
Abstract
Objectives:
To explore the feasibility of using a stroke-specific toolkit for six-month post-stroke reviews in care homes to identify unmet needs and actions.
Design:
An observational study including qualitative interviews to explore the process and outcome of reviews.
Setting:
UK care homes.
Participants:
Stroke survivors, family members, care home staff (review participants) and external staff involved in conducting reviews (assessors).
Interventions:
Modified Greater Manchester Stroke Assessment Tool (GM-SAT).
Results:
The observational study provided data on 74 stroke survivors across 51 care homes. In total, out of 74, 45 (61%) had unmet needs identified. Common unmet needs related to blood pressure, mobility, medicine management and mood. We conducted 25 qualitative interviews, including 13 review participants and 12 assessors. Three overarching qualitative themes covered acceptability of conducting reviews in care homes, process and outcomes of reviews, and acceptability of modified GM-SAT review toolkit. The modified GM-SAT review was positively valued, but stroke survivors had poor recall of the review event including the actions agreed. Care home staff sometimes assisted with reviews and highlighted their need for training to support day-to-day needs of stroke survivors. Assessors highlighted a need for clearer guidance on the use of the toolkit and suggested further modifications to enhance it. They also identified organizational barriers and facilitators to implementing reviews and communicating planned actions to GPs and other agencies.
Conclusion:
The modified GM-SAT provides a feasible means of conducting six-month reviews for stroke survivors in care homes and helps identify important needs. Further modifications have enhanced acceptability. Full implementation into practice requires staff training and organizational changes.
Introduction
Across England, Wales and Northern Ireland, national guidance and good clinical practice recommend a structured review of patients’ health and social care needs six months after a stroke and at intervals thereafter. 1 A national audit in 2016 found that less than a third of people received one, 2 despite the publication prior to three years of a suitable review tool, the Greater Manchester Stroke Assessment Tool (GM-SAT). 3
The GM-SAT covers common, long-term, post-stroke needs and was codeveloped with patients, carers and professionals. The toolkit comprises various resources to support uptake and delivery of reviews, including a form that guides the professional reviewer (assessor) through the review and a one-page summary report to capture and communicate the outcomes and actions (see http://bit.ly/GM-SAT). Prior to the development of the stroke-specific GM-SAT, generic assessment tools existed such as the Southampton Needs Assessment. 4 Other stroke-specific tools exist to support healthcare professionals to deliver reviews in primary care settings 5 or for stroke survivors to self-administer; 6 however, GM-SAT is recommended by the British Association of Stroke Physicians (BASP) 7 and the National Institute for Health and Care Excellence (NICE). 8
Despite the wide implementation of the GM-SAT in services providing six-month reviews, early validation excluded people in care home settings, which may affect acceptability in this substantial cohort (estimates suggest that 18% of care home residents in the United Kingdom are stroke survivors 9 ). Equity of access to stroke-specific rehabilitation and secondary prevention interventions is a particular issue for care home residents, 10 which catalysed efforts to enhance GM-SAT for use in care home settings.
Informal quality improvement work with service providers conducting reviews generated feedback which we incorporated with consensus from expert group meetings to modify the GM-SAT review form and summary report for use with care home residents. Some questions were removed as they were deemed irrelevant to care home residents (e.g. work; driving); others were modified (e.g. sex; transport) and some added (e.g. oral hygiene; skin integrity; foot care; concerns of care home staff). This article reports on the feasibility of the modified GM-SAT in care homes exploring barriers and facilitators to delivery, acceptability and the outcomes generated.
Methods
The study received research ethics approval from NRES Committee North West (No. 15/NW/0643) and was jointly funded by the Stroke Association and the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care Greater Manchester (NIHR CLAHRC GM). The University of Manchester acted as the sponsor and played no role in the design, execution, data analysis and interpretation, or write-up.
Design
We used parallel mixed methods to describe the process and outcome of reviews both quantitatively and qualitatively from different stakeholders’ perspectives, in order to explore feasibility and acceptability. An observational study collected summary data from a cohort of reviews in care homes between June 2015 and July 2016 and qualitative interviews were conducted with review participants (stroke survivors, family members and care home staff) as well as external staff involved in setting up and/or conducting six-month reviews (assessors).
Sites and participants
We recruited from services based in the North West of England. They were eligible if they were already using the original GM-SAT to deliver reviews in care home settings as part of routine care; willing to test the modified GM-SAT and provide anonymized data extracted from the summary reports of all reviews in care homes conducted during the study period. In addition, we invited a range of stakeholders to provide qualitative data on the review process describing their experiences providing or receiving care. All assessors and all review participants with capacity to consent were eligible for the interview.
