
Abstract
Objective:
To characterize how rehabilitation goals of older patients change over time and to explore professionals’ attitudes toward patient-centered goal-setting and their perspectives on rehabilitation goals.
Design:
Qualitative interview study.
Setting:
Three geriatric rehabilitation centers.
Subjects:
Ten patients (aged ⩾ 80), who had recently received inpatient geriatric rehabilitation, and seven professionals were purposively recruited.
Methods:
Semi-structured interviews. Patients were interviewed in the third or fourth week after discharge from inpatient rehabilitation, to reflect on their inpatient goals and to investigate long-term goals now that they were at home. A thematic analysis was performed.
Results:
During inpatient rehabilitation, participants’ main goals were regaining independence in self-care activities and going home. Post-discharge, patients were not at their baseline functioning level. Rehabilitation goals appeared to shift over time, and once at home, patients formulated more ambitious rehabilitation goals that were related to regaining full independence and being able to perform activities. Although professionals thought goal-setting together with the patient is important, they also stated that older individuals often are either unable to formulate goals or they set unrealistic ones. In addition, professionals indicated that goals have to be related to discharge criteria, such as performing basic self-care activities, and rehabilitation revolves around getting patients ready for discharge.
Conclusion:
During inpatient rehabilitation, patient goals are related to going home. After discharge, patients have ambitious goals, related to their premorbid functioning level. Rehabilitation services should distinguish between goals that are important while patients are inpatient and goals that are important after discharge.
Introduction
Although the goals of adults admitted with disability for rehabilitation have been studied, how goals change over time is unknown, as is whether the goals older people have as inpatients are similar to the goals they have when they are home again. Based on their health status, individual lifestyle, and environment, individuals have their own desired outcomes of the rehabilitation process, making goal-setting between professionals and patients essential for rehabilitation. 1 Because goals can be adapted to the patient’s needs and own definition of problems, they provide an important opportunity for patient-centered rehabilitation. 2 Such rehabilitation is of particular relevance for geriatric patients, who are characterized by their diversity in disability and complex health status due to aspects such as chronic medical conditions, polypharmacy, or premorbid disability.3,4
Several studies show that although most professionals try to have their patients participate in goal-setting, this effort is often not a part of their daily practice. For example, within stroke rehabilitation, professionals consider patient involvement in the goal-setting process as important, yet they tend to set goals based on their own assessment and the resources available. 5 To improve patient-centered goal-setting within geriatric rehabilitation, knowing what rehabilitation goals comprise from a patient perspective and how goals may change over time is important. Although some studies have investigated goal-setting together with the patient, they were mainly conducted within brain6–8 or stroke rehabilitation9–14 and provide insight into the goal-setting process rather than patient goals. One of the few studies that looked into geriatric rehabilitation goals from a patient perspective considered short-term goals within 24 hours after admission and found that patients’ most common goals were “going home” and “regaining independence in self-care.” Whether and how these goals change once they are attained and patients are discharged, however, remains unknown. 15
In this study, we used a qualitative approach to characterize how older patients’ rehabilitation goals change over time. Specifically, semi-structured interviews were held a few weeks after discharge from inpatient rehabilitation. Participants were invited to reflect on short-term rehabilitation goals they had while they were inpatients and to describe their long-term rehabilitation goals now that they were home. A secondary aim was to explore professionals’ attitudes toward patient-centered goal-setting and their perspectives on rehabilitation goals.
Methods
The study was conducted between March and June 2014 in three rehabilitation centers (Cordaan) in the Netherlands. The Medical Research Involving Human Subjects Act did not apply to this research project and therefore official approval by a Medical Ethics Research Committee was not required. At the time of admission, Cordaan initiates a rehabilitation plan with rehabilitation goals for each patient. However, no clear guidelines exist for whether these goals should be set according to a patient-centered approach, that is, together with the patient, or by the multidisciplinary team during team meetings. Further note that at the time of study, reforms had recently been implemented that allowed patients to continue with the rehabilitation process after discharge from inpatient rehabilitation. These reforms enabled rehabilitation nurses to conduct home visits post-discharge. During this study, professionals were learning to work with this new structure. We adhered the consolidated criteria for reporting qualitative research (COREQ) for improving the quality of reporting qualitative research (see Supplemental table). 16
Study design
To characterize how patient goals may change over time, and to gain a deeper insight into professionals’ attitudes toward patient-centered goal-setting and their perspectives on what rehabilitation goals comprise, a descriptive qualitative design was used, grounded in a phenomenological study approach.17–19 Phenomenology seeks to describe how individuals experience a specific phenomenon and how they interpret those experiences. We aimed to gain a deeper understanding of the essence of rehabilitation goals from a patient’s perspective and a professional’s perspective. A phenomenological method facilitates this reflection through gathering extensive narrative data from a small number of participants. 19
Patient recruitment
We did not aim for data saturation and purposively recruited 10 participants (aged ⩾ 80); that is, we selected participants according to criteria relevant for our research objective. 20 Because we aimed to gain insight into how rehabilitation goals change over time, we aimed to include participants who had made significant shifts in their functioning level. Therefore, we recruited participants who had experienced loss of functioning after acute hospitalization and who were subsequently admitted to geriatric rehabilitation for at least two weeks. During the rehabilitation process, patients’ functioning level had improved and they were discharged home to the community. To ensure patients were able to hold a conversation and to reflect on rehabilitation goals during inpatient rehabilitation, they were only recruited if they had no signs of cognitive impairment, as indicated in patients’ medical files, and if they were able to speak and understand Dutch. To approach eligible patients, R.v.S. joined transitional rehabilitation nurses during home visits, which was conducted within 48-hour post-discharge. All participants who were approached were willing to participate, and after verbal informed consent was obtained, R.v.S. came back in the third or fourth week post-discharge to conduct an interview.
