
Abstract
Objective:
To investigate construct validity and test–retest reliability of the parent-rated Hand-Use-at-Home questionnaire (HUH) in children with neonatal brachial plexus palsy or unilateral cerebral palsy.
Design and subjects:
For this cross-sectional study, children with neonatal brachial plexus palsy or unilateral cerebral palsy, aged 3–10 years, were eligible.
Main measures:
The HUH, Pediatric Outcome Data Collection Instrument Upper Extremity Scale (neonatal brachial plexus palsy only), and Children’s Hand-Use Experience Questionnaire (unilateral cerebral palsy only) were completed. The HUH was completed twice in subgroups of both diagnoses. Lesion-extent (indication of involved nerve rootlets in neonatal brachial plexus palsy as confirmed during clinical observation and/or nerve surgery) and Manual Ability Classification System levels (unilateral cerebral palsy) were obtained from the medical records. Spearman correlation coefficients between the HUH and all clinical variables, agreement, standard error of measurement, smallest detectable change and intra-class correlation were calculated.
Results:
A total of 260 patients participated (neonatal brachial plexus palsy: 181), of which 56 completed the second HUH (neonatal brachial plexus palsy: 16). Median age was 6.9 years for children with neonatal brachial plexus palsy, 116 had C5-C6 lesions. Median age for children with unilateral cerebral palsy was 6.4 years, 33 had Manual Ability Classification System Level II. The HUH correlated moderately with lesion-extent (rs =−0.5), Pediatric Outcome Data Collection Instrument Upper Extremity Scale (rs = 0.6) and Children’s Hand-Use Experience Questionnaire (rs = 0.5) but weakly with Manual Ability Classification System levels (rs = −0.4). Test–retest reliability was excellent (intra-class correlation2,1 = 0.89, standard error of measurement = 0.599 and smallest detectable change = 1.66 logits) and agreement was good (mean difference HUH1 − HUH2 = 0.06 logits).
Conclusion:
The HUH showed good construct validity and test–retest reliability in children with neonatal brachial plexus palsy or unilateral cerebral palsy.
Keywords
Introduction
Children with neonatal brachial plexus palsy or unilateral cerebral palsy may have difficulties using their affected arm.1–4 This use is often less frequent than expected based on functional capacities5–9 and a discrepancy is often observed between capacity measured in a clinical setting and the actual use of the arm and hand in daily life.7,9 The latter is one of the most important goals in rehabilitation interventions (i.e. the use of newly acquired function/capacities in daily use).
Parent-reported questionnaires assessing arm and hand performance in daily life are available,10–12 but none of them measures how often the affected hand is used spontaneously in the home environment.13–15
Measurement of the amount of daily life spontaneous use of the affected arm and hand in children with unilateral paresis aged 3–10 years can be done with the parent-reported Hand-Use-at-Home questionnaire (HUH). 16 This HUH includes a range of bimanual activities (e.g. closing a zipper, picking up a ball; see Appendix II in supplementary material) and has been validated in over 300 children with unilateral cerebral palsy or neonatal brachial plexus palsy using Rasch analysis. 16
The HUH enables rehabilitation specialists to investigate whether transition of newly acquired function and/or capacities to daily use actually has taken place and is therefore a valuable addition to existing outcome measures. However, how the HUH is associated with other used questionnaires for evaluating arm and hand functioning, disease severity and functional classification has not yet been evaluated. Furthermore, its test–retest reliability has not yet been examined. Conditional for the measure’s use in clinical practice and future research is the establishment of these psychometric properties.
Therefore, the aim of this study was to evaluate construct validity and test–retest reliability of the HUH in children with neonatal brachial plexus palsy or unilateral cerebral palsy.
Methods
This study had a cross-sectional design and was conducted at the Leiden University Medical Center (LUMC) and the Sint Maartenskliniek rehabilitation center (October 2013–May 2015). Ethical approval was obtained (LUMC P14.071, medical ethical committee Arnhem–Nijmegen 2013/395). All parents gave written informed consent.
Identification, recruitment and selection of patients
Children with neonatal brachial plexus palsy or unilateral cerebral palsy were eligible for this study if they were aged between 3 and 10 years and if their medical record was available. Children with neonatal brachial plexus palsy were recruited from the LUMC neonatal brachial plexus palsy care unit and those with unilateral cerebral palsy from 11 pediatric rehabilitation centers that are part of the Dutch Collaboration for Implementation of the Pirate Concept (LIPIC, http://www.piratenconcept.nl/).
Parents of eligible patients were invited to participate in this study and could complete the questionnaires online or on paper. Nonresponders were reminded once by (e-)mail and/or telephone.
Data collected
For this study, the HUH and an additional questionnaire had to be completed (i.e. Pediatric Outcome Data Collection Instrument (PODCI) for neonatal brachial plexus palsy and Children’s Hand-Use Experience Questionnaire (CHEQ/mini-CHEQ) for unilateral cerebral palsy).
For test–retest reliability purpose, a minimum of 50 test–retest questionnaires had to be collected. 17 Therefore, parents who completed the first HUH were asked to complete a second one within a period of two to four weeks after the first one. For this, the arm performance of the child had to be stable and participants who underwent specific arm or hand interventions (i.e. surgery, botulinum toxin injections or intensive arm training) less than three months prior to completing the first HUH or within two weeks thereafter were not invited. Parents were stopped being invited to complete a second HUH after 50 parents had returned their second questionnaire within the four-week time period.