Data collection and procedures
Our observational study and qualitative interviews ran in parallel. Our research procedure began when staff commissioned to visit care homes to provide reviews (assessors) notified the research team by telephone that a routine review had been arranged. The stroke survivor was then assigned a unique study number and the assessor provided anonymized demographic and clinical data about the stroke survivor, including the modified Rankin score as an indicator of stroke severity. 11 On completion of the review, the assessor sent the study team the anonymized modified GM-SAT summary report (see Supplemental Appendix 1). We extracted data on unmet needs and actions identified from the summary reports and entered these into a purpose-built study database. Unmet needs were defined as ‘a problem that is not being addressed or one that is being addressed, but insufficiently’. 3 If there was uncertainty about whether data met this definition, at least two researchers consulted to agree a classification at the point of data entry, and again on final data cleaning to ensure consistency across the whole data set. Using study numbers, researchers could link the descriptive and review data without having access to any personally identifying data on stroke survivors up to that point.
After each review was completed, assessors provided easy-access study information to the person reviewed if they deemed the stroke survivor had the capacity to consent. If the person agreed to be contacted about the research, their identifying information was securely passed to the research team, who arranged a visit to take informed consent and interview as soon as possible. The consolidated criteria for reporting qualitative research (COREQ) checklist was used to report the qualitative components of this study. 12 We provided stroke survivors with the option to include family members or care home staff in the qualitative interview if the latter had contributed to the review process (collectively called review participants). We estimated that approximately 15 of these interviews would be required to reach data saturation. 13 We planned to conduct purposive sampling based on stroke survivor sex, age, geographical location and whether or not they were resident in a care home before their stroke, and planned to conduct follow-up interviews three months later to explore opinions on longer-term review outcomes. Finally, we invited all assessors – including support staff instrumental in organizing reviews- to be interviewed separately.
All interviews followed semi-structured topic guides with a different guide for assessors and review participants (see Supplemental Appendix 2). Two experienced female researchers (E.P. and K.W.-N.) conducted all interviews with assessors, who were known to the researchers, and with review participants who were unknown. Informed consent was obtained prior to the interview. During interviews, we provided communication support resources (e.g. prompt cards) as required.
Data analysis
Quantitative data from our observational study were analysed descriptively including sample characteristics, categories of unmet needs identified, proposed actions to address and agents designated to carry out actions.
Qualitative interviews were audio-recorded with consent and transcribed by an external professional transcription service. We used field notes to support the interpretation of transcripts where non-verbal communication was utilized. We uploaded interview transcripts and field notes to the NVivo software for thematic analysis. 14 E.P. and K.W.-N. coded all interviews. In our analyses of interviews, we actively derived themes based on our study aims and the domains in the topic guides, for example, experiences of conducting or receiving reviews in care homes with the modified GM-SAT toolkit.
Results
We identified 14 services in the North West United Kingdom for potential inclusion as they conducted post-stroke reviews. Eight were eligible and all agreed to participate: five National Health Service (NHS) community stroke teams and three from a third sector organization commissioned to deliver reviews. Only two NHS services had administrative support for implementing reviews, and in the other services the professionals conducting the review were also responsible for all administrative tasks.
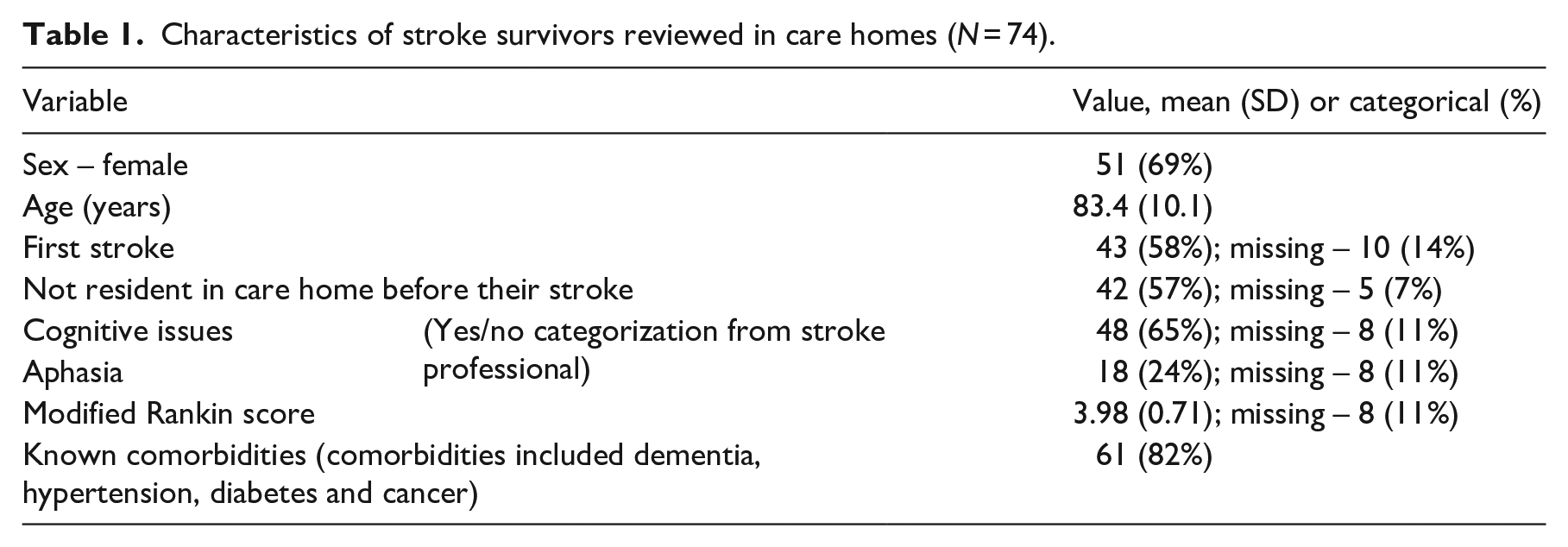
A total of 74 reviews were carried out across seven of the eight participating services in 51 different care home locations (one NHS service did not conduct any care home reviews during the study period). Reviews with modified GM-SAT took an average of 51 (range = 20–90) minutes and were all conducted by 11 professionals. The majority of stroke survivors reviewed were female and just over half were not resident in a care home before their stroke (see Table 1). They often had cognitive difficulties and comorbidities.
