
Abstract
Objective:
To review children’s and their families’ needs after a child’s traumatic injury and assessment tools to measure needs.
Data sources:
Medline, Embase, CINAHL and PsycINFO databases (2005–September 2017) were searched and screened for papers (of any design) investigating children’s and families’ needs after a child’s traumatic physical injury.
Review methods:
Data regarding children’s and families’ needs were extracted by two independent raters. Methodological quality of the identified papers was not assessed. Thematic content analysis drew out the key needs.
Results:
A total of 12 studies were identified, involving 932 participants including 105 injured adolescents and 827 family members or professionals. The needs of children under 12 years were identified indirectly from families or professionals. Most studies focussed on traumatic brain injuries. Two groups of needs were identified: person-related and service-related. Person-related needs were categorized into adolescent-specific needs, need for support with cognitive, emotional, social and physical problems and help with practical problems. Service-related needs were categorized into the need for information, educational needs and support during care transitions (specifically access to community-based services). These needs were largely unmet, particularly regarding information, emotional support and care transitions, which were compounded by professionals’ limited understanding of the children’s difficulties. We found no published measurement tools to assess children’s and families’ needs after a child’s traumatic injury.
Conclusion:
The evidence about children’s and families’ needs following a child’s traumatic injury was limited, but needs for information, emotional support and access to community-based services were consistently unmet.
Introduction
Injury is the most frequent cause of death and disability in children and young people after the first year of life. 1 For example, ~5000 children per year are hospitalized with traumatic injuries in the United Kingdom, 20% of which are considered serious. 2 Consequently, paediatric trauma is recognized as an area that requires specialist rehabilitation from a multidisciplinary team to optimize the injured child’s activity, social participation and well-being, while reducing stress on carer/family. 3 The post injury needs are often multi-faceted and include psychological and social difficulties, as well as physical injuries. 4 Over the past 20 years, there has been increasing recognition that trauma care, particularly rehabilitation, is often sub-optimal.4 –8
There is therefore an imperative to improve the quality of and access to rehabilitation for children with traumatic injuries, but there is little research to inform service delivery. We know little about whether existing rehabilitation services meet the needs of injured children and how this impacts on their recovery from a physical, social and psychological perspective. A first step to designing and commissioning effective, evidence-based rehabilitation services is to understand the nature and extent of the children’s (and their families’) needs and how best to measure them. Thus, this study will explore the state-of-the-evidence regarding (1) the needs of children with traumatic injuries and their families and (2) methods of measuring their needs.
‘Need’ is a complex concept and numerous definitions have been proposed, without consensus.9 –12 In this study, need is defined as a problem that significantly interferes with daily life.11,12
The types of need to be considered have not been pre-specified, nor the help or services that may be required to address the problems and needs.
Method
Identification of papers
An exploratory scoping review was undertaken. 13 Relevant papers were identified by searching Medline, Embase, CINAHL and PsycINFO databases from 2005 to September 2017. Keywords relating to assessments, needs and trauma were used and limits were set to include papers only involving children (Supplementary Appendix 1). One author (S.J.) screened titles and abstracts and then two authors (S.J. and S.F.T.) independently screened full texts to determine which papers met the following inclusion criteria.
Inclusion and exclusion criteria
Papers that addressed the following were identified for inclusion:
The needs of children (aged 0–18 years) following traumatic physical injuries affecting any part of the body, resulting in an admission to hospital.
The needs of parents, carers (unpaid) and other family members of children with traumatic physical injuries.
Needs identified by injured children, their parents, carers, other family members, healthcare and education providers.
Needs identified throughout the rehabilitation process in hospital and community settings.
Papers that addressed the following were excluded:
Needs of injured young adults aged >18 years.
Isolated dental trauma.
Only burn injuries.
Only non-traumatic brain injuries.
Non-accidental injuries, including sexual trauma.
Birth trauma.
Investigation of outcome measures, goal planning and treatment tools, where the focus was on the children’s functional abilities or health status, rather than their needs.
Assessment of needs before the participating children sustained traumatic injuries.
Needs following post-traumatic stress or emotional trauma, rather than physical trauma.
If a paper included a mixed sample of traumatic and non-traumatic and/or non-accidental injuries, the paper would be excluded unless the data for traumatic injuries could be extracted or over 50% of participants had traumatic accidental injuries. We also looked at assessment protocols which may be used to identify needs.