Recruitment of professional staff
For one month, to familiarize herself with the working procedure of the rehabilitation teams, R.v.S. attended several multidisciplinary team meetings, spent a few days with physicians and other team members at the rehabilitation centers, and joined transitional rehabilitation nurses during their home visits. In the next two months, we approached seven professionals for participation, including a nursing physician, physiotherapist, nurse, two transitional rehabilitation nurses, and two occupational therapists. All professionals were willing to participate, and after verbal informed consent, the interviews were conducted.
Interviews with patients
For data gathering, we decided to conduct semi-structured interviews because they allow for a detailed and in-depth exploration of patient experiences.19,21 We used a semi-structured interview guide during the interviews, consisting of a list of topics. R.v.S., who is an experienced researcher with formal training in interview techniques, conducted all interviews and began with an introduction of the researcher and clarification of the research topic. Participants were then asked to introduce themselves. Participants were invited to share their experiences with the rehabilitation process and to answer several questions regarding their recovery experience. R.v.S. then asked participants to reflect on their rehabilitation goals while they were inpatients and to describe the goals they had now that they were back home. Also, we used probing questions for more information and allowed participants to reflect on and share their experiences freely. 21 Interviews took between two and three hours and were audiotaped and transcribed verbatim by R.v.S. At the end, R.v.S. verbally summarized and discussed the interview with participants to provide them with the opportunity to clarify or add more information. Goals patients formulated during the interviews were compared with goals the multidisciplinary team formulated in participants’ rehabilitation plan.
Interviews with professionals
To reflect on professionals’ experiences with goal-setting, R.v.S. conducted semi-structured interviews with professionals. These interviews also began with a brief introduction of the researcher and clarification of the research topic. Professionals were asked to introduce themselves and to describe their jobs and were then invited to share their experiences with patient-centered goal-setting and to share their perspective on patient goals. Interviews took approximately one hour and were audiotaped and transcribed verbatim by R.v.S. A member check was conducted: a written summary was sent afterward, and the professionals were asked whether their perspective was correctly interpreted.
Data analysis
Thematic analysis was performed to identify, analyze, and report patterns in the data during six phases. 22 Note this analysis was an iterative process, which was conducted separately for the interviews with patients and with professionals. Data analysis was primarily performed by R.v.S. A senior researcher (S.M.S.) and professor (B.M.B.) in geriatric care provided supervision during all phases of data analysis, and R.v.S. discussed the results of each phase with S.M.S. and B.M.B. to ensure reliability and integrity of the data. First, R.v.S. read and re-read each transcript to become familiar with the data. Second, initial themes were identified using an open-coding approach, and all relevant topics were coded while reading through the transcripts. Third, the identified sub-themes were grouped into essential themes based on similarities, and connections were made between the different sub-themes and themes that derived through open coding. Fourth, by reviewing the themes in relation to the coded extracts and the entire data set, it was decided whether the identified themes and sub-themes had enough data to support them and which had to be removed. Fifth, the research team thoroughly discussed the themes and sub-themes and agreed on the final coding structure. R.v.S. then re-coded all interviews according to the final coding structure. During the sixth phase, quotes were labeled with relevant codes and translated into English.
