
Abstract
Objective:
To systematically assess the effectiveness of core-based exercise for correcting a spinal deformity and improving quality of life in people with scoliosis.
Data sources:
The PubMed, Embase, Cochrane Library, Cumulative Index of Nursing and Allied Health Literature (CINAHL), and Web of Science databases were searched from inception up to September 30, 2020.
Methods:
Clinical controlled trials were eligible if they compared the effectiveness of core-based exercise to other nonsurgical interventions in people with scoliosis. The revised Cochrane risk of bias assessment tool for randomized trials and the methodological index for non-randomized studies scale were used to assess the risk of bias. The outcomes included the Cobb angle, the angle of trunk rotation and quality of life. RevMan 5.3 was used, and intergroup differences were determined by calculating mean differences (MD) and 95% confidence intervals (CIs).
Results:
After screening 1348 studies, nine studies with 325 participants met the inclusion criteria. The exercise group had significantly lower Cobb angles (MD = −2.08, 95% CI: −3.89 to −0.28, P = 0.02) and significantly better quality of life as measured by the Scoliosis Research Society-22 questionnaire (MD = 0.25, 95% CI: 0.02 to 0.49, P = 0.03) than the control groups. However, no significant difference was observed regarding the angle of trunk rotation between groups (MD = −0.69, 95% CI: −2.61 to 1.22, P = 0.48). Furthermore, no serious adverse events were reported. The overall quality of evidence ranged from low to very low.
Conclusion:
Core-based exercise may have a beneficial role in reducing the Cobb angle and improving quality of life in people with scoliosis in the short term.
PROSPERO registration number:
CRD42020160509 (Available at http://www.crd.york.ac.uk/prospero/)
Introduction
Scoliosis is a musculoskeletal disorder that manifests as a sideways curvature of the spine (measured by the Cobb angle) and occurs in both adolescents and adults with a female-male distribution ratio >8:1 among individuals above the age of 10 years old.1,2 The prevalence of scoliosis in school children under the age of 16 years old varies from 3% to 5%, and that in adults ranges from 1.4% to 20%.3,4 Generally, scoliosis is classified as functional and structural based upon whether the curve with bending is fixed. Functional scoliosis refers to a type of scoliosis characterized by a temporary curvature in the spine without rotation of the vertebrae, while structural scoliosis is a multifactorial disorder that is associated with a loss of flexibility in one or more segments of the curved spinal column. 5 Ten to fifteen percent of adolescents with mild idiopathic scoliosis have a risk of the curve worsening, which is considered to be linked to underlying biomechanical and morphologic alterations along the trunk segment with actions of improper mechanical forces,6–8 and may sometimes cause complications, including cosmetic deformity, physical function decline and poor health-related quality of life.9,10
Exercise programs aiming to relieve clinical symptoms and prevent curve progression have been implemented widely in recent years. It appears that core-based exercise is one of the most promising physiotherapeutic approaches to contract muscles for the best realignment of the spine and spinal stability that counteract curve progression.11–13 In addition, it was recommended by the 2016 International Society on Scoliosis Orthopaedic and Rehabilitation (SOSORT) guidelines.11,14 However, only one systematic review explained the effect of stabilization exercise on back pain in adult idiopathic scoliosis with limited evidence, 15 and no quantitative meta-analysis has been performed. The present systematic review and meta-analysis aimed to investigate the evidence for the effectiveness of core-based exercise programs on curve magnitude and other health-related parameters among people with scoliosis.
Methods
We performed this systematic review and meta-analysis in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 16 and it was registered in the PROSPERO database (NO. CRD42020160509). Key terms including “scoliosis,” “core exercise*,” “core stabilization,” and “core strengthening” were used to search the PubMed, Embase, Cochrane Library, Cumulative Index of Nursing and Allied Health Literature (CINAHL), and Web of Science databases for studies reporting the effectiveness of core-based exercise in scoliosis before September 30, 2020. Studies were excluded if they were published in languages other than English. Additional studies were acquired from manually searching relevant systematic reviews. The reference lists of identified studies were also reviewed to identify other potentially relevant studies.
