
Abstract
Objective:
To compare the functional outcomes and length of hospital stay for patients treated with conventional physiotherapy compared to a new ankle trainer device after Weber B ankle fractures.
Design:
The patients were randomized, and then followed up at 3, 6, 12 and 52 weeks by a blinded physiotherapist.
Setting:
This study was done at a level 1 trauma centre.
Subjects:
One hundred and forty consecutive patients with Weber B ankle fractures that were operated on were screened for eligibility, of whom 113 were included in the study.
Interventions:
Conventional physiotherapy with stretching exercises, using a non-elastic band or using new ankle trainer.
Main measures:
Outcomes were evaluated with Olerud–Molander ankle score, Visual analogue scale for pain and ankle dorsiflexion at 3, 6, 12 and 52 weeks follow-up. Time of hospitalization and complications were registered.
Results:
Superior Olerud–Molander ankle scores were observed at three weeks follow-up in the ankle trainer group 40.9 (10.8), compared to the conventional group 35.3 (14.2) (P = 0.021). At one-year follow-up, there was no difference between the groups (P = 0.386). The ankle trainer group had a shorter hospital stay with a mean 2.6 days (0.98) compared to 3.2 days (1.47) in the conventional group (P = 0.026).
Conclusion:
The patients who were treated with the new ankle trainer device recovered more rapidly, evaluated by the Olerud–Molander ankle score and had a shorter stay in hospital compared to the conventional physiotherapy group. No between group differences could be observed at long-term follow-up.
Introduction
Most patients with ankle fractures, either operated or treated non-operatively, tend to complain of stiffness, oedema and pain. 1 This has also been referred to as ‘fracture disease’. It is thought to be caused by pain and the lack of physiological load to the joints, leading to stiffness of the joints.1,2 It has been reported that up to 77% of patients experience joint stiffness after cast removal in ankle fractures. 3 The majority of these changes occur within the first two weeks of immobilization.1,4,5 Although the evidence is conflicting, most studies tend to report that early rehabilitation after ankle fractures could avoid these side effects in the short term. 6 Long-term follow-ups have not demonstrated functional differences between early mobilization and immobilization after ankle fractures. 2 However, most studies that report early active rehabilitation to be superior compare the outcomes from patients who were treated with a cast postoperatively compared to patients who were allowed early range of motion. There is a lack of knowledge on the effect of different standardized rehabilitation protocols.
We have developed a novel spring-loaded device to facilitate early ankle motion where the patients perform active plantar flexion and the device facilitates passive dorsiflexion of the ankle. Our hypotheses were that the use of the ankle trainer would lead to improved functional outcome at short term follow-up and shorter hospital stay compared to conventional physiotherapy.
Materials and methods
The Regional Committee for Health Research Ethics (REK Reference No. 2014/1504) approved the study, and a written informed consent was obtained from all study participants. The study is registered in Clinicaltrials.gov (NCT04168307). The study was conducted between 28 November 2014 and 1 December 2017. The study was funded by Oslo University Hospital, which was also responsible for the study.
This was a prospective randomized controlled study, where the investigator was blinded for group affiliation. The study was conducted at a single level 1 trauma centre. Inclusion criteria were patients between 18 and 65 years with dislocated or unstable closed Weber B ankle fractures, who were operated according to our hospital’s guidelines. 7 The guidelines correspond to the Arbeitsgemeinschaft fur osteosynthesefragen (AO) recommendations, intending an exercise stable osteosynthesis. Only patients who were considered to have good compliance and could follow the rehabilitation protocol were included. Exclusion criteria were previous trauma to the tibia or fibula, previous ankle or foot surgery, symptomatic arthritis or arthrosis in the foot or ankle, generalized joint disease, multitrauma and other diseases that impaired walking or pathological fractures.
Patients were informed about the study the first day after surgery by a physiotherapist. If the patient accepted inclusion and fulfilled the criteria, they were randomized to intervention group by a web-based randomizer delivered by the Norwegian University of Science and Technology in Trondheim. Block randomization with blocks of 10 was used. Randomization was done by the physiotherapist including the patient. The investigator that evaluated the patients at six weeks, 12 weeks and 52 weeks was not including or randomizing patients. Baseline demographic data were collected and the patients were immediately instructed in postoperative rehabilitation according to which group they were randomized to. The patients were instructed to avoid any co-intervention and to contact the hospital with any question.
