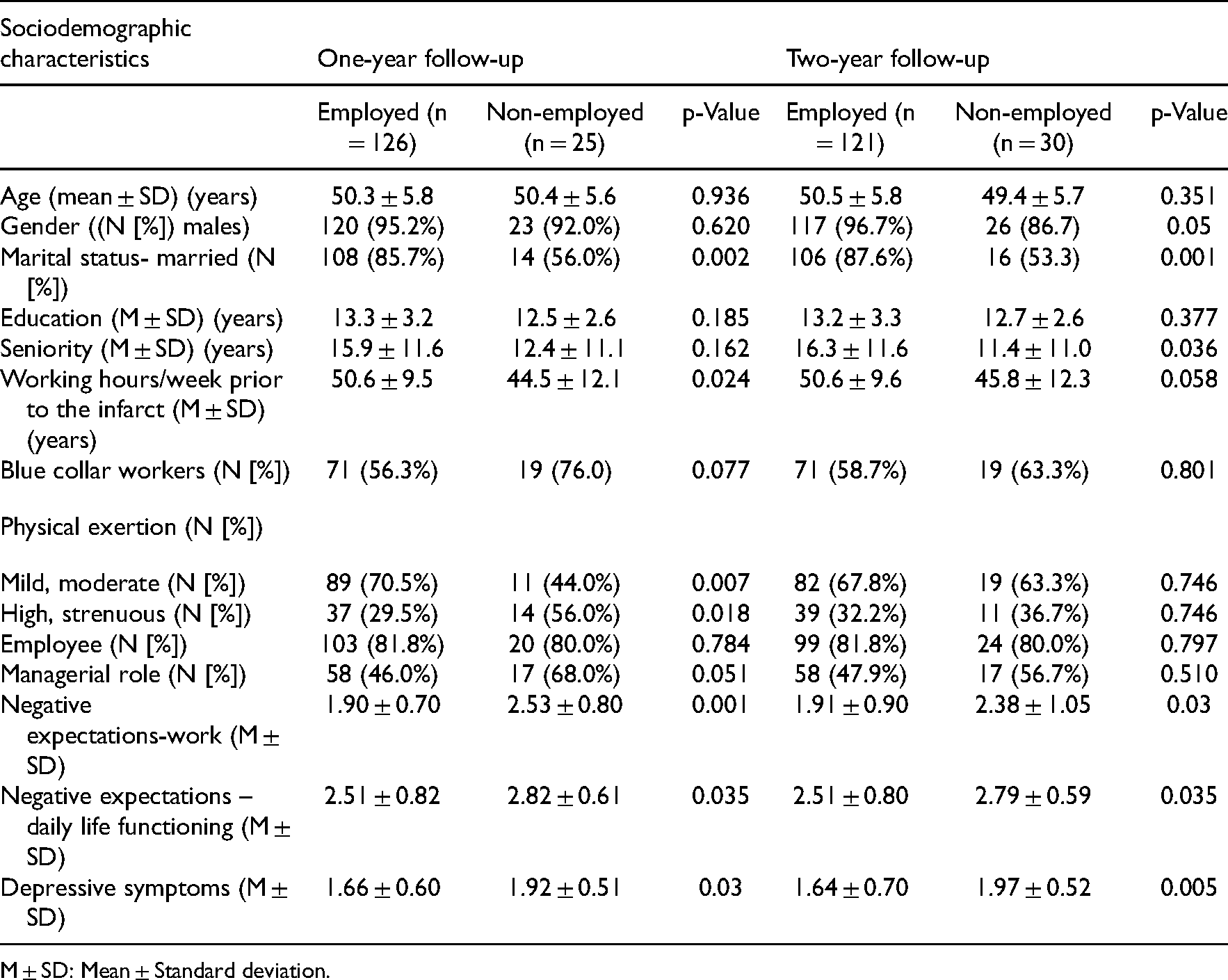
M ± SD: Mean ± Standard deviation.