Two reviewers (Juping Liang and Xuan Zhou) independently screened the titles and abstracts of the eligible studies. Studies were included if they met the following criteria: (1) population: scoliosis without surgery, irrespective of sex, age, race or ethnicity; (2) intervention: core-based exercise including all kinds of exercise related to the core muscles, such as core stability exercise and core strength exercise; (3) control: observation or general treatment without core muscle exercises; (4) outcomes: primary outcomes were curve magnitude (by measuring the Cobb angle) and clinical deformity measured by the angle of trunk rotation with a scoliometer in Adam’s test, as well as adverse events, which were reported as the number of participants who withdrew or experiencing any serious adverse events; the secondary outcome was the quality of life (assessed by the Scoliosis Research Society-22 questionnaire); and (5) study design: clinical controlled trial. Discrepancies were resolved by a third reviewer (Yuqi Yang).
Data were extracted by Shanshan Wang and independently confirmed by another reviewer (Lixia Wang). Information relating to studies and participant characteristics was extracted, including first author, year of publication, study design, number of participants enrolled (% female), characteristics, type of scoliosis, main curve, Risser grade, outcome measures and adverse events. Core-based exercise and control group interventions in parallel group trials were also collected. The schedule of the core-based exercise was defined by volume (number of sets and repetitions), frequency (number of training sessions per week), and duration (in weeks). When the same participants were reported in several publications, we retained only the one with the largest sample size to avoid duplication of information.
Two reviewers (Juping Liang and Dexuan Wang) independently assessed the risk of bias using the revised Cochrane risk of bias assessment tool (RoB 2.0) for randomized controlled trial studies (RCTs). 17 The methodological index for non-randomized studies (MINORS) scale was used to assess non-RCTs on a scale ranging from 0 to 24.18,19 Disagreements were resolved through consensus.
Statistical analysis was performed using Review Manager (RevMan 5.3). If two or more control groups performed various treatments in one trial, we combined the data from the control groups using the formula recommended by the Cochrane Handbook.17,20 A random-effects model was used with treatment effects reported as the mean differences (MD) and 95% confidence intervals (CIs), 17 with significant differences set at P < 0.05. The subgroup analysis was undertaken only for the primary outcome (Cobb angle) based on the core exercise only and the comprehensive exercise (including core muscle exercise) of the pooled studies. Heterogeneity across studies was tested with the I2 statistic. 21 Heterogeneity across studies was tested with the I2 statistic with values of 25%, 25% to 50%, 50% to 75%, >75% indicating no heterogeneity, low heterogeneity, moderate heterogeneity and high heterogeneity, respectively. Publication bias was estimated by a funnel plot. The Grading of Recommendations, Assessment, Development and Evaluations (GRADE) criteria were used to rate the overall strength of the evidence. 22 In these criteria, five main factors (risk of bias, imprecision, inconsistency, indirectness, and publication bias) were used to categorize evidence quality. The quality of the evidence was assessed based on the following criteria: high quality indicated that further research is very unlikely to change our confidence in the estimate of effects; moderate quality indicated that further research is likely to have an important impact on our confidence in the estimate of effects and may change the estimate; low quality indicated that further research is very likely to have an important impact on our confidence in the estimate of effects and is likely to change the estimate; and very low quality indicated that any estimate of effects is very uncertain.
Results
A total of 1348 records were identified from the initial database search. After excluding duplicates using EndNote X9, we found 1058 potentially relevant references; 919 articles were excluded after screening the titles and abstracts. Finally, we identified 139 studies that were subjected to full-text review. The results of two RCTs conducted by Schreiber et al. were analyzed and referenced as one due to having the same population and the same trial registration numbers.23,24 Finally, a total of nine articles including 325 participants with valid outcome data met the inclusion criteria. Figure 1 shows the PRISMA flow diagram of the studies included in this review.