The primary outcome measure of this study was the Olerud–Molander ankle score (OMAS) which is a scoring system for evaluating symptoms and function after ankle fractures. 8 It goes from a minimum of 0 to a maximum of 100. It has been translated and validated for evaluation of function after ankle fractures in a Norwegian population. 9 Secondary outcome measures were visual analogue scale for pain (VAS) measured by a 0–100 mm scale. The patients were instructed to report their average pain within the last 24 hours. Length of hospital stay, analgesic use and surgical site infections, including re-operations and the use of antibiotics were also registered. All other adverse events were also registered, including deep venous thrombosis and re-operations due to other causes. Passive dorsiflexion range of movement was measured with goniometer according to the method described by Lindsjø et al. 10
At follow-up after three weeks, the OMAS, VAS, infections/reoperations or use of analgesics or antibiotics were registered. This follow-up was performed by a physiotherapist (J.H.) that was not blinded for group affiliation. Follow-ups after 6, 12 and 52 weeks were performed by a blinded physiotherapist (G.B.). On these exams, all the above mentioned measures were repeated as well as passive dorsiflexion range of motion measures.
The rehabilitation started the first postoperative day immediately after inclusion and randomization. One group was instructed to use a spring-loaded ankle trainer for postoperative training and the other group was instructed to use a non-elastic band (conventional physiotherapy) for stretching the ankle in dorsal motion.
The ankle trainer device provides a passive stretch to the ankle joint in dorsal flexion and provides a pressure of approximately 60 N (equivalent to about 6 kg of pressure) when the ankle is actively plantar flexed (Supplementary Figure S1). The patients can adjust the resistance of the ankle trainer to increase the pressure as pain resolves. The patients attended three daily sessions with 10 minutes of exercises. The ankle trainer was used for the first three weeks after surgery. After that conventional rehabilitation was continued.
The conventional group was instructed to use a non-elastic band for active assisted dorsal ankle motion. The provided pressure from the non-elastic band was individually adjusted and was limited by the patient’s pain level. They attended daily sessions with 10 repetitions of a 30-second hold in maximum ankle dorsal movement in three sets.
Both groups were instructed to use crutches in stairs and on flat surfaces the first day after surgery, as well as general postoperative exercises for muscular control and circulation.
A power analysis was performed prior to the study. It was based on the smallest clinical relevant difference in OMAS of 12 scale values. In a similar study, the standard deviation of the OMAS was 20 in the groups treated with different surgical treatment, and we estimated this standard deviation for our population. 11
Eighty-eight patients were needed (44 in each group) for the study to have 80% power and level of significance of 5%. To compensate the loss to follow-up, we chose to include 113 patients (56 and 57 in each group).
All our data were analysed using the statistical software SPSS (version 24). Parametric data are presented as means with standard deviations. T-tests were used for analysis, and P-values of less than 0.05 were considered statistically significant. Categorical data were analysed with chi-square tests.
Results
One hundred and forty consecutive patients with closed Weber b ankle fractures were screened for eligibility. Twenty (15%) did not meet inclusion criteria, 5 (4%) refused to participate and 2 (1%) were not asked. One hundred and thirteen (80%) were included in the study. Fifty-six were randomized to the ankle trainer and 57 to the conventional therapy. There were four dropouts in the ankle trainer group and eight dropouts in the conventional groups (Figure 1). Baseline demographic data are presented in Table 1. No statistically significant difference between groups could be observed for any of the baseline demographic data (P > 0.05).
