
Abstract
Objective:
This systematic review aimed to investigate the effects of interventions intended for retraining leg somatosensory function on somatosensory impairment, and secondary outcomes of balance and gait, after stroke.
Data sources:
Databases searched from inception to 16 January 2019 included Cochrane Library, PubMed, MEDLINE, CINAHL, EMBASE, PEDro, PsycINFO, and Scopus. Reference lists of relevant publications were also manually searched.
Review methods:
All types of quantitative studies incorporating interventions that intended to improve somatosensory function in the leg post stroke were retrieved. The Quality Assessment Tool for Quantitative Studies was used for quality appraisal. Standardised mean differences were calculated and meta-analyses were performed using preconstructed Microsoft Excel spreadsheets.
Results:
The search yielded 16 studies, comprising 430 participants, using a diverse range of interventions. In total, 10 of the included studies were rated weak in quality, 6 were rated moderate, and none was rated strong. Study quality was predominantly affected by high risk of selection bias, lack of blinding, and the use of somatosensory measures that have not been psychometrically evaluated. A significant heterogeneous positive summary effect size (SES) was found for somatosensory outcomes (SES: 0.52; 95% confidence interval (CI): 0.04 to 1.01; I2 = 74.48%), which included joint position sense, light touch, and two-point discrimination. There was also a significant heterogeneous positive SES for Berg Balance Scale scores (SES: 0.62; 95% CI: 0.10 to 1.14; I2 = 59.05%). Gait SES, mainly of gait velocity, was not significant.
Conclusion:
This review suggests that interventions used for retraining leg somatosensory impairment after stroke significantly improved somatosensory function and balance but not gait.
Introduction
Somatosensory impairment is common after stroke, occurring in up to 89% of stroke survivors. 1 Proprioception and tactile somatosensation are more impaired in the leg than in the arm post stroke, 2 with the frequency increasing with increasing level of weakness and stroke severity.2,3 Leg somatosensory impairment also has a significant impact on independence in daily activities 3 and activity participation in stroke survivors, 4 as well as predicts longer hospital stays and lower frequency of home discharges. 5
Leg somatosensory impairment negatively influences balance and gait. Post-stroke plantar tactile deficits correlate with lower balance scores and greater postural sway in standing. 6 Tactile and proprioceptive feedback provide critical information about weight borne through the limb. 7 Accordingly, tactile and proprioceptive somatosensory deficits may hinder paretic limb load detection ability, potentially leading to reduced weight-bearing and contributing to balance impairment and falls post stroke. 8 Indeed, stroke survivors with somatosensory impairment have a higher falls incidence compared to those without somatosensory impairment. 3 In addition to reduced balance, impaired load detection may also contribute to gait asymmetry, particularly in the push-off phase. 8 In addition, leg proprioception influences variance in stride length, gait velocity, 9 and walking endurance in stroke survivors. 10 In fact, leg somatosensory impairment has been shown to be the third most important independent factor for reduced gait velocity in stroke survivors. 11
Two systematic reviews have previously investigated the effects of interventions for retraining somatosensory function after stroke.12,13 In the first review, published more than a decade ago, only four of the 14 included studies targeted the leg, 12 while the second only included studies of the arm. 13 Nevertheless, both reviews reported that there were insufficient data to determine the effectiveness of these interventions. A third systematic review evaluating the effectiveness of proprioceptive training 14 only included 16 studies with stroke-specific populations, of which only two specifically addressed the leg. From these three reviews, the effects of interventions for post-stroke leg somatosensory impairment remain unclear. In addition, the first review 12 was critiqued for including studies with participants without somatosensory impairment, and that did not report somatosensory outcomes. 15 Therefore, a targeted systematic review, addressing the limitations of previous reviews, is required to elucidate the effects of interventions for post-stroke leg somatosensory impairment.
It is of interest to clinicians and researchers to evaluate the effects of leg somatosensory retraining on factors that may ultimately influence activity and participation, as this could change practice. Therefore, this systematic review aimed to examine the effects of post-stroke leg somatosensory retraining on somatosensory impairment, balance, gait, motor impairment, and leg function.
Methods
A protocol was registered in the PROSPERO International Prospective Register of Systematic Reviews 16 (registration no. CRD42017058993) prior to commencement of this systematic review. The PRISMA guidelines 17 were utilised in the process and reporting of this review.
For the purpose of this review, the authors defined somatosensory function as the ability to detect, discriminate, and recognise body sensations. 18 Somatosensory modalities affected by stroke that have been previously reported were considered, including detection or localisation of tactile stimuli, proprioception or kinaesthesia, stereognosis or object recognition, pressure or weight discrimination, detection of vibration, texture discrimination, and two-point discrimination.3,13,18–21 Retraining of somatosensory function was defined as any interventions that addressed the remediation of the above-mentioned somatosensory modalities. Intervention methods included elements of education; repetitive practice and feedback in detecting, localising, discriminating, or recognising different sensory stimuli, pressure, or objects; proprioceptive training; and somatosensory stimulation.12,22,23
Electronic databases including Cochrane Library, PubMed, MEDLINE, CINAHL, EMBASE, PEDro, PsycINFO, and Scopus were searched to identify relevant publications, from inception to 16 January 2019. The search strategy (Supplemental Table S1) was developed in collaboration with a librarian by breaking down the review question into components: population, interventions, comparators, outcomes, and study design (PICOS). 24 Identification of key search terms was followed, using synonyms and variants of the search terms. The search strategy was trialled on several databases and adjusted accordingly to maximise the sensitivity of the search. Two reviewers (F.S.F.C., S.K.) independently screened titles and abstracts of the studies yielded from the searches to assess for eligibility. Full-text publications of potentially eligible studies were retrieved and further evaluated by the same two reviewers. In addition, reference lists of relevant publications, including available systematic reviews, the included studies, and narrative reviews, were manually searched for eligible articles.