As this was a scoping review to establish the state of the evidence, we did not assess the quality of the papers which met the selection criteria. 13 Two authors (S.J. and S.F.T.) independently extracted and tabulated information relating to the setting, participants, type of needs assessed, and the topics addressed during the data collection. For papers regarding needs assessments, we planned to extract data regarding their psychometric properties and clinical utility.
Thematic content analysis was used to draw out key needs from the identified papers.14,15 The identified papers were read several times independently by two of the authors (S.J. and S.F.T.) to familiarize themselves with the content. They then discussed the data to generate and agree upon the codes for the thematic analysis. The main findings relating to injured children’s and families’ needs were identified and coded. The codes were analysed, grouped and then sub-categorized into types of need. Finally, the findings were iteratively summarized and clustered until consensus was reached.
For papers about assessment of children’s and families’ needs, data about the setting, participants, method, clinical utility of the tools, psychometric properties tested and the results would be extracted using well-established methods.15 –17
Results
The search identified 2401 potentially relevant papers, which reduced to 50 once duplication was removed and titles and abstracts were screened (Figure 1). A total of 12 papers were identified after the full texts were examined. No papers regarding the psychometrics or clinical utility of measurement tools, to assess the needs of children with traumatic injuries and/or their families, were identified. Thus, this part of the review was not taken any further. No papers which included assessment protocols to identify children’s needs were found.
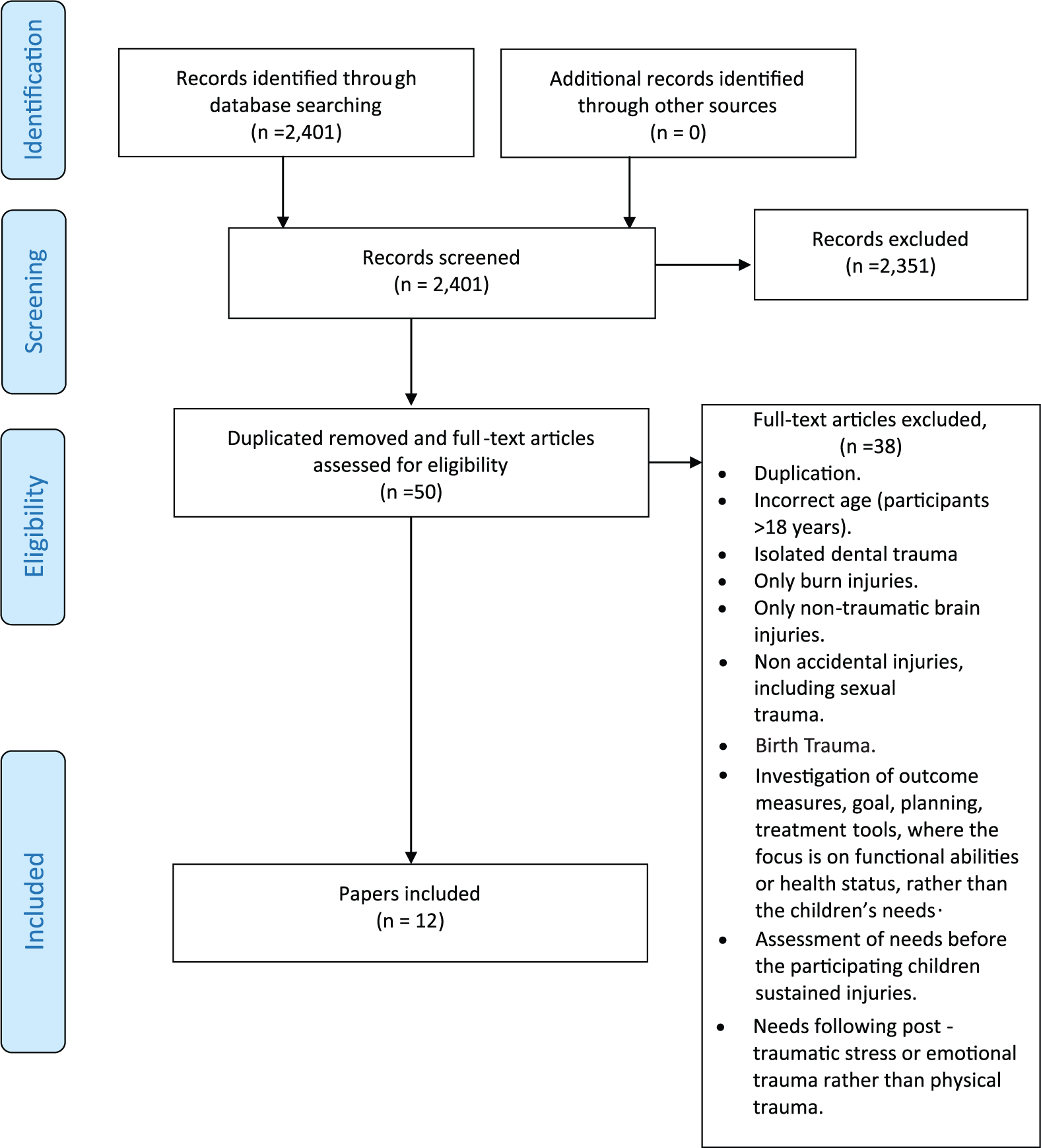
Flowchart of study selection process.
