
Abstract
Objectives:
To evaluate rehabilitation outcomes in patients with moderate to severe cognitive impairment.
Design:
Prospective observational cohort study.
Setting:
Rehabilitation unit for older people.
Subjects:
A total of 116 patients (70F) mean age (SD) 86.3 (6.4). Group 1: 89 patients with moderate cognitive impairment (Mini-Mental State Examination 11–20); and Group 2: 27 patients with severe cognitive impairment (Mini-Mental State Examination 0–10).
Intervention:
A personalised rehabilitation plan.
Main measures:
Barthel Activity of Daily Living score on admission and discharge, length of stay and discharge destination.
Results:
Of 116 patients, 64 (55.2%) showed an improvement in Barthel score. Mini-Mental State Examination was significantly higher in those who improved, 15.4 (SD 3.7) vs.13.2 (SD 5.1): p = 0.01. The mean Barthel score improved in both groups; Group 1 – 14.7 (SD 19.1) vs. Group 2 – 9.3 (SD 16.3): p = 0.17. Of 84 home admissions in Group 1, more patients returning home showed improvements of at least 5 points in the Barthel score compared with nursing/residential home discharges (32/37 – 86.5% vs. 10/28 – 35.7%: p = 0.0001). In Group 2 of 17 home admissions, 6/6 (100%) home discharges showed improvement compared with 3/7 (42.8%) discharges to nursing/residential home (p = 0.07). In Group 1, a discharge home was associated with significantly greater improvement in number of Barthel items than a nursing/residential home discharge (3.27 (SD 2.07) vs. 1.86 (SD 2.32): p = 0.007). A similar non-significant pattern was noted for severe cognitive impairment patients (3.5 (3.06) vs. 1.14 (1.06); p = 0.1).
Conclusion:
Patients with moderate to severe cognitive impairment demonstrated significant improvements in Barthel score and Barthel items showing that such patients can and do improve with rehabilitation.
Introduction
Rehabilitation has an important role in the recovery process after acute illness in older people.1,2 Patients with cognitive impairment recover either less well or more slowly or both during rehabilitation. Cognitive impairment resulting from dementia or delirium has been recognised to lead to poor functional recovery, higher nursing home placement and unplanned hospital admission compared with those observed in cognitively intact patients.3,4 It has also been identified as a factor contributing to increased length of stay in Older Peoples’ Rehabilitation Units. 5 As a consequence, it has been suggested that people with cognitive impairment have been excluded from access to multi-professional rehabilitation on the assumption that they are unable to benefit. 6 Some rehabilitation services have admissions criteria that exclude patients with a cognitive state or mental health status that might interfere with their medical, nursing and therapy treatments. 7 While it is important to get the right patients in the right environment for rehabilitation, there is a danger that patients with cognitive impairment are excluded from the process when they have the potential to improve.8,9 Optimising the chances of recovery in cognitively impaired patients is particularly important owing to adverse outcomes associated with this group of patients. For instance, there is evidence that half of patients admitted to hospital with a hip fracture or pneumonia die within six months compared with around 13% of cognitively intact individuals. 10
Although patients with cognitive impairment constitute a significant proportion of patients admitted with an acute medical illness, there is very little evidence of how best to optimise recovery through rehabilitation in such patients. The benefits of rehabilitation in such patients remain unclear and the perception that they are less likely to benefit remains. 11 The reasons for poor outcomes may not only be owing to poor cognition, but may also be owing to increased falls and adverse incidents, and less individual and group therapy per hospital stay. 12 Indeed, there is increasing evidence from meta-analysis that patients with mild to moderate cognitive impairment benefit as much as cognitively intact individuals. 13 It is possible that a combination of physical, cognitive and pharmacological interventions contribute to such findings. While patients with cognitive impairment may not learn new techniques or strategies, they might benefit from a pragmatic programme based on function, repetition of routine daily tasks and familiarity of environment. This probably requires the implementation of dedicated services to manage cognitive and behavioural issues to promote recovery of function and ambulation.11,14 There however remains very little research for evidence of benefit of rehabilitation in patients with moderate to severe cognitive impairment. The aim of this cohort study was to study rehabilitation outcomes in that group of patients.