Results
A total of 151 patients completed the study. The baseline sociodemographic, occupational, and psychological data are shown in Table 1, and the flow of patients is shown in Figure 1. Out of 168 patients identified for recruitment, 153 patients have met the inclusion criteria and opted to take part in the study. Patients were randomized into an intervention group (n = 74) and a control group (n = 79) of whom 2 were lost to follow-up (deceased).
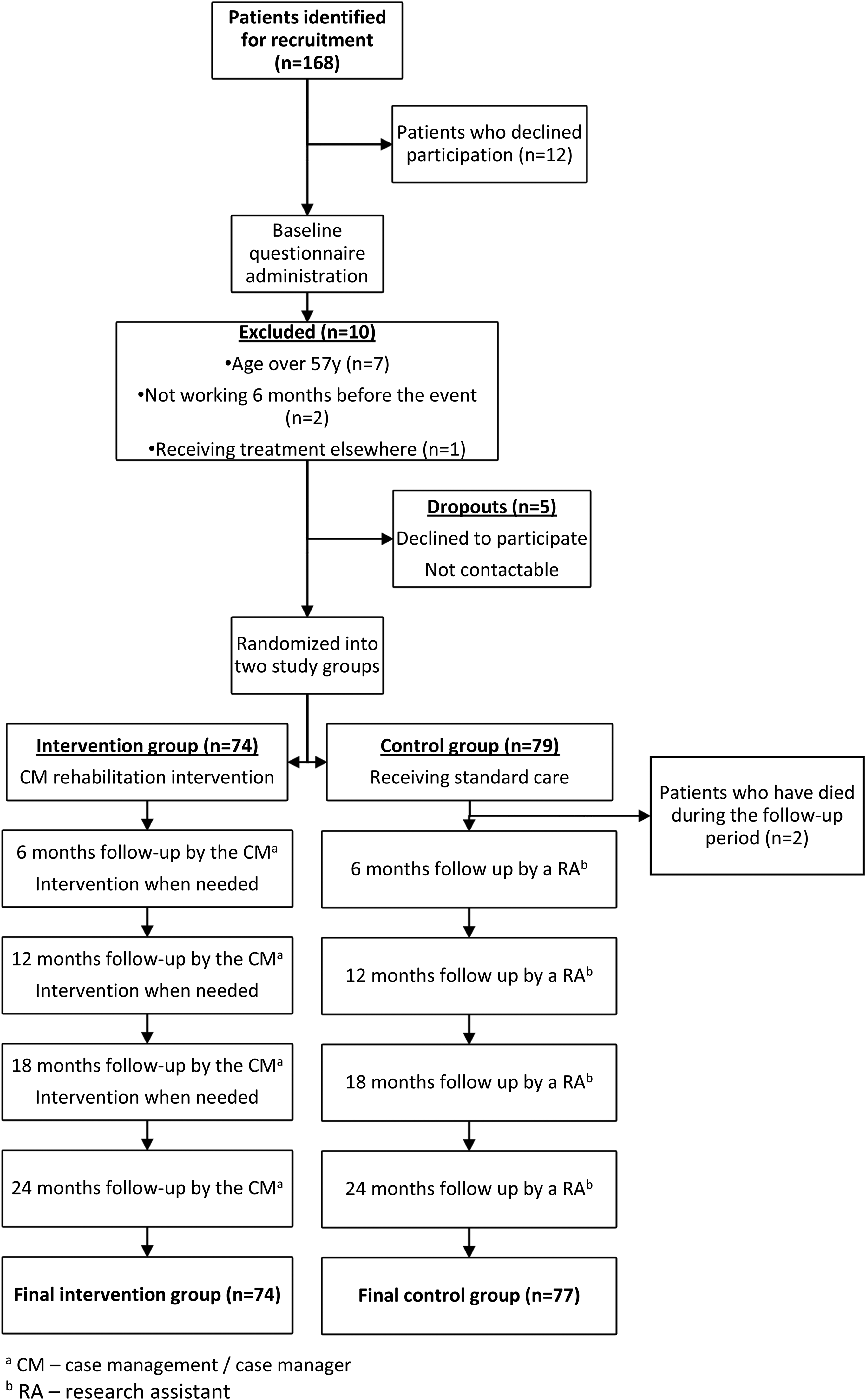
Flow chart of The study design.