The identified papers included 932 participants,18 –29 including 105 injured adolescents,19,20 418 parents (57 mothers, 25 fathers, 336 unspecified parents),18,19,21 –24,28 302 unspecified primary carers, 25 66 other family members (5 brothers, 2 sisters, 2 grandmothers, 57 unspecified),26,28,29 and 41 healthcare providers (occupational therapists, physiotherapists, psychologists, nurses, social workers, surgeons) 27 and unspecified numbers of teachers, 24 general practitioners, school counsellors and nurses. 20 A summary of the identified papers can be found in Table 1.
Details of the participants, types of need assessed, methods and the main topics explored in the identified studies.
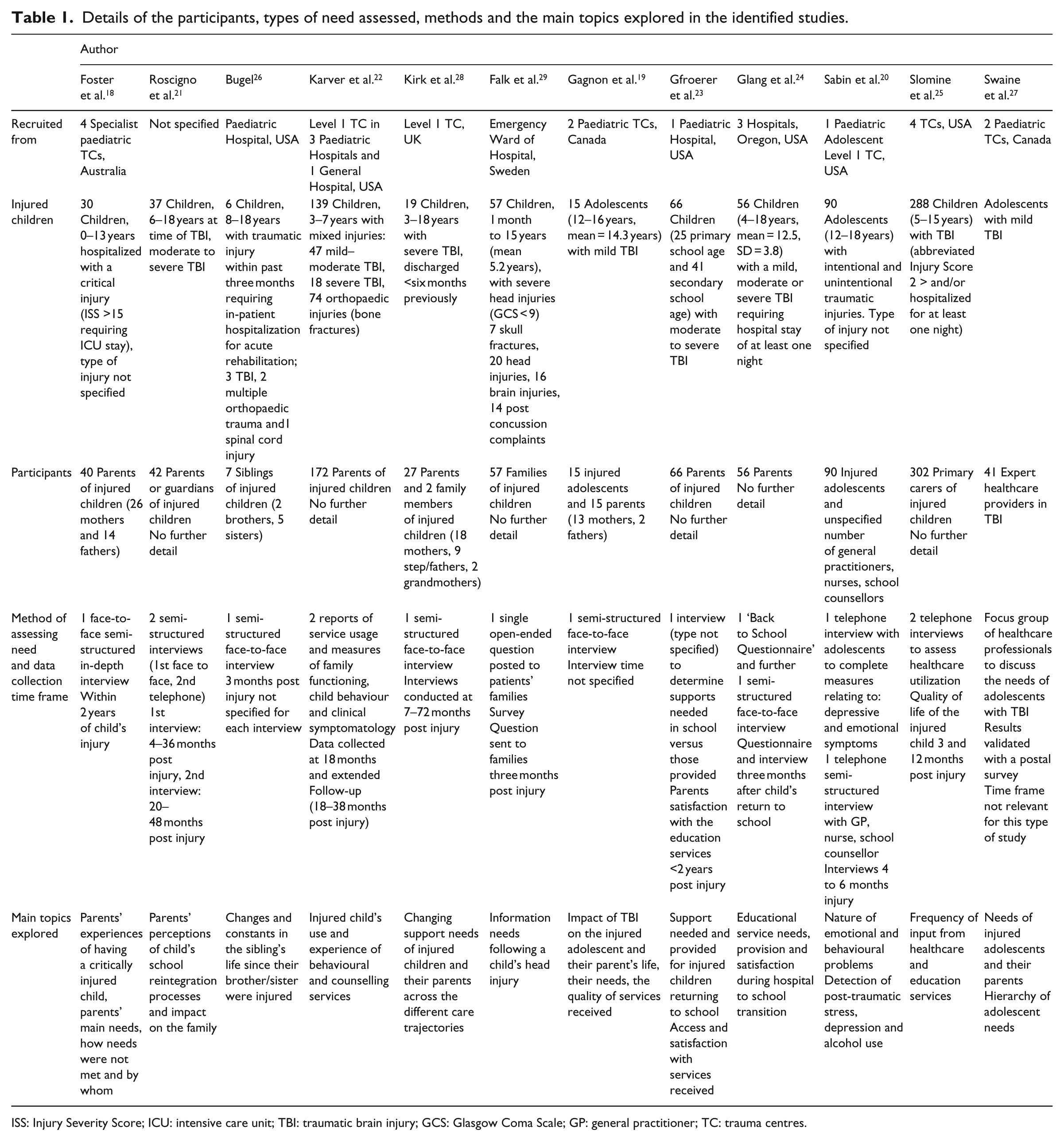
ISS: Injury Severity Score; ICU: intensive care unit; TBI: traumatic brain injury; GCS: Glasgow Coma Scale; GP: general practitioner; TC: trauma centres.
Only five papers specifically focussed on the needs of the injured child,20,22 –25 the others focussed on the families’ needs,18,26,29 or a combination of both.19,21,27,28 Papers directly collecting data from the injured child were limited to adolescents.19,20 The needs of younger children were ascertained indirectly from their family or professionals. Two papers involved health professionals and teaching staff,20,27 in addition to the injured adolescents. 20
Eight papers specifically focussed on children with solely traumatic brain injuries,19,21,23 –25,27 –29 two papers involved children with head, orthopaedic and/or spinal cord injuries,22,26 and two did not specify the type of traumatic injury.18,20 No papers included children with chest or abdominal trauma or orthopaedic injuries in isolation. The age range of the children involved was wide, from pre-school/nursery age to teenagers.18 –29 Most identified papers examined the participants’ long-term problems except Kirk et al., 28 Falk et al. 29 and Foster et al., 18 who focussed on the families’ needs during the acute and sub-acute phases of care.
All the included papers were exploratory and most used a cross-sectional design.18 –20,23,24,26 –29 The most common method of data collection was face-to-face semi-structured interviews18,19,21,24,26,28 (see Table 1 for further details).
Key themes
Two main groups of needs were identified: person-related needs and service-related. Person-related needs were sub-categorized into six types: adolescent-specific needs and needs for support with cognitive, emotional, social, physical problems and practical difficulties (detailed in Supplementary Table 2a). Service-related needs were sub-categorized into needs for information, educational support and support across care transitions (detailed in Supplementary Table 2b). The types of needs are summarized below.
Adolescent-specific needs
Adolescents had some specific needs which related to their age and developing independence. These were to be recognized as an individual, feel in control of their situation, be involved in decision-making and the opportunity to have confidential discussions, not involving their parents.19,27 Adolescents wanted to be cared for with other teenagers and benefit from their peer support.19,20,27 Specialist healthcare providers in traumatic brain injury believed that adolescents who had left home and/or were working would be managed most appropriately by adult services. 27
Need for support with emotional problems, cognitive problems and social problems
The need for support with cognitive, emotional and social problems (including behavioural problems) was frequently highlighted by participants who felt their needs were often unrecognized and unmet.20 –25,28,29 This was the case for children (and their families) with orthopaedic injuries, 22 as well as those with traumatic brain injury.19,21,23 –25,27 –29
Children needed help with feelings of frustration and depression (sometimes including suicidal thoughts21,28) which stemmed from being unable to do what they could prior to their injury, being viewed differently by other children and being bullied (or fear of being bullied).18,21,28 Children wanted to be accepted by their peers and to have their problems recognized and their needs addressed. However, this rarely happened particularly once discharged from hospital and returning to school.21,28