Outcome measures
The HUH assesses the amount of spontaneous use of the affected hand in children with unilateral upper limb paresis aged 3–10 years, performing 18 typical bimanual play and self-care activities. 16 Parents rate items using a 5-point rating scale (never–sometimes–regularly–often–always). After completion, the ratings are converted into a 3-point score (i.e. never/sometimes = score 0, regularly/often = score 1, always = score 2). A sum score can be calculated (range 0–36) and afterwards converted into the Hand-Use-at-Home score in logits (interval scale, range −4.69 to 5.17, see Appendix I in supplementary material). 16
The PODCI is designed to assess different aspects of daily living in children with musculoskeletal disorders. It has excellent psychometric properties, 18 and it is a widely accepted instrument to provide parent/patient-reported information about upper extremity functioning.13–15 A Dutch version is available and it is validated for children with neonatal brachial plexus palsy. 19 It consists of 85 questions and five scale scores and one total score can be calculated (range for all scales and total score 0–100, higher scores indicating better functioning/quality of life). Only the Upper Extremity and Physical Function Scale (8 items) was used in this study since this scale provides information about difficulties performing activities using the arms/hands (score 0–100; lower score, more difficulties).
The CHEQ is a questionnaire for children (aged 6–18) with unilateral functional limitations of hand use and is well validated for children with unilateral cerebral palsy.10,11,20 It was only partially validated for use in children with neonatal brachial plexus palsy 11 and has not yet been used in studies. Therefore, it was not used in this group.
The questionnaire consists of 29 bimanual activities, typically requiring the use of both hands. It assesses the child’s experience using their affected hand when performing the activities and counts how many of the activities are executed independently (with and without using the affected hand). In the mini-version of the CHEQ (http://www.cheq.se/miniquestionnaire), some items were deleted or replaced (with more age appropriate activities for children aged three to eight years) and this version was used for all unilateral cerebral palsy children <six years in this study. The psychometric properties of the mini-version of the CHEQ have not been established yet and therefore the summary of the results of the questionnaire is given as raw scores. To compare outcomes, we used the raw scores to calculate the percentage of the activities in which the affected hand was actually used (CHEQ(bim): items in which the affected hand is used divided by the number of independently executed items) as a measure of bimanual performance.
Patient characteristics
Of all participating children, sociodemographic and disease characteristics (age/gender/diagnosis/affected side) were obtained from the medical records.
In addition, for neonatal brachial plexus palsy, the following characteristics were obtained: lesion-extent (defined by clinical examination and/or during nerve surgery) divided into 4 groups based on lesion localization, (1) C5-C6, (2) C5-C7, (3) C5-C8 and (4) C5-T1 and treatment history which can consist of (1) conservative treatment, (2) primary surgery (nerve), (3) secondary surgery (orthopedic: i.e. tendon transfers, osteotomies) or (4) primary and secondary surgery. Treatment history in this study serves as proxy for lesion severity (i.e. severity of neurological damage) as children who were treated surgically have by definition more severe lesions than children who were treated conservatively.
For unilateral cerebral palsy, the Manual Ability Classification System level was obtained from the medical records. The Manual Ability Classification System is a reliable and valid classification for children with cerebral palsy, classifying the ability to handle objects in daily activities in five levels, with higher levels representing worse performance. 3
Data analysis
Statistical analyses were executed using SPSS 20.0 (IBM, Armonk, NY, USA). All continuous variables were expressed as means with standard deviations (SDs), or as medians with interquartile ranges (IQRs), based on their distributions. Missing values were replaced with predicted values using the Expectation–Maximization technique.
In concordance with the recommended quality criteria to investigate measurement properties of health status questionnaires (COSMIN) 17 we investigated the construct validity by testing the following hypotheses:
There is a moderate–good negative correlation between Hand-Use-at-Home scores and neonatal brachial plexus palsy lesion-extent. Neonatal brachial plexus palsy lesion-extent group 1 (C5-C6 lesions) will have higher Hand-Use-at-Home scores than the other groups since a greater lesion-extent will probably affect spontaneous hand use negatively.
There is a weak negative correlation between Hand-Use-at-Home scores and treatment history (proxy for lesion severity) in neonatal brachial plexus palsy. Conservatively treated children are more mildly affected than surgically treated children but may not necessarily score higher on the HUH.
There is a moderate–good positive correlation between the Hand-Use-at-Home scores and the PODCI Upper Extremity and Physical Function scale in children with neonatal brachial plexus palsy. Children with less difficulty performing daily life activities with their affected arm and hand will show more spontaneous use of their affected arm and hand.
There is a weak negative correlation between the Hand-Use-at-Home scores and Manual Ability Classification System levels in children with unilateral cerebral palsy because limitations in manual ability will hamper the performance of daily activities but may not necessarily affect the amount of arm and hand use in children with unilateral cerebral palsy.
There is a moderate–good positive correlation between the Hand-Use-at-Home scores and the CHEQ(bim) as children with unilateral cerebral palsy who use their affected hand in many of the CHEQ activities are likely to display more spontaneous use of the affected arm and hand.
To test the above hypotheses, Spearman correlation coefficients were calculated. Correlations 0.3 <rs < 0.5 were considered weak, 0.5 < rs < 0.75 moderate to good and rs > 0.75 good to excellent (P < 0.05). 21
In addition, we used a one-way analysis of variance (ANOVA) with Games-Howell post hoc testing to further examine our hypotheses regarding the HUH outcomes; group differences were examined for the lesion-extent and treatment history groups in neonatal brachial plexus palsy and the Manual Ability Classification System level groups in unilateral cerebral palsy.