Comparisons of sociodemographic (Table 1) and medical variables (Table 2) showed no statistically significant differences between the two groups supporting adequate randomization. Samples were diverse and included white- and blue-collar workers, independent contractors, and executives with an average education of more than 12 schooling years. Judging by the medical parameters, patients had undergone uncomplicated myocardial infarction, and in the majority of the cases, it was their first myocardial event. More than half of the patients had an intact ejection fraction (EF > 50%) and a New-York Heart Association (NYHA)-1 classification. No NYHA-3 or −4 patients were found. Only a few of the patients exhibited signs of heart failure.
The majority of study participants were enrolled in a cardiac rehabilitation program. The rates in the intervention and control groups did not differ statistically. During the first three months of follow-up, no statistically significant differences were found between the groups regarding occupational physician visitations (45% in the intervention group vs. 40% in the control group).
Table 3 summarizes the results for the outcome variables in this study. A clear difference emerged between the two study groups regarding the extent of work re-integration within six months of discharge from the hospital. Eighty-nine percent of the patients in the intervention group returned to work, and the majority of them (98%) resumed the same position/role. Eighty percent of those who returned to work were working full time. The corresponding figures for patients in the control group were: 74%, 73%, and 63%, respectively. All differences were found to be statistically significant (p = 0.0105, p < 0.0001, p = 0.0275, respectively). We found that the main reasons for not returning to work in the study group within the first six months were mainly medical.
Return-to-work rate and employment status at follow-up of the intervention and control groups.
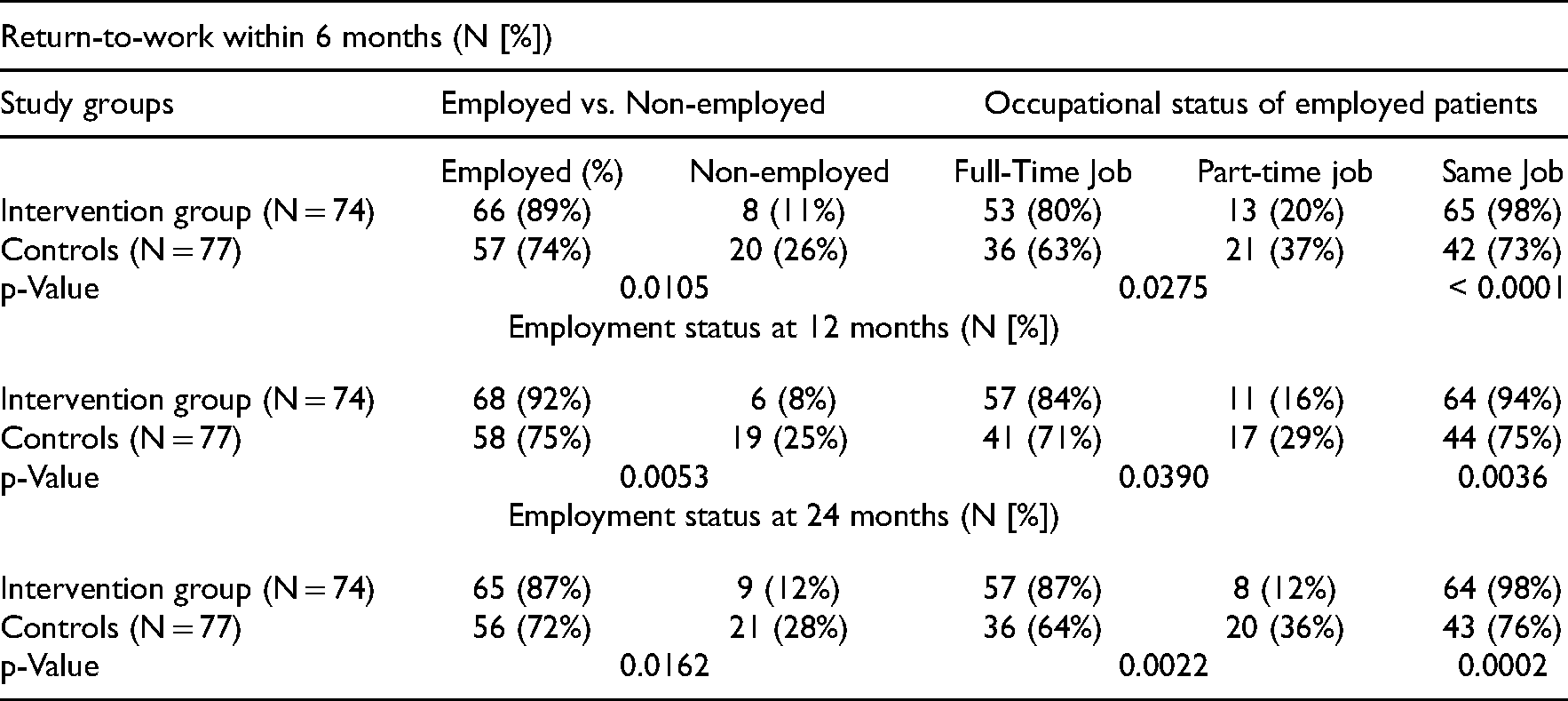