Characteristics of stroke survivors reviewed in care homes (N = 74).
In terms of extracting unmet needs and actions for data entry, there was a variation in how assessors completed the GM-SAT summary reports requiring considerable researcher consultation to ensure consistency in interpretation. We found that many participants (45/74) had multiple unmet needs identified at six months using the GM-SAT. The average per person was 2.5 (SD = 1.7; maximum = 6), with 111 identified in total. Unmet needs were identified across a wide range of categories, spanning health, well-being and social participation (Table 2). In some cases, the needs identified were serious and urgent. For example, low blood pressure readings that revealed a stroke survivor had not been having medication review or management. In this case, the resulting action was that the reviewer immediately called and faxed the patient’s general practitioner (GP). In another case, unmet needs included regular pain and the reviewer recorded an action that the patient ‘Should be on Gabapentin or Pregabalin for pain, but is not on either’.
Unmet needs identified across domains reviewed in the observational study (N = 74 reviews in care homes).
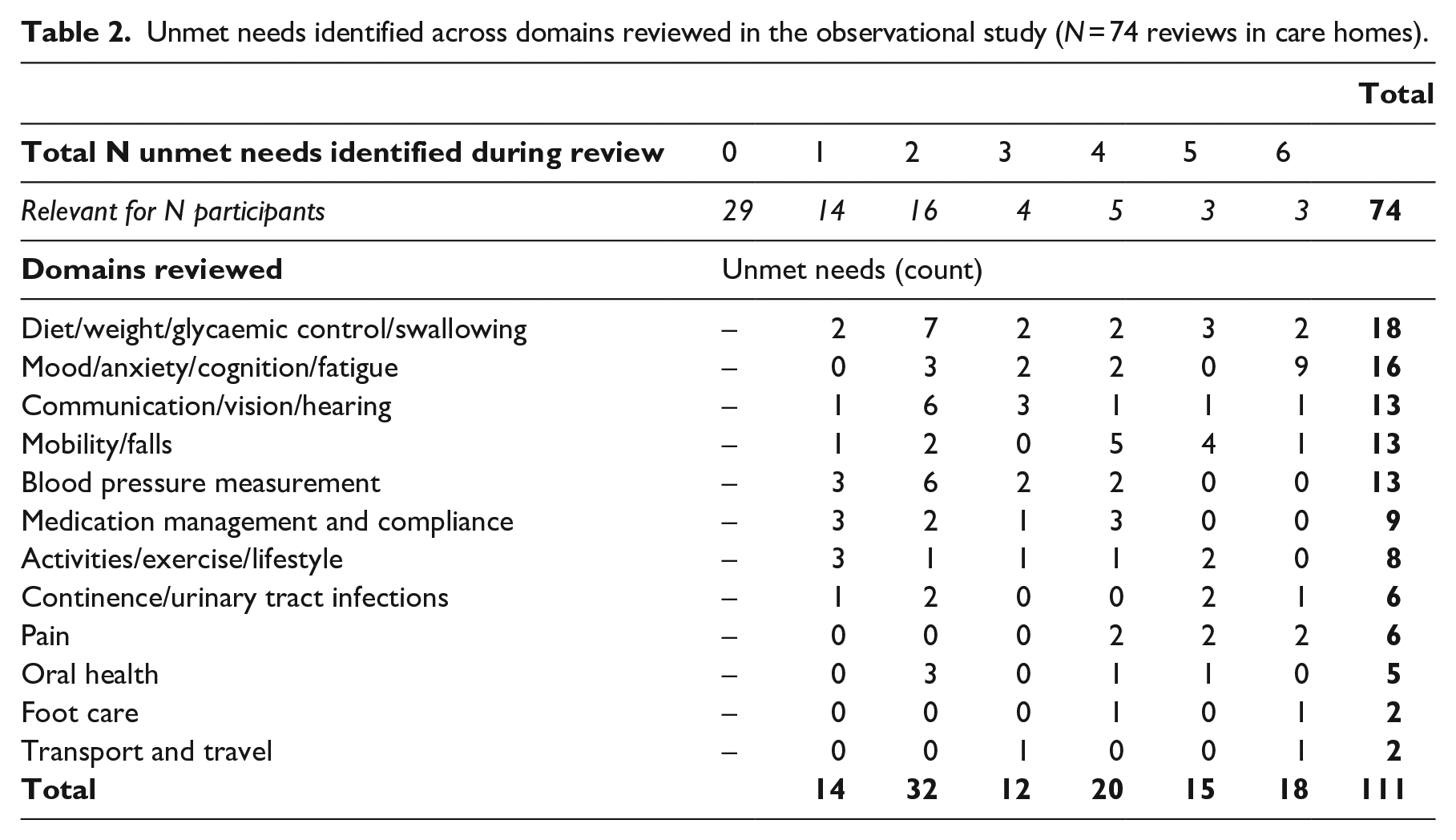
Referral action was noted on the summary forms for 29 of the 111 needs identified (e.g. for Speech Therapy, Occupational Therapy, Physiotherapy, Dietitians; Mental Health; Falls Services), but it was often unclear who should make this referral, for example, the GP, the care home staff or the assessor themselves. Disentangling ‘action’ from ‘agent’ was also challenging for the remaining 82 of the 111 needs. For example, 10 needs had ‘self-management’ components, such as the stroke survivor being advised to use aids or strategies (e.g. denture fixative, taking regular naps to address fatigue), but it was not clear how these would be implemented; 12 needs were categorized as requiring ‘information giving’ and it was unclear whether this was an action