Results
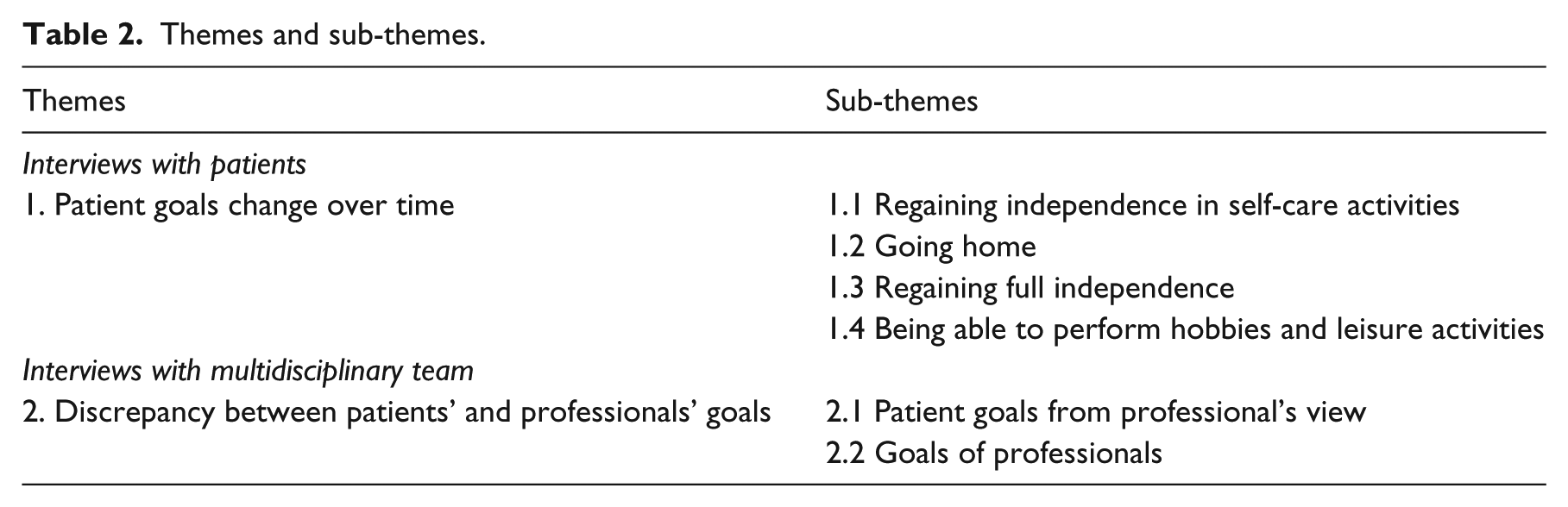
Two essential themes emerged from the data. The first theme describes how, related to patients’ functioning level, patient goals change over time. From the interviews with professionals, a possible discrepancy appeared between patients’ and professionals’ goals, which emerged as a second theme from the data. The themes and sub-themes are shown in Table 2 and described in the following paragraphs, using quotations that capture the essence of participants’ and professionals’ experiences.
Theme 1: Patient goals change over time
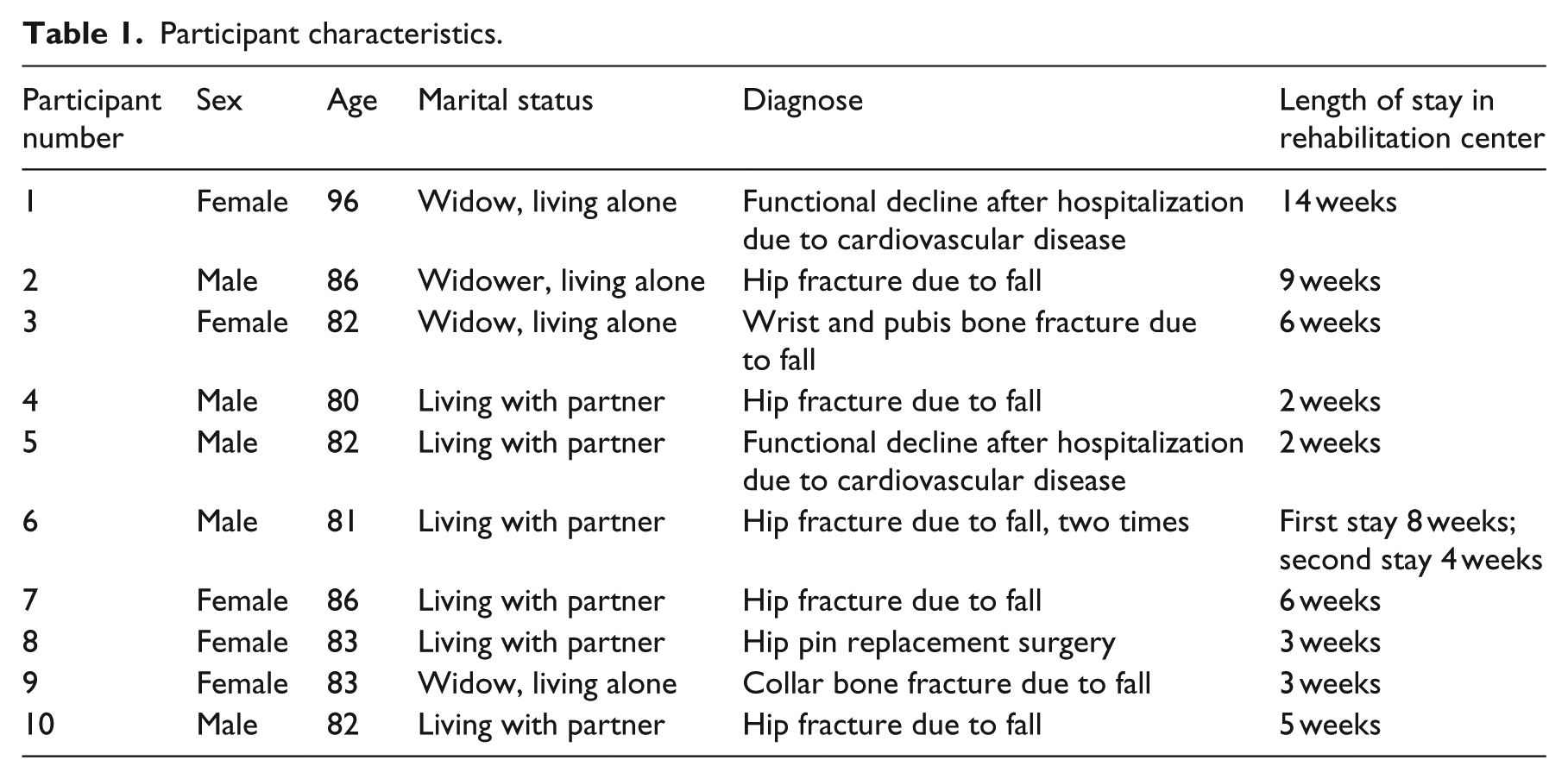
All 10 participants (mean age 85, Table 1) indicated they were independent and active before they were acutely hospitalized. Due to the acute health event, for example, a hip fracture, all participants experienced functional decline and, as participants described, at the start of inpatient rehabilitation, their level of functioning differed drastically from their premorbid level of functioning. For example, one participant stated, Before that time, I could do everything. Well not literally, but I was able to take care of myself. Everyone always told me they admired me for what I was capable of. But after those two weeks at the hospital, I couldn’t do anything anymore. (Participant 1, female (96))
Participant characteristics.
As participants became independent, during inpatient rehabilitation, their main goals were primarily related to regaining independence in self-care activities and going home.
Although their functional level had improved during inpatient rehabilitation, all participants were not at their baseline functioning level at the time of interviews, that is, three or four weeks after discharge. They all encountered difficulties in daily life and were unable to perform activities as they were used to. Rehabilitation goals appeared to shift over time, and once at home, participants formulated more difficult rehabilitation goals than the goals they had at the start of inpatient rehabilitation (Table 2).
Themes and sub-themes.
Sub-theme 1.1: Regaining independence in self-care activities (inpatient rehabilitation goal)
All participants became dependent on at least two basic activities of daily living (ADL) after hospitalization and mainly needed help with bathing, dressing, and toileting at the start of the rehabilitation process. Also, the vast majority were barely able to walk. All participants expressed that at the start of the rehabilitation process, their goal was to regain their independence: I wanted to be independent as soon as possible. And I worked on that from the start. After five, six weeks of calling for the nurse when I had to go to the toilet, I was fed up with it. I wanted to do it on my own. […] It was difficult but now I can do it again. (Participant 2, male (86))