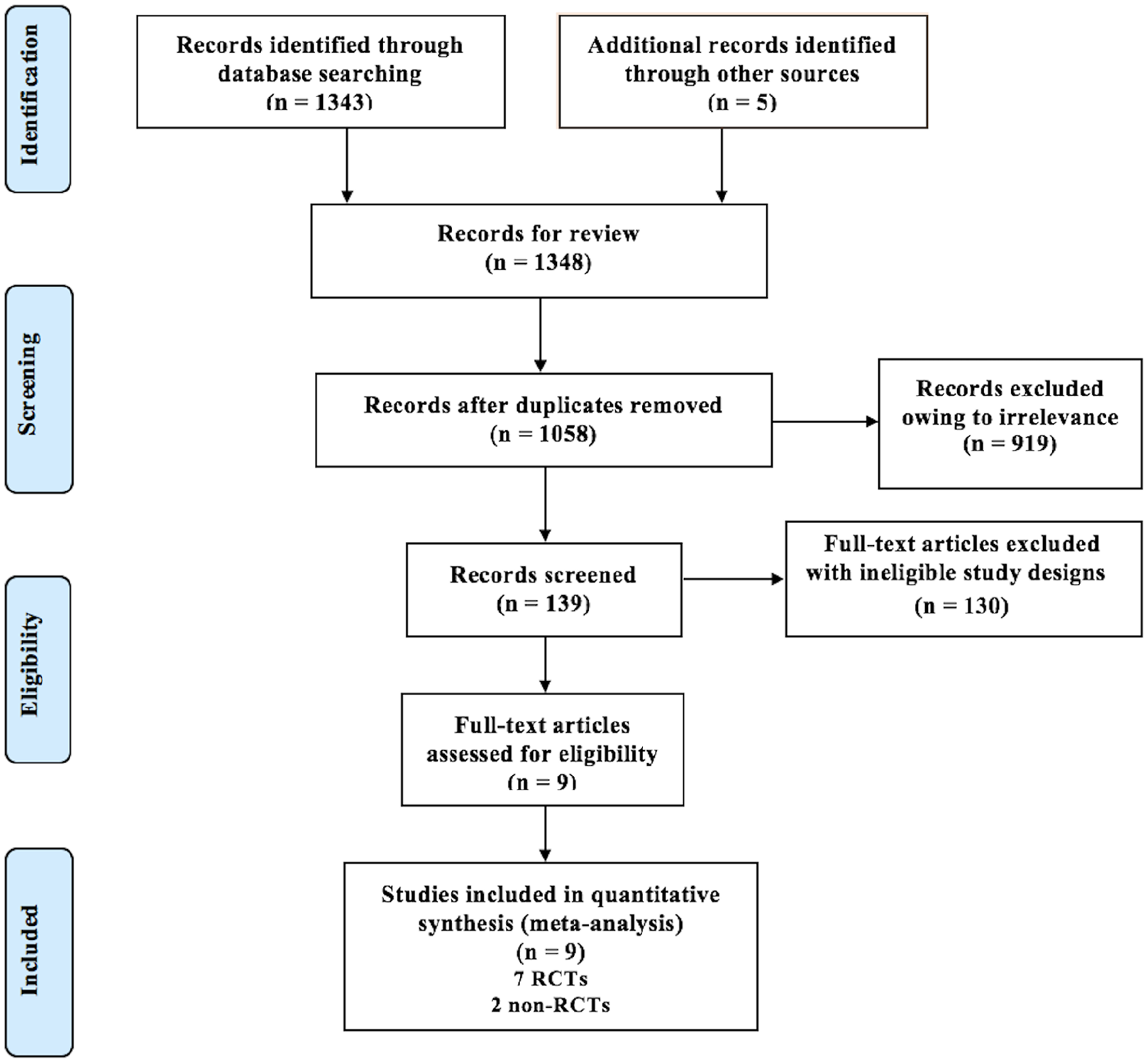
PRISMA flow diagram of included published studies.
Table 1 summarizes the study design, sample descriptions and outcomes in parallel group trials. Seven RCTs with 280 participants (158 in intervention groups and 122 in control groups) included 249 idiopathic scoliosis and 31 non-structural dorsolumbar scoliosis. Two non-RCTs had 45 adolescent idiopathic scoliosis. The main reason for noncompliance and dropout was time constraints in 11 participants.23–25 The mean age of the participants ranged from 12.1 to 23.6 years. The mean Cobb angle among patients with idiopathic scoliosis ranged from 11.7° to 35.0°, and it ranged from 7.1° to 7.6° among patients with functional scoliosis. The concept of core-based exercise underpinned the approaches used in four studies;26–29 the Schroth exercises (with the corrective movements) with core strengthening techniques were performed in two studies;23,24,30 two studies involved the Scientific Exercises Approach to Scoliosis with respect to spinal stabilization and strengthening of tonic antigravity muscle training;25,31 and one study involved Pilates methods, consisting of exercise on swiss balls aimed at improving trunk posture. 32 The frequency of exercise varied from daily to every other day,23–25,31 and the duration ranged from 6 weeks 30 to 48 weeks. 31 Supplemental Table S1 summarizes core-based exercise training and control group interventions in the parallel group trial.
Baseline demographic and clinical characteristic of included studies.