Also appearing in this table are the rates of those who maintained employment at one year and two years of follow-up. For sake of brevity, we do not present the figures for 18 months of follow-up. They are set in between the rates presented in the table and have no incremental value (but available from the authors upon request). In the intervention group, 92% were employed at one year of follow-up; of those, 94% retained the previous position/role, and 84% were working full time. The figures for the control group were notably lower and statistically significant with rates of 75% (p = 0.0053), 75% (p = 0.0036), and 71% (p = 0.039), respectively. The same trend was observed in the data from 2 years of follow-up. In the intervention group, 87% were employed at two years of follow-up of those 98% retained the previous position/role and 87% were working full time. The figures for the control group were notably lower with rates of 72% (p = 0.0162), 76% (p = 0.0002), and 64% (p = 0.0022), respectively.
No statistically significant difference was found between the intervention group and the control group regarding medical events that occurred during follow-up (diagnostic catheterization, percutaneous transluminal coronary angioplasty (PTCA), and hospitalizations).
The next step of the data analysis was to examine the value of baseline demographic, occupational, psychological, and clinical characteristics in predicting employment maintenance at one and two years of follow-up. The results are presented in Tables 4 and 5. Several of the sociodemographic variables were statistically significant predictors of this outcome at one year, two years of follow-up, or both (Table 4). The employed patients compared with the non-employed had a higher proportion of males and married patients. They had higher seniority, a higher average of working hours per week prior to the infarct, and were employed in jobs with mild or moderate physical exertion. Interestingly, only a low percentage of these patients occupied managerial roles. Furthermore, all three psychological variables were found to be predictors of the studied outcome. The employed patients had lower mean scores of negative expectations concerning return-to-work and functioning in daily life. Furthermore, they had a lower level of depressive symptoms.
Differences of the medical parameters at one and two years of follow-up, employed vs. non-employed subgroups.