Overall, participants felt like geriatric rehabilitation helped them resume their independence in basic ADLs.
Sub-theme 1.2: Going home (inpatient rehabilitation goal)
Besides being able to perform ADLs, participants indicated their goal was to go home as soon as possible. Many participants felt frustrated that they were admitted to the rehabilitation center because they were dependent on others and were unable to make their own decisions: “At one point you’re just sick of it. You are sick of being there. You are not able to pick your own food, to cook for yourself … you are dependent from help of others …” (Participant 7, female (87)).
Some of the participants also mentioned they did not feel like they were in the right place. They felt like other patients were in a worse situation, and participants could not identify themselves with these other older patients. For example, one participant stated, “You sit around the table with people in a much worse situation than I was. And because these people were in this bad condition I thought by myself, what exactly am I doing here?” (Participant 5, male (82)).
Because participants wanted to go home, the vast majority indicated they were extremely motivated during the rehabilitation process: My health condition started to improve because I do have quite some perseverance. All I could think of was going home. Every time I left physiotherapy, I said I want to and I can. They always had to laugh when I said that. (Participant 1, female (96))
During the interviews, some participants indicated that although their goal during inpatient rehabilitation was to go home, they wished they could have stayed longer at the rehabilitation center. In fact, a few participants indicated the time they had for inpatient rehabilitation was quite short, which was, according to one of the participants, made clear at the start of the rehabilitation process: “The second day I got there, the doctor came to me and said we work hard to get you home as soon as possible. I thought to myself, I just got here!” (Participant 9, female (82)).
A few participants stated they would have preferred to stay longer. One participant mentioned he went home at the moment he felt like he was starting to make progress, and another participant stated, “I was only allowed to stay there very shortly. So, I had to leave, even though I wanted to improve and regain my previous level of functioning” (Participant 7, female (86)).