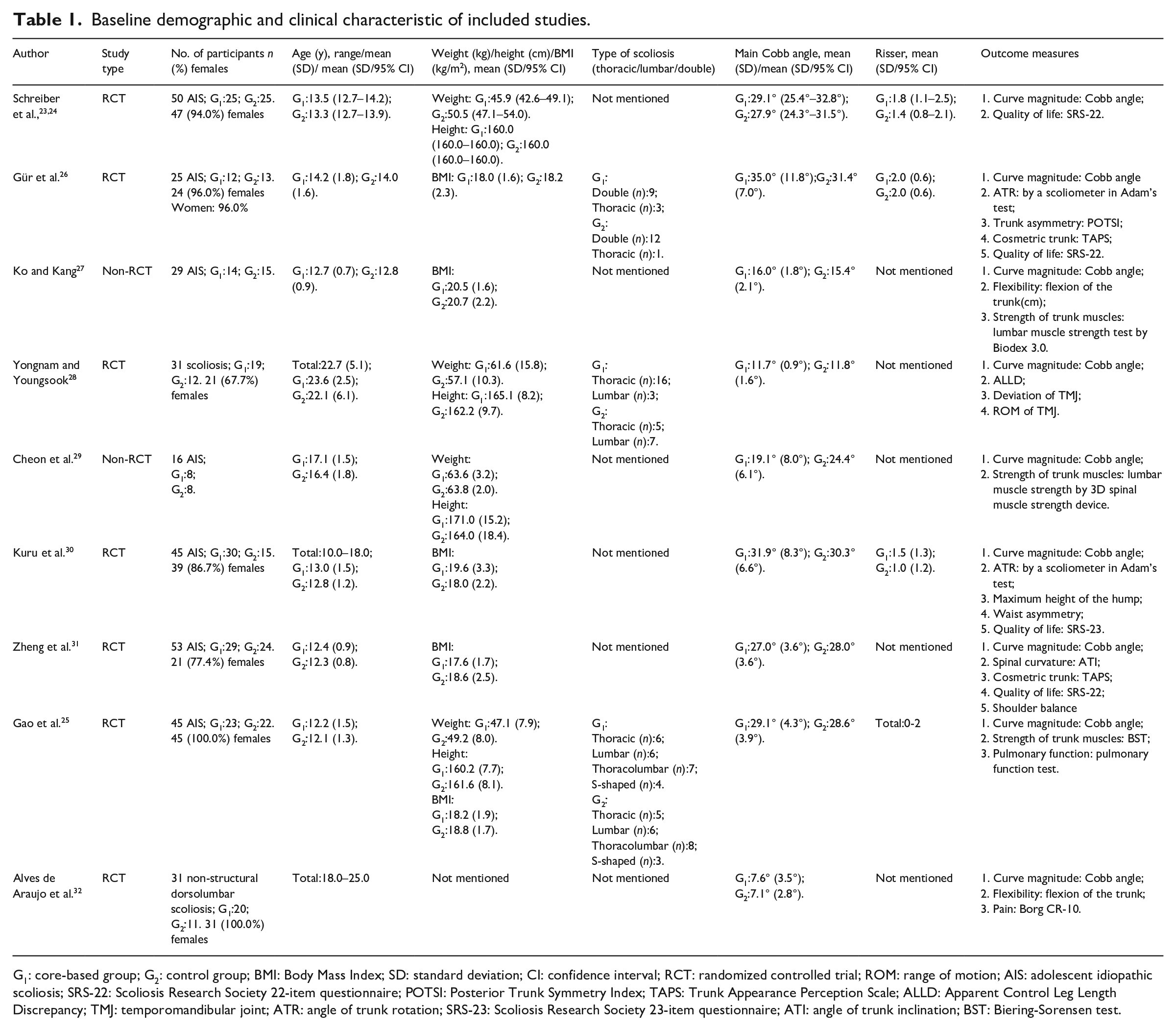
G1: core-based group; G2: control group; BMI: Body Mass Index; SD: standard deviation; CI: confidence interval; RCT: randomized controlled trial; ROM: range of motion; AIS: adolescent idiopathic scoliosis; SRS-22: Scoliosis Research Society 22-item questionnaire; POTSI: Posterior Trunk Symmetry Index; TAPS: Trunk Appearance Perception Scale; ALLD: Apparent Control Leg Length Discrepancy; TMJ: temporomandibular joint; ATR: angle of trunk rotation; SRS-23: Scoliosis Research Society 23-item questionnaire; ATI: angle of trunk inclination; BST: Biering-Sorensen test.