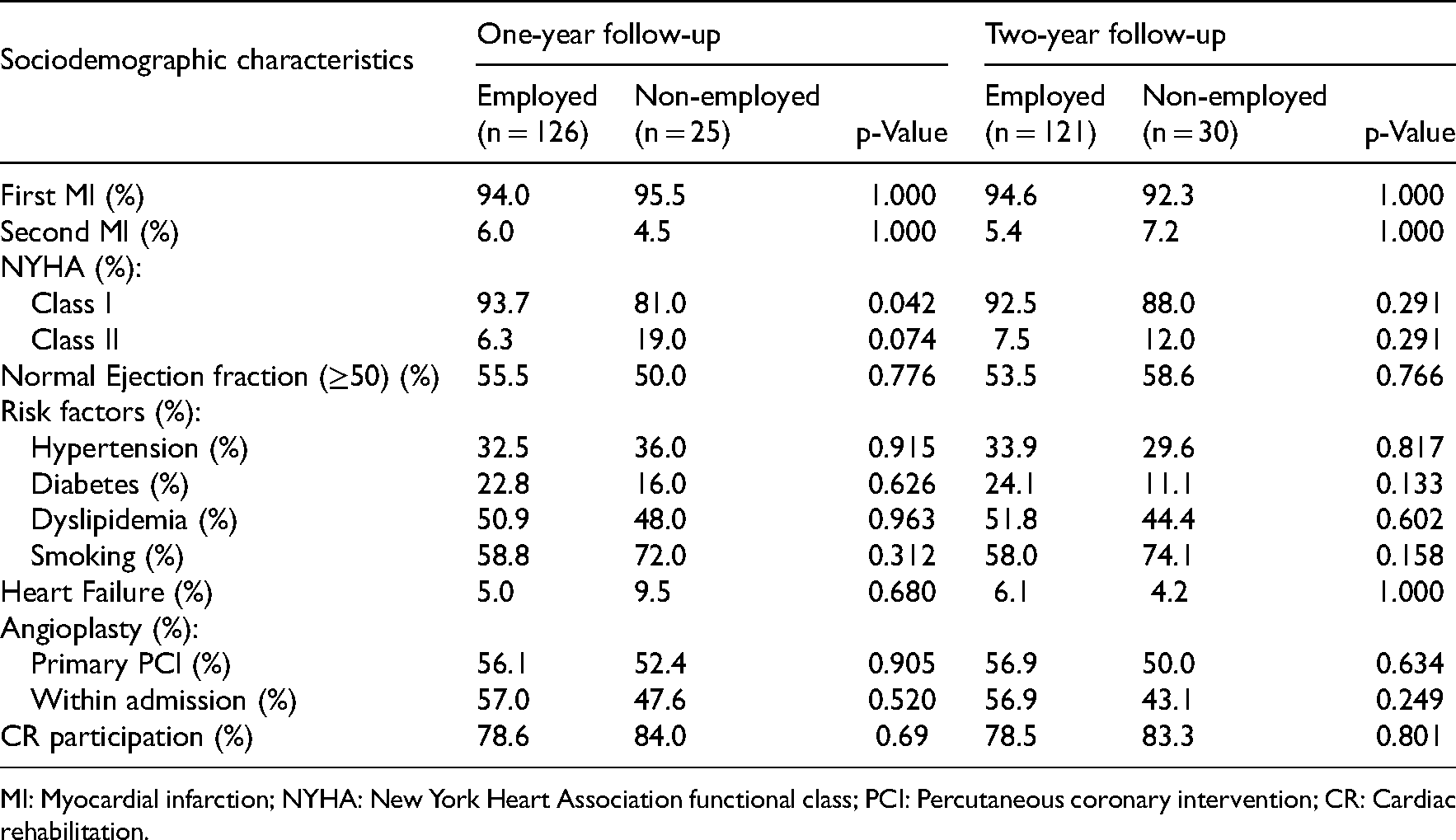
MI: Myocardial infarction; NYHA: New York Heart Association functional class; PCI: Percutaneous coronary intervention; CR: Cardiac rehabilitation.
Except for one variable, none of the medical variables turned out to be statistically significant (Table 5). Employed patients had a significantly higher proportion of mild myocardial infarction (NYHA class I). Finally, no difference between the groups was found in the percentage of patients attending the cardiac rehabilitation program. The rates at one year of follow-up were 78.6% and 84.0% for employed and non-employed patients, respectively. The respective corresponding percentages for two years of follow-up were 78.5% and 83.3%.