Test–retest reliability was investigated by computing the intra-class correlation coefficient (ICC2,1) with the minimum acceptable value being 0.70.17,22 We used the Bland–Altman method to assess agreement between both Hand-Use-at-Home scores. The standard error of measurement(agreement) using the within-subject variance (standard error of measurement = √error variance) and smallest detectable change (smallest detectable change = 1.96 × √2 × standard error of measurement) was calculated to determine the minimal change representing a real difference between two scores of an individual above measurement error (smallest detectable change(individual)). In addition, the smallest detectable change at group level was computed (smallest detectable change(group) = smallest detectable change(individual)/√n).
Results
In this study, a convenience sample of 260 children and their parents was included (181 neonatal brachial plexus palsy, median age: 6.9 years and 79 unilateral cerebral palsy, median age: 6.4 years) and completed the required questionnaires. A little more than the required amount of 50 second HUH for test–retest reliability analysis were gathered (N = 56: 16 neonatal brachial plexus palsy, 40 unilateral cerebral palsy, median age: 7.2 years). Table 1 provides the patient characteristics and Figure 1 shows the flow of these patients.
Demographic and clinical characteristics of included children with neonatal brachial plexus palsy or unilateral cerebral palsy.
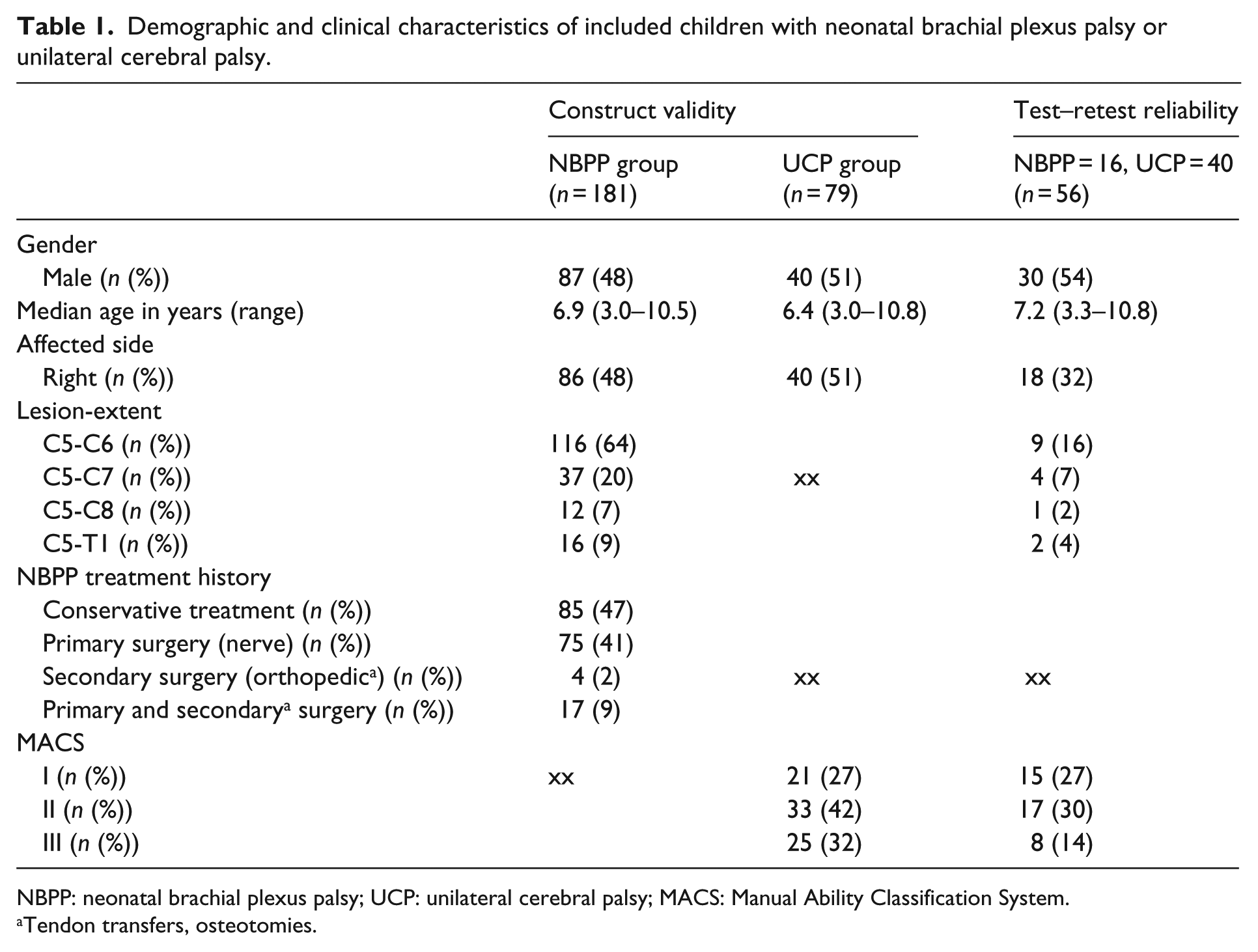
NBPP: neonatal brachial plexus palsy; UCP: unilateral cerebral palsy; MACS: Manual Ability Classification System.
Tendon transfers, osteotomies.