The RoB 2.0 tool assessment of the included RCT group studies is presented in Supplemental Table S2. Seven RCTs generated an adequately randomized sequence,23–26,28,30,32 but only two of them were conducted in a blinded fashion for the outcome assessment.23–25 The MINORS index was applied to 2 non-RCTs with 16 scores and 15 scores with moderate quality of evidence, as shown in Supplemental Table S3.27,29 The GRADE for all outcome measurements was inconsistent and ranged from low to very low quality (Supplemental Table S4), which means that, in the future, data that are robust and have a low risk of bias may overturn some of the results of the interventions assessed in this meta-analysis.
The Cobb angle (in degrees) is the gold standard for assessing the severity of scoliosis. When data collected from all included studies were pooled, we found a statistically significant decrease in the Cobb angle among patients who used core-based exercise (MD = −2.08, 95% CI (−3.89, −0.28), P = 0.02), but the heterogeneity was high (I2 = 82%) (Figure 2).
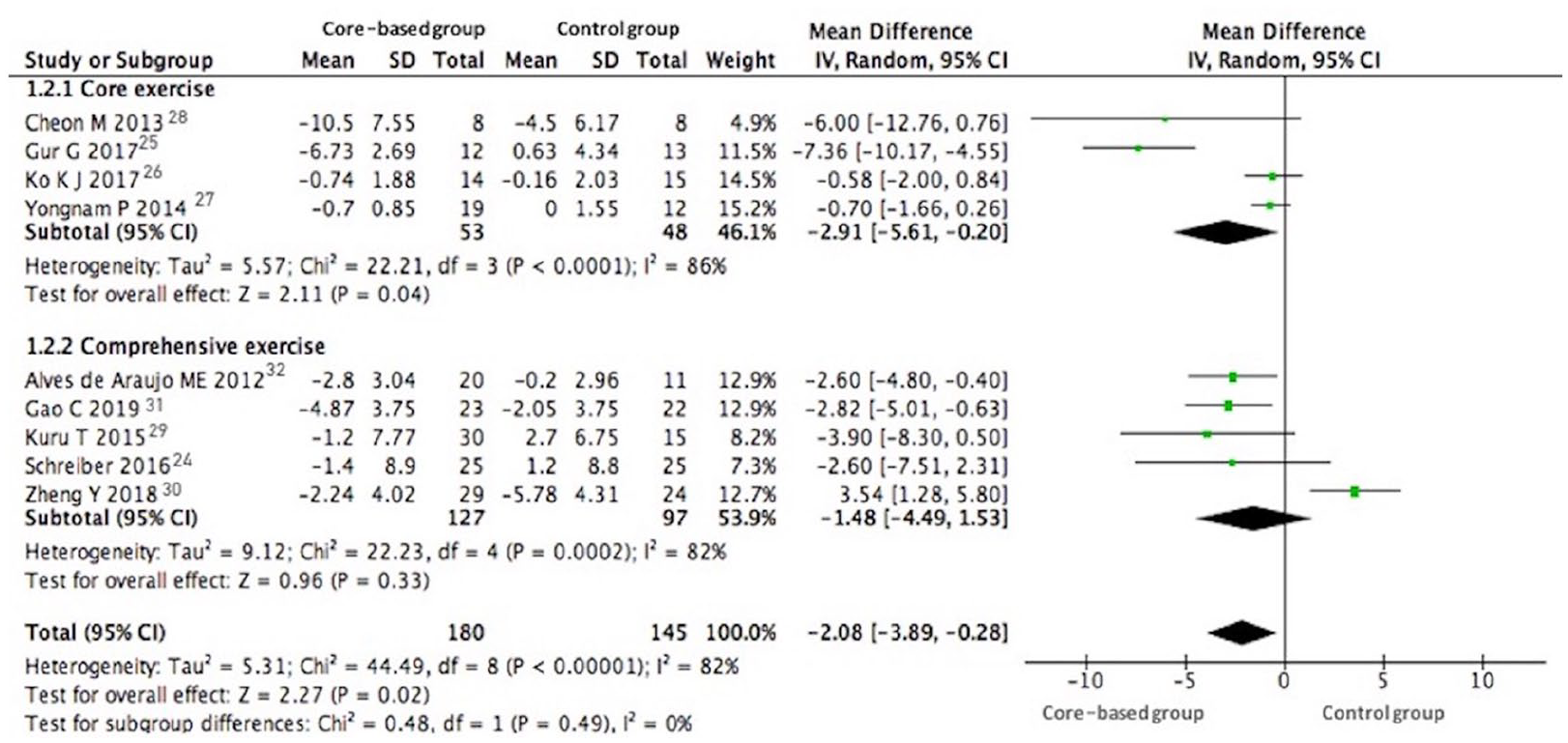
Cobb angle for core-based exercise compared with other forms of treatment. 1.2.1, core exercise only; 1.2.2, both core exercise and comprehensive exercise studies.