for the care home and whether they had been informed; 57 needs had actions that could be broadly categorized as requiring active monitoring or management from either the care home staff (n = 26), GP (n = 24) or both (n = 7). For care home staff, this might involve monitoring and action if required (e.g. ‘monitor tablet swallowing; consult with pharmacist or GP as needed’) or a prompt to immediate action (e.g. ‘care staff to arrange to cut toe nails’).
In addition to extracting these data (on needs and actions from the review summaries), we conducted qualitative interviews with 12 assessors and 13 review participants to explore their experiences of these reviews. Of the former, we interviewed the two female administrative assistants who supported organization of reviews and 10 of the 11 female professionals who delivered reviews agreed to be interviewed. Seven of these were from NHS community stroke teams: two therapy assistants, three stroke nurses (including one nutritional specialist), one occupational therapist and one physiotherapist. The remaining three professionals were from the third sector services, two of whom had a nursing background.
The 13 review participants were interviewed from five of the eight participating services: eight stroke survivors, three family members and two care home staff (see Table 3). All eligible review participants who agreed to be contacted were invited to interview as soon as possible after the review. However, seven of the eight stroke survivors interviewed could not remember any specifics about the review. These recall difficulties resulted in minimal data from stroke survivors, so we decided that the three-month follow-up interviews were not viable. We also decided that data from stroke survivors were not sufficient to warrant separate analysis, but rather than exclude them we incorporated them with the assessors’ data where we observed shared meaning.
Characteristics of the stroke survivor review participants interviewed (N = 13) a .