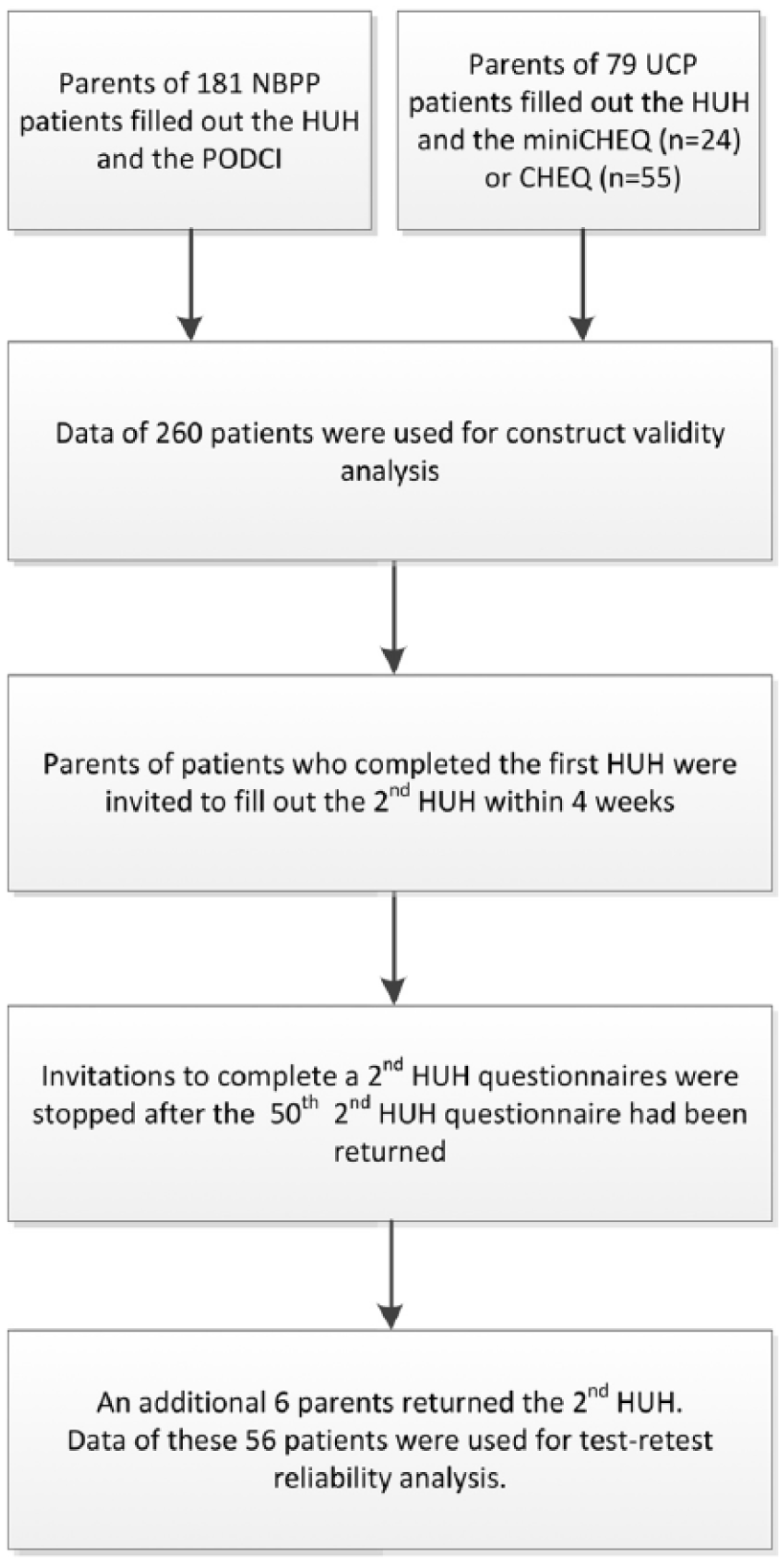
Flow of patients included in the Hand-Use-at-Home questionnaire validity and reliability study. NBPP: neonatal brachial plexus palsy; UCP: unilateral cerebral palsy; HUH: Hand-Use-at-Home questionnaire; PODCI: Pediatric Outcome Data Collection Instrument; CHEQ: Children’s Hand-Use Experience Questionnaire.
There were some missing values in the HUHs (five questions in three individuals). Seven PODCI Upper Extremity and Physical Function scales could not be calculated because parents reported that their child was too young to perform several items on this scale. Therefore, PODCI data of only 174 children could be used for analysis.
The HUH, PODCI Upper Extremity and Physical Function scale and CHEQ(bim) scores are presented in Table 2. The median Hand-Use-at-Home score for the neonatal brachial plexus palsy group was clearly higher than for the unilateral cerebral palsy group (1.06 and −0.34 logits, respectively). The median PODCI Upper Extremity and Physical Function scale score was 83.0 points (IQR 71.0; 96.0) and 24% obtained the maximum score. The CHEQ(bim) score was negatively skewed (median 100%). The number of independent activities was normally distributed (mean 16, range 3–28 activities).
Group outcomes and correlations with Hand-Use-at-Home Questionnaire for neonatal brachial plexus palsy (n = 181) and unilateral cerebral palsy (n = 79).

IQR: interquartile range; NBPP: neonatal brachial plexus palsy; HUH: Hand-Use-at-Home questionnaire; PODCI-UE: Pediatric Outcome Data Collection Instrument Upper Extremity Functioning scale; CHEQbim: Children’s Hand-Use Experience Questionnaire bimanual score (%): percentage activities independently executed using both hands; MACS: Manual Ability Classification System.
