
Abstract
Objective:
To review methods for measuring adherence to exercise or physical activity practice recommendations in the stroke population and evaluate measurement properties of identified tools.
Data sources:
Two systematic searches were conducted in eight databases (MEDLINE, CINAHL, PsycINFO, Cochrane Library of Systematic Reviews, Sports Discus, PEDro, PubMed and EMBASE). Phase 1 was conducted to identify measures. Phase 2 was conducted to identify studies investigating properties of these measures.
Review methods:
Phase 1 articles were selected if they were published in English, included participants with stroke, quantified adherence to exercise or physical activity recommendations, were patient or clinician reported, were defined and reproducible measures and included patients >18 years old. In phase 2, articles were included if they explored psychometric properties of the identified tools. Included articles were screened based on title/abstract and full-text review by two independent reviewers.
Results:
In phase 1, seven methods of adherence measurement were identified, including logbooks (n = 16), diaries (n = 18), ‘record of practice’ (n = 3), journals (n = 1), surveys (n = 2) and questionnaires (n = 4). One measurement tool was identified, the Physical Activity Scale for Individuals with Physical Disabilities (n = 4). In phase 2, no eligible studies were identified.
Conclusion:
There is not a consistent measure of adherence that is currently utilized. Diaries and logbooks are the most frequently utilized tools.
Introduction
Evidence demonstrates that higher doses of therapy are associated with better outcomes after stroke.1–3 However, providing high doses of therapy in practice is challenging and therapists face a number of barriers including limited resources and low tolerance among stroke survivors to participate in high-intensity therapy.4,5 Therapists are encouraged to establish independent practice outside of supervised therapy time as a way of increasing therapy dose. 3
The benefits of increasing therapy dose by prescribing independent practice, however, depend on adherence to the prescribed programme; studies suggest that adherence reduces over time. 6 Adherence has been defined as ‘the extent to which a person’s behaviour – taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a healthcare provider’. 7 Adherence to exercise programmes has been shown to be especially challenging after stroke, 8 with between 30% and 50% of patients ceasing their exercise programmes within the first year. 9
Measurement tools that quantify adherence to exercise programmes provide information for therapists about what the client is doing, in many cases, during times of the day when therapists are unable to observe the practice. Measurement of adherence can take various forms and there is no acknowledged gold standard. 10 Previous systematic reviews have assessed adherence to home-based rehabilitation, 11 self-reported measures of home-based rehabilitation, 12 patient or provider adherence questionnaires in physiotherapy 10 and measures assessing non-pharmacological self-management in musculoskeletal conditions. 13 These previous reviews have concluded that trials included largely self-developed questionnaires that lacked sufficient evidence of psychometric properties.10,12,13 However, to date, no review has summarized methods of measurement of adherence to exercise and physical activity recommendations in stroke.
It is important to use a method of measurement of adherence that is valid in the specific population, that is, the tool measures what it is supposed to measure. 14 Given the important role adherence plays in determining the efficacy of an intervention, the adherence measurement methods chosen should be guided by the specific patient diagnosis group and by evidence of their measurement properties when tested within this group.
With limited understanding of the best methods of measuring adherence (and associated psychometric properties of these methods) for the stroke population, the primary aim of this study was to identify adherence measurement methods used to quantify adherence to exercise and physical activity recommendations. The secondary aim was to report on the psychometric properties of the identified methods and synthesize findings to provide recommendations for both clinical and research use.
Method
This review was conducted in two parts. An initial search was conducted to identify adherence measurement methods to exercise or physical activity in the stroke population. Following this, a second search was conducted to identify studies investigating the psychometric properties of the methods identified in phase 1. This review is reported in accordance with the PRISMA guidelines. 15
Phase 1: identification of adherence measurement methods
A search in eight electronic databases (MEDLINE, CINAHL, PsycINFO, Cochrane Library of Systematic Reviews, Sports Discus, PEDro, PubMed and EMBASE) was conducted in July 2017 and updated in September 2018 to identify adherence measurement methods. The search strategy for MEDLINE is included in Supplemental Appendix 1. An equivalent search strategy was individualized for all other databases and no limits were placed on publication dates.