Literature search was restricted to humans and adults (19 years and above), and only studies published in English were included. There were no restrictions to publication date and study setting. Studies were included if participants had leg somatosensory impairment following a stroke, with no restrictions to the stage (acute, subacute, or chronic), category (ischaemic or haemorrhagic), or anatomical location of stroke. All types of quantitative studies incorporating interventions that aimed to improve leg somatosensory function after stroke were included. Studies that did not measure somatosensory impairment or employed somatosensory stimulation that produced muscle contraction were excluded, as muscle contraction could have been a confounding factor. Other reasons for exclusion were studies evaluating assessment tools, observational studies not investigating outcome of interventions, descriptive studies, expert opinions, qualitative studies, systematic reviews, conference abstracts, and unpublished studies.
The primary outcome was somatosensory impairment. Secondary outcomes were balance, gait, motor impairment, and leg function. Any measure of somatosensory impairment was considered, including modality-specific measures (e.g. Semmes–Weinstein monofilaments), 25 global measures of sensation (e.g. Nottingham Sensory Assessment), 26 and sensory subscales of impairment-based measures (e.g. Fugl-Meyer Assessment (FMA)). 27
Data were extracted by one author (F.S.F.C.) using a purpose-designed spreadsheet. A second author (S.K.) checked the data for accuracy. The following data were extracted from each study: study information (author(s), year of publication, location of study, study design), participant baseline information (demographics and characteristics), details of training intervention and dosage, details of control conditions (if any), follow-up period (if any), adverse effects, primary and secondary outcomes, and study results. Missing information required for data analysis was requested from the study authors.
Each included study was assessed for quality using the Quality Assessment Tool for Quantitative Studies, 28 which is valid and reliable. 29 Two reviewers (F.C.F.S., S.K.) assessed the quality of the articles independently, and discrepancies were discussed until consensus was reached. The Quality Assessment Tool for Quantitative Studies Dictionary 30 was utilised to guide ratings. Assessment components were selection bias, study design, confounders, blinding, data collection methods, withdrawals and drop-outs, intervention integrity, and analyses. All components except intervention integrity and analyses were given a rating of strong, moderate, or weak. A global rating was awarded based on ratings of the six components – strong for no weak ratings, moderate for one weak rating, and weak for two or more weak ratings.
Descriptive analyses of the included studies were summarized. Effect sizes, pooled standard deviations (SDs), and P-values (two-tailed) of controlled clinical trials were calculated using a preconstructed Microsoft Excel spreadsheet called Effect Size Calculator. 31 Standardised mean difference (SMD) was used as the effect size to enable analysis of similar outcome measures with different scales. 32 Calculations for each study were based on post-intervention outcomes, at the latest time points, as recommended in the Cochrane handbook for systematic reviews of interventions. 33 Effect size bias was corrected using Hedges’ g, 34 from which the 95% confidence intervals (CIs) were derived. The null hypothesis was rejected if the P-value was less than 0.05. Heterogeneity between studies was assessed by calculating the I 2 statistic 35 using another preconstructed Microsoft Excel spreadsheet. 36 An I 2 value greater than 50% was considered of substantial heterogeneity. 35 A meta-analysis was conducted by pooling the Hedges’ g values to calculate the summary effect size (SES). 24 A random-effects model of meta-analysis was applied as it was expected that heterogeneity between studies would be relatively high. Subgroup analyses were conducted for studies using similar outcome measures. In studies that had more than one outcome measure using the same assessment tool within the same sample (e.g. light touch measured at multiple sites of the limb), a hierarchy of the preferred measure was set up a priori and only the SMD based on the measure highest on the list was calculated. 37 A narrative summary was provided for data not statistically analysed (e.g. studies without a control group or used a paired design, data not available, discrete data).
Results
A flow diagram of the study selection process is presented in Figure 1. A total of 16 studies were included at the end of the selection process.