Spearman’s rho.
In children with neonatal brachial plexus palsy, the Hand-Use-at-Home scores correlated moderately with lesion-extent (rs = −0.5) and weakly with treatment history (rs = −0.3). There was a moderate correlation between Hand-Use-at-Home scores and the PODCI Upper Extremity and Physical Function scale (rs = 0.6). In children with unilateral cerebral palsy, the Hand-Use-at-Home scores correlated weakly with the Manual Ability Classification System (rs =−0.4) and moderately with the CHEQ(bim) (rs = 0.5) (all P < 0.001).
Table 3 shows differences in Hand-Use-at-Home scores between subgroups of patients with neonatal brachial plexus palsy or unilateral cerebral palsy. For neonatal brachial plexus palsy, we found significant differences between levels of lesion-extent (F = 15.65, P < 0.001) and treatment history (F = 8.41, P < 0.001). Greater neonatal brachial plexus palsy lesion-extent was associated with lower Hand-Use-at-Home scores. All lesion-extent subgroups differed significantly from the C5-C6 subgroup (P < 0.001). A history of primary and/or secondary surgery in children with neonatal brachial plexus palsy was associated with lower Hand-Use-at-Home scores (P < 0.001). In children with unilateral cerebral palsy, there were significant differences in Hand-Use-at-Home scores between Manual Ability Classification System levels (F = 7.09, P = 0.002). There was no significant difference between Manual Ability Classification System levels I and II, but Manual Ability Classification System level III was clearly associated with lower Hand-Use-at-Home scores (P = 0.001).
Mean Hand-Use-at-Home Questionnaire scores and differences within groups for lesion-extent and treatment history in children with neonatal brachial plexus palsy (n = 181); and for Manual Ability Classification System levels in children with unilateral cerebral palsy (n = 79).
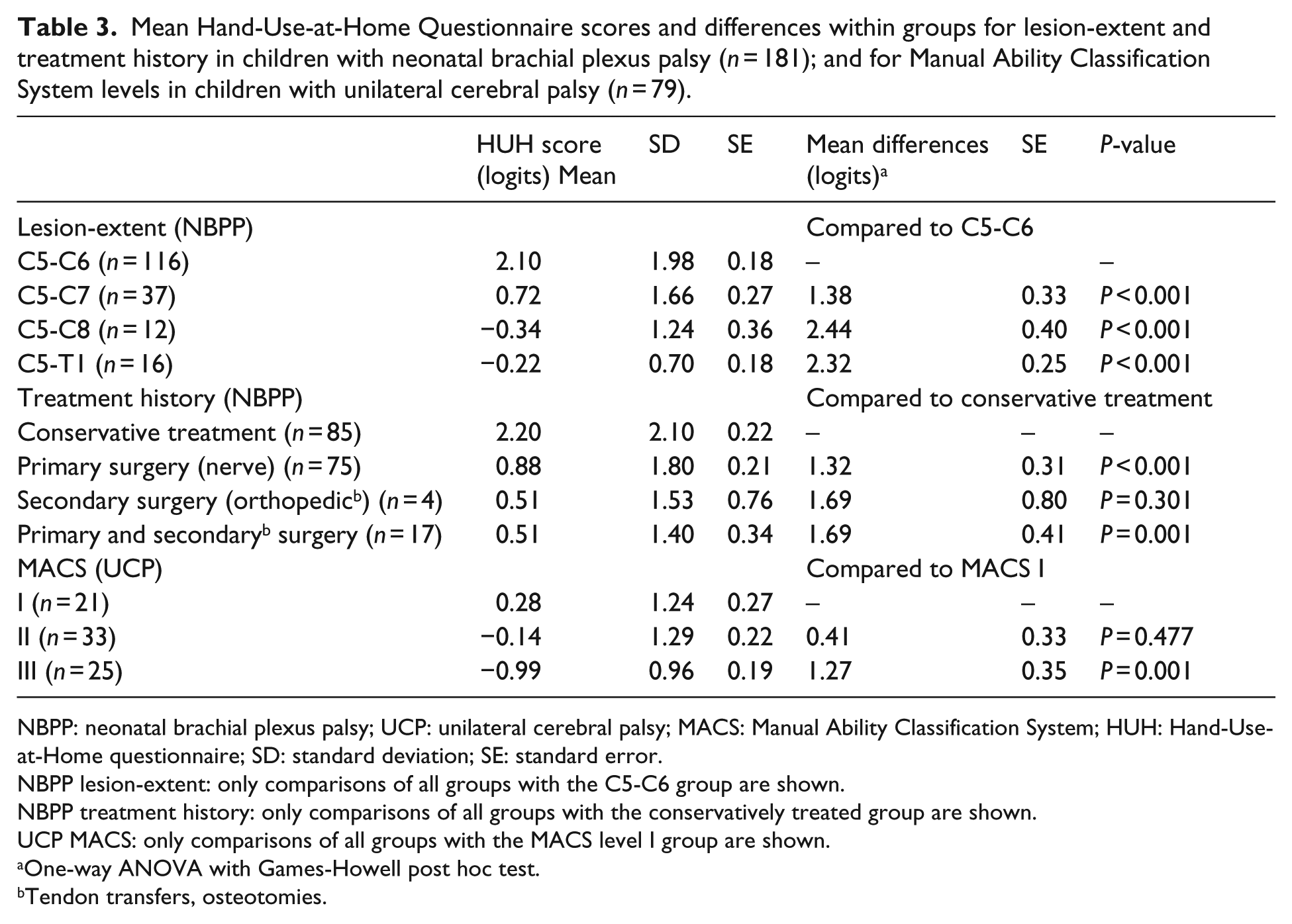
NBPP: neonatal brachial plexus palsy; UCP: unilateral cerebral palsy; MACS: Manual Ability Classification System; HUH: Hand-Use-at-Home questionnaire; SD: standard deviation; SE: standard error.