Sub-theme 1.3: Regaining full independence (long-term rehabilitation goal)
Once participants were able to perform basic ADL activities, they were discharged to go home. Yet being at home was not so easy for them. Participants described encountering difficulties in daily life, and some participants were still unable to perform basic ADL activities such as bathing. In fact, all participants were unable to perform instrumental activities of daily living (IADL), such as grocery shopping or performing household tasks. For example, one of the participants said, I’m reluctant to do the smallest things. […] things you usually did without even thinking. Like making coffee or tea. Gosh, you keep walking back and forth in the kitchen. […] I did everything by myself, dusting the furniture and watering plants on my balcony. I cleaned the bathroom, but now I just can’t do that. And don’t ask me why, because I don’t know. (Participant 1, female (96))
Consequently, participants were more dependent on the help of others, and regaining full independence was a goal for every participant. They expressed how they felt like they had “lost control over their lives” now that they were receiving more help than they were used to. Although participants indicated they appreciated the help they got, they felt like they were not able to make their own decisions. For example, one participant stated, It is a life with limitations now. I feel like I lost control over my own life. There are a lot of people near me with all the best intentions. And, of course, I appreciate it, but they try to put you in a certain direction. (Participant 5, male (82))
For example, with regard to grocery shopping, being unable to get their own groceries could be annoying for participants: They asked me if I needed any groceries, so I asked for eggs and tea. But they came back with 30 eggs! And tea to make a pot of tea. I want tea to make one cup. Thanks a lot, and I appreciate it that you got it for me, but what do I need 30 eggs for? I started giving them away! (Participant 9, female (83))
Both statements reflect how participants felt like they had lost control over their lives now that they were so dependent on the help of others. Also, from their stories, patients appeared to have experienced disappointment with regard to their level of functioning after discharge, and they hoped their functioning level would improve. One of the participants expressed his frustration by describing what he was capable of before: I did everything! […] I’ve got a huge garden and an old house, so I was taking care of both. Well, of course! […] I also took my bicycle for a ride now and then. Well, yes, I did everything! Everything! (Participant 6, male (82))
Sub-theme 1
4: Being able to perform hobbies and leisure activities (long-term rehabilitation goal).
In addition to difficulties with ADL and IADL activities, all participants indicated they were not able to perform their hobbies and leisure activities like they used to. Before participants were hospitalized, they went to church, volunteered, took care of their gardens, took senior gym classes, or participated in hobby clubs and activities at their senior apartment. At home, participants were not able to perform these activities, and because they missed doing them, their goal was to perform them again. For example, one participant stated, I am a Jehovah’s Witness and I always practiced door-to-door evangelism. I used to do that for 70 hours a month, and that went very well actually. But now I miss doing that, you know? I hope it will get better soon, because having a curved back while standing at peoples’ door is embarrassing! (Participant 9, female (83))
In addition to performing leisure activities close to home again, many participants also expressed their goal to travel again to friends or family. For example, three participants used to drive to their friends and family, and other participants indicated traveling through the country by train again as goal. Also, some participants stated that they hoped to go on a holiday abroad again: I am planning to go to Switzerland in June. […] I want to do some mountain hiking, but you can’t get at those forest trails with your walker. So I want to get there with my alpenstocks. I mean no long tours or anything but some short mountain trails. I aim to achieve that; that’s my goal. (Participant 7, female (86))
This quote captures many of participants’ perspectives, showing that they still set ambitious goals for themselves. Despite their old age and significant loss of functioning, participants expressed that they hoped their functioning level would improve. Not being able to do the things they wanted to do could be quite frustrating: “Well when I think about it, I want to do everything of course. Because inside my head I can do anything, you know. However, my body refuses” (Participant 1, female (96)).
Theme 2: Discrepancy between patients’ and professionals’ goals
Based on the interviews, professionals apparently had difficulty setting goals with their patients. This difficulty seems to have been caused by a discrepancy between patient goals and rehabilitation goals from a professional’s perspective. Professionals explained that patients often do not set goals, or they set goals that are too ambitious. In addition, professionals’ goals were mainly related to discharge criteria, and as they explained, they were not able to take into account patients’ long-term goals.
Despite these difficulties, professionals did say that providing a patient-centered rehabilitation process and setting rehabilitation goals together with the patient were important to them. For example, a nurse stated, I think the team is willing to consider the perspective of the patient. I notice my colleagues really work in the best interest of their patients. […] In that way, it makes more sense why you are doing certain things, because you know why you are helping them then.
Also, participants mentioned that once you ask patients to set goals, you gain insight into issues you would not have thought of as a professional. One of the occupational therapists explained, One patient told me she would like to pet her dog again. […] I never thought she would say that and I think, when a patient tells you she wants to pet her dog again, it should be written down in her rehabilitation plan so she feels like she has been listened to.
