
Abstract
Objectives:
To explore the perspectives of healthcare professionals and commissioners working with a stroke Early Supported Discharge service in relation to: (1) the factors that facilitate or impede the implementation of the service, and (2) the impact of the service.
Design:
Cross-sectional qualitative study using semi-structured interviews. Data were analysed by two researchers using a thematic analysis approach.
Setting:
Two Early Supported Discharge services in Nottinghamshire.
Participants:
Purposive sampling identified 35 key informants including practitioners, managers and commissioners.
Results:
The identified facilitators to the implementation of evidence-based services were: (1) the adaptability of the intervention to the healthcare context, (2) the role of rehabilitation assistants and (3) cross-service working arrangements. Perceived challenges included: (1) lack of clarity regarding the referral decision making process, (2) delays in securing social care input and (3) lack of appropriate follow-on services in the region. Most respondents perceived the impact of the services to be: (1) reducing in-hospital stay, (2) aiding the seamless transfer of care from hospital to the community and (3) providing intensive stroke specific therapy. Commissioners called for greater evidence of service impact and clarity regarding where it fits into the stroke pathway.
Conclusions:
Early Supported Discharge services were perceived as successful in providing home-based, stroke specific rehabilitation. Teams would benefit from capitalising on identified facilitators and developing strategies to address the challenges. The remit and impact of the services should be clear and demonstrable, with teams strengthening links with other health and social care providers.
Keywords
Introduction
With the rising costs of hospital care, the development of services that provide home-based rehabilitation for stroke patients has attracted increasing interest. Early Supported Discharge schemes aim to facilitate the transfer of care from hospital to home, allowing people to continue rehabilitation in a familiar environment. Cumulative evidence from randomized controlled trials shows that Early Supported Discharge services delivered by coordinated, multidisciplinary teams can significantly reduce the length of in-hospital stay and improve long-term functional outcomes for patients with mild to moderate stroke. 1
Driven by the strong evidence base and national policy guidelines,2,3 Early Supported Discharge schemes are currently being implemented both in the UK and internationally. The Early Supported Discharge consensus document 4 helped clarify the core characteristics of effective evidence-based services. However, a Care Quality Commission Stroke Review revealed that existing schemes do not always comply with the models of services advocated by research evidence. 5 Reasons for the observed variation in the quality and accessibility of Early Supported Discharge services have yet to be explored.
Attention is drawn on how best to bridge the gap between evidence-based recommendations and their implementation in clinical practice.6,7 Implementation efforts may be facilitated or hindered by contextual influences, such as the attitudes of practitioners, the organisational structure and the availability of resources.8,9 A good understanding of these factors is considered an essential first step in informing improvement strategies and achieving lasting changes in practice.10,11
The accounts of professionals who drive the implementation of healthcare innovations allow an insiders’ perspective into contextual factors affecting the process.12,13 Drawing on clinical expertise, they can offer a frontline view of the issues that arise when developing a new service and the extent to which the benefits reported in clinical trials are evident in practice.
Previous research has paid minimal attention to the opinions of key stakeholders involved in Early Supported Discharge services. This study set out to explore the perceptions of healthcare professionals and commissioners regarding: (a) the challenges and facilitators to the implementation of an evidence-based service and (b) the perceived impact of Early Supported Discharge services.
Methods
The study sample was drawn from two Early Supported Discharge services in the East Midlands. The two sites will be referred to as Site A and Site B. The services were selected based on the fact that they were informed by an evidence-based service specification document. 4 At the time of the study both services were in their first year of operation and were delivering the service at around full capacity. Both teams used specific eligibility criteria for acceptance of patients to the Early Supported Discharge service including: Barthel Index ≥ 14/20; transfer independently or with assistance of one (+/-equipment); sufficiently medically fit to be managed at home; identified achievable rehabilitation goals. The team composition and links with other services in the region (e.g. existence of community stroke team) is outlined in Table 1.