Methods
In a prospective observational study we recorded rehabilitation outcomes in a cohort of consecutive patients with moderate to severe cognitive impairment admitted for rehabilitation. Patients were recruited by a researcher over a one-year period on a 50-bedded (2 wards) general rehabilitation unit for older people in the United Kingdom. Data were obtained by referring to notes, interviewing nurses and therapists, and direct patient assessment. Participants were recruited into the study within the first week of admission and followed until discharge. All individuals admitted for rehabilitation had been transferred from an acute setting after an admission with an acute medical or surgical condition. Participants were transferred after being assessed by a multidisciplinary team as having the potential to benefit from rehabilitation by improving their functional ability. Individuals with hip fracture and stroke were not admitted to these general rehabilitation wards for operational reasons. Individuals transferred were deemed to have sufficiently recovered from their acute illness to be able to participate in the rehabilitation process. As this was an observational study, there was no defined time period for rehabilitation, but an analysis was made at discharge or at a cut-off point of 80 days, whichever was the shorter.
Cognition was assessed on admission using the Mini-Mental State Examination 15 and participants were grouped according to their cognition using the score as described by the British National Institute for Health and Clinical Excellence guidelines 2006. 16 Group 1 participants had moderate cognitive impairment (Mini-Mental State Examination: 11–20), and participants in Group 2 had severe cognitive impairment (Mini-Mental State Examination: 0–10). We also assessed cognitive function using the Frontal Assessment Battery 17 and screened for anxiety and depression using the hospital anxiety and depression score. 18 Functional ability was also assessed on admission using the Barthel Activities of Daily Living (ADL) score. 19 This score was calculated within two days of admission. Function was then reassessed after intervention at two and six weeks and at discharge. The Barthel ADL score is made up of 10 discrete items referring to ADL. As it is not scored in a continuous fashion, our primary outcome was improvement in the score of at least 5 points. We also evaluated improvement in the number of items on the Barthel score as an outcome measure. Comorbid illness has been shown to affect outcome measures, such as length of stay, mortality and functional outcome. Information relating to comorbidities was collected and scored using the Charlson Comorbidity Index. 20