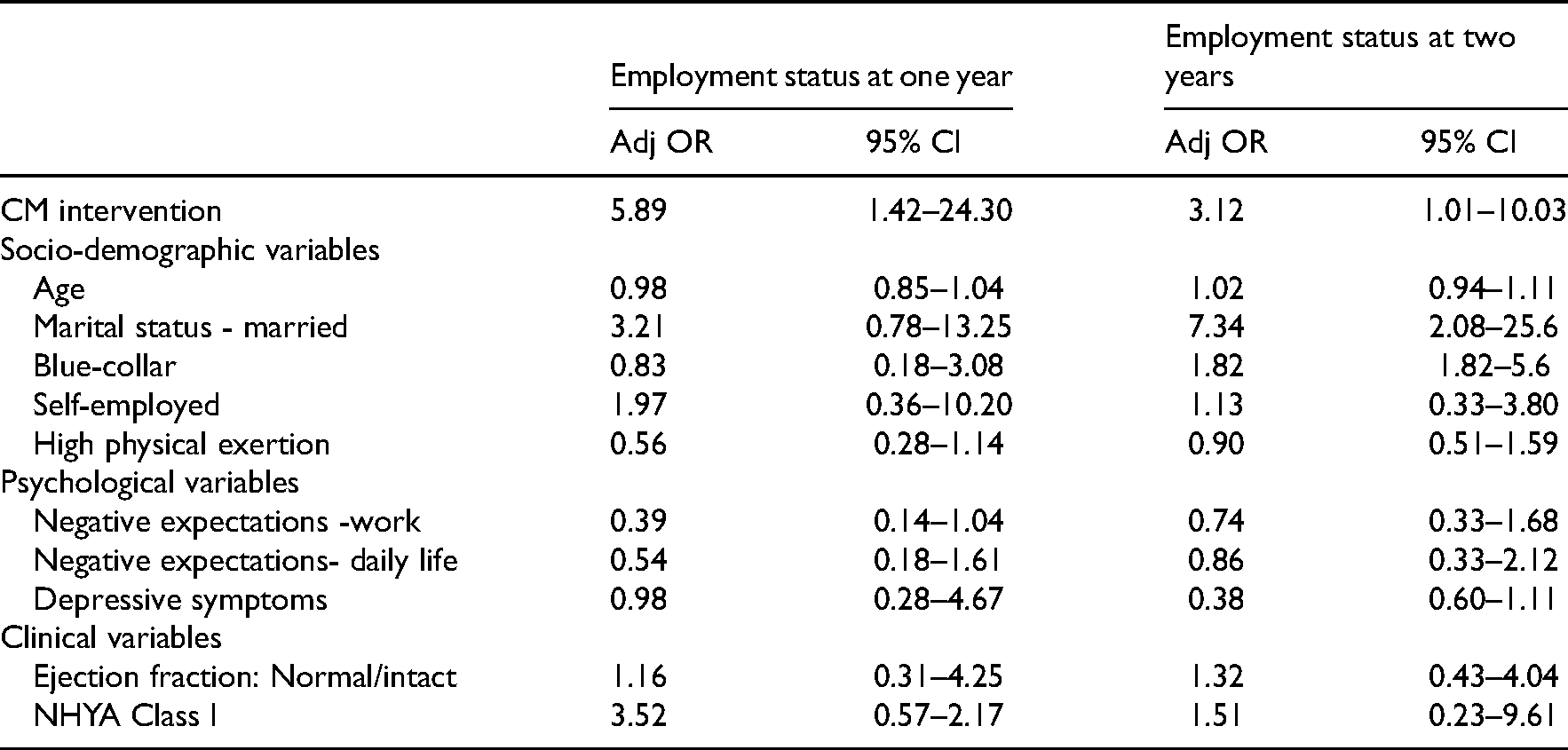
Table 6 presents the results of logistic regression analysis testing the relationship between employment status at follow-up and case manager intervention while adjusting for potential confounding variables. The case manager intervention was associated with increased odds of maintaining employment at follow-up of one year (OR = 5.89, 95% CI 1.42–24.30) and two years (OR = 3.12, 95% CI 1.01–10.03), after adjustment for sociodemographic, occupational, psychological, and clinical variables.
Results of logistic regression analysis of employment status at one and two years of follow-up by CM intervention, adjusting for potential confounding variables.