NBPP lesion-extent: only comparisons of all groups with the C5-C6 group are shown.
NBPP treatment history: only comparisons of all groups with the conservatively treated group are shown.
UCP MACS: only comparisons of all groups with the MACS level I group are shown.
One-way ANOVA with Games-Howell post hoc test.
Tendon transfers, osteotomies.
Test–retest reliability (Table 4) was found to be good with an intra-class correlation coefficient (ICC2,1) of 0.89 (P < 0.001). The absolute agreement is presented in Figure 2. The mean difference (SD) between the first and the second assessment was 0.06 logits (0.85) The standard error of measurement(agreement) was 0.599 logits, which resulted in a smallest detectable change(individual) of 1.66 logits and a smallest detectable change(group) of 0.22 logits.
Test–retest reliability for the Hand-Use-at-Home Questionnaire in children with neonatal brachial plexus palsy or unilateral cerebral palsy (n = 56).
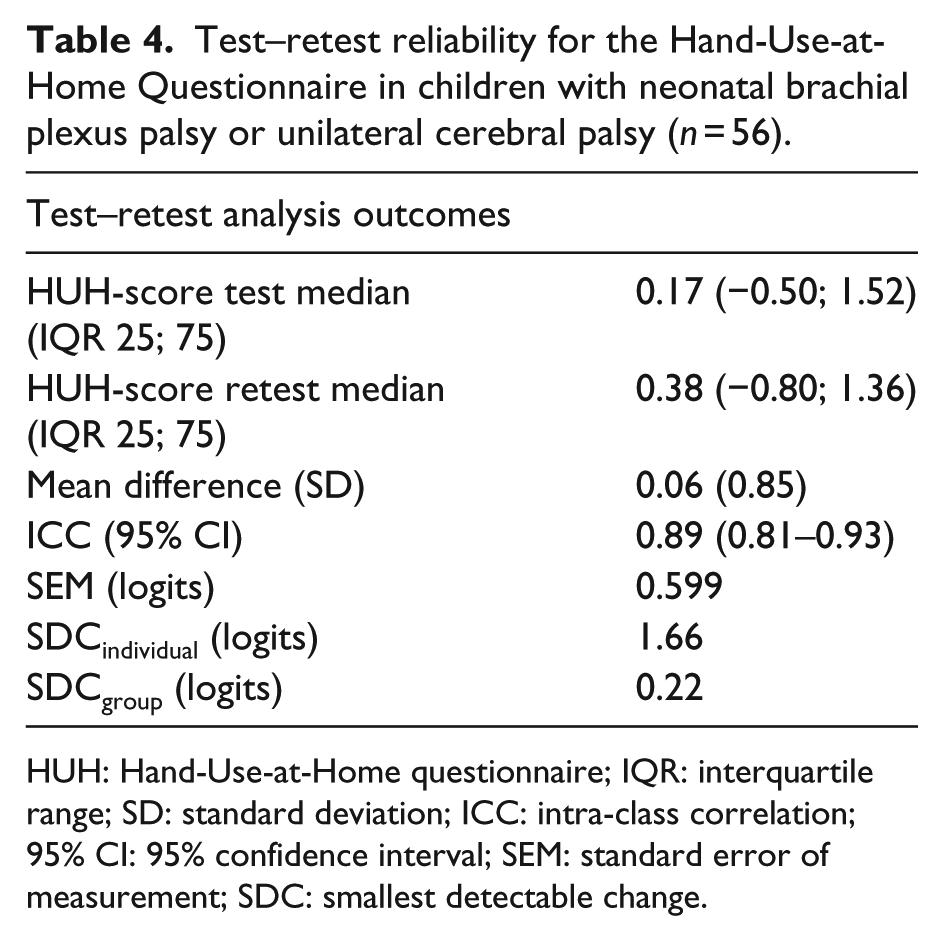
HUH: Hand-Use-at-Home questionnaire; IQR: interquartile range; SD: standard deviation; ICC: intra-class correlation; 95% CI: 95% confidence interval; SEM: standard error of measurement; SDC: smallest detectable change.