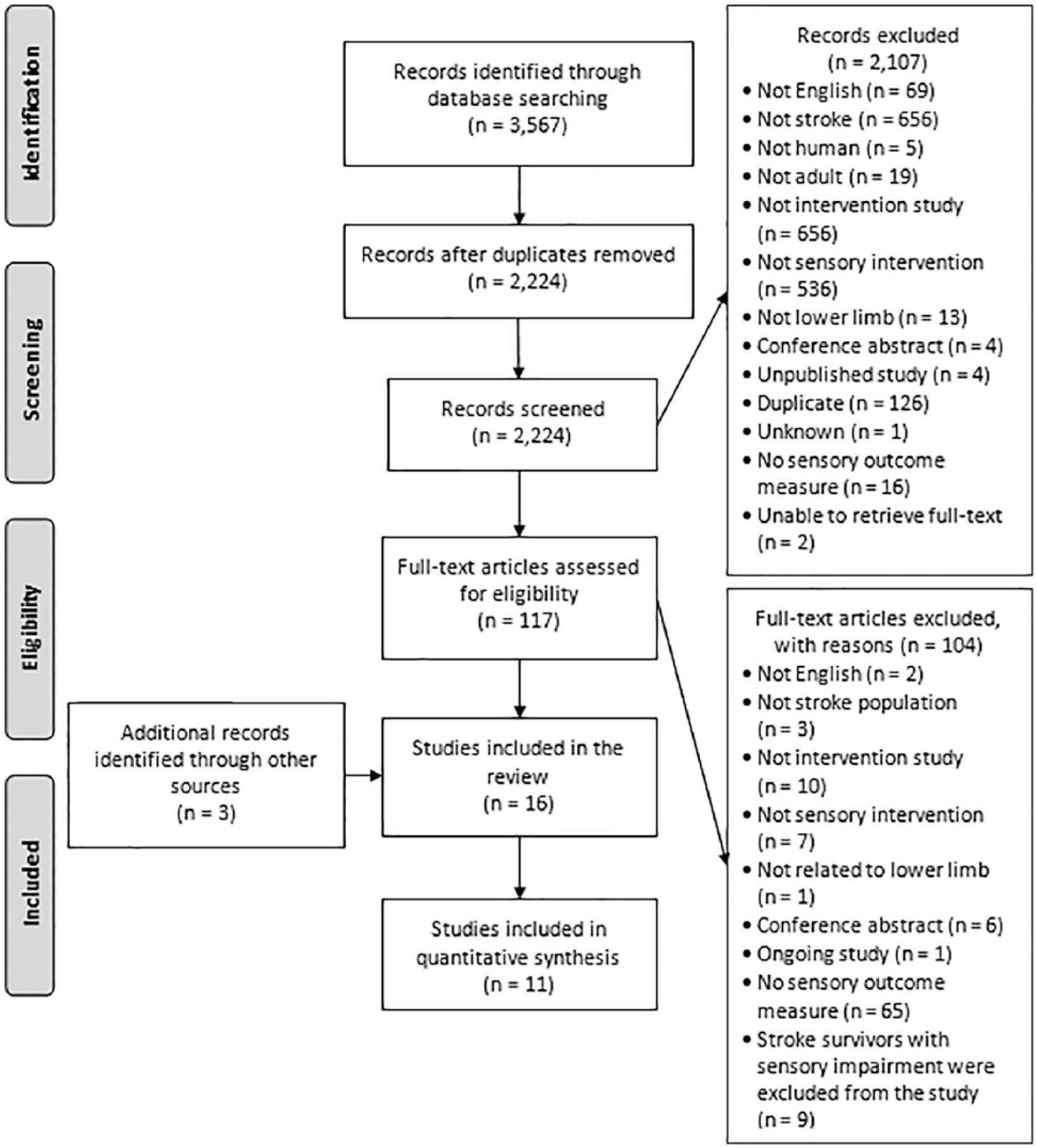
PRISMA flow diagram. 17
Description of included studies
Characteristics of the 16 included studies are displayed in Table 1. There were a total of 430 participants ranging in age from 18 to 82 years. Time since stroke ranged from seven days 38 to nearly 16 years. 39 Eight studies were set in inpatient rehabilitation,22,38,40–45 and the included studies were executed in nine different countries.
Characteristics of included studies.
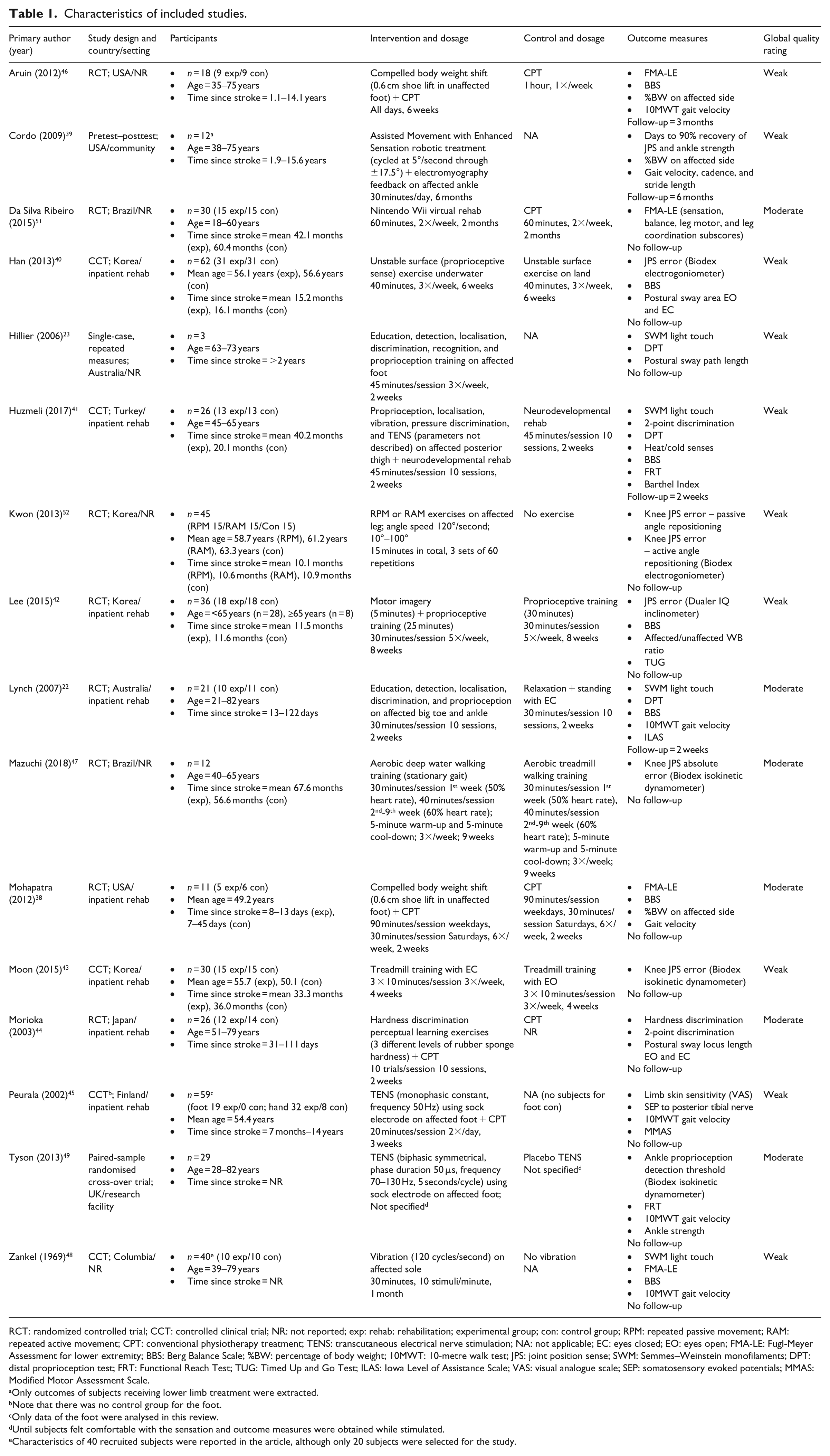
RCT: randomized controlled trial; CCT: controlled clinical trial; NR: not reported; exp: rehab: rehabilitation; experimental group; con: control group; RPM: repeated passive movement; RAM: repeated active movement; CPT: conventional physiotherapy treatment; TENS: transcutaneous electrical nerve stimulation; NA: not applicable; EC: eyes closed; EO: eyes open; FMA-LE: Fugl-Meyer Assessment for lower extremity; BBS: Berg Balance Scale; %BW: percentage of body weight; 10MWT: 10-metre walk test; JPS: joint position sense; SWM: Semmes–Weinstein monofilaments; DPT: distal proprioception test; FRT: Functional Reach Test; TUG: Timed Up and Go Test; ILAS: Iowa Level of Assistance Scale; VAS: visual analogue scale; SEP: somatosensory evoked potentials; MMAS: Modified Motor Assessment Scale.