When data collected from four controlled studies with only core exercise were pooled, a statistically significant decrease in the Cobb angle was identified among patients with scoliosis (MD = −2.91, 95% CI (−5.61, −0.20), P = 0.04, I2 = 86%) (Figure 2, 1.2.1). A subgroup analysis of comprehensive exercise studies showed no difference in the Cobb angle (MD = −1.48, 95% CI (−4.49, 1.53), P = 0.33, I2 = 82%) (Figure 2, 1.2.2). In addition, the funnel plot had an asymmetrical distribution regarding the Cobb angle, which suggested that there was a high risk of publication bias (Supplemental Figure S1).
Three of the included trials reported the angle of trunk rotation (in degrees) measured with a scoliometer™ in the standing forward bending position (the maximum angle of trunk rotation was recorded), 33 but we failed to find a significant difference between groups in the pooled analysis of these four studies (MD = −0.69, 95% CI (−2.61, 1.22), P = 0.48, I2 = 74%) (Figure 3).

ATR for core-based exercise compared with other forms of treatment.
Core-based training was well tolerated among scoliosis in most included studies. In the pooled analysis, the overall dropout rate was 3.33% (6/180) in the core-based group and 3.45% (5/145) in the control group. Nevertheless, no adverse events, such as progression of symptoms or death, were reported among the participants during the training period.
Quality of life was evaluated by the Scoliosis Research Society-22 questionnaire. It is made up of 22 questions covering five domains: pain, self-image, function/activity, mental health, and management satisfaction. 34 Only one study reported the score of the management satisfaction domain. The total score of the Scoliosis Research Society-22 questionnaire was used by two studies to provide self-reported data on quality of life outcomes. We found significant improvements in total score of quality of life [score: 1 (worst) to 5 (best)] in the core-based exercise group (MD = 0.25, 95% CI (0.02, 0.49), P = 0.03, I2 = 52%) (Figure 4(a)). Data from three studies using the self-image subscale [score: 1 (worst) to 5 (best)] were combined. The results showed significant between-group differences in follow-up scores (MD = 0.08, 95% CI (0.01, 0.14), P = 0.02, I2 = 0%) in three controlled studies (Figure 4(b)). Two studies presented data using the self-reported pain relief subscale [score: 1 (worst) to 5 (best)] at baseline and after core exercise. No difference in pain scores was observed for self-report data on pain relief between baseline and postexercise (MD = 0.11, 95% CI (−0.11, 0.34), P = 0.32, I2 = 43%) (Figure 4(c)). The function subscale [score: 1 (worst) to 5 (best)] was used by two studies to provide functional outcomes. Participants who underwent core-based exercise reported better functioning after training than participants who received the traditional intervention and bracing (MD = 0.12, 95% CI (0.03, 0.20), P < 0.05, I2 = 0%) (Figure 4(d)). Data from two studies that used the mental health subscale function subscale [score: 1 (worst) to 5 (best)] were combined. A statistically significant between-group difference in mental health was found (MD = 0.30, 95% CI (0.14, 0.46), P < 0.05, I2 = 21%) (Figure 4(e)).