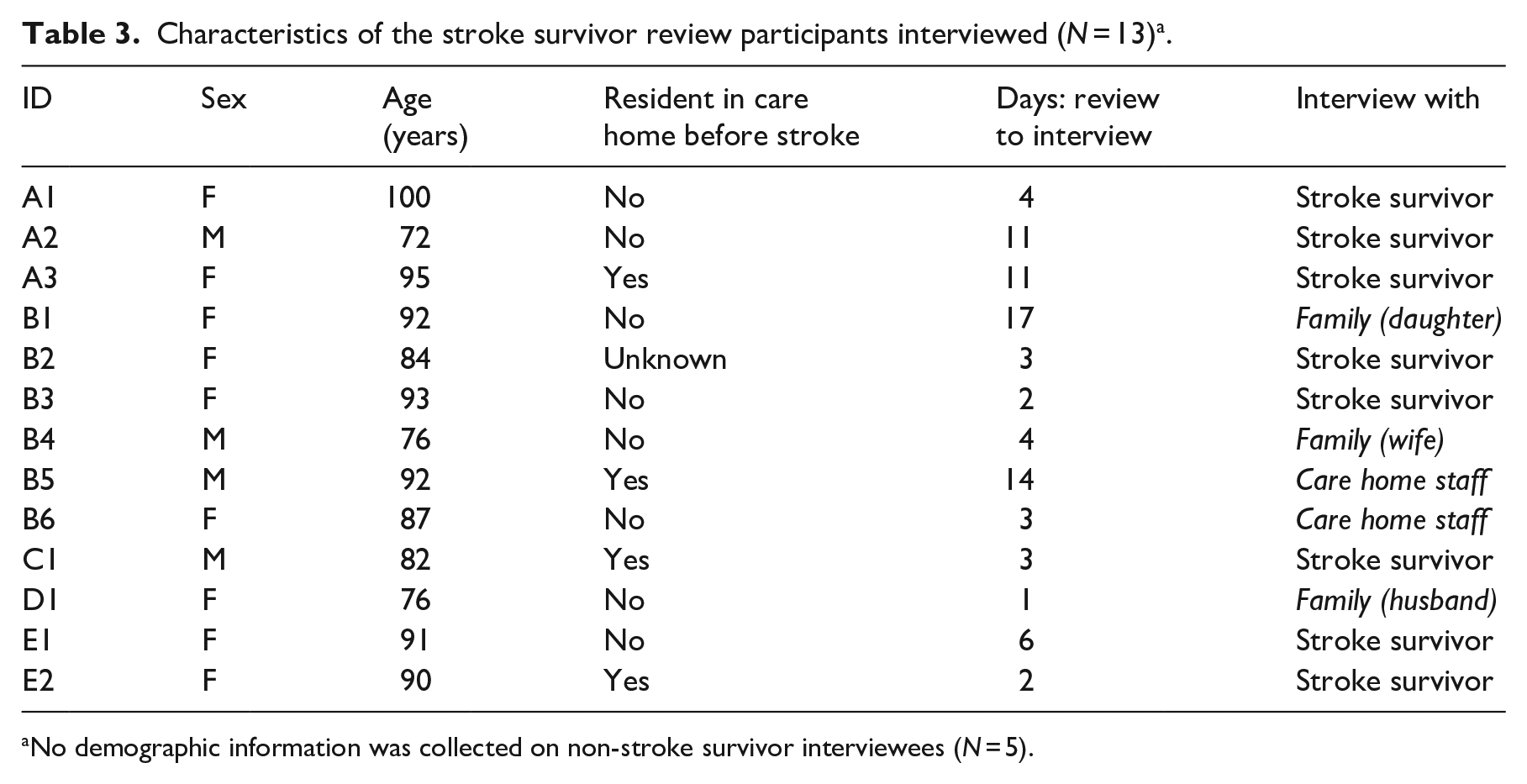
No demographic information was collected on non-stroke survivor interviewees (N = 5).
Themes are outlined in Figure 1, with full presentation below.
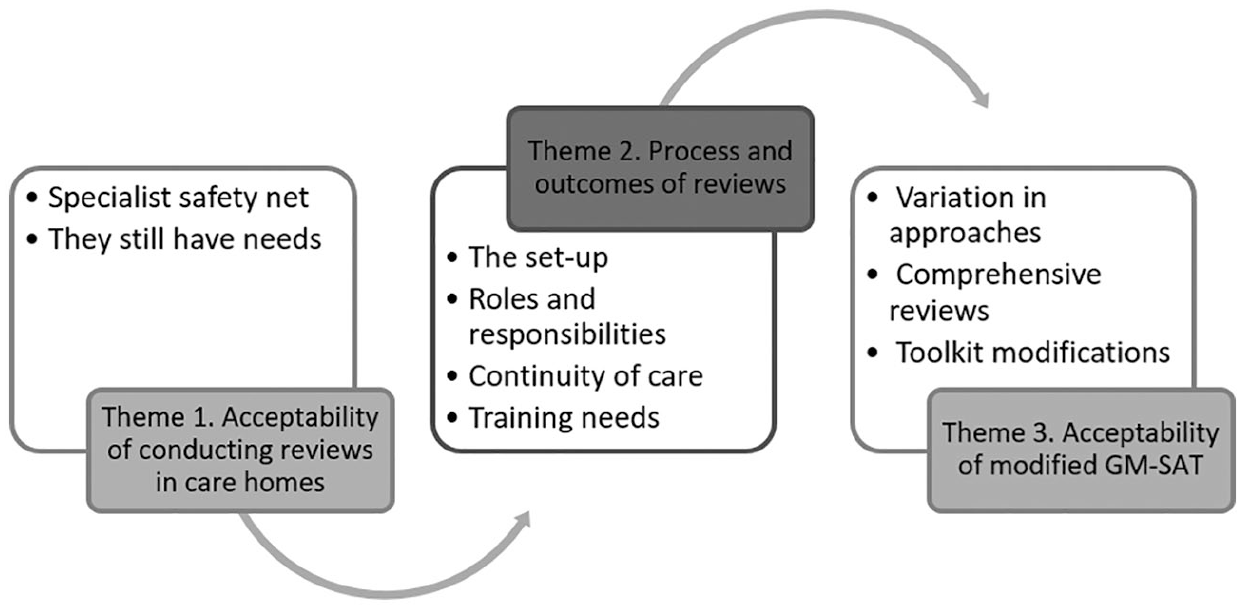
Qualitative themes, using study aims as the framework.