Only outcomes of subjects receiving lower limb treatment were extracted.
Note that there was no control group for the foot.
Only data of the foot were analysed in this review.
Until subjects felt comfortable with the sensation and outcome measures were obtained while stimulated.
Characteristics of 40 recruited subjects were reported in the article, although only 20 subjects were selected for the study.
Three studies used a similar retraining approach, which included a combination of education, detection, localization, discrimination, recognition, and proprioception of the hemiparetic leg.22,23,41 There was a range of proprioceptive training strategies, including treadmill training with visual deprivation, 43 compelled body weight shift,38,46 and aquatic gait training. 47 Other interventions included vibration stimulation41,48 and transcutaneous electrical nerve stimulation (TENS).41,45,49 Intervention dosages ranged from a single dose lasting up to approximately two hours 49 to 30 minutes daily for six months. 39
Outcome measures used in the included studies are described in Table 1. Common somatosensory modalities were light touch, measured with Semmes–Weinstein monofilaments in three studies, and joint position sense (JPS), measured in five studies with the Biodex equipment, 50 and in three other studies with the distal proprioception test (DPT). The most common measure for balance was the Berg Balance Scale (BBS), used in five studies. Gait velocity was the main outcome measure for gait. Motor impairment measures included the modified Motor Assessment Scale and ankle strength. Leg function measures included Timed Up and Go (TUG), Barthel Index, and the Iowa Level of Assistance Scale.
Quality appraisal
A summary of the quality appraisal of included studies is presented in Supplemental Table S2. Of the 16 included studies, 10 were rated as weak and six rated as moderate. None of the studies had a strong rating. In the selection bias component, four studies scored somewhat likely to be representative of the target population,22,38,44,46 and none of the studies scored very likely, due to incomplete reporting of recruitment processes. A total of 14 studies were rated strong in study design for being controlled trials. However, only five of these trials described the randomisation method.22,44,47,49,51 The four studies that were rated as weak in the confounders component (i.e. confounders not accounted for) either did not provide sufficient information to ascertain whether or not there were important between-group baseline differences,23,46,48 or there were important differences that were unaccounted for including sex and age. 45 Only three studies had blinding of both outcome assessors and study participants.22,44,47 In total, 10 studies were rated as strong for data collection methods and one received a weak rating. 44 Five studies were rated separately for somatosensory measures and secondary outcomes due to the use of measures with a range of psychometric properties, all receiving a strong rating for balance or gait measures, and a weak rating for somatosensory measures.22,23,39,41,45 The majority of studies reported 80%–100% of participants completing the study and scored a strong rating in withdrawals and drop-outs. Only two studies reported percentage of compliance with treatment protocol,39,47 and only two of the randomised trials performed an intention-to-treat analysis.22,47
Intervention effects
Study results, calculated effect sizes, and CIs are summarised in Supplemental Table S3. Somatosensory outcomes, which included JPS, light touch, and two-point discrimination, showed a significant heterogeneous positive SES (SES: 0.52; 95% CI: 0.04 to 1.01; Figure 2). However, subgroup analyses of JPS (SES: 0.36; 95% CI: –0.25 to 0.96) and light touch (SES: 0.28; 95% CI: –0.86 to 1.41) were not significant. A significant heterogeneous positive SES was found for BBS scores (SES: 0.62; 95% CI: 0.10 to 1.14; Figure 3). SES of weight-bearing on the affected side was not significant (SES: 1.52; 95% CI: –1.71 to 4.74). There was an outlying data set in weight-bearing distribution on the affected side (Supplemental Table S3). A sensitivity analysis was conducted with the exclusion of this data set, and a consistently non-significant SES was found (SES: 1.09; 95% CI: –0.06 to 2.24). Gait velocity SES was not significant (SES: 0.42; 95% CI: –0.58 to 1.41; Figure 4).