Studies were included if they were (1) published in English, (2) included participants diagnosed with stroke (or greater than 80% of study population was diagnosed with stroke), (3) quantified adherence to exercise or physical activity recommendations, (4) were patient or clinician reported measures, (5) were defined and replicable measures and (6) were tested in patients >18 years old. Studies were included if they were conducted in any therapeutic setting including inpatient, outpatient and community settings. Studies using objective tools (which are not patient or clinician reported) such as accelerometers were excluded. Conference abstracts which described eligible adherence measurement methods were included.
Once duplicates were removed, titles and abstracts of all identified studies were reviewed for inclusion by two independent reviewers and agreement achieved through discussion when needed. The same two reviewers screened the full-text articles for the inclusion and exclusion criteria. A third reviewer was available to resolve differences. Data extracted included the population that the tool had been used with, the setting the tool had been used in, the type of intervention it was measuring, whether it was patient or clinician administered and study and measurement-specific information.
Phase 2: properties of included adherence measurement methods
To identify the psychometric properties of included adherence measurement methods, a search in eight electronic databases (MEDLINE, CINAHL, PsycINFO, Cochrane Library of Systematic Reviews, Sports Discus, PEDro, PubMed and EMBASE) was conducted in February 2018 and updated in September 2018. The search strategy for MEDLINE is included in Supplemental Appendix 2. An equivalent search strategy was individualized for all other databases and no limits were placed on publication dates.
Studies were included if they (1) were published in English, (2) included participants diagnosed with stroke (or greater than 80% of study population was diagnosed with stroke) and (3) reported research investigating at least one psychometric property for an adherence measurement method identified in phase 1. The primary psychometric property of interest was validity.