Each participant had formal input from physiotherapists, physiotherapy assistants and occupational therapists. Each participant had a personalised rehabilitation plan depending on individual abilities, but with the intention of addressing rehabilitation needs on a daily basis. All patients had informal therapy by nursing staff when mobilising and through support for ADL.
Ethical approval was obtained from the Dorset Research Ethics Committee, and consent was obtained from all participants. Participants with severe cognitive impairment who could not give informed consent were included after assent was obtained from their next of kin. If this was not possible they were excluded.
Statistical analysis
Fisher’s exact probability test was used to analyse categorical data and the Wilcoxon signed ranks test was used to compare non-parametric data. We made a separate analysis comparing the number of patients showing an improvement in Barthel score by place of discharge (back home or a nursing/residential home) for patients admitted from home. Univariate analyses were used to investigate the association between the various patient characteristics.
Results
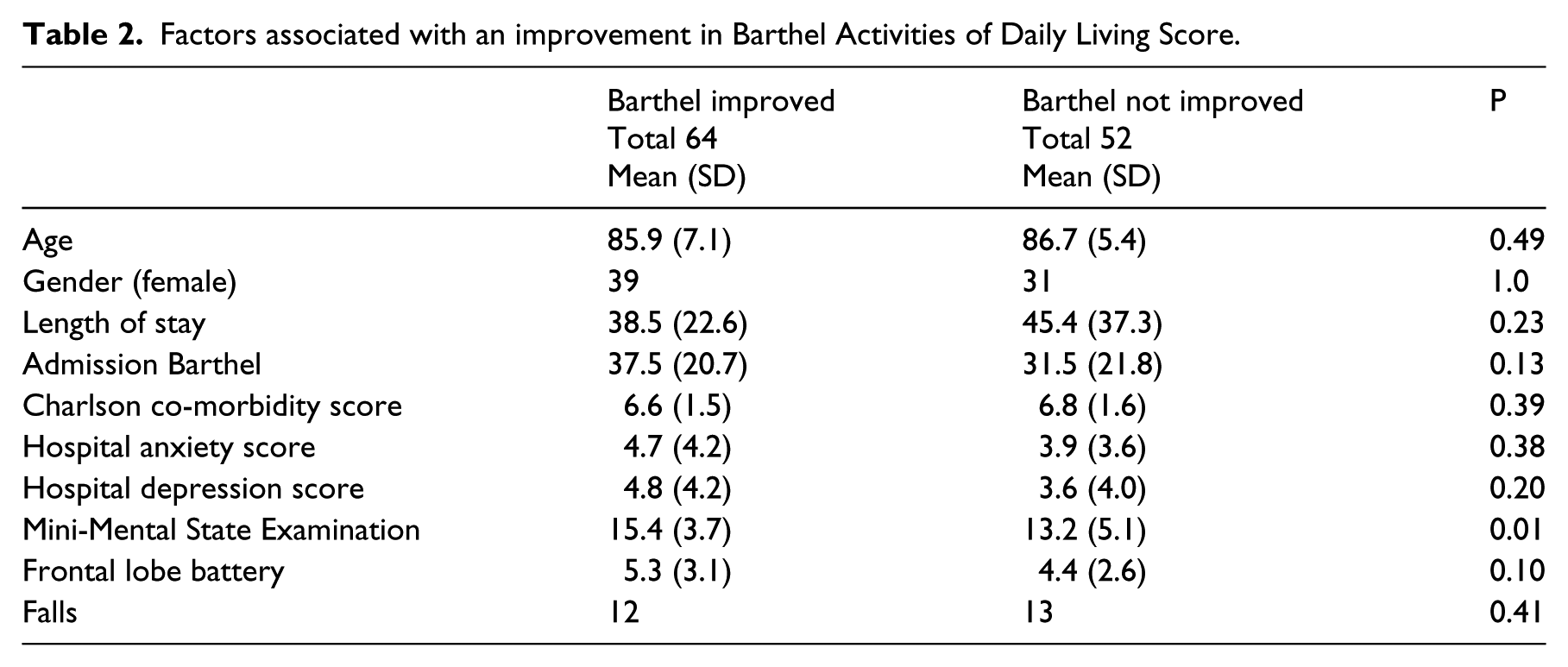
We studied 116 patients (70 F) mean (SD) age 86.3 (6.4) (Figure 1). Group 1 (Mini-Mental State Examination 11–20) included 89 patients and Group 2 (Mini-Mental State Examination 0–10) included 27 patients. At the time of the study the unit had a mean length of stay of 36.6 days (SD 26.6). Group 1 had a mean length of stay of 42.5 days (SD 32.0) and Group 2 was 38.7 days (SD 23.5). Demographic details of the two groups of patients are given in Table 1. Group 1 had a significantly better Barthel Score on admission with no significant differences with the Charlson Co-morbidity Index. Overall, 55.2% (64/116) of patients showed an improvement in Barthel score after rehabilitation. When one excluded the number of patients who died (19 patients) and the ‘other’ group who were transferred to the acute hospital for medical reasons (nine patients), the number of patients showing improvement rose to 72% (64/88). There was no significant difference in the number of patients showing improvement between the two groups with 52/89 (58.4%) showing improvement in Group 1 compared with 12/27 (44.4%) in Group 2. Similarly there was improvement in the mean Barthel score in both groups; Group 1 with 14.7 (SD 19.1) vs. Group 2 with 9.3 (SD 16.3); p = 0.17. The factors associated with an improvement in Barthel score are highlighted in Table 2. The average Mini-Mental State Examination score was significantly higher in the Group that improved (15.4 (SD 3.7) vs. 13.2 (SD 5.1) p = 0.01).