The occupational therapists mentioned that using a goal-setting instrument when they set goals together with patients could be helpful, and they were familiar with the Canadian Occupational Performance Measure (COPM). However, they did not perform the COPM often. According to the therapists, they encountered time-related issues and difficulties with scoring when using the COPM, and they thought the COPM was often too difficult for older patients to perform at the start of the rehabilitation process.
Sub-theme 2.1: Patient goals from a professional’s perspective
Based on the interviews, professionals often feel as though older individuals no longer have goals, because of their old age. For example, one of the transitional rehabilitation nurses said, “I think older patients do not set goals for themselves anymore. People are happy being home, drinking coffee, and watching television. Perhaps people just stop setting goals at a certain age.”
Also, according to professionals, patients are not able to indicate what they want or need, because they do not know what to expect. Another transitional rehabilitation nurse said, What I notice is that patients are almost never able to tell me what kind of goals they have. […] They have no expectations and seem satisfied. I can say it for them, which I previously did, and they politely agree with me, but that is not how it should go.
On the other hand, however, professionals stated that patients often want to achieve unrealistic things: “One patient wanted to walk a trail of almost 200 kilometers; I think that is way too ambitious” (Transitional rehabilitation nurse).
According to the professionals, they often have to alter such goals to make them more realistic.
Sub-theme 2.2: Goals of professionals
Professionals expressed that rehabilitation revolves around getting patients ready for discharge as soon as possible, and therefore, rehabilitation goals need to be discharge-related. Subsequently, rehabilitation goals are formulated from a professional’s perspective, as explained by one of the occupational therapists: Honestly, we are focusing on getting people at home as soon as possible. […] When goals are not related to discharge, we cannot take them into account. […] You end up with goals that are not always patient goals, but they are essential, such as going to the toilet.
Even though professionals aim to hear rehabilitation goals from patients themselves, professionals appear to point them in a certain direction: I always ask patients what they need in order to get home. Most of the time patients start very vague. They say I want everything or, for example, grocery shopping. I try to limit that by asking: What do you need to go home […]? Eventually, you get to things like walking with crutches, making transfers, or going to the toilet. (Physiotherapist)
So even though professionals ask patients about their goals, getting people home as soon as possible is the main focus during rehabilitation. In fact, the physiotherapist further explained, I already have in mind which goals need to be attained before discharge at the moment the patient enters the room. However, I want to hear it from the patient him- or herself. They have to indicate their discharge goals. So I try to point them in the right direction, and eventually they will tell.
Two transitional rehabilitation nurses who recently started to conduct home visits after discharge from inpatient rehabilitation explained that they noticed now that participants often formulate new rehabilitation goals once they are at home. These nurses indicated that patients are not often aware of these goals during inpatient rehabilitation: “What I notice now that we visit patients at home is that when you still treat people at home, patients formulate new goals. For example, one patient told me that suddenly he became afraid of travelling by tram.”
However, the transitional rehabilitation nurses further explained that they pay a home visit to review patients’ medication and health status, and they actually cannot help patients attain rehabilitation goals once they are at home. Long-term goals or newly formulated goals post-discharge are hence not formulated in patients’ rehabilitation plan: “I often see that goals are insufficiently formulated in patients’ rehabilitation plan. For example, this morning I visited a patient and the only goal that was formulated in his rehabilitation plan was receiving home care for his compression stockings!”
This statement, expressed by one of the transitional rehabilitation nurses, illustrates how patients’ rehabilitation goals are formulated in their rehabilitation plan. Goals are mostly related to going back home or being able to perform ADL activities, and long-term rehabilitation goals are often not formulated in patients’ rehabilitation plan. Table 3 compares the long-term goals formulated by participants during the interviews and the goals formulated by professionals in their rehabilitation plan.
Most important rehabilitation goals according to the participants post inpatient rehabilitation and rehabilitation goals in participant’s rehabilitation plan.