Once duplicates were removed, titles and abstracts of all identified studies were reviewed for inclusion by two independent reviewers and agreement was checked. The same two reviewers screened the full-text articles for the inclusion and exclusion criteria. A third reviewer was available to resolve differences.
Papers identified in phase 1 were grouped according to the type of adherence measurement method used. For phase 2, we planned to assess measurement properties following the recommendations of the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN). 16
Results
The review process for both searches is shown in the flowchart (Figure 1). Phase 1 identified a total of 48 articles for inclusion in our review, which included seven different adherence measurement methods (several studies evaluated multiple tools). Phase 2 failed to identify any articles which identified the psychometric properties of included adherence measurement methods for inclusion in our review.
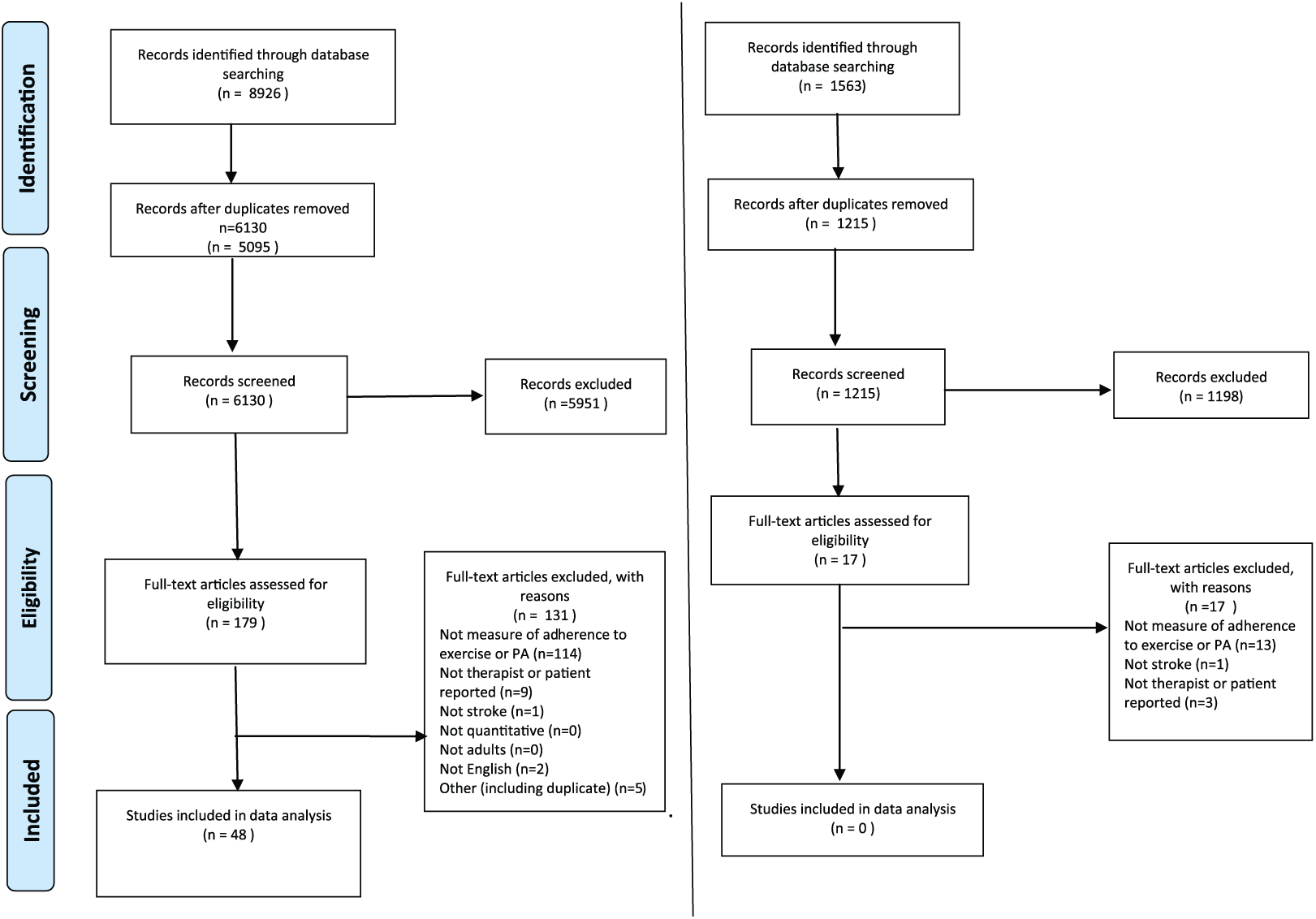
Flowchart showing selection process for phases 1 and 2. Phase 1 - identification of adherence measurement methods and phase 2 - measurement properties of adherence measurement methods.
Phase 1: identification of adherence measurement methods
A total of 6130 citations were identified using the search strategy; of these, 179 articles were selected for full-text review and 48 studies were identified as being eligible for inclusion. These 48 articles contained seven separate adherence measurement methods. Table 1 provides a summary of adherence measurement methods and study design. We found that researchers used different terms for their adherence measurement methods and there is no widely accepted terminology; we describe the adherence measurement methods based on the terminology used by the researcher within the study description. Supplemental Table 1 presents the method and characteristics of the included adherence measurement methods.
Types of adherence measurement method and type of study in which the method was used.