Summary of the key characteristics of each service.
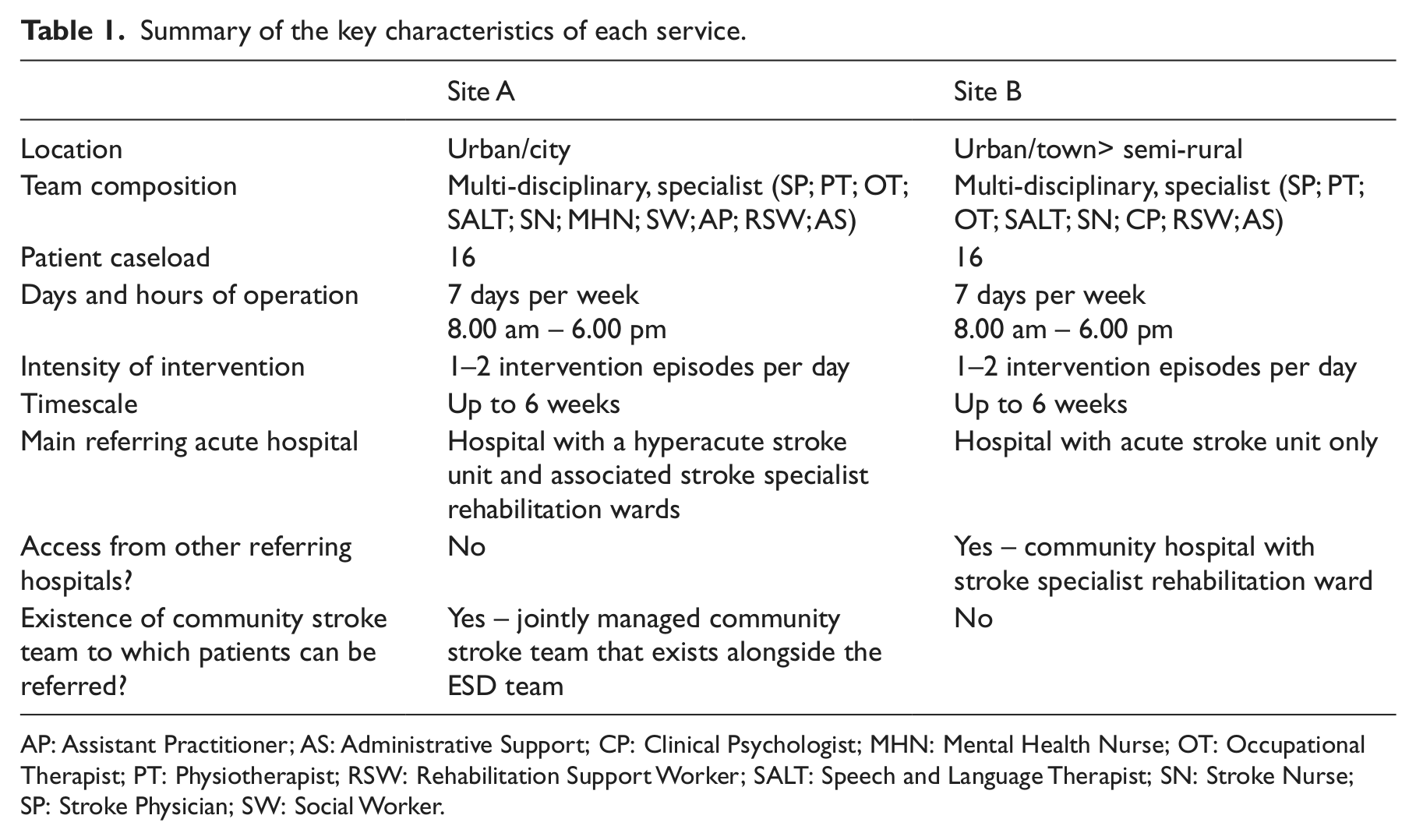
AP: Assistant Practitioner; AS: Administrative Support; CP: Clinical Psychologist; MHN: Mental Health Nurse; OT: Occupational Therapist; PT: Physiotherapist; RSW: Rehabilitation Support Worker; SALT: Speech and Language Therapist; SN: Stroke Nurse; SP: Stroke Physician; SW: Social Worker.