Theme 1: acceptability of conducting reviews in care homes
Specialist safety net
Almost all stroke survivors interviewed felt that the reviews were positive and valuable, despite not remembering many specifics of the review, including setup or outcomes. However, one stroke survivor – who was quite unwell – said, ‘Well . . . I don’t think anything is useful to me now’. Similarly, an assessor also questioned the value of reviews for particularly severely impaired individuals:
It does have value on a lot of occasions, but if you’re knowing you’re going to see someone who’s got severe Alzheimer’s, aphasic . . . you probably wouldn’t be able to help them anyway, because they are beyond that sort of help. (A3 – assessor)
However, this same reviewer described the importance of including relatives in reviews with these individuals.
In most cases, reviews were viewed as a ‘safety net’ (C1 – assessor) for a vulnerable population and could have spilled over benefits for improving care home staff knowledge more generally:
It doesn’t matter to me if the person’s got dementia or cognitive issues, I still, I find them valuable with the staff and I just think it gets the care home staff thinking sometimes . . . just reminding them about basic things and all that, you know, and just making them aware of the effects of the stroke. (C1 – assessor)
The benefit of a stroke specialist reviewing recovery was echoed by the wife of B4 and the husband of D1 for example:
She comes in with a different perspective and she’s professional, she’s the expert. I think it was reassuring to [stroke survivor] just that somebody else is coming in. The care in here, the caring goes on, but they aren’t stroke specialists, they’re covering a multitude of conditions here. (D1 – husband)
One care home staff summarized the general importance of reviews for her residents:
I do think it’s valuable. I think it’s important as well, because we don’t know everything about everybody’s care, and specifically when it comes to a stroke, everybody is affected differently. So, I do feel the questionnaires are valid, and that the reviews are valid, just for that alone. (B3)
They still have needs
Some professionals expected that care home residents would have fewer unmet needs than their community-based counterparts because of the 24-hour care that they receive. This was supported by the daughter of participant B1, who was positive about the review but felt that her mother was well looked after and that needs were generally dealt with as they arose. However, there were often surprises that could be picked up in reviews:
Before I’d done any reviews in a care home I did sort of think, is this of value? Because people are being looked after, but actually in a care home quite a few things can come up, especially if somebody wasn’t in a care home before they had their stroke and they are now in a care home, there can be quite a few sort of teething problems that we pick up. (F1 – assessor)
In addition, stroke professionals highlighted the complex care and stroke-specific needs of this demographic that could be challenging to address for care home staff without specialist expertise.
Theme 2: process and outcomes of reviews
The setup
From the assessors’ perspective, methods of identifying stroke survivors who were due a review were variable and would depend on commissioning and resource. For example, one professional described identifying individuals for review through a hand-search of paper records; no administrative support or electronic system existed at the time of interview. In general, the mechanisms for ensuring that all eligible stroke survivors were offered a review were ‘hit and miss’ (D1 – assessor).
Once identified, most assessors arranged the review appointment with care home staff and families were sometimes contacted; stroke survivors were rarely included in the appointment setup:
I can either arrange it with the family if family are quite involved, so that it’s quite useful sometimes . . . or I can liaise with the care home and arrange to go and see somebody. (F1 – assessor)
Stroke survivor review participants interviewed did not think they had been involved in the setup of reviews but, as above, recall difficulties were common.
Roles and responsibilities
As highlighted in the observational study, professionals from a variety of backgrounds could facilitate a review. Stroke-specific knowledge was seen as the most important facilitator for conducting a successful review:
I think we presumed that it would be better for nursing staff to do and in reality I think it’s about your skills as a practitioner in stroke that matter really more than anything. (E1 – assessor)
As in Theme 1, review participants appreciated having someone with stroke-specific skills and knowledge to help deliver a comprehensive review.
Continuity of care
In many cases, the professional conducting the review may not have met or treated the stroke survivor previously, so additional background data to support the review process might be sought, for example, discharge summaries. However,
. . . Even if the person knows you and has dealing with your team in the past, they might not have been as open, when you’re dealing with them, and I think actually, asking the questions, even if you [think you] know the answers, you might be surprised at the answers. (A1 – assessor)
One stroke survivor interviewed who could not remember the review content (A2), only remembered that the professional conducting his review was someone he had met previously and that he found this continuity comforting.
In terms of communicating outcomes, assessors tended to verbally summarize with review participants immediately post review, with the one-page summary report sent later to the stroke survivor as well as their GP. Care home staff might not be sent a copy of the report directly but wanted it: ‘A copy of the [full] review for the care plan . . . would have been helpful, definitely’ (B5, care home staff).