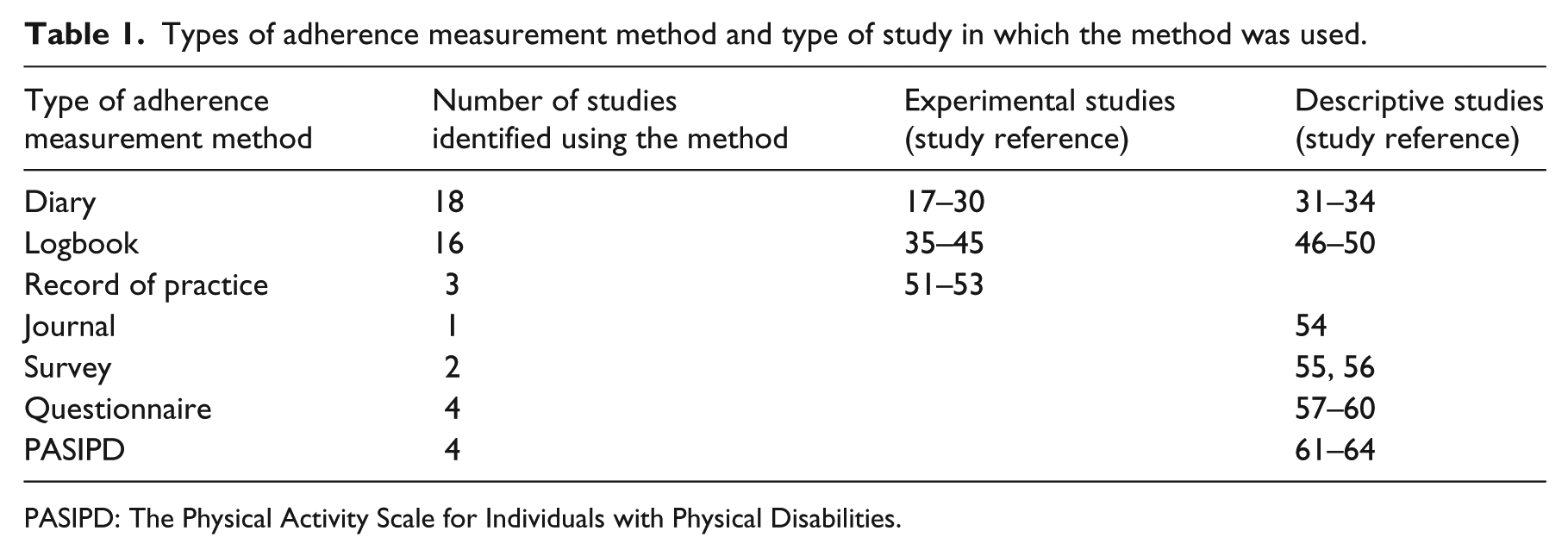
PASIPD: The Physical Activity Scale for Individuals with Physical Disabilities.
Of the adherence measurement methods identified, diaries and logbooks were used most frequently. Studies seldom described the content within the diaries/logbooks. Some studies identified the parameters of exercise or activity that were recorded. The duration and frequency of exercise or physical activity were most frequently recorded in the diary or logbook.
Diaries were used in 18 of the identified studies. All home diaries were completed by the patient. Three of the identified studies utilized diaries as a component of the constraint-induced movement therapy (CIMT), where the focus was on recording the amount of activity performed with the affected upper limb.17,31,32 Many of the included studies used diaries to record the duration or frequency of exercise or physical activity that was performed.18–28,31 The type of physical activity performed was included in the diary in seven studies.17,18,20,23,27,31,32 The specific method of recording in the diaries was not described in six of the identified studies.21,28–30,33,34
Logbooks or daily activity logs were used as adherence measurement methods in 16 of the included studies. Four of the studies used a log to record time of functional activity and/or adherence to mitt use during CIMT.35,36,46,47 A further study used a logbook to record type of activity performed during a goal-directed upper limb activity programme. 37 The most frequently recorded exercise or activity parameter was duration.35,36,38–40,46–50 Other parameters recorded in the logbooks included weekly step activity, 41 intensity 38 and number of sets and repetitions of exercise.42,49,50 Other studies did not provide any specific details regarding method of recording in the logbooks.43,44
Three of the included studies reported that subjects were asked to keep a ‘record of practice’ or recording sheet indicating how often they exercised.51–53 In the study reported by Malagoni et al., 52 participants were asked to fill out a daily training record indicating exercise completion and any adverse events. This record was then used by the authors to produce an adherence percentage (‘retention rate’), where the number of planned sessions relative to the recorded sessions was calculated. It was not clear whether this methodology was developed by the authors or based on previous research.
Hayward et al. 54 utilized a journal for recording adherence in their case study. Repetitions and a quality reflection were recorded.