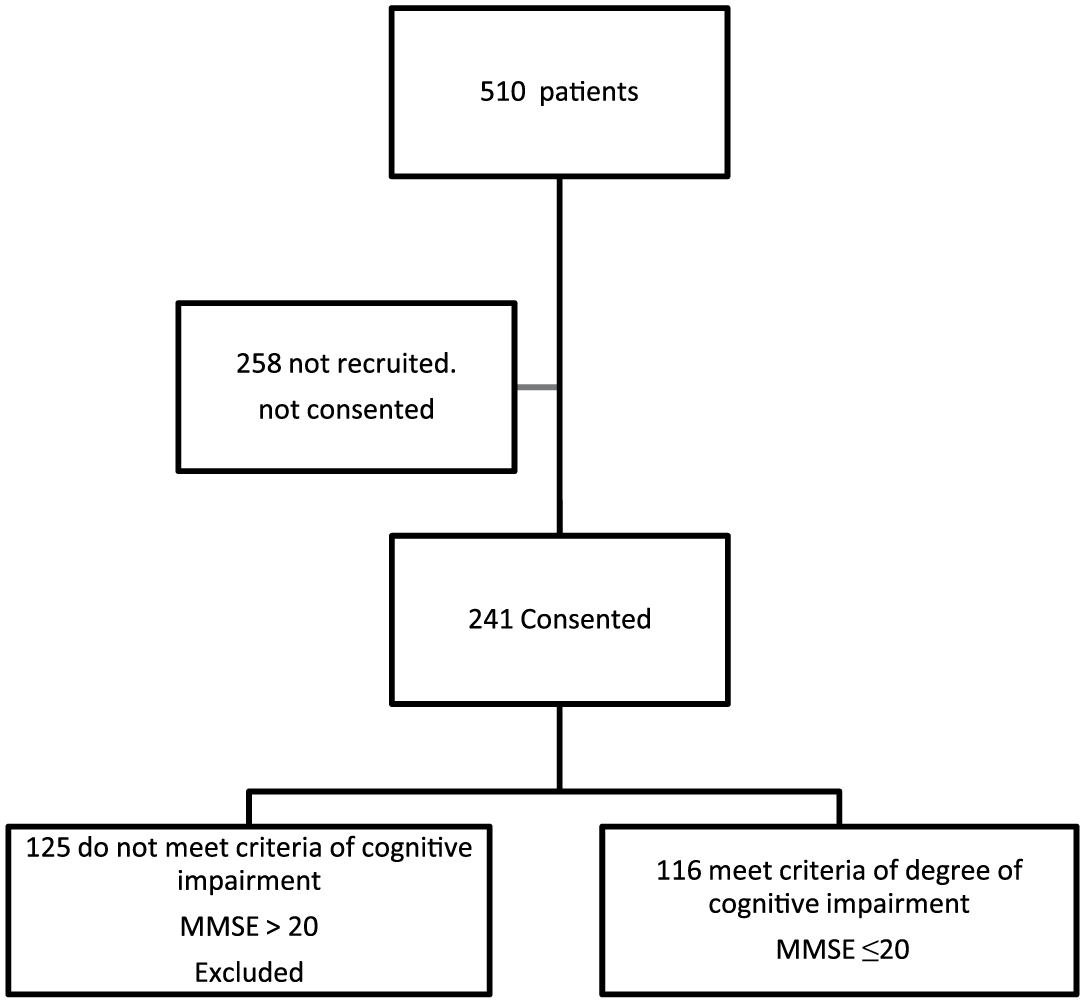
Flow diagram indicating recruitment to the study.
Patient Demographics.
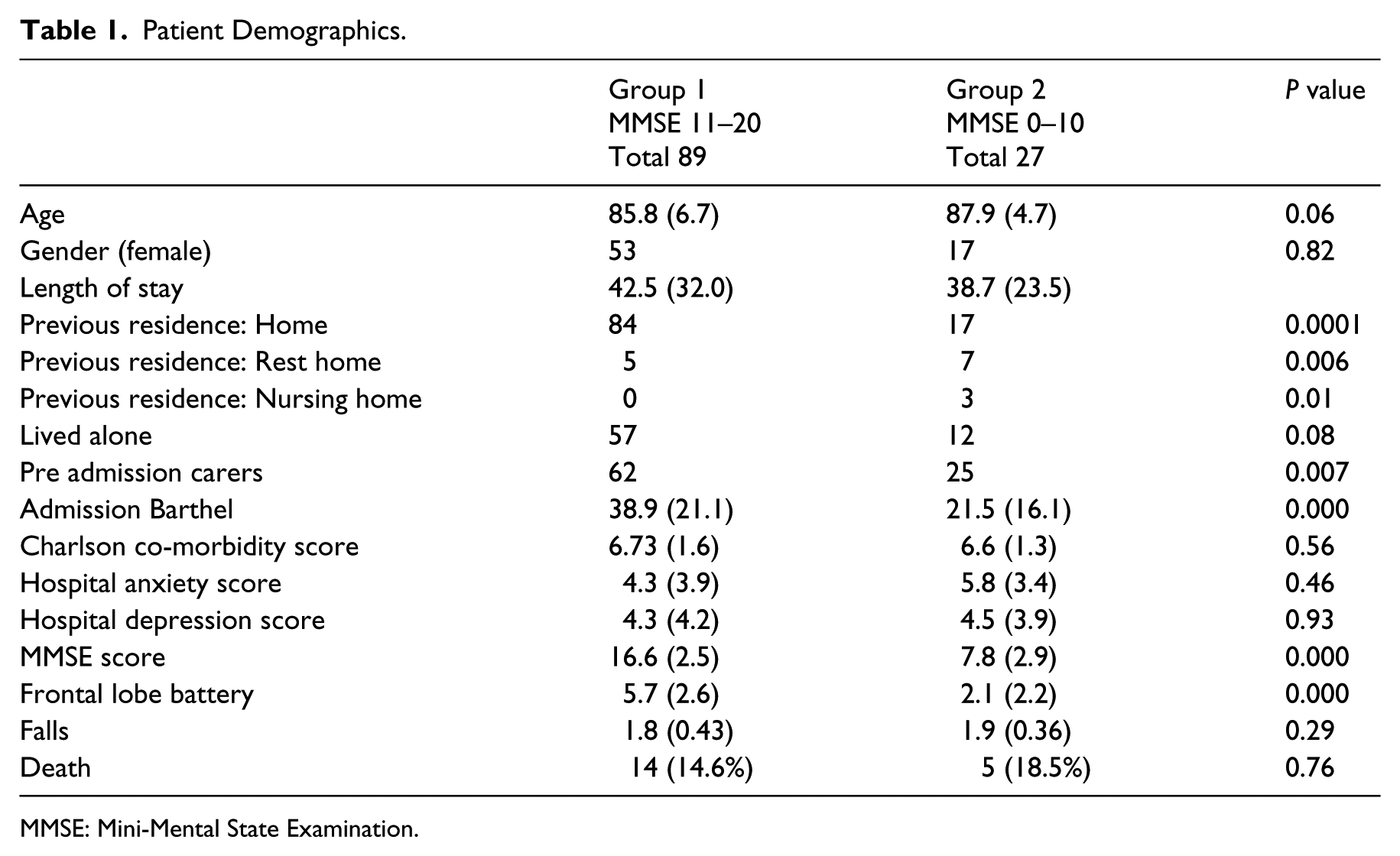
MMSE: Mini-Mental State Examination.
Factors associated with an improvement in Barthel Activities of Daily Living Score.
We evaluated the characteristics associated with patients who were discharged home (Table 3). Patients with a higher admission and discharge Barthel score, Mini-Mental State Examination and frontal lobe battery were more likely to be discharged home. In both groups, patients admitted from home and discharged back home were significantly more likely to have improved their Barthel score compared with nursing/residential home discharges (38/43 (88.4%) vs. 13/35 (37.1%); p = 0.0001). Of the own home discharges in Group 1, 32/37 (86.5%) patients improved their Barthel score compared with 10/28 (35.7%) of nursing/residential home discharges (p = 0.0001). In the severely cognitive impaired 6/6 (100%) own home discharges showed an improvement compared with 3/7 (42.8%) patients discharged to placement (p = 0.07). There was a similar pattern of improvement in relation to Barthel score items. In both groups, a discharge home required an improvement in at least three Barthel items. In patients with moderate cognitive impairment, a discharge home was associated with a significantly greater difference in the improvement of Barthel score items than a nursing/residential home discharge (3.27 (SD 2.07) vs. 1.86 (SD 2.32); p = 0.007). A similar pattern was noted for severe cognitive impairment patients, although this did not reach significance levels (3.5 (3.06) vs. 1.14 (1.06); p = 0.1).
Characteristics associated with patients who were discharged home.