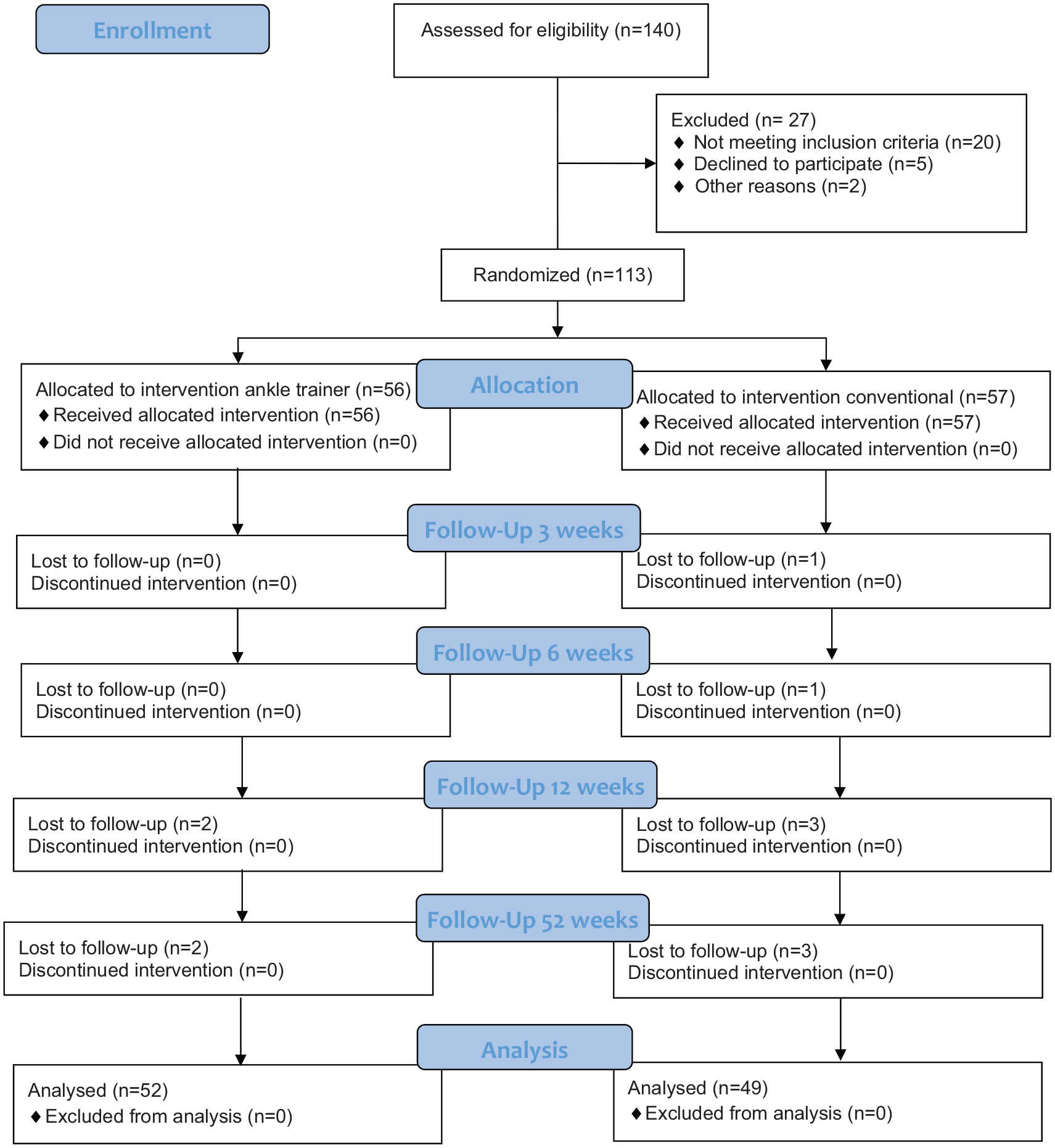
Flowchart.
Baseline demographic data.