This review identified a survey exploring exercise beliefs and adherence, originally developed by Miller. 65 The written exercise survey collected data including whether or not participants recalled being provided with a home exercise programme. For those that indicated a ‘yes’ response, data on adherence, non-adherence, reasons for non-adherence, perception of loss of function since discharge and exercise attitudes were collected. 55 This survey was developed after a literature review and was pilot tested and reviewed by experts in the field. The author acknowledged that a limitation of their study was a lack of information about the validity of the survey. An additional study included in this review used a phone survey to assess adherence; however, no details of the survey were available. 56
Four papers included in this review used questionnaires as adherence measurement methods. Jurkiewicz et al. 57 developed a 16-item questionnaire comprising questions about the type and amount of exercise performed, factors that motivated patients to participate and reasons why they missed their workout. Touillet et al. 58 described using a semi-structured activity questionnaire, which explored type of activity as well as duration and frequency. In a study exploring longitudinal patterns of adherence to exercises in people with stroke, Yao et al. 59 utilized the Questionnaire of Exercise Adherence, a 14-item questionnaire consisting of three dimensions: adherence to exercise, effective supervision and advice seeking. An additional study included in this review developed a questionnaire that examined consistency between prescribed treatment and exercises completed. 60
The Physical Activity Scale for Individuals with Physical Disabilities (PASIPD) was included in four papers identified in this review.61–64 The PASIPD is a 13-item self-report tool that assesses physical activity in three domains: recreation, household and occupational activities.
Phase 2: psychometric properties of included adherence measurement methods
The search for the second phase of this review, aimed at synthesizing the published psychometric properties of the adherence measurement methods, identified 1215 citations, and a total of 17 papers were sought in full text. Of these studies, none of the studies met all the inclusion criteria. Hence, analysis of the psychometric properties of the located adherence measurement methods was not possible.
Discussion
This review identified that while there are adherence measurement methods used to assess adherence to exercise or physical activity recommendations after stroke, there are no published psychometric studies of these tools. Seven adherence measurement methods have been described in the literature: diaries, logbooks, record of practice, journal, surveys, questionnaires and the PASIPD. There is no clear consensus on the optimal adherence measurement method to exercise or physical activity recommendations after stroke, since it remains plausible that existing approaches are not valid. The findings of this review are consistent with other reviews involving other populations, demonstrating that researchers tend to use tools that are developed and administered in an ad hoc manner, and existing measures have not been adequately psychometrically tested.10–13
Additional methods of monitoring were used in a number of other studies included in this review, including telephone monitoring and follow-up face-to-face meetings.17,22–28,40 In addition, Gunnes et al. 23 combined participant-reported diaries with an adherence form completed by the physiotherapist on review of the diary. The adherence form was intended as a method of quality assurance and was completed at regular review appointments. The author combined the two measures and expressed this as a single value representing adherence. Given that use of a diary or logbook is commonly used, determining the validity and reliability of these approaches seems to be an important area of future research.
While no studies met the inclusion criteria for phase 2 of the review, we excluded one study involving a coded physical activity diary. 66 This study was not included as it described patterns of physical activity rather than adherence to a prescribed programme. These types of coded diaries are frequently used in stroke research activity trials; each day is divided into time intervals and codes are provided that represent specific activities. Patients are asked to choose the primary activity performed over the time interval. It is hypothesized that this sort of diary use may be easier for stroke patients to comply with as it minimizes writing, but there is as yet not research to support this suggestion. Therapists may consider this method of diary use when aiming to measure stroke patients’ adherence to exercise programmes, but further research should be conducted prior to assuming that a diary of exercise represents actual exercise completed.
While participants were responsible for self-reporting in most studies, some studies also incorporated caregiver involvement into the recording process. Caregivers were required to either record the amount of exercise performed in the logbook or sign-off the completed exercises.38,45,48 Caregiver support may increase the consistent use of adherence measurement methods; however, consideration must be given to the demands and burden placed on the caregiver. Again, however, there were no published studies to determine whether caregivers are more or less accurate in their reporting of completed exercise and the role of caregivers in physical activity and exercise studies warrants further research.
Our review did locate one tool; the PASIPD is a 13-item self-report tool that captures physical activity in three domain areas (recreation, household and occupational activities). While we could not synthesize findings from psychometric studies completed specifically in a stroke population, the PASIPD has published reliability and validity coefficients (test–retest reliability .77; criterion validity correlation .3) when used for measuring physical activity in individuals with disabilities (mixed population).61,67 Thus, the PASIPD may be considered to be a tool for measuring physical activity in a population of people with disabilities. However, it was not designed to be a tool for measuring adherence, although it was used for this purpose in one study identified in this review. 62 To use the PASIPD as an adherence measurement method, Brown et al. 62 adapted the original assessment; however, it has not had psychometric evaluation for this purpose. Thus, further research to understand the validity and reliability of the PASIPD as an adherence measurement method is still required.