Purposive sampling was used to identify a group of key stakeholders involved with the two services: clinical practitioners delivering the intervention, managerial staff, people involved in commissioning and hospital staff referring into the service. 14 The initial contact with each site was made through the existing local stroke research network. Each interviewee recommended other potential participants until a comprehensive list of healthcare professionals and commissioners was built. 15 With line manager permission information sheets were provided and informed consent was obtained.
Face to face semi-structured interviews were conducted by either one of two researchers (MK, RF) and lasted approximately 45 min. Questions were not fixed but needed to cover the following topics: respondents’ involvement with the service, factors facilitating or impeding the implementation of the service, perceived impact and suggestions for improvement. Interviews were audio recorded, transcribed verbatim and anonymised.
The transcribed text was initially coded to the following broad categories: facilitators, challenges and impact. Data within each category were then summarised into themes following a procedure described by Braun and Clarke. 16 Key themes included issues that were frequently raised by participants. Interviews from each site were analysed separately but the results were then compared to identify similarities and differences. To minimise researcher bias, data were analysed independently by two researchers (MK, NC). Differences in coding and interpretation were discussed and new insights allowed refining of the thematic network. A qualitative data analysis software package (QSR NVivo 9, QSR International Pty Ltd.) was used to organise the data electronically.
Results
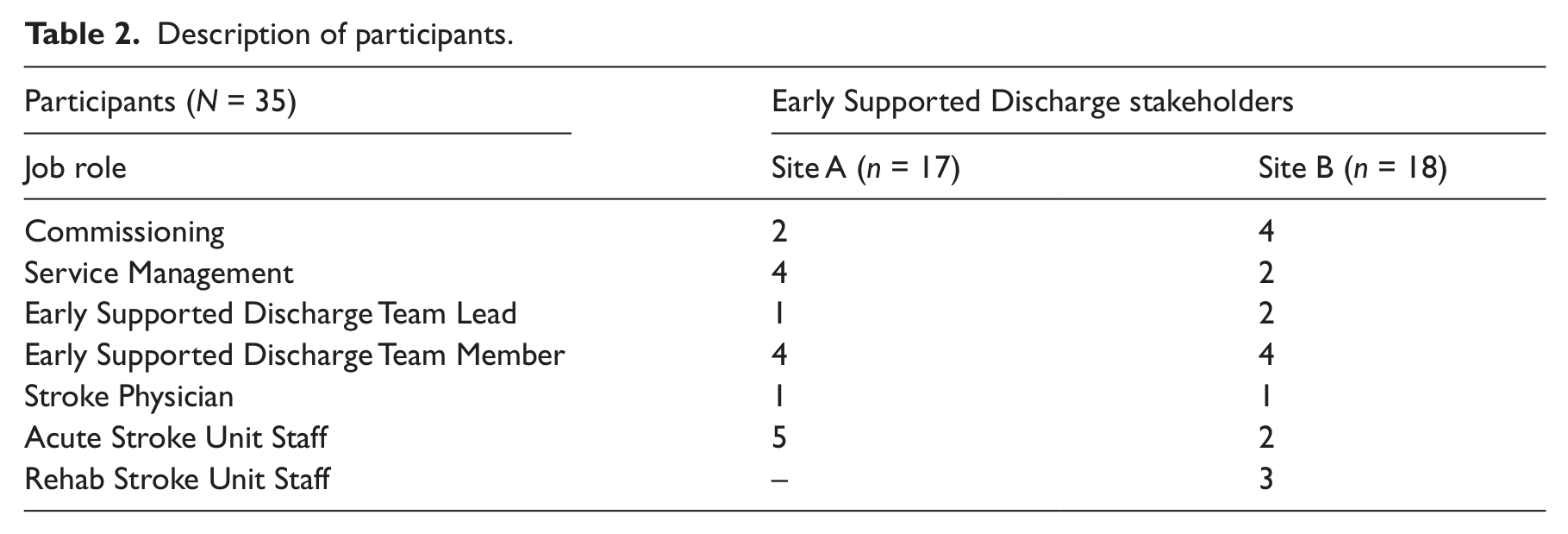
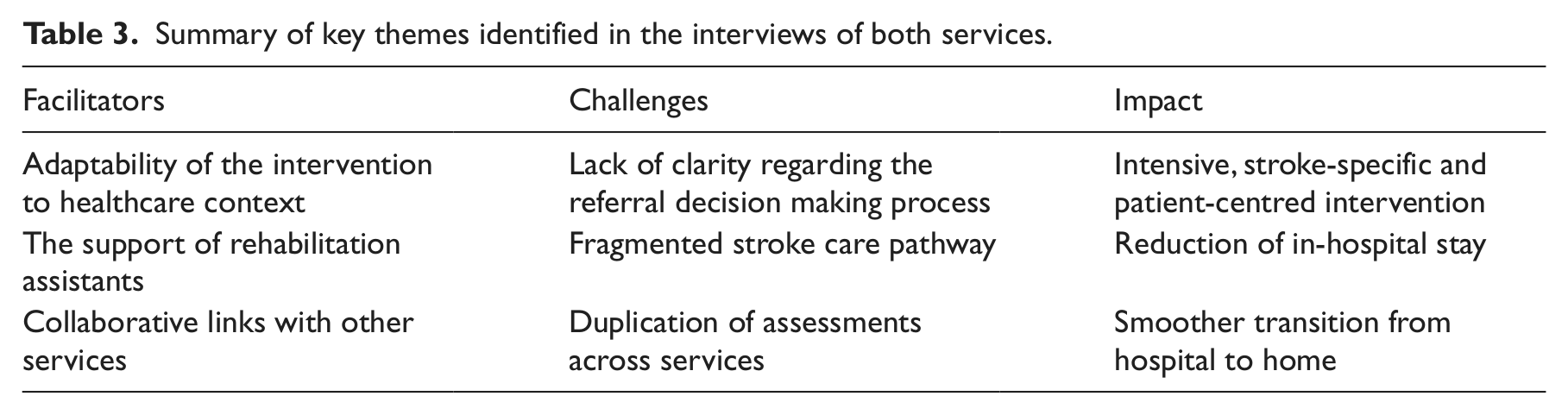
Thirty-five people working in an Early Supported Discharge-relevant job role were interviewed (see Table 2). Comparison of the results of the two sites indicated considerable overlap in the views of respondents. The themes outlined below represent recurring topics of discussion in both sites (Table 3). Discrepancies between the two sites are highlighted and reported.
Description of participants.
Summary of key themes identified in the interviews of both services.
Facilitators
Five respondents from both sites described the eligibility criteria governing patient access to the service as clear enough to permit the identification of appropriate cases without being too restrictive, attaining a balance between flexibility and specificity: ‘I think the criteria are good because they are not too defined or too loose; I think there are very few inappropriate people that come through’ (Stroke Physician, 1). However, most respondents stressed the need to adapt certain components of the intervention to respond to the local healthcare context and the variation that characterises the stroke population ‘No two stroke cases are ever going to be the same; our systems need to be reflective of that’ (Commissioning, 23). To determine eligibility, the Site A team evaluated the severity of disability but the safety of the home environment and the identification of specific rehabilitation goals were set as a priority.