Most parents reported a need for support for themselves as well as their child.18,19,28,29 They often struggled with feelings of guilt surrounding the child’s accident; wondering if they could have stopped it happening or managed the situation differently.18,28,29 Once in hospital, uncertainty regarding the injuries, potential for recovery, fears about changes to their child’s appearance and confronting the fact that their child may never be the same again were of concern.18,19,28,29
Several aspects of hospital-based care were identified which could contribute to meeting these needs. These included the following:
Opportunities to develop trusting relationships with healthcare professionals, other injured children, parents and families, to share their ‘emotional burden’, discuss their feelings and be reassured.18,19,27 –29
After discharge, families reported that they often felt unprepared for the responsibility of caring for their injured child, which they found overwhelming.18,28 They described difficulty obtaining information and accessing help and services (detailed in the relevant sections below). Unsurprisingly, parents often felt abandoned by services18,28 and felt they were forced to act as an advocate for their child.21,28
Need for help with physical problems
As might be expected in research where studies on children with traumatic brain injuries and concerning long-term support predominate, the need for help with physical problems was identified less frequently than those for cognitive, emotional and social problems, and the needs were felt to be recognized and met more often.18 –21,23,25,28
The identified studies consistently recognized that regular post-discharge review appointments were important for ongoing symptom management, health maintenance and to facilitate return to physical and academic activities.19,20,25 Four studies identified the need for rehabilitation including speech therapy, occupational therapy, physiotherapy and audiology to address physical problems.23 –25,28
Need for help with practical difficulties
Parents needed help to balance spending time with, and caring for, their injured child with work and home commitments. This help was often provided by family and friends. 18 They also required help finding affordable accommodation, parking and refreshments plus help to complete insurance and benefit claims from healthcare professionals.18,21
Need for information
In the early stages, parents,18,19,27,29 siblings 26 and injured adolescents 19 needed information about diagnosis and the immediate plan of care, the child’s prognosis for survival and recovery, and updates about any developments.18,19,27,29 Although parents and adolescents wanted information to be readily available, the desired detail varied.19,28,29 Some felt they were given insufficient information.19,28 While others, particularly during acute care, acknowledged that they were unable to absorb much detail and only wanted simple, essential information. 28 Similarly, healthcare providers felt that the provision of information was important, but that too much information during acute care may lead children to focus unduly on their symptoms. 27
In the post-acute stages, injured children and families reported the need for information about what to expect from the recovery process; possible sequelae to the injuries and activity restrictions: what was normal; how to provide everyday care and prevent further injuries; what care/services would be provided after discharge and how to optimize return to activities and school.18 –21,24,27 –29 After discharge, primary care providers, educational and community services were parents’ main source of information. However, this was frequently problematic as relevant referrals were not made and staff often had insufficient knowledge to provide the information needed.18,20,21,23 –25,27,28
Need for support across care transitions