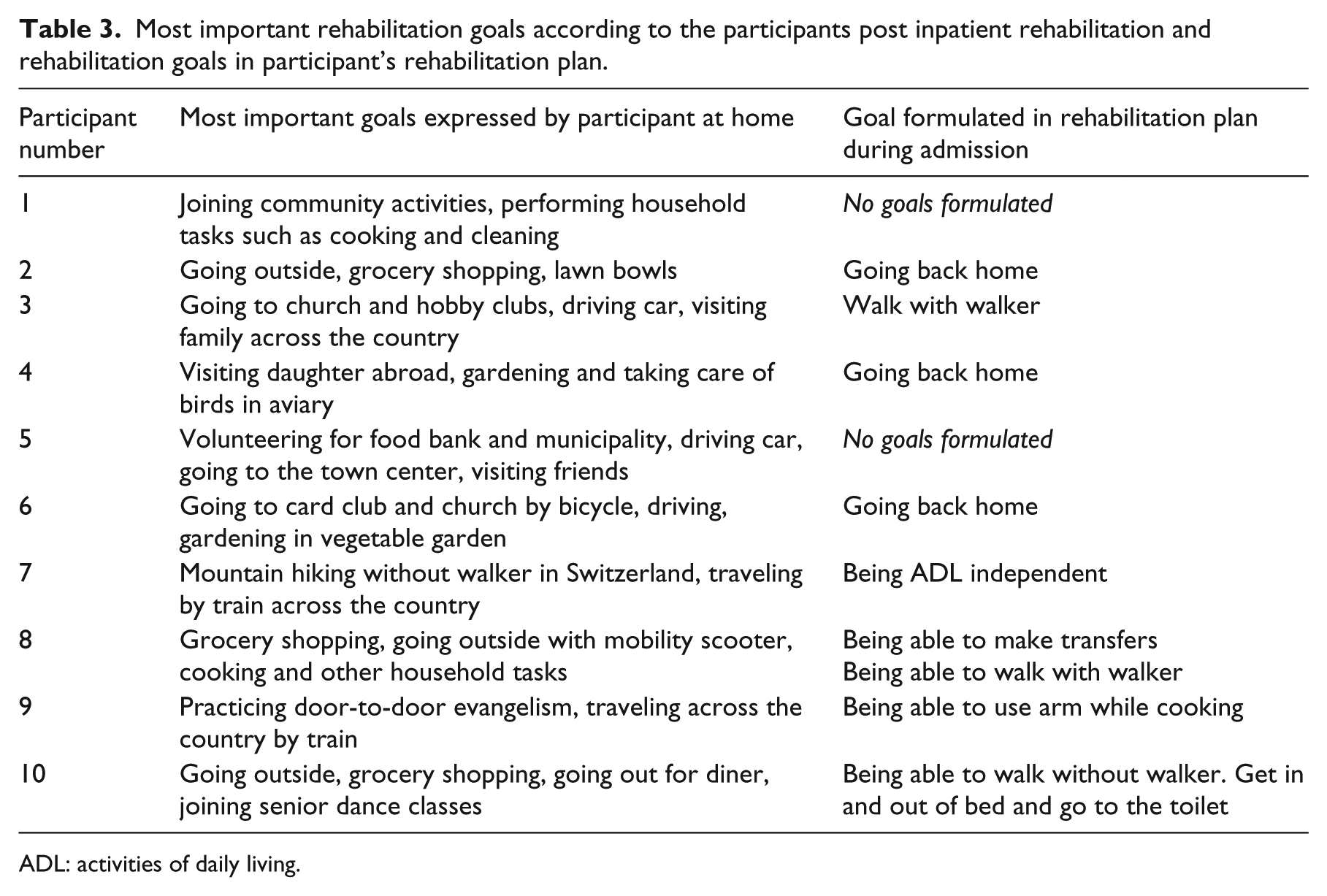
ADL: activities of daily living.
Discussion
This qualitative study showed that during inpatient geriatric rehabilitation, patient goals are related to regaining independence in self-care activities and going home. Post-discharge, patients are not at their baseline level of functioning, resulting in several ambitious long-term goals. With regard to the working method of the multidisciplinary team, professionals seem to think providing a client-centered goal-setting process is important. However, according to the professionals, during inpatient rehabilitation, older individuals are often unable to formulate goals, or they set unrealistic goals. Importantly, the rehabilitation process revolves around getting patients ready for discharge, resulting in goals that are related to discharge, for example, being able to perform basic self-care activities.
The finding that patients aim to regain independence and want to go home is supported by Kus et al., 15 who found that within 24 hours of being admitted, geriatric rehabilitation patients most often mentioned going home and regaining independence in self-care as their primary goals. The current study also thoroughly investigated patient goals in the longer term, and in a geriatric stroke rehabilitation setting, similar results were found: 10 participants’ main goals were to be physically active, travel, and visit family again. In this study as well, however, patients were discharged when they were able to go home rather than when they had attained their long-term goals. This discrepancy between patients and professionals regarding recovery has also been described in other stroke rehabilitation settings; 5 whereas professionals looked at recovery from the moment when patients were hit by a stroke and focused on, for example, independence in ADLs, patients wished to return to their pre-stroke status.
A possible explanation for the lack of patient-centered goal-setting in this study is that goal-setting can be difficult,8,23,24 particularly when concerning geriatric patients. 25 Therefore, to define and agree on patient goals, the goal-setting process might improve through the use of a goal-setting instrument. In this study, the occupational therapists were familiar with the COPM, 26 yet patients encountered difficulties regarding its scoring procedure. A complementary instrument could be Goal-Attainment Scaling (GAS), 27 which is particularly appropriate for assessing goal-attainment within geriatric rehabilitation, considering its excellent responsiveness to change. 28 Also, training and education might help professionals learn how to apply goal-setting instruments properly.5,29 When administered correctly, goals can eventually help develop a structured and more efficient rehabilitation process, because they can provide guidance and motivation for the interventions that will be undertaken during the rehabilitation process. 29 Hence, GAS should be administered at the start of inpatient rehabilitation, and again post-discharge, to evaluate whether inpatient goals are attained and to set new long-term goals together with the patient once he or she returns home.