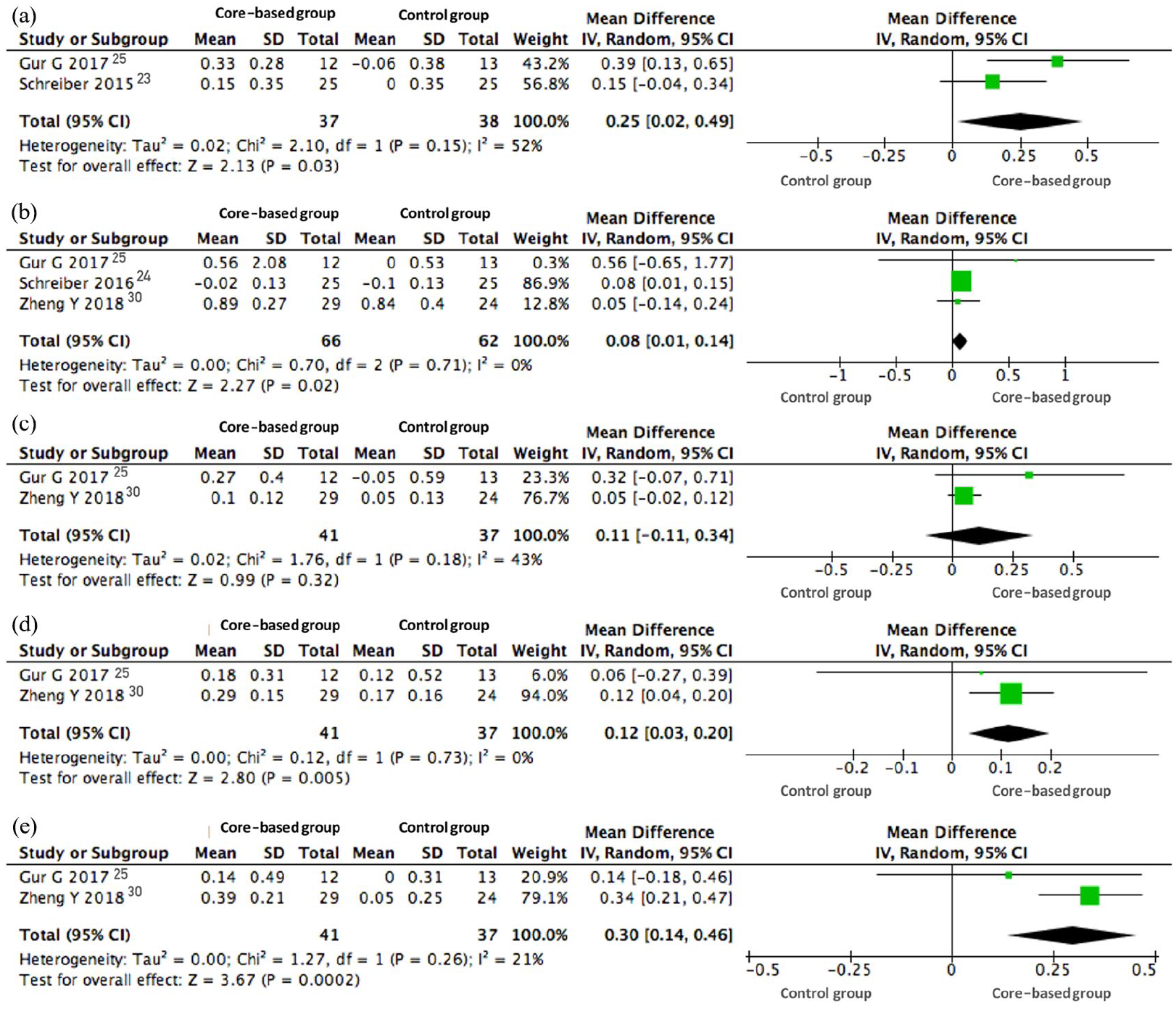
Quality of Life (evaluated by SRS-22) for core-based exercise compared with other forms of treatment: (a) total score, (b) self-image, (c) self-reported pain relief, (d) function, and (e) mental health.
Discussion
The principal finding of this systematic review and meta-analysis of scoliosis is that core-based exercise might be beneficial for reducing the Cobb angle and improving health-related life status, and this type of exercise was well-tolerated among these patients. Pathological muscle alterations in both the lumbar multifidus and deep paraspinal muscles may alter the motor control of the trunk segment, which leads to asymmetric loading of the spine, imbalanced growth of the vertebral body, and the progression of scoliosis with pelvic tilt. 35 Some forms of exercise were recommended to prevent curve progression in scoliosis from including studies.36,37 In addition, core-based exercise, which focused on trunk control and coordination, was proven to be beneficial for enhancing the strength and endurance of trunk stabilizer muscles measured by Lovett’s manual muscular strength test and lumbar muscle strength test by Biodex 3.0, improving intersegmental trunk coordination, and maintaining a neutral spine in participants with low back pain, athletes, and healthy people.38–40 Negrini et al. reported that the average Cobb angle was reduced by 3° in the Scientific Exercises Approach to Scoliosis group (including spinal stabilization, strengthening, muscular retraction and motor coordination), whereas it stayed unchanged in the traditional physiotherapy group.41,42 Similarly, previous studies found that core exercise was associated with a reduced Cobb angle 32 and reported a greater correction of the Cobb angle among patients with scoliosis who used the core muscle release technique based on core stability exercises and manipulation than among patients who used flexion and extension exercises and electrotherapy with an interferential current therapy machine. 43 It was likely that the differences in control programs, including the intensity (30 minutes to 90 minutes) and frequency of core training (one time to three times every week), increased the heterogeneity in the analysis of the Cobb angle.