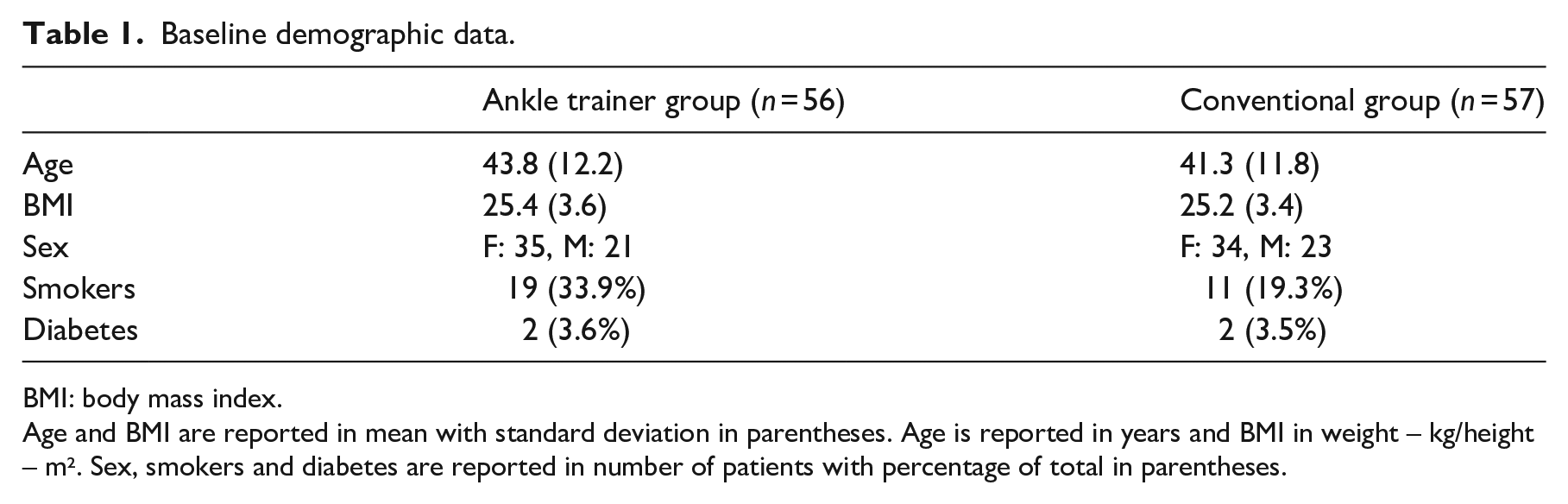
BMI: body mass index.
Age and BMI are reported in mean with standard deviation in parentheses. Age is reported in years and BMI in weight – kg/height – m². Sex, smokers and diabetes are reported in number of patients with percentage of total in parentheses.
Table 2 describes complete data for the clinical outcomes. The ankle trainer group had superior OMAS after three weeks compared to the conventional group (P = 0.021), while at 52 weeks, no difference between the groups on the OMAS (P = 0.386) could be observed. There was neither difference in VAS between the groups at any follow-up nor difference in the number of patients using analgesics or measured passive dorsiflexion at any of the follow-ups.
Clinical outcome data.
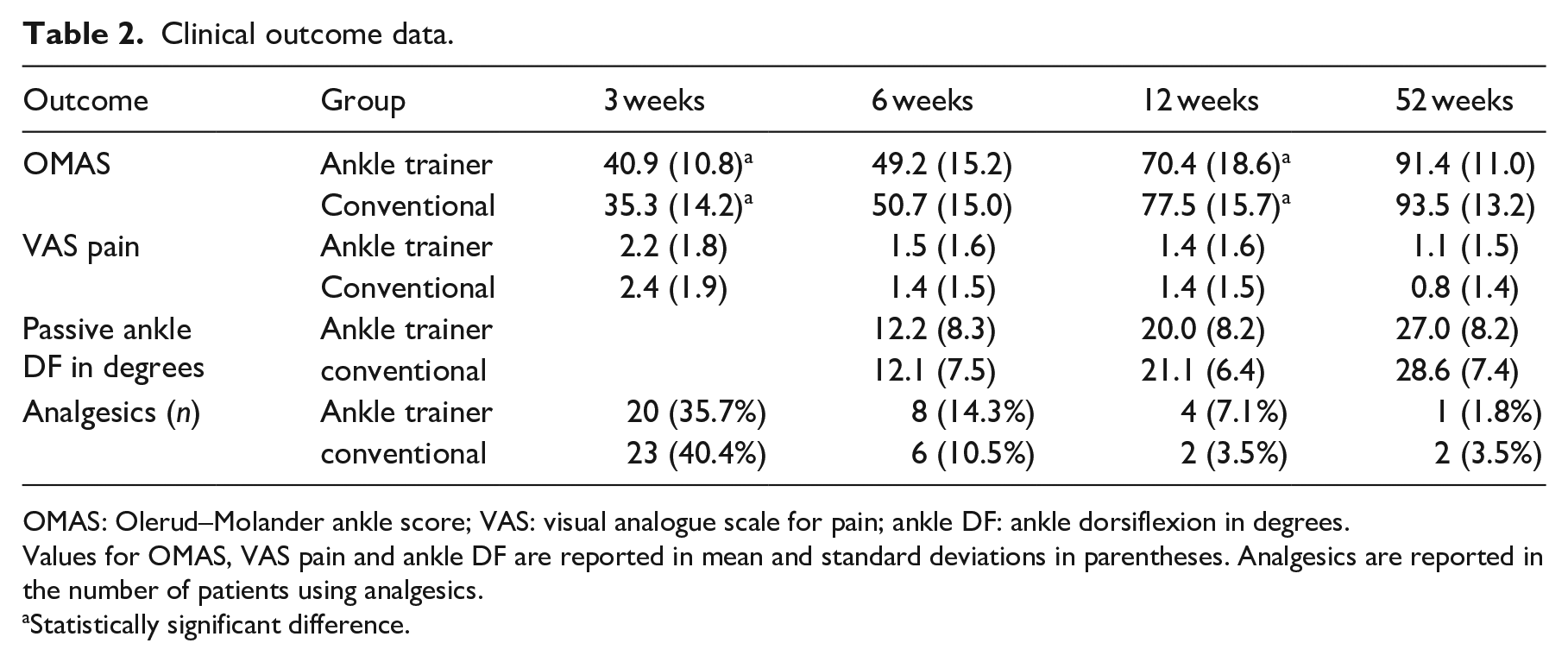
OMAS: Olerud–Molander ankle score; VAS: visual analogue scale for pain; ankle DF: ankle dorsiflexion in degrees.