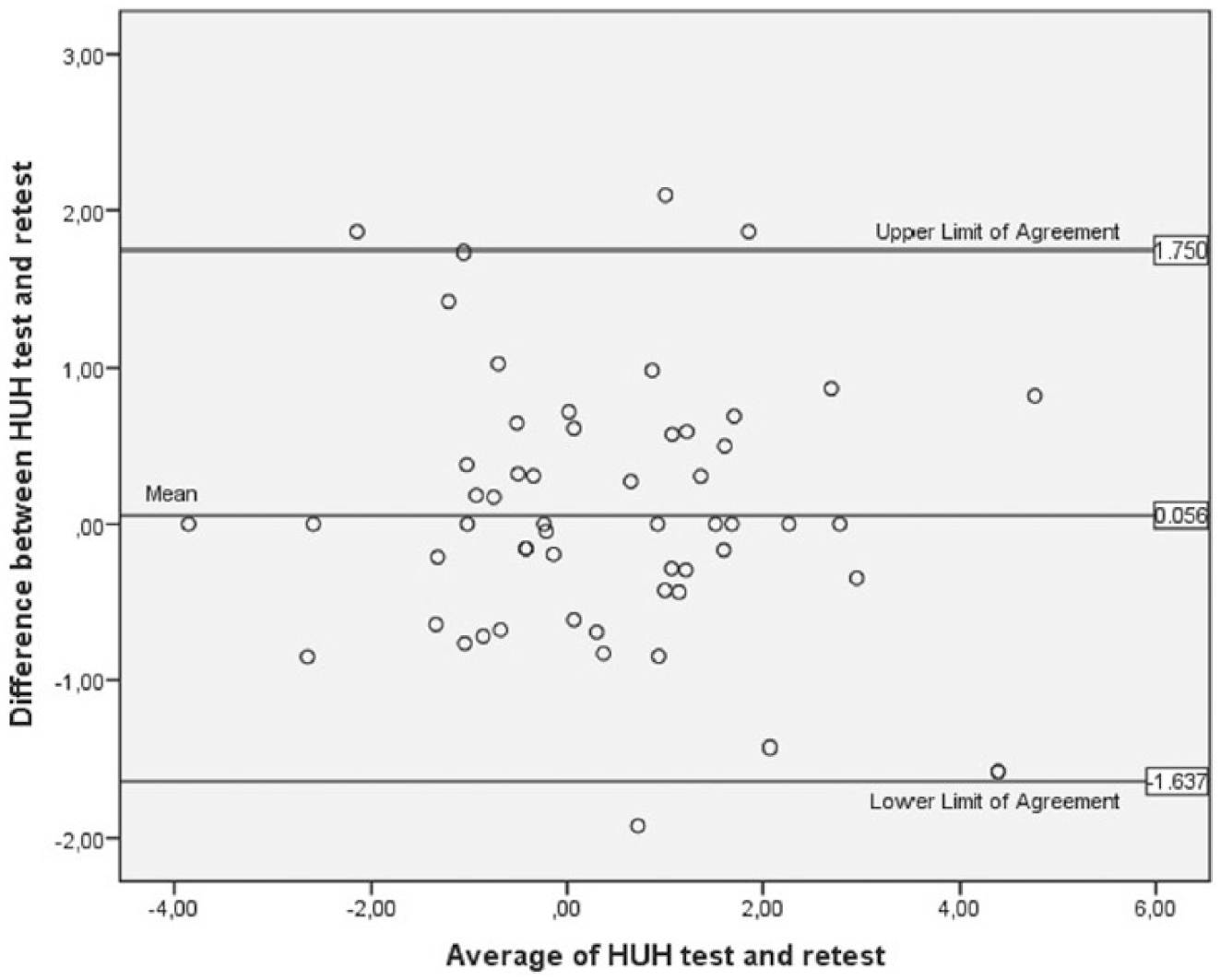
Bland–Altman plot showing agreement between the Hand-Use-at-Home Questionnaire (HUH) test and retest. (Limits of agreement are located at ±2 standard deviations from the mean difference.)
Discussion
Results of our study showed that the HUH is a valid and reliable measure to be used in children with neonatal brachial plexus palsy or unilateral cerebral palsy aged 3–10 years old. The correlation between the HUH and lesion-extent indicated that greater lesion-extent is associated with less spontaneous hand use. The weak correlation with Manual Ability Classification System levels in children with unilateral cerebral palsy indicated that a good ability to handle objects is not directly associated with a high amount of spontaneous use of the affected arm and hand. Test–retest reliability was found to be excellent based on a good intra-class correlation coefficient and good agreement.
The test–retest reliability results indicate that parents’ observations can reliably be used to measure the amount of spontaneous hand use in children with neonatal brachial plexus palsy or unilateral cerebral palsy. In an instrument with high test–retest reliability, repeated measurements in an unchanged subject will result in similar outcomes that are not influenced by characteristics of the instrument.17,22 The absolute agreement between the repeated assessments was good as indicated by the standard error of measurements. When Hand-Use-at-Home scores of two groups of children are compared, a group difference of 0.22 logits can be regarded as a real difference, which is not due to natural variation. For individual children, a change in Hand-Use-at-Home scores needs to be >1.66 logits to be significantly different.
Little is known about spontaneous use of the affected hand at home in children with unilateral upper limb paresis. Clinical assessments capture arm and hand use in a test setting but do not provide insight into actual daily life performance, nor in the amount of hand use. Spontaneous hand use was investigated in a few studies but only with regard to children with unilateral cerebral palsy.7,23 A qualitative study showed that children with unilateral cerebral palsy spontaneously use their affected hand mainly in tasks that absolutely require the use of both hands. 7 Another study used an accelerometer in the home environment to objectively measure arm movements, as was done in adults before. 23 This study found that children with unilateral cerebral palsy used their affected arm, but it was not possible to conclude from the data whether this use was related to bimanual activities.