Injured children and their families viewed transitions between care settings, particularly discharge from hospital and return to school as key points when their needs were often unmet.18 –21,23 –25,27,28 Information about community and educational services was considered particularly poor,18 –21,23 –25,27,28 which was compounded by lack of communication between the families, healthcare professionals and educational services.18 –21,24,25,27,28 This meant that referrals from specialist trauma centres to primary care, community, social and education services were often not made.20,21,25,28 Consequently, injured children and their family had great difficulty accessing the support and services they needed.20,21,25,28
Furthermore, staff from community, primary care and education services often had insufficient understanding of the child’s injuries and their impact, to support return to everyday activities and education.19 –21,24,25,27,28 For example, symptoms such as difficulty concentrating, poor memory or fatigue were often misinterpreted as bad behaviour or laziness.19,21,28 This was most keenly felt when the child had no physical signs of an injury.21,28
Families identified the following as ways to improve transitions between care settings:18 –21,24,25,27,28
Specialized services with knowledgeable, expert staff providing long-term support including regular reviews and ongoing telephone support to facilitate return to physical and academic activities.19,21,25,27,28
Provision of a key worker to negotiate links between hospital, community and education services.19,27,28
A collaborative environment with co-ordinated systems and clear leadership.18,21,27,28
Home visits, multidisciplinary meetings and information exchange (including written information about the injury) between the family and all relevant services to ensure an effective handover.18,20,21,28
Need for educational support
Return to education was considered an important transition, and the extent to which needs were met was mixed.19,21,23,24,27,28 As noted above, parents felt their child’s need for educational support was difficult to access and they often had to advocate for their child themselves.21,24,28 This frequently involved the need to:
Educate teachers about their child’s injuries and the impact on academic performance, behaviour, activity (particularly sports) and the adjustments needed.19,21,24,27,28
Monitor the school environment to ensure adaptations, accommodations, specialist services and individualized educational plans (such as a personal assistant, special needs classes, home-school programmes) were in place and adhered to.21,23,24,28
(In some cases) move schools, hire tutors and set their own curriculum, often involving support groups or educational psychologists.21,28
Discussion
The results of this review indicate that the needs of children with traumatic injuries and/or their families are often unmet, particularly the need for information, emotional support, and support during care transitions. Healthcare and educational professionals often showed limited awareness and understanding of the nature of the children’s injuries and the resultant challenges they caused. In turn, this hindered referrals to appropriate services and meant that symptoms were often misinterpreted, particularly those which were not physically obvious, such as fatigue, cognitive problems or pain. Clearly further work is needed to develop interventions, resources and/or staff development opportunities to address these shortcomings. The need to increase awareness and understanding of the difficulties injured children face and to develop effective pathways to ensure comprehensive and timely access to services have been clearly identified. If successful, such interventions and service developments should improve equity of access, quality of services and outcomes. Currently, there is negligible evidence about how to achieve this, but there is a body of knowledge from other sudden-onset disabling conditions with an uncertain trajectory for recovery, such as adult neurological rehabilitation, with important principles that may be suitable for adaption to childhood trauma.30 –33