Values for OMAS, VAS pain and ankle DF are reported in mean and standard deviations in parentheses. Analgesics are reported in the number of patients using analgesics.
Statistically significant difference.
The ankle trainer group had a significant shorter hospital stay with a mean of 2.6 days (0.98) compared to 3.2 days (1.47) in the conventional group (P = 0.026).
No difference in complications were observed between the groups (P = 0.140). The ankle trainer group had six superficial surgical site infections, while the conventional group had one superficial and one deep infection. The superficial infections were treated with antibiotics and the deep infection underwent surgical revision. No other adverse events were registered.
Discussion
There was no difference in functional outcomes, measured by the OMAS, ankle dorsiflexion motion or pain between the groups at one-year follow-up. However, the group that was randomized to the ankle trainer device had higher OMAS at three weeks follow-up and shorter hospitalization than the control group.
It has been well documented that patients suffering from an ankle fracture might sustain long lasting pain, stiffness and oedema.1,2 Based on this, the technique for operating ankle fractures is based on achieving an exercise stable fixation allowing early range of motion. Although early range of motion exercises, at least theoretically, would avoid many of the usual postoperative problems, it has not been proven that early mobilization lead to better functional outcomes than immobilization in the long term.1,2,12 However, several studies have showed a tendency for improved functional outcomes in the short term follow-up if early range of motion is allowed.1,2,12,13 Some studies have also investigated the relationship between early weight bearing and functional outcomes. The reported results are similar to the results from the above mentioned studies allowing early range of motion exercises, with improved functional outcomes in the short term (6–12 weeks) that even out at later follow-ups.12,14,15
Most other studies compare early versus late mobilization and early versus late weight bearing. Obviously, no study could be completely comparable to this study, as the device investigated in this study is completely new. However, a few studies investigate differences in functional outcomes between rehabilitation protocols that both focus on motion exercises. Jansen et al. 13 compared conventional physiotherapy alone to conventional physiotherapy in addition to the use of an active controlled motion device. The group that received the active controlled motion device reported superior functional results as long as the device was used. 13 Contradictory to this, Moseley et al. 3 were not able to detect any between group differences at four weeks or three months follow-up on the lower extremity functional scale or dorsiflexion range of motion when comparing one group that received regular postoperative exercises with one group that received additional short duration with stretching exercises and another group with additional long duration exercises.
The patients from both groups of our study were mobilized immediately after surgery and were all allowed early range of motion exercises and partial weight bearing. The differences in treatment protocol between the groups therefore seem to be smaller in our study than in other studies on the topic. Despite this homogeneity of rehabilitation protocol, we were able to observe statistically significant differences in favour of the ankle trainer group on the outcomes of length of hospitalization and OMAS at three weeks follow-up. This is the same time period that the ankle trainer was used. However, it should be recognized that this observed difference between groups at three weeks follow-up did not reach the predefined minimal clinical important difference in OMAS of 12 scale points. Application of manual therapy aims to evaluate the stiffness of the restricted tissue and adapt the applied force to the patient’s characteristics in each moment. The ankle trainer device has the theoretical advantages that it provides a passive stretch to the ankle joint in dorsal flexion and provides a pressure when the ankle is plantar flexed (Supplementary Figure S1). The active plantar flexion given to the applied resistance is intended to increase venous pump activation, which in turn increases circulation. The ability to adjust the load pressure may also contribute to an improved control of the axial pressure against the ankle joint. Alternating contraction of agonist and antagonist muscles acting on the ankle joint may reduce joint stiffness and increase joint stability. The load pressure of the brace may correlate to the load pressure given by the ground when walking, compared to conventional postoperative stretching and open kinetic chain exercises.