Furthermore, core-based exercise was considered a method to help individuals increase concentration, reduce emotional disturbance, and improve their self-efficacy.44,45 Scoliosis significantly affects the quality of life of patients, and there is a negative correlation between the severity of scoliosis (measured by the Cobb angle) and quality of life. 46 Some authors suggested that the improvements in functional capacity and quality of life observed after therapeutic exercise, including core exercises in patients with adolescent idiopathic scoliosis, might be attributed to a reduction in symptoms that, together with better postural parameters, could influence self-confidence and personal satisfaction, 47 which was consistent with our findings.
Although a review has reported the effectiveness of core exercise in reducing pain in a heterogeneous group of patients with low back pain, 48 pain did not reveal statistical significance in people with scoliosis. Notably, some researchers found that there was a trend toward reduction of pain with an average of 0.2 points evaluated by pain-factor structure in the Scoliosis Research Society-22 questionnaire, which was reported as the minimal clinically important difference. 49 Although adolescent idiopathic scoliosis can be responsible for low back pain in major cases, a linear relationship between back pain and the magnitude of the deformity still cannot be expected for any individual patient. 50 In addition, no exercise-associated angle of trunk rotation improvement was reported, which might be explained by the relatively short duration of therapeutic exercise since a previous meta-analysis reported that continuous exercise lasting at least six months could obtain positive changes. 51
There are several limitations to this study. First, there are only a limited number of clinical trials with small samples that have assessed the effectiveness of core-based training among scoliosis. Second, two of the nine parallel group trials included in the pooled analysis were non-RCTs, which highlights the heterogeneities of the pooled analysis that was conducted in this study. Finally, most of the included studies were single center-based and had a relatively short follow-up period. Future multicenter, well-designed randomized controlled trials with a longer follow-up duration are needed.
Core-based exercise is relatively safe and a key element for significantly improving the Cobb angle and quality of life among people with scoliosis. However, this analysis showed no other difference between the experimental group and the control group for angle of trunk rotation and self-reported pain relief in the Scoliosis Research Society-22 questionnaire. Nevertheless, the interpretation and application of these results require caution to consider the methodological shortcomings and poor data quality of the included trials. Consequently, future high-quality studies with longer duration of follow-up and standardized exercise prescription should consider determining the best core exercise protocol to use to improve long-term clinical endpoints among people with scoliosis.
Clinical messages
Core-based exercise, a safe conservative treatment, could effectively decrease the Cobb angle and improve quality of life in people with scoliosis without adverse events.
The quality of the evidence is low, reducing the strength of the findings.
Supplemental Material
sj-pdf-1-cre-10.1177_0269215520975105 – Supplemental material for Effect of core-based exercise in people with scoliosis: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-cre-10.1177_0269215520975105 for Effect of core-based exercise in people with scoliosis: A systematic review and meta-analysis by Xin Li, Jie Shen, Juping Liang, Xuan Zhou, Yuqi Yang, Dexuan Wang, Shanshan Wang, Lixia Wang, Hong Wang and Qing Du in Clinical Rehabilitation
Supplemental Material
sj-pdf-2-cre-10.1177_0269215520975105 – Supplemental material for Effect of core-based exercise in people with scoliosis: A systematic review and meta-analysis
Supplemental material, sj-pdf-2-cre-10.1177_0269215520975105 for Effect of core-based exercise in people with scoliosis: A systematic review and meta-analysis by Xin Li, Jie Shen, Juping Liang, Xuan Zhou, Yuqi Yang, Dexuan Wang, Shanshan Wang, Lixia Wang, Hong Wang and Qing Du in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors would like to thank Xiaoqing Zhu for methodological assistance during the protocol.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the General Program of National Natural Science Foundation of China (81972030), Advanced and Appropriate Technology Promotion Projects of Shanghai Municipal Health Commission (2019SY021), and Chongming District Medical Key Specialty Project.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.