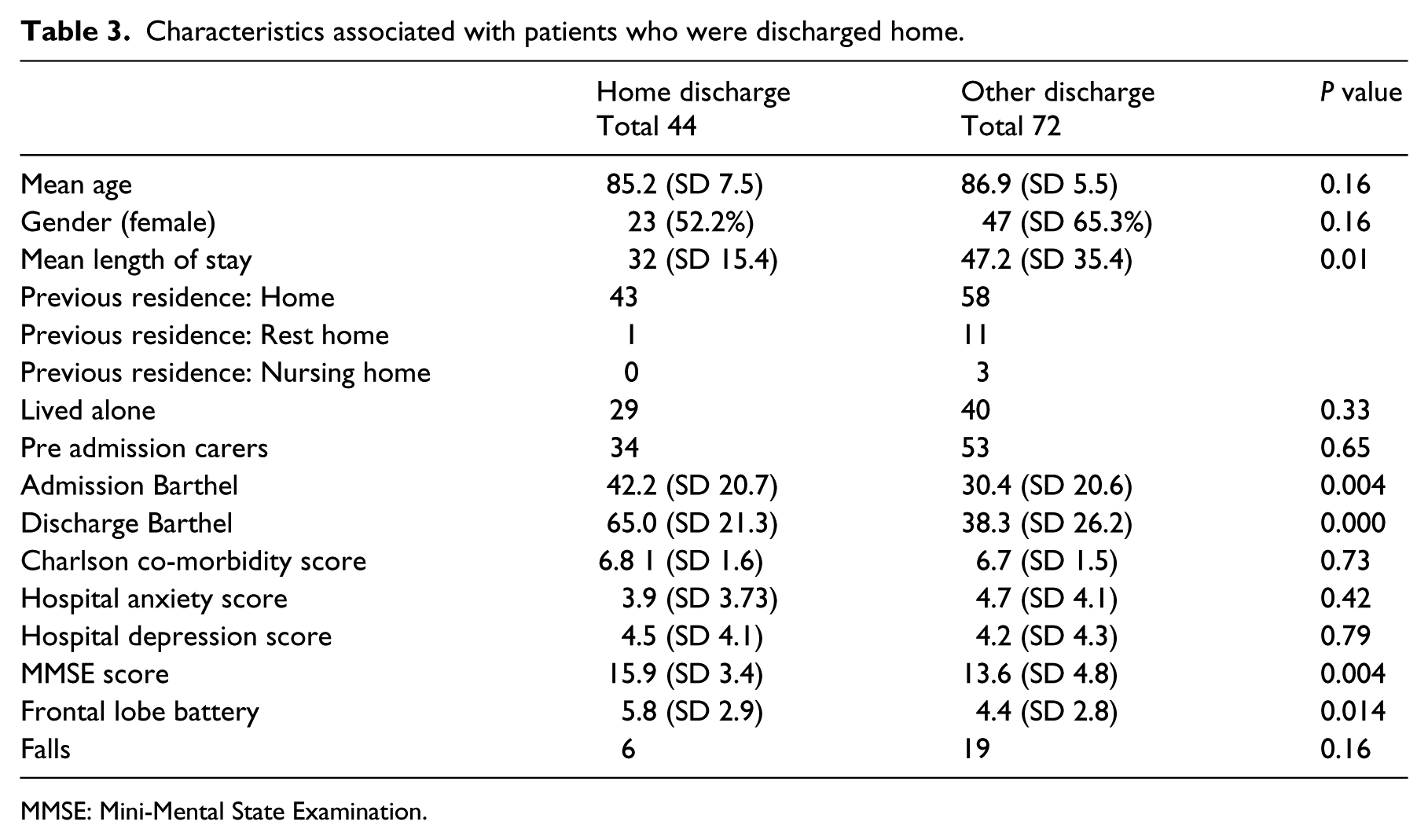
MMSE: Mini-Mental State Examination.
Discussion
Rehabilitation of cognitively impaired patients after acute illness aims to improve physical functioning as well as cognitive function and behaviour, and includes the management of any residual delirium. In this UK-based, prospective, cohort study from a rehabilitation practice for older people recovering from acute illness 55.2% of patients showed an improvement in the Barthel score after rehabilitation. This was a cohort of very frail patients and when the patients who died or had to be retransferred to the acute site for medical reasons were excluded, 72% of patients showed improvement on the Barthel score. In this cohort, the Mini-Mental State Examination was the most important factor associated with improvement in ADL, and discharge Barthel score was an important determinant of whether a patient was able to be discharged home. The number of patients showing improvement did not differ in a statistically significant way in either group, even those with severe cognitive impairment. When examining the patients who were admitted from home and discharged back home, we found that they had a significantly higher improvement in their Barthel score compared with those discharged to a nursing/residential home. Home discharges were associated in an improvement in at least three items of the Barthel score.