Discussion
This randomized controlled trial was aimed to prospectively assess the effectiveness of an extended case-management rehabilitating intervention on vocational reintegration of patients who underwent an uncomplicated acute MI. The findings indicated that 89% of the patients in the intervention group returned to work within six months, which was significantly higher than the rate for the control group (74%). Moreover, 98% of the former group have returned to the same job, at a significantly higher rate than in the latter group (73%). The high RTW rate in the intervention group was similar to the 96% reported in another study in which a comprehensive rehabilitation program was employed. 7 These rates were higher than those reported in other studies of long-term follow-up of over 12 months, which added psychological intervention to the usual care. In the intervention groups, the median RTW rate was 75.5% whereas in the usual care groups it was 66.6%.18–24
The effectiveness of the case management program, as outlined above, can be attributed to several factors such as early intervention (during hospitalization or immediately thereafter); an early referral to the occupational medicine clinics; and charting an occupational rehabilitation program, all in addition to the provision of brief psychosocial intervention. The early return-to-work prevented the phenomena often observed for patients with long sick leave, having their job modified or replaced by other workers 25 and we believe this explains the high rate of return to the same job observed here.
The major findings of this study were that case management was associated with 5.9-fold increased odds of maintaining employment during one year of follow-up, even after adjusting for demographic, occupational, psychological, and clinical factors. Ninety-two percent of the patients were employed at this time and of these, 94% remained in the same job. The corresponding figures for the control group were 75% and 75%, respectively. An encouraging finding in our study was the effectiveness of the intervention that persisted for two years after the event (OR = 3.1, 95% CI: 1.01–10.0). Eighty-seven percent of the intervention group were employed, and 98% of these have retained the same job. The corresponding figures for the control group were 72% and 76%, respectively. Not unexpected, the employment rate of patients in the control group, is very similar to that observed in other studies in which typically short-term cardiac rehabilitation was employed.4,6,26
The success of the comprehensive case-management program in facilitating long-term maintenance of employment may be explained, in addition to the factors mentioned above, by containing other components of disability management/vocational rehabilitation programs, suggested by rehabilitation specialists as important for enhancing work re-integration, namely: occupational counseling, monitoring and providing support and alleviating any difficulties during work reintegration, addressing personal and work related-obstacles that might affect an individual's decision to return-to-work, and providing coordination between all relevant parties.6,7,27,28
The majority of the participants in this study participated in a regular cardiac rehab program (see Methods). However, the findings here showed that rehab participation had no effect on employment status either at one year or two years of follow-up. No difference was found between the study groups in the participation rates in cardiac rehab programs. No or little effect of cardiac rehab enrollment on employment status was observed in many other studies;6,28 and was also the overall finding of Hegewald et al. 27 who conducted a systematic review of 39 randomized controlled trials that aimed to evaluate the effects of interventions intended to enhance return-to-work in patients with coronary heart disease compared to usual vs. no care. To illustrate, they found that person-directed combined interventions, applying both psychological counseling and physical conditioning versus usual care, may have increased return-to-work for up to six months. However, there was low-certainty evidence that such interventions increased the proportion of participants working in the long term (follow-up of 1 to 5 years, RR = 1.14, 95% CI 0.96–1.37). Furthermore, they even found that work-directed counseling by family physicians, nurses, and other clinicians, did not have a better impact on return-to-work. Thus, although the general expectation is that cardiac rehab programs, in addition to their benefits to health status and quality of life, would also facilitate return-to-work of patients with coronary heart disease, often this expectation was not met. It appears that these programs, which focus primarily on improving daily function and reducing cardiovascular risk factors, usually lacked many of the components that are directly relevant to work reintegration as listed above such as psychosocial and occupational counseling.
Consistent with findings of other studies,3,7–9 long-term employment in our study was not related to cardiac state or cardiovascular risk factors, nor was it associated with occupational factors. Rather, it has been shown to be related to the same demographic factors that were found to be positively related to return-to-work in the literature: male gender, married status, longer tenure, low intensity of physical effort, and higher income prior to the cardiac event.3,7 Moreover, our study shows that negative psychological factors turned out to be determinants of the detachment from employment at one- and two years of follow-up: negative expectations concerning return-to-work, daily functioning, and depressive symptoms, all congruent with the findings of other studies.8,16,29,30 Nonetheless, the intervention programs proved to be a powerful determinant of long-term employment over and above the demographic, occupational, and psychological factors.