In our study, professionals indicated that inpatient rehabilitation centers on getting patients ready for discharge, and goals are subsequently related to discharge criteria. Given the economic situation of healthcare providers and the current focus on cost reductions, this finding is not surprising. Although the Dutch government stimulates older individuals to live independently longer in order to prevent rising healthcare costs, 30 rehabilitation periods are as short as possible, and professionals are forced to provide rehabilitation with the resources available. However, taking into account the hazardous effect of functional decline is still important: individuals who have experienced functional decline are at risk of developing persistent disability 31 and are susceptible to hospital readmission 32 and nursing home admission. 33 Evidently, older individuals point out that the loss of the ability to live independently in the community is the most important threat to their quality of life after having experienced functional decline. 34 This finding underscores the need to address long-term goals that are important for patients to achieve once they are home.
During this study, the Dutch government had recently implemented reforms that made providing outpatient (i.e. home) rehabilitation after inpatient rehabilitation possible. Home rehabilitation might be an important and more affordable opportunity for long-term goal attainment and full recovery: several studies have shown the cost-effectiveness of home rehabilitation programs,35–37 and, importantly, the positive effect on functioning outcomes.38–40 Because individuals are in their own environment, a rehabilitation approach can be provided that is adjusted to their individual activities and specific daily needs, 41 which provides a great opportunity for long-term goal attainment. In addition, in this study, patients indicated their goal during rehabilitation was to go home and, supporting previous findings, 2 professionals also stated that patients often do not know what to expect and have difficulties formulating goals. As pointed out by Wade 42 earlier, rehabilitation teams should “work towards patient-centered goals over time and across settings as the patient changes.” Home rehabilitation might provide professionals with the opportunity to address patients’ long-term goals post-discharge and help patients achieve goals that are important to them once they are home again.
Due to the qualitative nature of the data, generalization to other older populations might be limited. In addition, the perspective of the professionals was representative of only a small number of team members. However, the chosen sample was appropriate for the purpose of this study, that is, to gain insight into how patient goals change over time and to explore professionals’ attitudes toward patient-centered goal-setting and their perspectives on rehabilitation goals. We decided to conduct interviews in the third or fourth week post-discharge to allow participants to reflect on the rehabilitation process and their rehabilitation goals while they were inpatients and to inquire whether participants had developed any long-term goals. However, being able to only retrospectively ask patients what their admission goals were at the start of the rehabilitation process may have resulted in recall bias. Also, conducting interviews with patients after a longer period could have provided us with information on the feasibility of the goals formulated during the interviews. Furthermore, besides qualitative interviews and information from patients’ rehabilitation plans, we used no other data sources. For example, data on goal-setting interviews with professionals and patients, which could have been informative as well.
This study has generated insight into how rehabilitation goals of older patients change over time. During inpatient geriatric rehabilitation, patient goals are mainly related to going home and regaining independence in basic self-care activities. Back at home, patients formulate new and more ambitious goals, which are related to their premorbid level of functioning. Professionals expressed that rehabilitation revolves around getting patients ready for discharge as soon as possible, and rehabilitation goals formulated by professionals are mainly discharge-related. Hence, rehabilitation services should distinguish between goals that are important while patients are inpatient and goals that are important to achieve after discharge. Further research can build on this knowledge and help inform future interventions that aim for a more patient-centered approach to goal-setting during inpatient rehabilitation and home rehabilitation once patients are back home again.
Clinical messages
During inpatient geriatric rehabilitation, patients’ goals are related to going home and discharge criteria are professionals’ main focus.
At home, patients are not at their previous level of functioning and have ambitious rehabilitation-level goals related to their pre-illness state.
Supplemental Material
supplementary_Material – Supplemental material for A qualitative study of patient-centered goal-setting in geriatric rehabilitation: patient and professional perspectives
Supplemental material, supplementary_Material for A qualitative study of patient-centered goal-setting in geriatric rehabilitation: patient and professional perspectives by Rosanne van Seben, Susanne M Smorenburg and Bianca M Buurman in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors would like to acknowledge healthcare provider Cordaan (the Netherlands) for its support and the staff and patients who participated. R.v.S., S.M.S., and B.M.B. contributed to the design of the study. R.v.S. was responsible for acquisition of data. All authors contributed to analyses and interpretation of data. All authors contributed substantially to drafting the article or revising it critically.
Authors’ note
Rosanne van Seben is now affliliated to Department of Internal Medicine, Section of Geriatric Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.