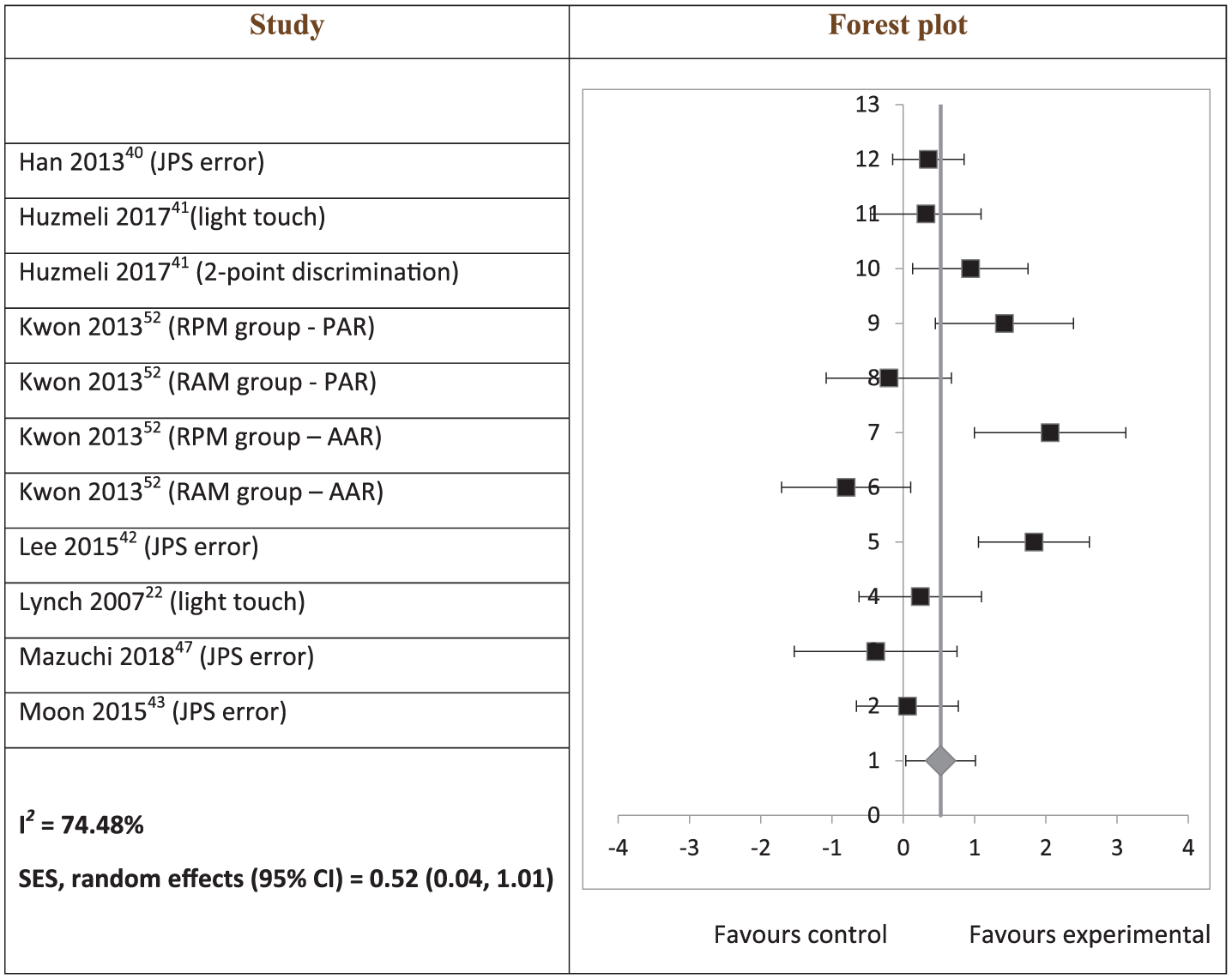
Hedges’ g (95% CI) and summary of effect size (95% CI) on somatosensory outcomes.
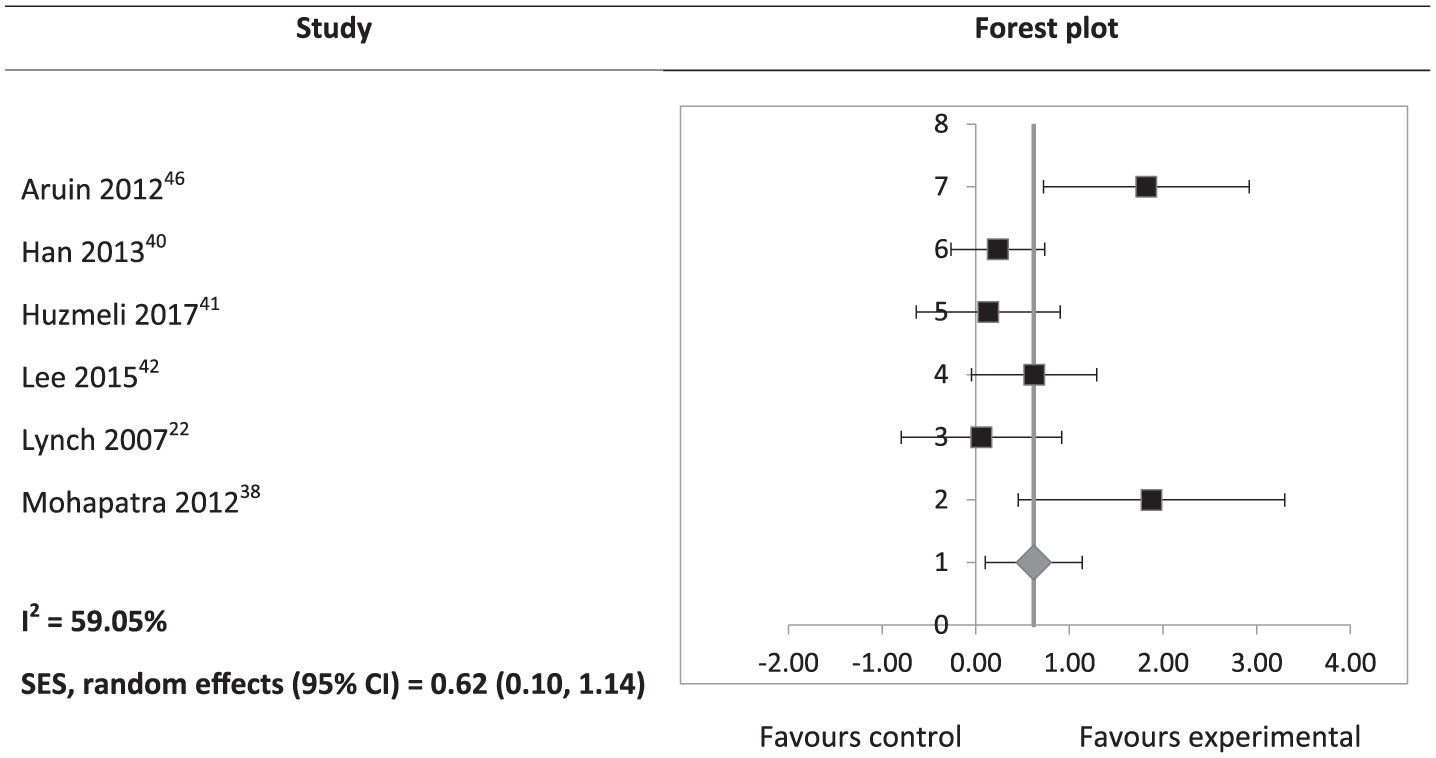
Hedges’ g (95% CI) and summary effect size (95% CI) on Berg Balance Scale scores.
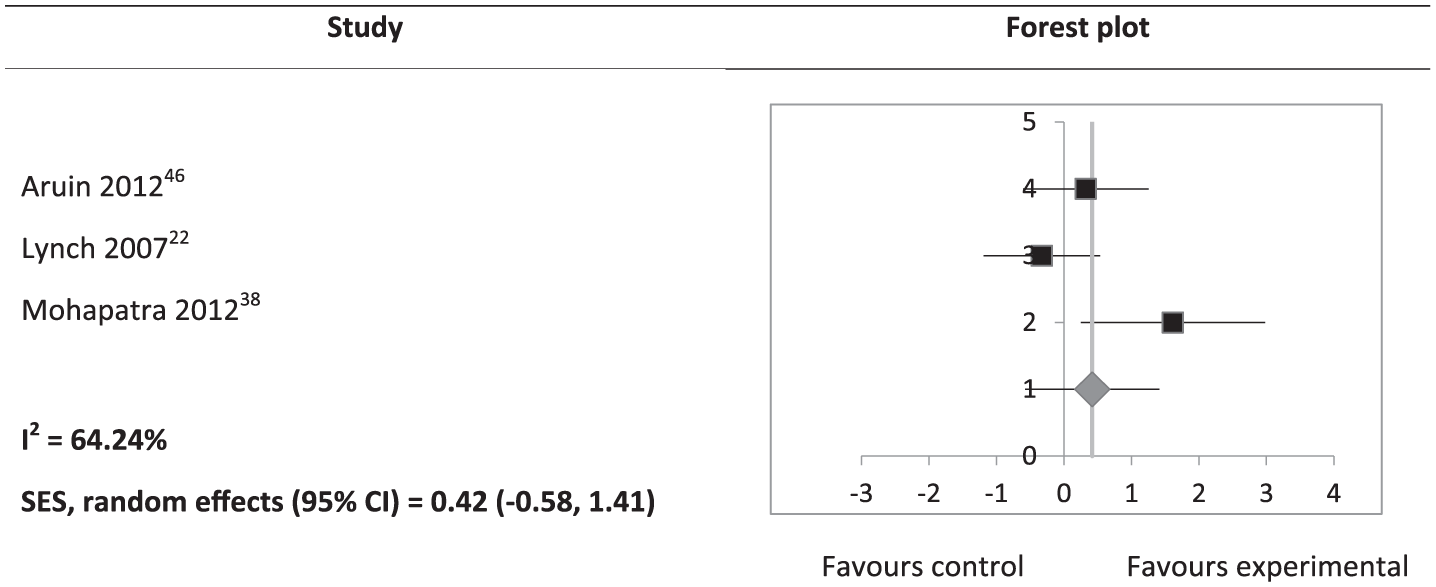
Hedges’ g (95% CI) and summary effect size (95% CI) on gait velocity.
High clinical heterogeneity and insufficient data prevented meaningful pooling of postural sway area, motor impairment, and leg function outcomes (Supplemental Table S3). Effect sizes of postural sway area, both eyes open and closed, were significant in one study, 40 but not significant in the other. 44 For results pertaining to motor impairment and leg function, only the Barthel Index effect size was significant (SMD: 1.07; 95% CI: 0.24 to 1.89; P = 0.01). 41 Non-significant findings included the FMA for lower extremity (P-values ranging from 0.13 to 0.61),38,46,51 Iowa Level of Assistance Scale (SMD: 0.00; 95% CI: –0.86 to 0.86; P = 1.00), 22 and TUG (SMD: 0.19; 95% CI: –0.46 to 0.85; P = 0.56). 42 Details of data synthesis are available from the corresponding author.