The identified papers focussed primarily on the long-term needs of children with traumatic brain injuries. Further work is needed to establish the needs of children with other types of injuries, such as orthopaedic, chest or abdominal injuries in whom physical problems may predominate, and to more thoroughly understand children’s and their families’ needs in the (sub)acute stages of rehabilitation and how needs change over time.
Most of the identified papers asked the injured child’s family (primarily parents) about their child’s and/or family’s needs rather than directly involving the injured child. The only injured children who participated themselves were adolescents.19,20 Although in the clinical setting, the injured child and their family are generally considered a single unit, it cannot be assumed that families accurately present the injured child’s views.34,35 Further work to directly report injured children’s views is warranted, despite the methodological and ethical challenges involved.
In addition to reviewing children’s and families’ needs, we aimed to review ways to measure their needs. This proved impossible as no standardized measurement tools were identified from the searches. Comprehensive, psychometrically robust, user-friendly measurement tools are needed to accurately identify and understand the scale and nature of children’s and families’ problems and to identify what is needed to address these problems. Work to develop such a tool is underway.
This study has several limitations. The searches were restricted from 2005 to September 2017, as we wanted to ensure our findings reflected reasonably current practice. However, relevant papers published before this period may have been missed. Additionally, ‘need’ is difficult to define and may be expressed using a variety of terms, so it is possible that using the key search term ‘need’ did not identify all relevant papers. As this review aimed to explore the scope of evidence regarding injured children’s needs, we did not evaluate the quality of identified papers nor exclude those of poor quality, so the strength of this evidence needs to be treated with some caution. Furthermore, the predominance of participants with traumatic head injuries and a focus on long-term support means that generalizability should be viewed cautiously and not extrapolated to all types of injury and all stages of rehabilitation. Nevertheless, the consistency of the main needs, and the similarities with other research on patients’ and families’ needs in adults with severe trauma and other sudden on-set disabling conditions suggests convergence.30 –33,36 –38
Clinical Messages
Injured children and their families need information and support for cognitive, emotional, social and physical problems, help with practical difficulties, and during education and care transitions.
Adolescents have specific needs.
These needs are often unmet.
Development of suitable tools to measure injured children’s and families’ problems and needs is warranted.
Footnotes
Acknowledgements
The authors thank Jo Whitcome and Elham Aalai (Clinical Librarians) for their advice on the search strategy. They also thank Helen Blakesley (Major Trauma Rehabilitation Co-ordinator at Royal Manchester Children’s Hospital) for her insights into the met and unmet needs of children with traumatic injuries and Deborah Aitken for her overall support. S.J. and S.F.T. were responsible for the organization and execution of the research project; conceptualization of the idea, the design, analysis and writing of the manuscript. S.J. additionally conducted the systematic search of the databases. N.D. reviewed, improved and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: S.J.’s work on this project was partially supported by a part-time Trauma and Orthopaedic Research Secondment, funded by the Royal Manchester Children’s Hospital Charities. This manuscript is independent research supported by the National Institute for Health Research (HEE/ NIHR ICA Programme Clinical Doctoral Research Fellowship, Miss Samantha Jones, ICA-CDRF-2016-02-021). The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.