Regarding the length of the intervention, in Site B, it could be extended further than six weeks to compensate for the lack of stoke specialist community rehabilitation service in the region. Alternatively, the intervention could last only a few weeks to benefit milder spectrum patients. This flexible approach was endorsed by three respondents in Site A who argued that ‘sticking to the magic six week timeframe’ could unnecessarily prolong the service and delay new admissions: ‘There is some reluctance to discharge someone even if they have achieved their goals… people may need us for a few days’ (Service Management, 5).
The contribution of rehabilitation assistants (carried out by either assistant practitioners or support workers) in promoting the sustainability of the service was discussed by the majority of respondents. Their role involved: (a) delivering rehabilitation treatment plans, set by qualified therapists, (b) updating therapists on patients’ progress and (c) completing outcome assessments. In Site A, assistant practitioners were more autonomous than support workers, being able to progress rehabilitation goals or take over the care of less complex patients. According to eight respondents, assigning rehabilitation assistants to deliver the repetitive everyday exercises allowed the highly skilled staff to focus on the more specialist elements of rehabilitation: ‘It’s about being able to break down the role and make sure that the right skilled person is doing the right part of the intervention’ (ESD Team Lead, 3).
Participants agreed that the development of strong links with other services was critical to the success of early supported discharge. The Site B team reported that their close working relationship with the acute service had facilitated the identification of appropriate patients: ‘We’ve really endeavoured to build up a good relationship with the different organisations and I think the better that is, the better the team runs because you are getting referrals and good understanding’ (ESD Team Lead, 29). Key factors enabling a successful collaboration between services were identified. Participation in meetings and common training events was seen as an effective way of developing and sustaining communication channels. It was also suggested that working arrangements, such as staff rotations across services, promoted a better understanding of each team’s role, permitted the exchange of skills and knowledge and gave service users a sense of continuity along the pathway ‘We could have some rotational element between staff so you can really share that sort of approach and the learning’ (ESD Team Lead, 3).
Challenges
Hospital staff was perceived as occasionally reluctant to hand over patients to the Early Supported Discharge service as discussed by four team members in Site A. This could result in an unnecessarily prolonged in-hospital stay. Hospital staff attributed their scepticism to knowledge gaps regarding the content and the outcomes of Early Supported Discharge as well as the actual referral decision-making process. The need for more information around these issues, particularly in the first year of the service operating, was emphasised by seven respondents: ‘Just getting a bit more understanding of what the content is so that we can decide that Early Supported Discharge is in the best interests of the patient’ (Acute Stroke Unit Staff, 8). Another area of uncertainty related to the optimal time for deciding on patients’ suitability for Early Supported Discharge. In Site A, opinions varied with two respondents arguing that discussions with Early Supported Discharge services should be made ‘the minute patients arrive in the acute unit’. Four others argued that the first two weeks after stroke is a very early stage for such decisions as ‘A lot of recovery will be happening while patients are still on the acute’. In practice, the Site A team reportedly adopted a flexible approach, allowing for staff clinical expertise and experience to inform decision making.
Four commissioners underlined the need to clarify the position of Early Supported Discharge in the context of the stroke pathway: ‘To be honest I am bit foggy about where Early Supported Discharge sits alongside intermediate care and re-enablement and how these are married up’ (Commissioning, 23). The process of securing social care input was presented by 11 respondents as ‘one of the biggest stumbling blocks’ to patients’ timely discharge, offsetting the effect of Early Supported Discharge. Most team members in Site A reported that the inclusion of a social worker in the team mitigated the problem. On the contrary, the Site B team stopped providing the service after delays were observed in the discharge of patients waiting for care packages: ‘Patients were bottlenecking up at the other end because their care packages wouldn’t be ready; at eight weeks we’d still got these patients’ (Service Management, 18).