Data from five studies were not included in data synthesis due to having a cross-over design, 49 data being unavailable, 48 or having no control group.23,39,45 Non-significant findings were reported for two-point discrimination,41,44 vibration, 48 skin sensitivity, 45 and DPT.22,23,41 Significant improvements were reported for hardness discrimination, 44 configuration of somatosensory evoked potentials, 45 and in two out of three subjects for light touch. 23 The TENS cross-over trial reported significant improvement post intervention in ankle plantarflexion JPS and plantarflexor strength, but not ankle dorsiflexion JPS and dorsiflexor strength. 49 The assisted movement with enhanced sensation robotic therapy trial 39 reported that 100% of subjects had 10% or more improvement in ankle JPS, 73% of subjects had 10% or more improvement in ankle dorsiflexor strength, and 91% of subjects had 10% or more improvement in ankle plantarflexor strength post intervention. Significant improvements were reported in weight-bearing on the affected side 39 and Forward Reach Test 49 post intervention, and a downward trend over time in postural sway area. 23 A significant improvement in gait velocity was reported by two studies,39,49 but not significant in one study. 45
Adverse effects
Four studies addressed adverse effects.39,46,47,49 Two studies reported no adverse effects.46,47 Reported adverse effects were skin abrasion from self-over-treatment (one subject) 39 and one subject reported a day of pain post treatment. 49
Discussion
This review aimed to examine the effects of interventions for leg somatosensory impairment after stroke primarily on somatosensory impairment and secondarily on balance, gait, motor impairment, and leg function. Results of meta-analyses suggest that there is evidence that these interventions improve somatosensory function and balance, but not gait, outcomes. However, it may be premature to make firm conclusions about gait outcomes as pertinent variables other than gait velocity, such as gait symmetry, have not been assessed. The effects of these interventions on motor impairment and leg function remain unclear because pooling of data was not possible due to a high degree of clinical heterogeneity and insufficient data.
The findings in this review suggest that interventions for post-stroke leg somatosensory impairment improve somatosensory function. Meta-analysis of somatosensory function was limited to the proprioception (JPS error), light touch, and two-point discrimination modalities of the leg. Although JPS error subgroup analysis was not significant, all but one study 52 included in the analysis reported significant improvements post intervention. Although unlikely, it is possible that this one study 52 may have skewed the results due to their mixed findings: a significant decrease in JPS error in the repeated passive movement group and an increase in JPS error in the repeated active movement group. Studies that measured proprioception using the DPT, unable to be included in the subgroup analysis, reported no statistically significant improvement,22,23 although one of them reported clinical improvement. 23 This apparent lack of improvement was attributed to the lack of sensitivity of DPT.22,23 Light touch training effects appear ambiguous as there were inconsistent findings among the three included studies. One study reported between-group difference in only one (first metatarsal) of seven points of the foot, 22 one reported significant improvement in two out of three subjects, 23 and the third 41 showed a non-significant effect size. Two-point discrimination similarly demonstrated no improvement associated with retraining of somatosensory impairment, 44 although this may also be due to the lack of sensitivity of the instrument. 41 However, the overall positive findings support the incorporation of interventions for addressing leg somatosensory impairment in stroke rehabilitation. Specifically, the JPS modality may be a suitable starting point of retraining.
Results of this review also suggest that interventions for post-stroke leg somatosensory impairment improve balance. Although pooling was not possible for postural sway area and a non-significant finding was found for weight-bearing on the affected side, three of seven studies that reported these outcomes showed significant positive effect sizes.38,40,46 The remaining studies reported either significant improvements post intervention39,42,44 or a downward trend over time 23 (see Supplemental Table S3). A potential reason for improvement in balance, as a result of addressing leg somatosensory impairment, may be the improved perceptive ability through perceptual and motor learning, which is transferred to the motor performance of improved postural control. 44 Improvement in balance may in turn reduce falls risk in stroke survivors. This is especially important given the association between somatosensory impairment and a higher falls incidence in stroke survivors compared to those without somatosensory impairment. 3
There are a few possible reasons for the finding that interventions for post-stroke leg somatosensory impairment had no effect on gait outcomes. First, gait post stroke can be influenced not only by somatosensory information,11,53 but also by other factors including muscle strength,11,53–55 spasticity, 55 cognition, 56 visuospatial perception, 57 motor function,53,56 and balance.53,54 Changes to somatosensation alone may not be enough to influence gait. It may be necessary to retrain somatosensory function in conjunction with interventions that address these other factors. Second, the interventions in most of the studies included in this review may not have been applied in tasks specific to gait. There is strong evidence for effectiveness of task-specific training for recovery after stroke, 58 as a result of neuroplasticity. 59 The use of intensive gait-specific training has been recommended for improving gait ability after stroke.60,61 An example of gait-specific retraining of somatosensory function may be ankle proprioceptive discrimination throughout a gait cycle. Third, results may have been influenced by the small sample sizes and varying methodology of the included studies.
Only gait velocity was measured in the three studies included in the meta-analysis. Another variable pertaining to gait that could be considered in assessing treatment effectiveness is symmetry. 7 Gait symmetry can be measured using step length, or temporal measures such as stance or swing times. 62 It has been suggested that leg proprioceptive and tactile information provides critical feedback that is able to modify gait patterns, 7 potentially improving gait symmetry in stroke survivors. Improved somatosensory feedback can contribute to more accurate timing and amplitude of muscle contractions in response to the external environment,63,64 thereby improving gait symmetry. It is not possible to make the conclusion that retraining of leg somatosensory function would not affect gait at all, as none of the studies statistically analysed gait symmetry. One study assessed stride length and reported a significant within-group improvement, 39 but data were not included in the meta-analysis due to a lack of a control group. Gait symmetry should be assessed when evaluating effectiveness of leg somatosensory interventions in future trials.