The current prospective case-management intervention study has several strengths. To the best of our knowledge, it is the first study to examine the impact of such an intervention on return-to-work and maintenance of employment after acute myocardial infarction. The intervention was carried out by a single clinical social worker within the occupational medicine clinic for patients with acute myocardial infarction who participated in a cardiac rehabilitation program. It started very early, before the loss of fitness for work and adoption of the sick role, and in an effort to sustain the same employment. It commenced before or during the cardiac rehab program - timing which is consistent with the new guidelines on cardiac rehabilitation that strongly advise initiating return-to-work support during rehab and not after it has concluded. 27 The intervention was oriented towards vocational rehabilitation and contained many of the components, listed above, that are often missing in the regular rehab programs, including the one employed in the current study. As part of the intervention, the case manager coordinated simultaneously between all relevant parties, preventing the bouncing of patients from one body or one professional to another, and thus saving a lot of time. Patients continued to receive guidance and support long after the cardiac rehab program was completed, they were monitored every six months and had the case manager intervene when various difficulties (personal and occupational) arose during work reintegration. This has resulted in a prolonged period of maintaining employment. Moreover, these patients kept the same job they held before the event, at least for the duration of the follow-up – an outcome that is in contrast to the adverse changes in employment reported in the literature for coronary heart disease patients. Another important strength of this study is that the case management program helped facilitate work adjustment and re-integration of patients with coronary heart disease who were employed at different workplaces and was not dependent on the initiative and willingness of a given workplace to undertake case management of workers after a cardiac event. This study also contributed to the paucity of data regarding long-term work re-integrating of patients with coronary heart disease. The majority of the relevant studies in the literature (not reviewed here) were limited to no more than one year of follow-up.
The present study has several limitations. It was conducted for patients with uncomplicated (largely first) acute myocardial infarction, and we do not know how effective the case management program would be for patients with a more severe cardiac state. The case manager monitored the patients in the intervention group every six months during the follow-up period (see methods) and at the same time collected the follow-up data. Thus, stemming from the study design both the case manager and research assistant could not be blinded to their designated study group. Yet, both used the exact same standard follow-up phone questionnaire. Most of the patients participated in cardiac rehabilitation in conjunction with the case management intervention. It remains to be tested if case management intervention would be as effective for patients who do not participate in rehab. There are many patients with coronary heart disease who do not attend rehab programs despite a recommendation by their cardiologist to do so. 31 Unfortunately, the small number of subjects in the intervention group (n = 17) who did not participate in cardiac rehabilitation, did not provide sufficient statistical power to examine this issue here. Finally, the study participants’ place of work was not recorded in the data. This prevented us from testing, whether the benefits of the intervention were obtained irrespective of the place of work.
Clinical implications
Extensive case-management rehabilitation intervention program that starts before or during cardiac rehab and continues for two years after hospitalization may have a considerable positive impact on the return-to-work of cardiac patients to the same employer and the same jobs and more importantly, their long-term maintenance of employment This intervention should start early and include coordination between the relevant parties, provision of occupational counseling before resuming work and providing long-term psychosocial support before and after return-to-work. We recommend integrating a case manager in rehabilitation programs of post-acute-myocardial infarction patients as a means to encourage the return to full and gainful employment.
Future intervention studies aimed at enhancing the reintegration of patients with coronary heart disease in work could explore the possibility of incorporating into the classical cardiac rehabilitation programs various disability management components that are more directed towards the occupational rehabilitation of such patients. Alternatively, the application of long-term case management strategies may be provided by external occupational medicine professionals during and after the cardiac rehabilitation programs.
Clinical messages
A long-term case-management program among myocardial infarction patients that coordinates between relevant parties and provides psychosocial support alongside occupational counseling may facilitate their return to work and maintenance of their previous jobs.
It can be provided by occupational medicine professionals and included in the classical cardiac rehab programs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Security Services of Israel, “The Fund for Demonstrating Projects”, The Ministry of Labor and Social Affairs, Jerusalem, Israel (grant number Budget item number 21020201), and Maccabi Healthcare Services, Israel.