Another issue that was stressed by seven respondents from both sites was the lack of specialist community services that could respond to the complex needs of more disabled patients. Respondents identified a gap in the pathway that led to the Early Supported Discharge service admitting more dependent patients: ‘Sometimes they think we are social care and we are not….we have done things above and beyond what we are expected to do’ (ESD Team Member, 10). In Site B, the team viewed the lack of a community stroke service as one of the biggest challenges to their work. Patients with ongoing needs would have to be referred to generic rehabilitation settings: ‘Patients who need more intensity than an outpatient programme could provide or those for whom home environment is more suitable, fall into a black hole at the moment’ (ESD Team Lead, 29).
Eight interviewees also talked about the unnecessary duplication of assessments across services and stressed the need to improve data-sharing practices between hospital and Early Supported Discharge teams. It was envisioned that a further integration of the pathway would involve the establishment of joint performance monitoring systems.
Perceived impact of an Early Supported Discharge service
The majority of Early Supported Discharge members from both sites described their service as successful in reducing the length of hospital stay without compromising the intensity of rehabilitation input. ‘Patients are able to come out of the hospital sooner which is what they prefer, and they are able to continue specialist rehabilitation in their own environment…so they can have some of their normal life going on and have their family involved’ (ESD Team Lead,3).
The role of Early Supported Discharge in ‘bridging a big part of the gap in community-based rehabilitation’ formed a major theme in the interviews of Site B team. In Site A, five interviewees emphasised the contribution of the service in improving collaboration between the acute and community stroke services: ‘Transfer between the services has improved and works in a much more seamless way’ (Service Management, 4).
Nineteen respondents described the provision of specialist stroke care as critical for the successful rehabilitation of stroke patients in the community, maximising their recovery potential and facilitating the continuity of care across services. It was seen as a key component of the service, defining its identity and role. As commented by an interviewee, ‘Having the knowledge to deal with stroke patients is what sets the service aside from other community services’ (Acute Stroke Unit Staff, 16).
According to 11 respondents, the home-based model of rehabilitation offered therapists an ecologically valid appraisal of patients’ difficulties and, therefore, allowed tailoring the intervention to patients’ needs and priorities. ‘It is less about a body in a bed that needs a bit of fixing; to me, it feels more of a holistic service; just being in peoples’ houses, seeing what problems they actually have and adapting the service around that’ (ESD Team Member, 30). Emotional issues could be addressed in a timely manner during Early Supported Discharge according to seven respondents who observed that emotional and cognitive difficulties may not be fully expressed before hospital discharge: ‘Even people that have minimal physical impairments can be really anxious because their whole life has changed’ (ESD Team Lead, 29). It was acknowledged, however, that fully tackling these issues within the brief timeframe of Early Supported Discharge service can be extremely challenging.
Three commissioners requested greater evidence as to whether Early Supported Discharge is ‘the most efficient and effective way of providing rehabilitation and helping patients make the best of their recovery’(Commissioner, 34). They argued that the current economic climate stresses the need for a more rigorous evaluation of the services’ outcomes. It was suggested that the mechanisms through which the Early Supported Discharge outcomes are communicated should be further improved: ‘we need more info on the outcomes of the intervention…they need to demonstrate what they can offer…to sell themselves really’ (Acute Stroke Unit Staff, 16).
Discussion
This study explored contextual factors associated with the implementation of Early Supported Discharge services. Identified facilitators included: the adaptability of the intervention to meet patients’ needs and the local context, the involvement of rehabilitation assistants in delivering rehabilitation plans and the development of strong links with collaborating services through boundary spanning working arrangements. Uncertainty regarding the referral decision-making process, delays in securing social care input and lack of appropriate follow-on community services were perceived as the main challenges to the smooth operation of the service. The need to promote joint data recording systems across services was also stressed. Respondents’ accounts conveyed a predominantly positive picture regarding the impact of their service. However, a clear message from the interviews of commissioners was that services need to be able to demonstrate the effectiveness of the Early Supported Discharge intervention.