There are a number of weaknesses and limitations to this study. The design of the study is not a randomized controlled trial and does not provide level A evidence of the benefit of rehabilitation in patients with moderate to severe cognitive impairment. However, this was a study based in a clinical practice and the design was limited by practical factors. The numbers of patients were also relatively small, particularly in the severe cognitive impairment group. This might have been, in part, owing to difficulties getting such patients accepted for rehabilitation and difficulties getting consent and assent in this group. Patients were selected for rehabilitation and therefore there was a potential bias toward patients who were likely to improve. One can argue that the benefits observed might therefore have been inflated and would have been less had the cohort been unselected. Another limitation was the intervention was not quantified on an individual patient basis and care plans were very much tailored to patient need and ability. Rehabilitation in patients with cognitive impairment is complex and requires attention to cognition and behaviour, as well as physical rehabilitation. There is very little research of rehabilitation outcomes in such a post-acute setting in moderately to severe cognitively impaired patients, and we believe that our study outcomes contradict some perceptions about the rehabilitation of patients with moderate to severe dementia where the benefits of rehabilitation are often questioned on the mistaken premise that there is little prospect of improvement.
Although the Mini-Mental State Examination was the most important determinant of improvement in Barthel score, patients in both groups showed improvements in their ADL. Even small gains in function have the potential to improve the quality of life of patients and their carers, regardless of place of discharge. However, going home and maintaining the current place of residence is often seen as an important outcome measure of rehabilitation. Our study shows that while patients who are more cognitively impaired are more likely to be discharged to a nursing/residential home, an important determinant in achieving a home discharge was discharge Barthel score, even when considering other important factors such as preadmission carers and whether they lived alone. Patients who were discharged home made significant improvements in their Barthel score from admission when compared with those patients discharged to a nursing/residential home. In this cohort 35%–44% of patients were able to maintain their residential status at home. The level of disability, as determined by the Barthel score on admission, may well have resulted in discharges to a nursing or residential home had it not been for rehabilitation. This is an important outcome considering the potential cost and lifelong implications of a nursing or residential home placement. Our findings suggest that determining who needs rehabilitation in cognitively impaired subjects should be based on function as well as cognitive ability.
Modern patient care now requires more efficiency, with significant emphasis on reducing length of stay for operational and managerial purposes. Our results show that for cognitively impaired patients, rehabilitation to recover from acute illness is a process that requires time. 21 The average length of stay was considerably above what would currently be considered to be acceptable in a hospital. While this may cast some doubt over rehabilitation efficiency, consideration needs to be taken of the frailty of the patient in determining the intensity of rehabilitation regimes. The results show benefits and gains to be had from hospital-based rehabilitation, and emphasises the need to have proper facilities and opportunities for rehabilitation, with staff trained and prepared in the rehabilitation of patients with cognitive impairment. More out-of-hospital services are being commissioned to support older people at home and provide alternatives to hospital admission and avoid lengthy hospital stays. 22 Indeed the rehabilitation of patients with dementia and delirium might be better if carried out at home. 23 Our results show that patients showing improvements in Barthel score and number of Barthel items are more likely to be discharged home than those who do not, and that home discharge is a worthwhile goal to pursue in the rehabilitation of patients with moderate to severe dementia.
Clinical messages
A total of 55% of patients with moderate to severe cognitive impairment showed improvement in total Barthel score and in the number of Barthel items with rehabilitation. Both moderately and severely cognitively impaired patients showed improvement.
Patients showing improvements in Barthel Score and number of Barthel Items are more likely to be discharged home than those who do not.
Footnotes
Contributors
MV, LP, JS and JK were responsible for the study concept and design. MV was responsible for the data analysis and interpretation, while LP arrange the acquisition of data. JS, JK and SCA provided data interpretation. All authors took part in the preparation of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.