After the summary report had been sent by post and the stroke professional had completed any actions for which they were the designated agent (e.g. sending information sheets or making referral), there were very few mechanisms for following up. Generally, this was cited as due to commissioning arrangements or limited resources/systems for communicating with other agencies. This was highlighted as a major area for improvement.
Training needs
Both of the care home staff interviewed raised a desire for stroke-specific knowledge and training to enable them to better meet the needs of their residents with stroke on a day-to-day basis. For assessors, a challenge to communicating review outcomes was the potential for care home staff to feel judged or ‘under review’ themselves as part of the process. Assessors highlighted issues balancing relationships with care home staff:
I think if you’ve not met the care staff before, you just need to be really careful about how you sort of go in. You’re not going in and telling them what to do, they’re the ones that are caring for the client, but just about how can we support you looking after this person, more that sort of attitude, really . . . you have to kind of manage the needs of the care staff, in other words, not rubbing them up the wrong way, but looking after the needs of the client from other parties that we wouldn’t normally perhaps do. (F1 – assessor)
Theme 3: acceptability of modified GM-SAT
Variation in approaches
A variety of different approaches to using the GM-SAT were highlighted by assessors. Some used it in ‘more of a conversation-style’ (D1 – assessor) and this could be useful for accommodating varying cognitive or communication needs. When used in this way, the GM-SAT may be useful as a prompt to ensure that no items had been missed as ‘I would forget stuff if it wasn’t there’ (D1 – assessor). Others used the tool more systematically:
I structure it exactly the way as it is, cause I just think it’s so comprehensive that if you leave out any part of that, then you’re not doing the patient justice, you’re not asking them. (A1 – assessor)
The modified GM-SAT was viewed as highly acceptable for conducting reviews, regardless of the approach being used. No review participants interviewed recognized the term ‘GM-SAT’ or the paperwork itself, but they appeared to find the review process broadly acceptable.
Comprehensive reviews
Professionals highlighted the holistic nature of GM-SAT, which could identify needs that they found difficult to address. For example, needs that related to a desire for more social participation may required care home residents to access support to travel and attend external groups or events, which was often difficult. Professionals acknowledged that this could make carrying out the GM-SAT review a challenge: ‘It sometimes feels a bit like you’re asking a question but don’t have a solution’ (E1 – assessor). However, they maintained that it was still necessary to ask questions and hear answers/provide reassurance. Care home staff echoed the importance of understanding needs from a ‘spiritual, cultural, emotional, and physical wellbeing place’ (B3).
In general though, care home residents were perceived as having less autonomy and more medical or safety considerations, which could affect the acceptability of such a holistic review. Assessors used some judgement and sensitivity before asking certain questions of all review participants, which may explain why family members – who remembered the process far better than stroke survivors – tended to find the questions acceptable.
Toolkit modifications (assessors only)
The modifications to GM-SAT were felt to be useful in care homes and had potential for use with community-dwelling stroke survivors too:
I do find the little bits on the one we use for the nursing homes are quite good because sometimes you don’t think twice about nail care and skin integrity and things like that with everybody. (B1 – assessor)
Or, on the contrary, they questioned the rationale for adaptation/removal of some questions:
We shouldn’t assume that people don’t have sex because they’re in a care home. (F1 – assessor)
Assessors also highlighted that, while the modified GM-SAT was useful in care home reviews, remembering to take the correct tool for a review, depending on stroke survivor location, was an administrative burden that could be reduced by having a single modified tool. In addition, some improvements were suggested to the layout and ordering of questions to give more space for notes alongside each question and improve the flow of items, in terms of grouping similar topics together, for example, lifestyle questions are useful all together (healthy eating, smoking, alcohol, exercise).
Discussion
This exploratory roll-out of a modified GM-SAT suggests that the toolkit is feasible for conducting post-stroke reviews in care homes, although additional enhancements have been identified to improve acceptability and reduce administrative burden. Quantitative data and qualitative feedback on reviews with GM-SAT in these settings show that they identify a range of specific issues across domains of health, emotion and social participation that, while potentially challenging to address, speaks to the value of these reviews for picking up important and relevant unmet needs in this population. Additional qualitative data reveal barriers and facilitators related to delivery of reviews as well as effective continuity of care.
We have highlighted professionals’ uncertainty around addressing identified needs in terms of ‘what happens next and by whom’. This could reflect the variety of commissioning structures and resources available for follow-up and communication. Where annual reviews are not commissioned and/or communication linkages between services are not well supported, there is little infrastructure to follow up on actions identified. Given that six-month and follow-up reviews are mandated in national guidelines, 1 this could and should be resolved through commissioning of a comprehensive package of Life After Stroke services.
The study also revealed that individuals conducting reviews come from a wide range of professional backgrounds, including junior therapy assistants. This suggests positive potential for mobilizing a workforce to increase capacity for delivering reviews in future. The need for stroke-specific skills, knowledge and training was highlighted as important by all stakeholders in order to conduct effective reviews and – in the case of care home staff – meet needs on a day-to-day basis.