In both sites, decision making regarding patients’ eligibility to access the service was informed by the criteria set in an evidence-based service specification document, case by case clinical considerations and a focus on patient safety. This is in line with practices in other services offering Early Supported Discharge interventions both in the UK 17 and internationally. 18 In addition, and echoing the findings of the Early Supported Discharge consensus, 4 most respondents agreed that the length of the service should be adapted to patients’ needs and the availability of other community- based stroke services in the area. This flexible approach was seen by most respondents as a factor promoting the responsiveness of the service to patients’ needs and the local characteristics of healthcare provision. Subjectivity in the decision-making processes, however, may lead to inconsistencies that undermine the evidence-based components of the service. Early Supported Discharge has been shown to be beneficial for mild to moderate stroke patients, 1 so being overly inclusive may compromise these positive outcomes. In this study, the service criteria were stretched to accommodate for the lack of community services for patients with more complex needs. It is important that stakeholders address the continuity of care beyond Early Supported Discharge in a timely manner.
The analytical approach of this study permitted the exploration of similarities and differences between the two Early Supported Discharge models and allowed consideration of variation and contradiction in the results. A limitation of the qualitative design is that it does not permit statistical generalisation of the findings. However, the lessons learned in this study could be transferable to other services. The sampling strategy ensured that viewpoints from a range of key stakeholders were represented in the data. The fact that similar issues were raised by participants from different services and professional backgrounds further supports the transferability of the findings. The relevance of these findings to different models of Early Supported Discharge interventions needs further exploration.
The two teams operated within an urban and semi-rural setting respectively; therefore, the need to examine the specific challenges associated with the implementation of Early Supported Discharge within rural setting remains. Furthermore, the opinions of service users should also be explored in order to obtain a more rounded appreciation of the service. 19 The interviews were conducted when both services were at an early stage of their development. It is, therefore, unclear whether our findings generalise to later phases of service implementation. Understanding the longer term challenges is necessary in order to identify ways of promoting the sustainability of the service. 20 Future research should explore how these models have evolved over time and have become established beyond the initial period of their operation.
Our findings highlight the contribution of Early Supported Discharge services in filling a gap in the stroke pathway at a critical stage of transfer from hospital to home. The need for clarity of procedures operating between services has been identified by healthcare professionals as critical for the success of the interventions. 21 Similarly, the importance of building mutual trust and support between stakeholders is stressed, particularly when the intervention crosses professional and organisational boundaries. 21 According to Greenhalgh et al., 22 organisations that support external boundary-spanning roles of their staff are more likely to successfully assimilate innovative interventions. It is suggested that encouraging working arrangements that promote interaction between hospital and community teams, may allow professionals to obtain a better understanding of the role and function of collaborating services. Future studies should evaluate the value of interactive educational interventions as an arena of knowledge exchange between stakeholders with the view of addressing the identified barriers and improving evidence-based practice.
Interviewees were unanimous in their request for a more seamless and streamlined experience for their patients. As noted by Fitzgerald et al., 23 owing to the complexity of their nature, innovative healthcare services cannot be implemented without interacting and impacting on the function of other services in the pathway. The importance of considering services as ‘events in systems’ and not in isolation from the broader organisational context is emphasised. 24 Service specifications should look at the whole picture and clarify the decision-making process that guides a patient’s journey through the stroke care pathway. 25
Clinical messages
Early supported discharge services were perceived as a positive development, contributing to the integration of the stroke care pathway.
Perceived facilitators to the implementation of services included the adaptability of the rehabilitation intervention, the support of rehabilitation assistants and collaborative links with other services.
Identified challenges involved delays in securing social care and uncertainty around patients’ referral to the service.
Footnotes
Acknowledgements
The authors wish to thank the participants for their time. We are grateful to Dr Amanda Crompton for her helpful comments on the manuscript.
Conflict of interest
None declared.
Funding
This research was funded by the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care for Nottinghamshire, Derbyshire and Lincolnshire (NIHR CLAHRC NDL). The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.