Several studies reported difficulties in using the affected arm in children with neonatal brachial plexus palsy and found a relationship between lesion-extent and arm capacity.1,2,4 The actual amount of spontaneous use has, to our knowledge, not been reported for neonatal brachial plexus palsy before. Our study found a moderate relation between (greater) lesion-extent and (lower) amount of spontaneous hand use (Tables 2 and 3). In the C5-C6 group, the amount of spontaneous hand use was relatively high but only 22 children (19%, all treated conservatively) had a maximum Hand-Use-at-Home score. A possible explanation for this high amount of spontaneous use in the C5-C6 group could be that these children had fully recovered, as occurs in about 70% of the children with neonatal brachial plexus palsy. 2 The association between treatment history (proxy for lesion severity) and amount of hand use was less strong but conservatively treated children had significantly higher Hand-Use-at-Home scores than children who were treated surgically. Even so, in all treatment groups, there was a wide spread in outcomes indicating that a favorable or a worse prognosis for lesion recovery early in life does not automatically lead to more or less spontaneous hand use later in life. The secondary surgery group (n = 4) was too small to explain any relationship with spontaneous hand use. Our findings also indicate that the HUH is able to distinguish between levels of lesion-extent.
The eight daily activities in the PODCI Upper Extremity and Physical Function scale show similarities with items in the HUH, but three are unimanual items and some can be performed using only the preferred hand. In contrast, the HUH consists of only bimanual items, hierarchically ordered according to how strong they elicit the use of the affected hand. The moderate relationship between both instruments, measuring different constructs, indicates that children performing well on the PODCI Upper Extremity and Physical Function scale are not automatically inclined to use both their hands simultaneously during daily life activities.
Studies in children with unilateral cerebral palsy found that higher Manual Ability Classification System levels coincided with lower outcomes on unimanual capacity and bimanual performance measures.24,25 We found that the children with a lower capacity to handle objects independently (Manual Ability Classification System level III) actually did show significantly less spontaneous use of their affected hand than children with Manual Ability Classification System level I or II. The weak association between Manual Ability Classification System and the HUH, however, indicated that a good ability to use the affected hand (Manual Ability Classification System level I) does not automatically result in a high amount of use of this hand in daily activities.
The association between the HUH and the CHEQ(bim) in children with unilateral cerebral palsy was weak. The number of independently performed activities was normally distributed over the sample, but most of these activities were executed using the affected hand (median 100%). The activities of the CHEQ all specifically require the simultaneous use of both hands and can hardly be performed unimanually, which explains the high CHEQ(bim) percentages. In contrast, only a few HUH activities explicitly require the use of the affected hand; they elicit the use of the affected hand to an increasing extent in order to assess whether the affected hand is spontaneously used. Our findings indicate that children with unilateral cerebral palsy do use their affected hand if the task specifically demands bimanual task execution but that spontaneous use of the hand in activities in which the affected hand is not needed can be different. The moderate correlation between both instruments indicates that the HUH measures a different construct requiring a specific item set.
In both diagnosis groups, we found significant relationships between arm and hand capacity reflected by the Manual Ability Classification System levels (unilateral cerebral palsy) and lesion-extent (neonatal brachial plexus palsy) and the amount of spontaneous hand use. This indicates that the amount of hand use is negatively influenced by decreasing abilities to use the arm and hand. However, there still is a large portion of unexplained variance in the Hand-Use-at-Home score, which might be explained by the presence of developmental disregard (i.e. lack of spontaneous use of the affected arm/hand in developing children).8,26
Future studies are warranted to establish the possible relationship between developmental disregard and HUH outcomes.
This study had a number of limitations. First, the sample in the neonatal brachial plexus palsy group was relatively heterogeneous in terms of lesion-extent and treatment history, which might have positively influenced HUH outcomes. The unilateral cerebral palsy sample contained a relative large group of children with Manual Ability Classification System level III compared to the general unilateral cerebral palsy population, which might have negatively influenced HUH outcomes. Second, there is no golden standard to establish amount of hand use. Therefore, in our study, we used two widely accepted arm outcome measures (PODCI Upper Extremity and Physical Function scale and CHEQ) to examine to what extent the HUH measures a different construct of arm and hand performance. Finally, this study had a cross-sectional design, only measuring arm/hand use at one point in time. Future studies, for example, on analyzing functional outcomes of surgical interventions, are warranted to evaluate the responsiveness of the HUH. To be able to use the HUH in different countries, it should be officially translated into different languages and cross-culturally adapted. An English translation is currently underway.
In conclusion, our study found that the HUH has good psychometric properties to measure a specific aspect of arm and hand performance: the amount of spontaneous use. It can reliably be used by parents of children with unilateral upper limb paresis, aged 3–10 years, to report spontaneous arm/hand use of their child during daily activities. It provides clinicians and researchers with more insight in daily life performance.
Clinical messages
The HUH is able to distinguish between levels of lesion-extent in children with neonatal brachial plexus palsy.
A good ability to use the affected hand does not automatically result in a high amount of hand use.
Supplemental Material
Supplementary_Material – Supplemental material for Hand-Use-at-Home Questionnaire: validity and reliability in children with neonatal brachial plexus palsy or unilateral cerebral palsy
Supplemental material, Supplementary_Material for Hand-Use-at-Home Questionnaire: validity and reliability in children with neonatal brachial plexus palsy or unilateral cerebral palsy by Menno van der Holst, Yvonne Geerdink, Pauline Aarts, Duco Steenbeek, Willem Pondaag, Rob GHH Nelissen, Alexander CH Geurts and Thea PM Vliet Vlieland in Clinical Rehabilitation
Footnotes
Acknowledgements
The authors would like to thank Dr Stéphanie L van der Pas (Department of Medical Statistics, LUMC) for her help with the statistics in this study. M.V.D.H and Y.G. authors contributed equally.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.