Two previous systematic reviews12,13 that investigated the effects of interventions for somatosensory impairment in the stroke population, although not specific to the leg, reported that there had been insufficient evidence to determine their effects and highlighted the need for high-quality controlled trials. Results from this review suggest that although several additional controlled trials examining the effects of interventions for somatosensory impairment, particularly in the leg, have been undertaken in recent years, the quality of these recent trials either remains poor or is difficult to assess due to incomplete reporting. In view of this, future studies should adhere to reporting guidelines for transparent reporting, such as CONSORT for randomised trials 65 and TREND for non-randomised trials. 66 Contrary to these previous reviews, the medium summary effects of this review provide preliminary evidence to support retraining of somatosensory function in the leg after stroke, for improving somatosensory function and balance.
Quantifiable and precise somatosensory assessment measures are vital in order to diagnose impairment, evaluate the extent of impairment and treatment effectiveness, and facilitate clinical decision-making about outcomes being achieved. 67 The psychometric properties of many of the somatosensory outcome measures used in studies included in this review have not been established or were not reported in the studies, which is consistent with an observation about the dearth of literature examining frequently-used somatosensory assessment tools. 68 This had implications for quality ratings of the included studies. Several studies used a range of measures; some such as the timed 10-metre walk test 69 and the BBS 70 have demonstrated good psychometric properties,71,72 while others such as the DPT 73 have not had psychometric properties established. In order to provide a fair rating, five studies were given two different ratings: a strong rating for balance or gait measures and a weak rating for somatosensory measures.22,23,39,41,45 Furthermore, there are concerns raised about the lack of standardisation, responsiveness, and generalisability of somatosensory measures used in stroke rehabilitation. 68 For example, a study examining the psychometric properties of the sensory subscale of the Fugl-Meyer Assessment (FMA) found that the high ceiling effect, and poor to moderate reliability, validity, and responsiveness, did not support its clinical use in stroke rehabilitation. 74 The FMA was used in three of the included studies in this review.38,46,51 On a positive note, several leg proprioception assessment tools included in this review have been tested for their psychometrics, including electrogoniometers 75 and digital inclinometers.76,77 However, these tools have not been tested in the stroke population, and their usage in clinical settings remains limited. Future research should focus on establishing the psychometric properties of these tools in stroke rehabilitation. Development of leg somatosensory measures that are quantifiable, sensitive to change, and available for clinical use may also be required for assessing treatment effectiveness and enabling better quality trials in somatosensory rehabilitation.
There was a diverse range of interventions used in the studies included. This highlights a need for developing standardised retraining methods of leg somatosensory function that can be reliably replicated across trials and in clinical settings, to increase consistency of interventions. An approach for retraining of somatosensory function has been developed, 78 which has been demonstrated to be effective albeit only in arm studies.79–81 The approach is derived from theories of perceptual learning and somatosensory processing neurophysiology, and are consistent with the learning-dependent principles of neuroplasticity. 78 The key elements of the approach are task-based (goal-directed), guided attentive exploration with vision occluded, immediate and precise feedback, calibration (within and across different sensory modalities, e.g. other limb and vision), anticipation trials, repetition, graded progression, and transfer of training effects to novel stimuli. Further exploration regarding the application and effectiveness of these principles, particularly in the leg, may be beneficial in establishing a standardised approach to addressing somatosensory impairment.
Somatosensory information, both from the joint (proprioception) and from the skin (tactile), has been demonstrated to be associated with perception of verticality, 82 which in turn is related to balance. 83 It is possible that enhanced proprioceptive and tactile feedback contributes to a more accurate perception of verticality, thereby positively influencing balance. Furthermore, increased weight-bearing on the affected side has been found to be associated with a reduction in postural sway. 84 It was suggested that a reduction in postural sway could be due to enhancement of somatosensory information enabled by increased weight-bearing on that leg. 84 Based on this review’s meta-analysis, interventions aimed to improve somatosensory function did not appear to increase weight-bearing on the affected side. However, in two studies38,46 where interventions specifically targeted weight-bearing on the affected side, there were larger improvements of weight-bearing on the affected side in the experimental group compared to the control group. Further research into interventions aimed to increase weight-bearing on the affected side may be useful in clarifying its role in reduction of postural sway.
There are obvious strengths and limitations in this review. The main strength is the use of the PRISMA guidelines, 17 which enable transparent and complete reporting. One of the limitations is that the inclusion of non-randomised as well as randomised trials of varying quality permitted inclusion of a high risk of bias across studies. However, the reviewers wanted to report all available studies on post-stroke interventions that aimed to improve leg somatosensory function. All the included studies had small sample sizes with the highest being 62 participants. 40 These small sample sizes, plus the high risk of selection bias within studies as noted in quality appraisal, mean that outcomes from these studies may not be representative of the wider stroke population. In addition, interpretation of the results may have been influenced by the heterogeneity of interventions and outcomes included. A risk of publication bias also exists due to the exclusion of non-English publications and unpublished studies. 24 Nonetheless, the inclusion of non-English studies of randomised trials in systematic reviews found that language restrictions did not appear to bias results of conventional interventions. 85
Clinical messages
Interventions aimed at retraining leg somatosensory function post stroke are shown to be effective for improving somatosensory impairment and balance, but not gait.
Many of the somatosensory assessment tools used in the leg have not been tested for their validity and reliability in stroke rehabilitation.
There is a varied range of intervention methods intended for retraining leg somatosensory function after stroke.
Supplemental Material
Supplemental_Material – Supplemental material for Sensory retraining of the leg after stroke: systematic review and meta-analysis
Supplemental material, Supplemental_Material for Sensory retraining of the leg after stroke: systematic review and meta-analysis by Fenny SF Chia, Suzanne Kuys and Nancy Low Choy in Clinical Rehabilitation
Footnotes
Acknowledgements
We thank the authors of the included studies who responded to our requests for information.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.