We were only able to collect the single-page GM-SAT summary reports due to difficulties anonymizing the full review forms, and considerable researcher consultation was required to ensure consistency in interpretation for extracting data on unmet needs. The full GM-SAT review forms would likely have supported contextualization and interpretation and it would be useful to collect both forms for future research, to compare, contrast and explore completeness of the data. However, the challenges of data interpretation related to unmet needs and actions have revealed genuine learning points for clinical practice. For example, there is a need for improvements in the GM-SAT toolkit and guidance as well as enhancements in workforce training to help ensure clarity and promote consistency in reviews across populations. As a next step, we have implemented this learning through the development of an improved review toolkit, called GM-SAT2, which is freely available on-line (http://bit.ly/GM-SAT) and applicable for all stroke survivors, regardless of residential location or cognitive abilities. It includes guidance documents and we have delivered workforce training events to support consistency in implementation and delivery.
In the observational study, we aimed to capture only ‘unmet needs’ and their associated actions as we felt this would give us insight into the ‘added value’ that a review offers for care home residents, who may be more likely to have needs being met or managed by care home staff. However, this was challenging to extract with consensus and also means that we have no data on the ‘met’ needs of this population at the time of the review, including if/how all possible domains of need were actually reviewed. Knowing all needs – considered, met and unmet – would increase understanding of how to improve reviews, as well as how care home staff can be supported to meet the day-to-day needs of their stroke survivor populations.
This limitation of our quantitative data is overcome in part by our qualitative interviews that explore a range of stakeholder views. Professionals from the care homes, NHS, third sector and administrative personnel all participated and we sought viewpoints from stroke survivors themselves as well as family members, where appropriate. These stakeholders commented broadly on the process and outcomes of reviews in this population. It is a limitation that we were unable to gather more stroke survivor viewpoints; planned interviews with them were stopped early due to recall issues. Pragmatically, some delay before interview was necessary, and while interviews were conducted within a few days, any delay may have affected stroke survivors’ recall.
In addition, our sample was drawn from services that were already routinely conducting reviews in care homes using GM-SAT; the experience and opinions of these assessors may be different to those who are not conducting reviews with this toolkit in this population. However, suggestions for improving reviews from early adopters may help increase spread and sustainability.
Despite the limitations of this work, the study adds to the sparse literature on the care of stroke survivors in long-term facilities.10,15 Other tools to support the conduct of post-stroke reviews have not been validated in care home settings 6 or designed for use in primary care settings 5 so we are optimistic that the updated toolkit derived from this work (GM-SAT2) will be a useful resource for clinical practice. We invite feedback from readers to further enhance its usefulness as an evolving toolkit.
Post-stroke reviews are an important safety net for this vulnerable population of care home residents. This study has highlighted difficulties in setting up and delivering reviews to all eligible stroke survivors; the importance of stroke-specific knowledge for conducting reviews; and the barriers to effective continuity of care – particularly since the six-month reviews typically standalone with little resource to implement actions identified and follow-up. In line with national guidance in England, Wales and Northern Ireland, 1 this study recommends that long-term, follow-up reviews of care home residents – and all community-based stroke survivors–should be standard practice, with commissioning structures that ensure better identification of review candidates, continuity of care and designated follow-up responsibilities; ideally from those with stroke-specific skills and training. Improving long-term care for stroke survivors and the provision of post-stroke six-month reviews has been prioritized by the NHS Long Term Plan 16 and NHS Commissioning for Quality and Innovation (CQUIN), 17 respectively, with publication of companion practical guidance to support implementation of reviews that readers may find useful. 18
Clinical messages
The modified Greater Manchester Stroke Assessment Tool is an acceptable toolkit, supporting delivery of a comprehensive needs assessment during six-month reviews with care home residents. An updated toolkit (GM-SAT2) is now available for reviews in all settings.
Stroke-specific knowledge and enhanced training would support a diverse range of professionals to deliver reviews.
Commissioning needs to provide additional resource for implementation of reviews and to ensure continuity of care when reviews highlight unmet needs requiring action.
Supplemental Material
GM-SAT_resub_to_CR_-_supplementary_RS – Supplemental material for Six-month reviews for stroke survivors: a study of the modified Greater Manchester Stroke Assessment Tool with care home residents
Supplemental material, GM-SAT_resub_to_CR_-_supplementary_RS for Six-month reviews for stroke survivors: a study of the modified Greater Manchester Stroke Assessment Tool with care home residents by Emma Patchwood, Kate Woodward-Nutt, Katy Rothwell, Catherine Perry, Pippa Tyrrell and Audrey Bowen in Clinical Rehabilitation
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: A.B.’s salary at the University of Manchester is partly funded by the Stroke Association and other NIHR grants. E.P.’s salary at the University of Manchester is fully funded by the Stroke Association.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.