This systematic review was deliberately limited to identifying adherence measurement methods through methods of client or therapist report (and thus, we excluded approaches such as the use of accelerometers). We made this decision because there is already systematic review evidence for the role of accelerometry to monitor physical activity after stroke, concluding that accelerometers yield valid and reliable data about physical activity after stroke. 68 Despite this strong evidence, the uptake of accelerometers by clinicians to monitor activity remains limited 69 and there is anecdotal evidence that independent use by stroke survivors is difficult. Furthermore, the use of accelerometers does not allow the therapist to monitor specific components of adherence such as counting repetitions. It is therefore important for clinicians to have inexpensive, readily available, quick and reliable adherence measurement methods that they or their patient could administer to measure adherence. This review has identified that currently such a method does not exist in the stroke literature.
The majority of studies identified in this systematic review recruited community-dwelling participants who were capable of participating in an unsupervised exercise programme. Of the studies incorporating cognitive and communication function into their inclusion and exclusion criteria, participants were excluded if they had issues that would prevent them following instructions relating to the intervention or method of assessment, including a lack of ability to follow two-step commands or mild cognitive deficits. A number of studies reported a mini-mental state examination (MMSE) cut-off score indicative of mild cognitive impairment (MMSE 18–23).17,18,22,23,27,30–32,52,61,70 Thus, our findings also failed to identify adherence measurement methods that may be suited to a population with greater levels of disability.
As the adherence measurement methods identified in this review varied in terms of their format and detail, at this stage, it is not possible to recommend which is most likely to provide the most reliable and valid information in the stroke population. The most frequently used adherence measurement method identified in this review is the patient diary. The main limitation of this method is the possibility of inaccurate reporting with a bias towards over-reporting. 71 Exploration of some of the more advanced applications of diary use identified in this review, such as a coded diary and regular therapist review, warrants further investigation and validation.
Understanding adherence is a complex concept and there are a multitude of factors that may influence adherence in people with stroke. 72 First, the theories around behaviour change (such as the theory of planned behaviour) show that factors such as attitude, norms and control influence intention (and subsequently behaviour). 73 Second, work shows that the process of establishing new habits (such as completing a self-directed programme) varies considerably among individuals and new activities often take weeks to become routine. 74
The issue of bias was addressed in a small number of the included studies and must be considered in analysis. Studies that rely on patient self-report can be subject to many forms of bias including recall bias, optimism bias and social desirability response bias.75–78 Recall bias has been identified as a limiting factor in survey-based studies 65 and self-report instruments such as diaries were reported to be vulnerable to patient’s inaccuracies. 23
The findings of this review echo those conducted in other fields. A systematic review of exercise adherence in the musculoskeletal field concluded that the measures identified were unacceptable for use and highlighted the importance of the development and evaluation of appropriate measures. 79 The development of a validated measure of adherence to exercise or physical activity in people with stroke should be a priority to provide researchers and clinicians with a greater understanding of this important concept. 80
Limitations of this systematic review include possible bias as studies not published in English were not included. The grey literature was not searched in this systematic review which may be a further limitation. The greatest limitation, however, remains the lack of published psychometric studies testing whether or not the clinical tools used to monitor adherence to physical activity and exercise programmes for stroke survivors are sound.
There is a lack of a uniform method of measurement of adherence to exercise or physical activity recommendations in the stroke population.
This study has identified diaries and logbooks as the most frequently used adherence measurement methods; however, there is a lack of standardization between tools.
Supplemental Material
Supplemental material for A systematic review of measures of adherence to physical exercise recommendations in people with stroke
Supplemental material, Supplemental_Material for A systematic review of measures of adherence to physical exercise recommendations in people with stroke by Tamina Levy, Kate Laver, Maggie Killington, Natasha Lannin and Maria Crotty in Clinical Rehabilitation
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.