Six of the patients in the ankle trainer group (10.7%) had a surgical site infection compared to two (3.5%) in the conventional group (P = 0.14). However, seven out of eight of these were superficial infections that healed uneventfully with antibiotics. Early ankle mobilization before wound healing has been associated with increased complication rates such as wound infection and fixation failure.1,2,16,17 Infection rates after surgically treated ankle fractures generally vary from 1% to 10% in the literature, although some have reported even higher infection rates, up to 27%.2,16,17 Both groups from our study were mobilized within a day after surgery which did not seem to lead to increased incidences of adverse events when comparing with the results from previous studies with more restrictive rehabilitation protocols.2,16,17 Only one deep surgical site infection, needing surgical revision in a total of 113 patients from both groups, must be considered a very low number of serious adverse events.
The study had some limitations. A follow-up time of 12 months might be too short to make conclusions on the final result, although it might be considered unlikely that the result will be different at a later time point. As the purpose of the study was to investigate the short term results of a group treated by an ankle trainer device compared to conventional physiotherapy, we believe the follow-up time is sufficient to answer this question. Eleven patients were also absent to follow-up, which could represent a weakness of the study.
As this study only include patients who received surgery as treatment for their ankle fracture, the results could not automatically be generalizable to ankle fractures that are treated conservatively. It has been described that fractures treated conservatively also suffer from the same problems in terms of long lasting stiffness and pain. 1 A Cochrane review concluded that there is little evidence for rehabilitation interventions during the immobilization period after conservative orthopaedic management and no evidence for stretching, manual therapy or exercise compared to usual care following the immobilization period. 1 From a logical point of view, the effect of the ankle trainer device would be the same when used for these patients, and it could therefore be anticipated that the ankle trainer device would have the same effect in patients treated non-operatively as observed in this study.
The strength of this study is that it was a prospective randomized trial where the physiotherapist was blinded for group affiliation. The main outcome of OMAS is a well-established outcome score that has been validated for ankle fractures. 9 This study is also to our knowledge the first randomized controlled trial to compare the use of an ankle trainer versus conventional physiotherapy after surgically treated ankle fractures.
The clinical implications from this study are two-sided. The excellent outcome scores from both intervention groups, as well as a low complication rate, support the results from most other studies that early mobilization lead to overall excellent outcomes after surgically treated ankle fractures.
In addition, the new ankle trainer device show superior results compared to conventional physiotherapy in the period it was used. The ankle trainer device is the standard rehabilitation protocol at our hospital after the findings from this study
Clinical messages
The ankle trainer device shortened hospital stay and led to better Olerud–Molander ankle scores at three weeks follow-up compared to conventional physiotherapy for surgically treated Weber b ankle fractures.
No long-term differences in terms of pain, function or ankle motion could be observed between patients treated with the ankle trainer device and patients treated with conventional physiotherapy.
Supplemental Material
Suppl_Material – Supplemental material for Compared to conventional physiotherapy, does the use of an ankle trainer device after Weber B ankle fracture operation improve outcome and shorten hospital stay? A randomized controlled trial
Supplemental material, Suppl_Material for Compared to conventional physiotherapy, does the use of an ankle trainer device after Weber B ankle fracture operation improve outcome and shorten hospital stay? A randomized controlled trial by Marius Molund, Jan Hellesnes, Gøran Berdal, Bernt Stray Andreassen and Geir Stray Andreassen in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors want to thank Espen Sjåberg for help with including patients in the study.
Author Contributions
M.M., J.H. and G.S.A. initiated this study and designed it. G.B. and J.H. monitored the progress and collected the data. B.S.A. wrote the first version of the article, organized the data and did the statistical analysis. M.M. wrote the final version of the article and G.S.A. revised it. M.M. is the guarantor of the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was funded by Oslo University Hospital.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.